
Abstract
The literature highlighted the need for evidence-based occupational therapy teleinterventions to improve work participation among adults with attention-deficit/hyperactivity disorder (ADHD). This study aimed to assess the efficacy of a self-tailored, metacognitive, telehealth intervention to enhance the performance of adults with ADHD at work (Work-MAP). The outcome measures were efficacy and satisfaction with performing self-selected work goals, executive functions, and quality of life. Participants in this randomized controlled trial were 46 adults with ADHD. Group A (n = 31) received the synchronous, hybrid-telehealth intervention in 11-weekly 1-hour individual sessions. Group B (n = 15) completed the intervention after a waiting phase. Following the intervention, participants showed and maintained significant improvements in all outcome measures (strong-to-moderate significant effects) to the 3-month follow-up. The Work-MAP teleintervention appears effective for improving work participation (i.e., performance), executive functions, and quality of life of adults with ADHD.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a childhood-onset neurodevelopmental disorder. The Diagnostic and Statistical Manual of Mental Disorders (5th ed., text rev.; DSM-5-TR; American Psychiatric Association [APA], 2022) defines it as patterns of developmentally inappropriate and impairing levels of inattention, hyperactivity, and impulsivity. Furthermore, ADHD is a lifespan disorder with a high incidence of further neurodevelopmental disabilities and prevalence rate of 2.5% to 5.0% in the adult population (Kooij et al., 2019). The DSM-5-TR (APA, 2022) and other evidence emphasize that ADHD is characterized by behavior patterns associated with impairments in multiple daily living domains, including the work domain (e.g., Fuermaier et al., 2021).
According to the American Occupational Therapy Association (AOTA, 2020), the work domain has high importance in adults’ lives (Fuermaier et al., 2021). It contributes to self-esteem and shapes identity by defining a meaningful role, supports health, and promotes subjective well-being (e.g., Roney & Soicher, 2021). Effective work participation and performance at work require implementing complex abilities, such as self-management relative to time, planning, problem-solving, and self-activation (Barkley & Murphy, 2010). Executing these and other abilities may lead to better performance of goal-directed activities at work.
The term personal projects (Little, 2020) describes the person’s ability to set goal-directed activities and organize their days (Rosenblum, 2017). In a work context, the term describes setting and satisfactorily performing self-selected work goals. Studies have used goal-directed work activities to examine employment experiences and as an intervention outcome measure (e.g., Roddy et al., 2021). This study used the Canadian Occupational Performance Measure (COPM; Law et al., 2005) to set participants’ self-selected work goals (derived from their goal-directed work activities) and evaluate their perceptions by ranking the efficacy of and satisfaction with the performance of those goals. Low rankings of goal-directed activities at work may be a manifestation of poor performance at work.
Adults with ADHD struggle with impaired work performance (Anker et al., 2019) and often report major impairments while working due to their ADHD symptoms (Joseph et al., 2019). Furthermore, ADHD has been associated with tendencies toward unemployment, job instability, work accidents, and sickness absences (e.g., Fuermaier et al., 2021). Occupational therapy is based on the belief that active engagement in occupation supports and maintains health and participation (AOTA, 2020). Therefore, it is crucial that occupational therapists identify evidence-based interventions to address the work participation challenges of adults with ADHD (Smith et al., 2017) and, by that, promote their health (Grinblat & Rosenblum, 2022).
The term executive functions (EF) refers to a set of higher level cognitive functions that are the underlying mechanisms required to perform and participate effectively in complex, nonroutine, self-directed activities in varied situations and environments (AOTA, 2020). Executive functions influence the individual’s performance at work (Barkley & Murphy, 2010), and EF deficiencies have been described as consistent and discriminating predictors of adult ADHD (Adler et al., 2017). Thus, EF deficiencies of adults with ADHD might interfere with their ability to perform well at work.
Along with deficient work performance and EF challenges, adult ADHD has been tied to a lower quality of life (QoL; Engel-Yeger, 2022). The literature indicates associations among employee performance, well-being at work, and QoL (e.g., Fogaça et al., 2021) and relationships among EF, goal-directed activities, and QoL (e.g., Little, 2020). Therefore, higher EF and improved efficacy of and satisfaction with the performance of self-selected work goals may manifest in better QoL. Because QoL and occupational performance are outcomes targeted in occupational therapy interventions (AOTA, 2020), it is important to address this need as reflected in adults with ADHD.
Despite the wide-ranging implications of poor work performance of adults with ADHD—including possible implications on their mental health and QoL—most adults with ADHD remain untreated (e.g., Kooij et al., 2019). To our knowledge, evidence-based occupational therapy interventions aiming to improve work performance among adults with ADHD are still scarce and required (Adamou et al., 2021).
The Metacognitive Self-Tailored Telehealth Intervention for Adults with ADHD Performance at Work Enhancement (Work-MAP) was designed based on the current literature and occupational therapy models. The person-environment-occupation-performance model (Baum et al., 2015) was used to identify and raise self-awareness of factors in these domains that enable and hinder each participant’s performance at work. Driven by this comprehensive analysis, each participant chooses meaningful goal-directed work activities as personal intervention goals.
Given EF’s possible contribution to work-performance success among adults with ADHD, Work-MAP considers the personal EF features of each participant as key elements in developing and executing this self-tailored intervention. The dynamic interactional model of cognition (Toglia, 2018) promotes performance by changing personal factors (metacognitive components of strategies and self-awareness), activity, and environment, and all three areas are simultaneously addressed within the Work-MAP intervention. In addition, Work-MAP promotes self-generating personal strategies and increases efficient strategy use across meaningful everyday work activities, consistent with the dynamic interactional model. The Work-MAP protocol comprises three modular units reflecting the essential elements of the model for employment success for adults with learning disabilities and ADHD (Gerber, 2001).
Work-MAP was designed as a synchronous and hybrid teleintervention; most sessions are conducted online. Although the literature addresses the benefits and relevance of telehealth use for occupational therapists and their clients, especially for adults with ADHD, evidence-based occupational therapy teleinterventions for this population remain scarce (Nobakht et al., 2017).
The aim of this study was to evaluate the effects of Work-MAP on the efficacy of and satisfaction with the performance of self-selected work goals, EF, and QoL among adults with ADHD.
Methods
Design
This randomized controlled trial used a waiting-list control design. The data were collected between June 2018 and December 2019 following ethical approval (University of Haifa Ethics Committee, approval No. 032/17). All participants signed written informed consent forms before participation. This study is a part of a larger study reported previously (Grinblat & Rosenblum, 2022) according to CONSORT guidelines (Supplemental Table 1) and registered through ClinicalTrails.gov (Identifier: NCT05270226).
Participants
We calculated a sample size of 50 participants using G*Power software guidelines, considering the medium effect size of f2(V) = .0625, significance of α = .01, and power of 0.90. People with ADHD from communities across Israel were invited via email or social networks to participate in the study. A research assistant interviewed via telephone volunteers who signed informed consent, presented a formal medical ADHD diagnosis, and manifested ADHD symptoms according to the Adult ADHD Self-Report Scale version 1.1-Screener (ASRS Screener; Kessler et al., 2005) as an initial screener. Participants completed self-reported questionnaires online (details follow) to confirm inclusion and exclusion criteria.
The inclusion criteria were (a) 20 to 45 years of age, (b) worked at least 3 months at the same workplace, (c) did not receive additional functional treatment during the study period, and (c) read and wrote Hebrew fluently. An additional inclusion criterion was a formal medical ADHD diagnosis by an expert neurologist, psychiatrist, or family doctor based on the DSM-5 (APA, 2013) and ADHD symptoms according to the ASRS Screener (Kessler et al., 2005). Participants’ ADHD symptom consistency (Pawaskar et al., 2020) was also confirmed as medium-to-high probability of ADHD according to the Brown Attention-Deficit Disorder Scales (BADDS; Brown, 2012). Because the BADDS assesses a wider range of attentional/EF impairments than the ASRS (Brown et al., 2011) captures, we also used the BADDS to examine possible differences between Groups A and B, describe sample background characteristics, and accurately direct the intervention to participants’ specific needs. Furthermore, considering the central role of EF deficits in adult ADHD (e.g., Adler et al., 2017), all participants had at least one EF deficit according to the Behavior Rating Inventory of Executive Function-adult (BRIEF-A; Roth et al., 2005). People who self-reported co-occurring mental health disorders, motor or neurological disabilities, chronic diseases, or significant injuries were excluded from participation. However, considering this population’s high coexisting incidence, participants with co-occurrence of specific learning disabilities were not excluded.
Initially, 209 adults contacted the researcher to participate. Of them, 73.6% were excluded based on the exclusion criteria. The resulting sample included 52 adults with ADHD, who were allocated and randomized into Group A (n = 35) or Group B (n = 17). Of these, 46 (88.4%) completed the intervention (Figure 1). Thus, the data analysis was based on the 46 participants in Group A (n = 31) and Group B (n = 15).
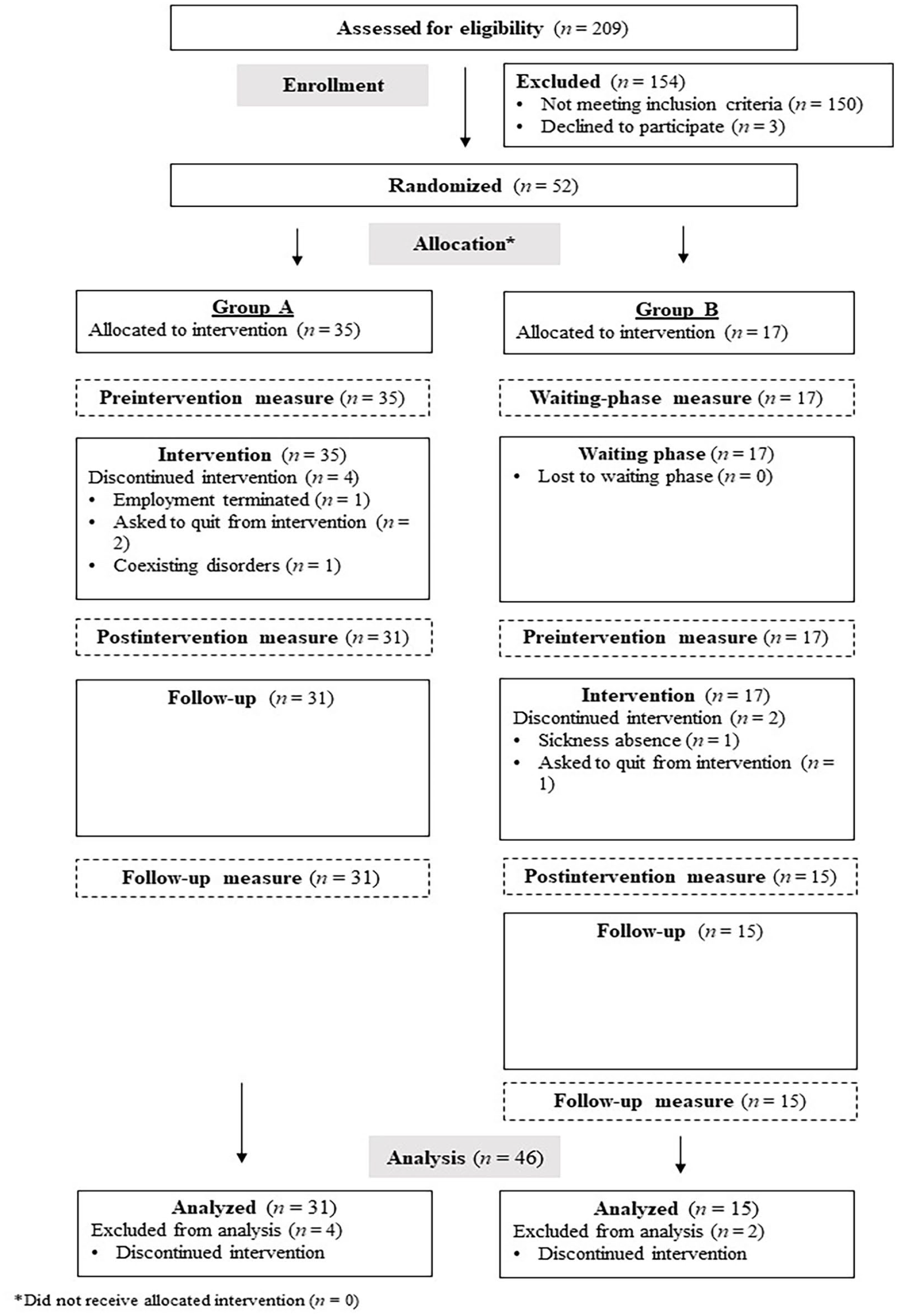
CONSORT Flowchart of Participants’ Allocation to the Study and Study Procedures.
Randomization and Blinding
The randomization sequence was created using a manual permuted block design, with a 1:2 allocation and a block size of 6. The main researcher performed the randomization using six sealed envelopes—four for Group A and two for Group B. Participants randomly chose an envelope when they enrolled. The randomization results were blinded for the participants and occupational therapists who performed the intervention processes.
To address potential bias, participants completed the study assessments online independent of occupational therapist involvement, except for the COPM score (third intervention session). The main researcher was available by telephone if participants needed assistance. Neither the occupational therapists nor the participants were exposed to any study measure’s preintervention or postintervention scores except the first COPM measure.
Procedure
Participants completed the study assessments at three or four time points (Figure 1), depending on their group allocation. Group A completed the study questionnaires 1 week before their first intervention session (preintervention measure, baseline), immediately after the last intervention session (postintervention measure, 12–13 weeks after baseline), and 3 months after intervention (follow-up measure, approximately 6 months after baseline). Group B completed the study measures at the same intervals as Group A throughout the study period (preintervention, postintervention, follow-up). Group B waited while Group A received the intervention and completed an additional assessment 11 to 12 weeks before their first intervention session (waiting-phase measure, approximately 3 months before baseline). After completing the follow-up assessment, all participants received a voucher for their time and effort.
Intervention
All study participants (Groups A and B) received the same intervention of 11-weekly 1-hour individual sessions. The intervention was a synchronous and hybrid teleintervention. Eight of the 11 sessions were conducted online (via videoconferencing), and three were face-to-face. See Table 1 for a description of the intervention protocol content.
Intervention Protocol Content.
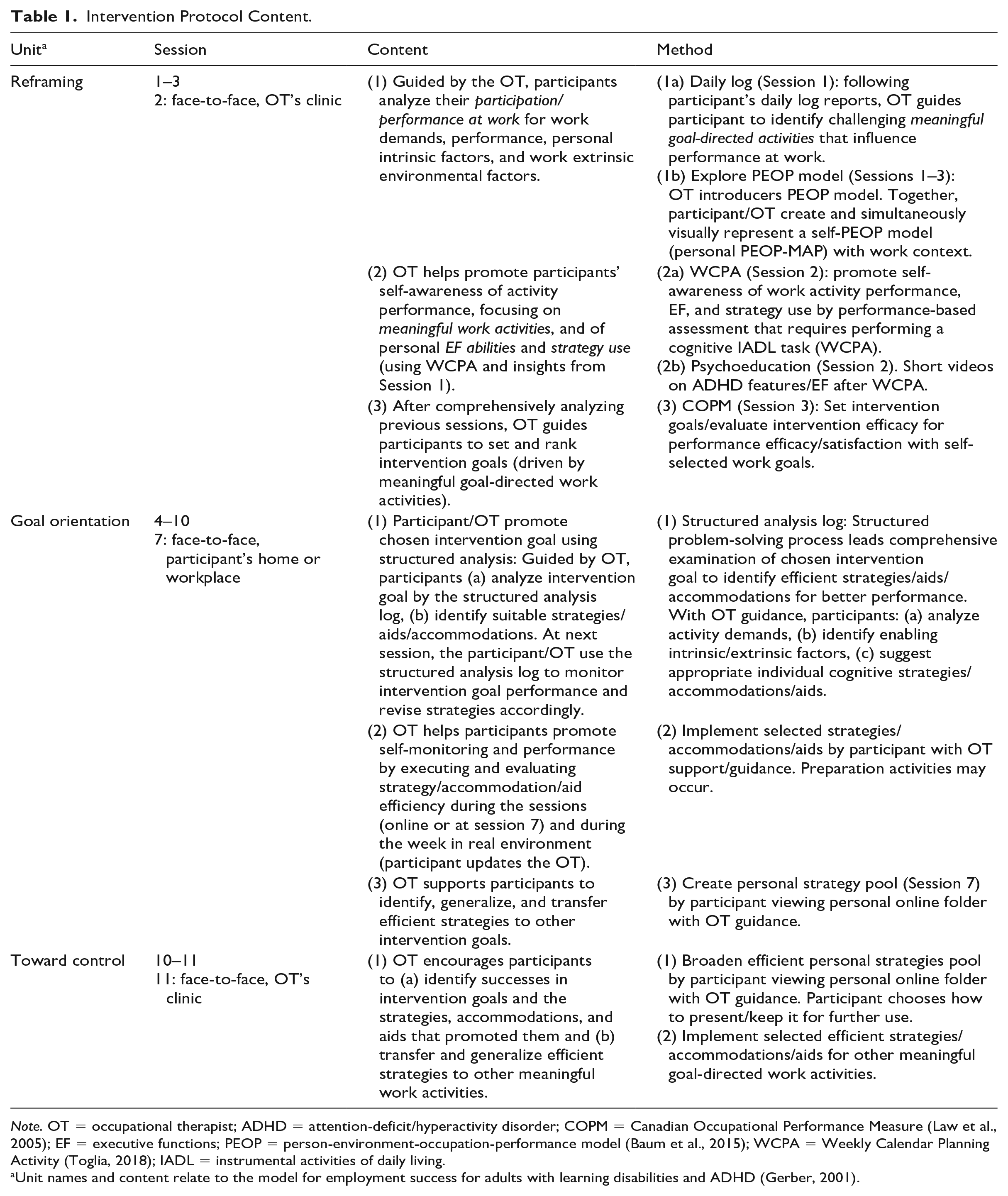
Note. OT = occupational therapist; ADHD = attention-deficit/hyperactivity disorder; COPM = Canadian Occupational Performance Measure (Law et al., 2005); EF = executive functions; PEOP = person-environment-occupation-performance model (Baum et al., 2015); WCPA = Weekly Calendar Planning Activity (Toglia, 2018); IADL = instrumental activities of daily living.
Unit names and content relate to the model for employment success for adults with learning disabilities and ADHD (Gerber, 2001).
The main researcher chose seven occupational therapists to implement the intervention. To enhance and monitor the intervention’s fidelity and ascertain its reliability, the main researcher (a) developed a standardized written protocol, (b) trained and guided the occupational therapists in an 18-hour training session, and (c) counseled the occupational therapists in personal online meetings every 1 to 2 weeks during the intervention periods. All sessions were videorecorded and audiorecorded and documented in a written log.
Instruments
Screening and Background-Characteristics Questionnaires
ASRS Screener
The ASRS Screener (Kessler et al., 2005) is a standardized, well-validated, reliable, self-reported, six-item screening scale for adult ADHD. It has been validated for Hebrew (Zohar & Konfortes, 2010).
BADDS
The BADDS (Brown, 2012) is a standardized, well-validated, and reliable self-report screening scale for adult ADHD. The scale’s items are grouped into five clusters: organizing and activating to work (activation), sustaining attention and concentration (attention), sustaining energy and effort (effort), managing affective interference (emotion), and utilizing working memory and accessing recall (memory). Cluster t scores greater than 65 are considered clinically significant. We used the validated Hebrew version (Brown, 2012). In this version, total t scores of less than 40 indicate a low risk of ADHD, 40 to 54 indicate medium risk, and 55 or higher indicate high risk.
Sociodemographic Questionnaire
The self-reported sociodemographic questionnaire included questions about participants’ sociodemographic status, diagnoses, and current employment status.
Outcome Measures
COPM
The COPM (Law et al., 2005) is a primary outcome measure of self-perception of performance efficacy and satisfaction with the performance of self-selected work goals. Its reliability, validity, and responsiveness have been satisfactory to excellent. During the semistructured interview, participants identify two meaningful activities in which they perceive the most significant performance difficulties at work or that most influence their work performance. Those two activities are set as work goals. Participants rate each work goal for performance efficacy from 1 (not able to do at all) to 10 (able to do extremely well) and rate satisfaction with performance similarly. During the study measures, participants rerank their work goals. A score change of two or more points is considered clinically significant (Law et al., 2005).
BRIEF-A
The BRIEF-A (Roth et al., 2005) served as a screening tool and primary outcome measure. The BRIEF-A is a standardized, well-validated, reliable, and ecological self-report scale capturing adults’ views of their EF in their everyday environments. The score includes a global executive composite (GEC) index representing the overall EF score, composed of behavioral regulation index (BRI) and metacognition index (MI) scores with nine nonoverlapping score scales. Scores of 65 or more (SD > 1.5) indicate a clinical deficit. We used the validated Hebrew version (e.g., Grinblat & Rosenblum, 2016).
Adult ADHD Quality-of-Life Questionnaire
The Adult ADHD Quality-of-Life Questionnaire (AAQoL) (Brod et al., 2005) is a secondary outcome measure. It is a standardized, well-validated, and reliable self-report questionnaire that measures the QoL of adults with ADHD (Zare et al., 2017). Moreover, it has demonstrated good responsiveness to changes in ADHD symptom severity (Marfatia et al., 2011). The AAQoL results yield a total QoL score and four-subscale scores. Minimally, an eight-point difference in AAQoL scores is considered a clinical improvement (Tanaka et al., 2019).
Data Analysis
All statistical analyses were performed using SPSS (version 25) with a significance level of p < .05. Data analysis was completed in several stages: (a) Demographic and occupational variables of Groups A and B were compared using chi-square tests. (b) T tests for independent variables were used to examine differences in the dependent variables between the groups before the intervention and differences in Group B scores during the waiting phase (waiting-phase and preintervention measures). (c) Tests of within-subject effects were used to examine the existence of interaction effects between the two groups. Based on those results, the two groups (A and B) were treated as one (N = 46) in further analyses. (d) Descriptive statistics were used to describe the entire sample. (e) Repeated-measures multivariate analysis of variance (MANOVA) with Bonferroni correction and pairwise comparisons (p < .05) were used to evaluate differences among preintervention, postintervention, and follow-up assessments. Partial eta-squared (ηp2) was reported as the effect size using Cohen’s (2013) benchmarks to define small (ηp2 = .01), medium (ηp2 = .06), and large (ηp2 = .14) effects.
Results
Between-Group Differences
As presented in Table 2, chi-square and t tests for independent variables yielded no significant differences between Group A (n = 31) and Group B (n = 15) in demographic and occupational characteristics. Furthermore, no significant group differences (A and B) were found in number of workplaces since the age of 20 years, t(44) = −.55, p = .54. The BADDS (Brown, 2012) scores showed similar ADHD characteristics in both groups, t(44) = .48, p = .63.
Participants’ Demographic and Occupational Characteristics by Group and All Sample.
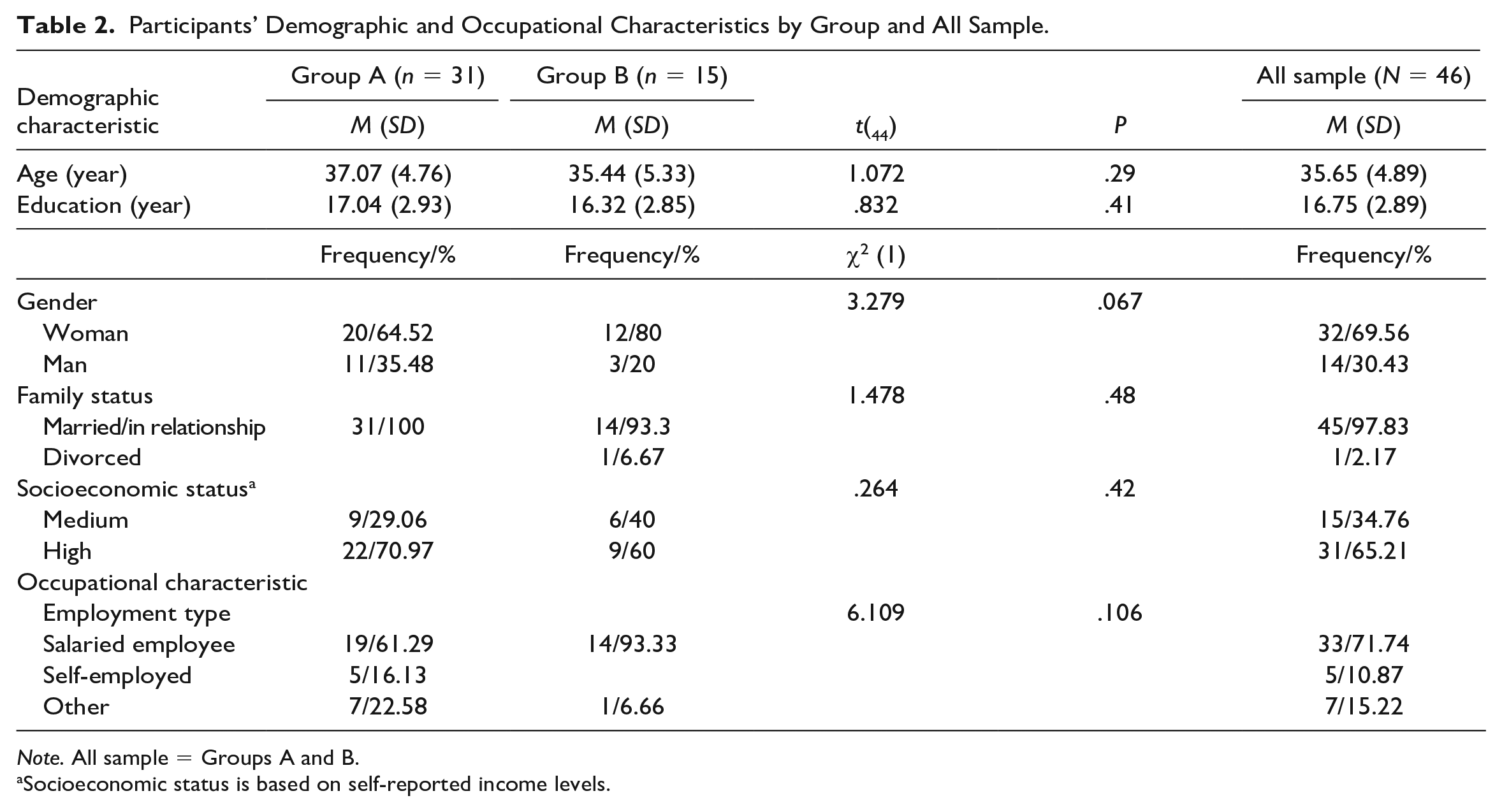
Note. All sample = Groups A and B.
Socioeconomic status is based on self-reported income levels.
As shown in Table 3, t tests for independent variables yielded no significant differences in the dependent variables between groups before the intervention. The t tests for independent variables yielded no significant differences in the dependent variables for the Group B scores during the waiting phase (waiting phase and preintervention measures): BRIEF-A GEC, t(13) = −.21, p = .83; AAQoL total, t(14) = .48, p = .63. However, repeated-measures MANOVA yielded significant differences between preintervention and postintervention measures in dependent variables for Groups A and B: BRIEF-A GEC, F(1, 44) = 12.26, p < .001, ηp2 = .22; AAQoL total, F(1, 44) = 23.36, p < .001, ηp2 = .35; COPM efficacy, F(1, 41) = 59.66, p < .001, ηp2 = .59; COPM satisfaction, F(1, 41) = 60.64, p < .001, ηp2 = .59. Tests of within-subject effects revealed no interaction effect between the groups. The significant differences between the dependent variables’ preintervention and postintervention measures were similar for both groups, and the change occurred following the intervention. Therefore, the two groups (A and B) were treated as one (N = 46) in further analyses.
Differences Between Groups in BRIEF-A, COPM, and AAQOL Scores Preintervention.
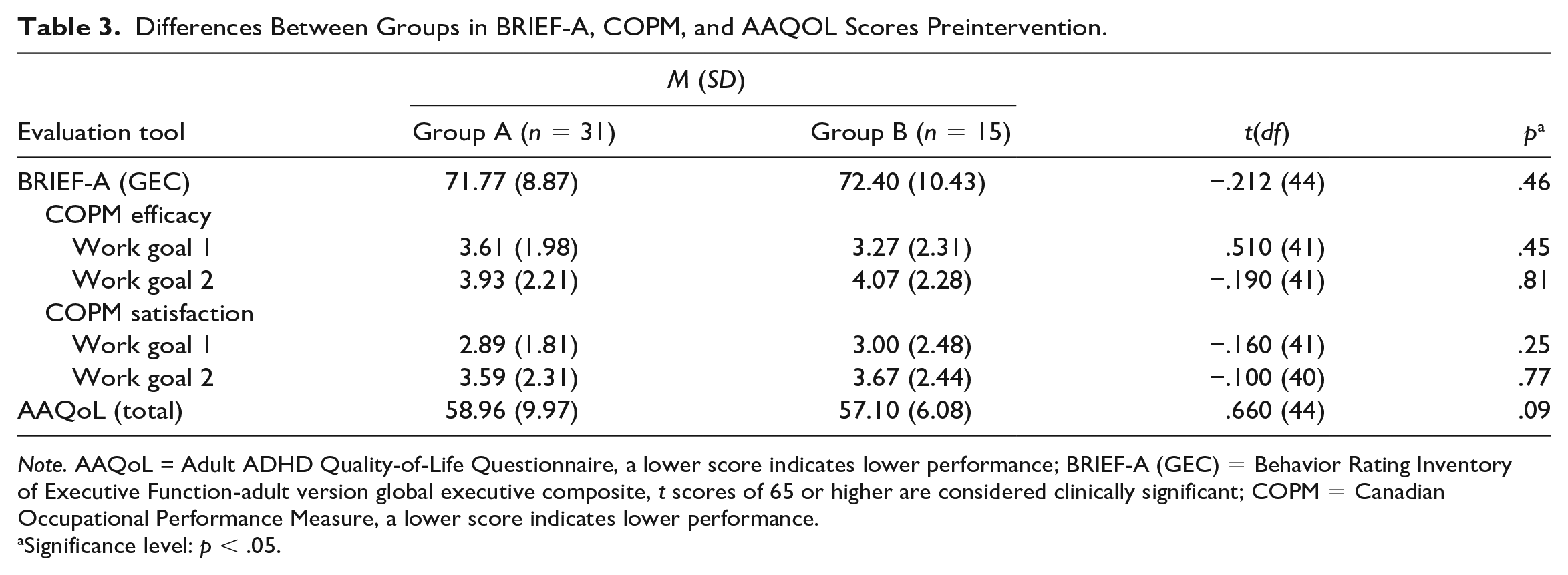
Note. AAQoL = Adult ADHD Quality-of-Life Questionnaire, a lower score indicates lower performance; BRIEF-A (GEC) = Behavior Rating Inventory of Executive Function-adult version global executive composite, t scores of 65 or higher are considered clinically significant; COPM = Canadian Occupational Performance Measure, a lower score indicates lower performance.
Significance level: p < .05.
Descriptive Information: Entire Sample Characteristics
Table 2 shows the demographic and occupational characteristics of the 46 participants. Their ages ranged from 25 to 44 years, and most of them (69.5%) were women. Their mean number of workplaces since age 20 years was 6.38 (SD = 7.24). Of all participants, 17 (36.95%) had professional jobs (e.g., engineers), and 19 (41.30%) worked in therapeutic or educational areas. Preliminary analysis of BADDS (Brown, 2012) scores revealed that most participants (n = 38, 82.61%) were at high risk of ADHD. Using 65 as the t-score cutoff representing clinical significance, most (n = 42, 91.30%) of the sample experienced clinical deficits in at least one BADDS cluster. More specifically, more than half of the sample struggled with clinical deficits in the activation (n = 32, 69.6%), attention (n = 28, 60.9%), effort (n = 34, 73.9%), and memory (n = 24, 52.2%) clusters.
Intervention Effects
Performance Efficacy and Satisfaction With Performance of Self-Selected Work Goals
Preliminary analysis of the participants’ 92 self-selected work goals reflected the diverse activities that, according to the participants, affected their performance at work. Although most (n = 82, 89.13%) goals referred to the work domain, others referred to instrumental activities of daily living (IADLs; n = 9, 9.8%) and leisure (n = 1, 1%) (see Supplemental Table 2).
We examined those goals for performance and satisfaction with performance using the COPM. The repeated-measures MANOVA on the COPM scores indicated significant changes in both variables along the study stages with strong effects, F(4, 39) = 22.45, p < .000, ηp2 = .69, and F(4, 36) = 22.96, p < .000, ηp2 = .72, respectively. Post hoc Bonferroni tests (p < .05) revealed that participants’ performance and satisfaction with performance scores increased significantly following the intervention for the two goal-directed work activities. Table 4 reflects this outcome measure’s ANOVA values for the three study measures. Participants maintained their achievements to the follow-up, and no significant decline occurred across the maintenance phase (p = ns).
Comparison of Outcome Measures: All Sample Over Study Stages.
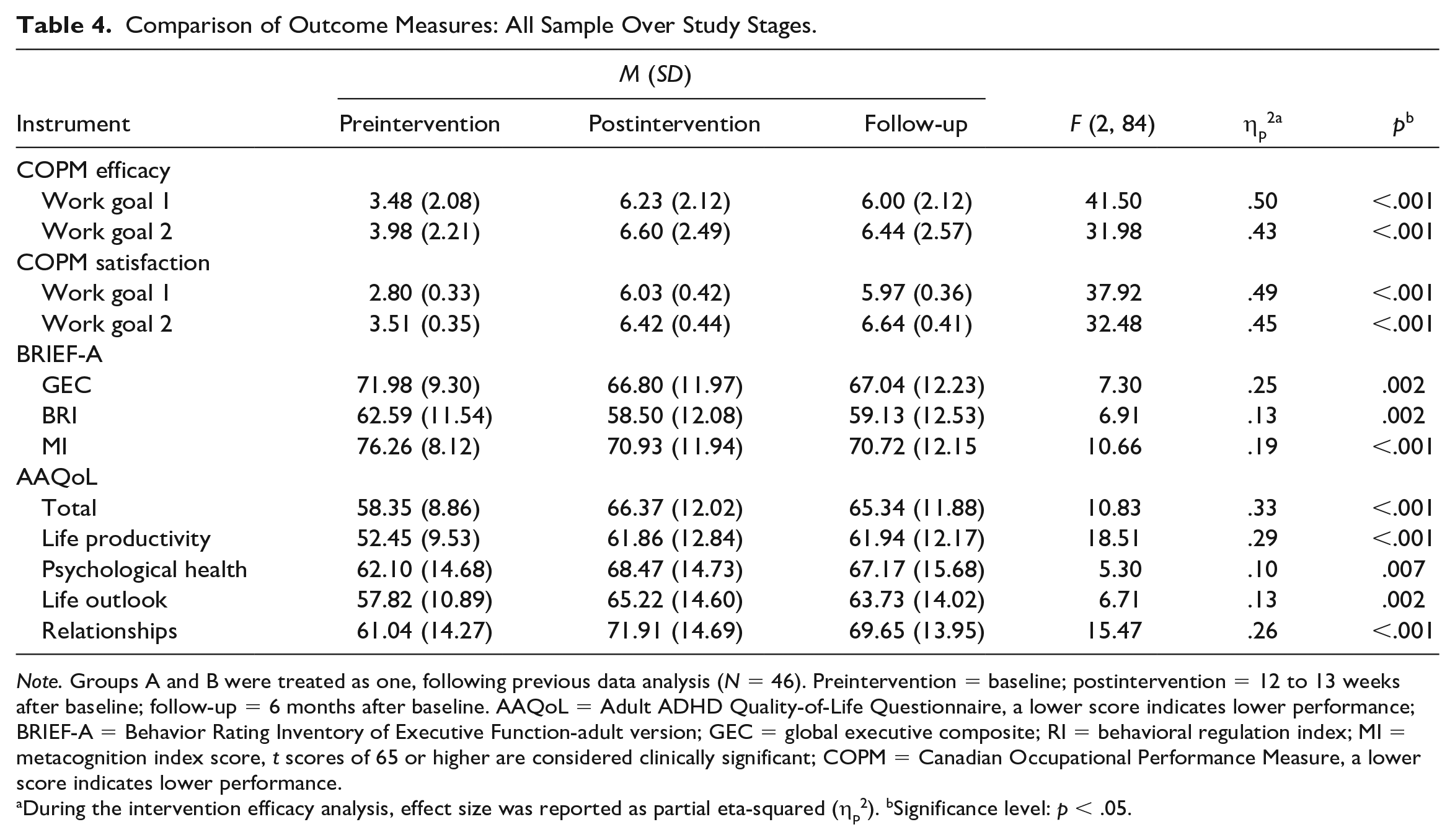
Note. Groups A and B were treated as one, following previous data analysis (N = 46). Preintervention = baseline; postintervention = 12 to 13 weeks after baseline; follow-up = 6 months after baseline. AAQoL = Adult ADHD Quality-of-Life Questionnaire, a lower score indicates lower performance; BRIEF-A = Behavior Rating Inventory of Executive Function-adult version; GEC = global executive composite; RI = behavioral regulation index; MI = metacognition index score, t scores of 65 or higher are considered clinically significant; COPM = Canadian Occupational Performance Measure, a lower score indicates lower performance.
During the intervention efficacy analysis, effect size was reported as partial eta-squared (ηp2). bSignificance level: p < .05.
Executive Functions
Significant changes were found in the BRIEF-A MI and BRI scores across the study stages with moderate effect, F(4, 180) = 5.09, p < .001, ηp2 = .102, and in GEC scores with strong effect, F(2, 44) = 7.30, p < .002, ηp2 = .24. Post hoc Bonferroni tests (p < .05) showed that participants’ BRI, MI, and GEC scores significantly decreased (improved) following the intervention. Table 4 shows that participants maintained the improvements to the follow-up (p = ns). Following the intervention, 15.2% (BRI) and 19.5% (MI) of participants improved their t scores from the abnormal to the normal range.
Quality of Life
Significant differences were found over the study stages in the AAQoL total, F(2, 44) = 10.83, p < .000, ηp2 = .33, and four-subscale scores, F(8, 176) = 5.36, p < .001, ηp2 = .19, with strong effects. Post hoc Bonferroni tests (p < .05) revealed significant increases in total AAQoL and subscale scores following the intervention. As shown in Table 4, improvements were maintained to the follow-up (p = ns).
Discussion
This study evaluates the effects of the Work-MAP intervention on the performance at work of adults with ADHD. The descriptive analysis reinforces the literature regarding the ADHD population’s difficulties with work longevity, as the participants’ average number of workplace transitions was similar to previous evidence (Grinblat & Rosenblum, 2022).
Preintervention and postintervention measures demonstrate significant improvements in participants’ performance efficacy and satisfaction with performance in self-selected work goals, EF, and QoL. Moreover, participants maintained those improvements for 3 months after the intervention. The participants’ performance efficacy and satisfaction with the performance of self-selected work goals, as measured by COPM, indicate that they experienced higher work performance and were more satisfied with it following the Work-MAP intervention. The change in scores has a strong effect. In addition, the change is of more than 2 points, indicating clinically significant improvements (Law et al., 2005).
The most common intervention goals (meet specific work activity deadlines, create, manage, and follow daily/weekly routines) align with the literature indicating reduced work productivity and work-task performance for adults with ADHD (e.g., Joseph et al., 2019). Although most participants’ intervention goals refer to work domain activities, approximately 10% address activities in other occupational domains (IADL, leisure), demonstrating the dynamic interrelatedness and interactions among all occupations. This diversity highlights the need for a holistic viewpoint that considers varied occupational demands and contexts while examining and treating the person’s performance at work.
We observed significant improvements in the participants’ EF (BRIEF-A MI and BRI scores with moderate effect) after implementing Work-MAP. Thereby, this intervention broadens the narrow body of knowledge related to existing evidence-based, metacognitive occupational therapy interventions that enhance the EF of adults with ADHD (Kastner et al., 2022).
Notably, the intervention goals demonstrate the EF deficits that, according to the literature, underlie the poor work performance of adults with ADHD (e.g., Barkley & Murphy, 2010). For example, achieving most intervention goals listed in Supplemental Table 2 requires various EF abilities, such as inhibition, initiation, planning, setting priorities, problem-solving, and organization in space and time.
The participants’ QoL also demonstrated significant improvements following Work-MAP, with strong effects in the AAQoL’s total and four-subscale scores. The pre-post measures of average QoL in this study (total and most subscales) changed at least eight points from the baseline, meaning participants considered the QoL improvement significant (Tanaka et al., 2019). Hence, Work-MAP joins the existing evidence-based occupational therapy interventions that enhance the QoL of adults with ADHD (Kastner et al., 2022). From a broader perspective, the Work-MAP’s success in significantly improving participants’ performance efficacy and satisfaction with self-selected work goals, EF, and QoL aligns with occupational therapy aims, which recognizes QoL and occupational performance improvement as its ultimate goal (AOTA, 2020).
The Work-MAP addresses the needs of adults with ADHD for occupational therapy teleinterventions focusing on work performance (Nobakht et al., 2017). Importantly, occupational therapists rapidly expanded their use of telehealth to deliver services during the COVID-19 pandemic (e.g., Hoel et al., 2021). Because we examined Work-MAP’s efficacy as telehealth during routine (prepandemic) days, the promising findings regarding its effectiveness enable occupational therapists to add a practical intervention to their toolbox for use during either pandemic or routine times.
The study has several limitations. Given the participants’ nonrepresentative demographic and occupational characteristics, the results cannot be generalized to all adults with ADHD. Although the G*Power calculation indicated a sample size of 50, the data analysis was based on 46 participants. Hence, the study is potentially underpowered. Nevertheless, the significant improvements were maintained to the follow-up. Because the outcome measures used were subjective, the possibility of bias may limit the findings’ validity. We assessed the results’ stability over a short period (up to 3 months from the end of the intervention). Further research is needed to assess the Work-MAP intervention using objective, performance-based measures with larger, more representative samples. In addition, future studies should include long-term follow-up (at 6 months and 1 year). Finally, further studies could examine the Work-MAP’s implications for other occupations and daily living areas.
Conclusion
This study provides initial evidence of the Work-MAP’s efficacy as a useful occupational therapy intervention to enhance the performance at work of adults with ADHD. It addresses the need for evidence-based occupational therapy research necessary to determine the effectiveness of work-participation interventions (Smith et al., 2017). The Work-MAP’s telehealth aspects enrich occupational therapists’ toolboxes with an evidence-based telehealth intervention that can be used during routine or pandemic times. We hope occupational therapists who implement Work-MAP will contribute to the better performance of meaningful, goal-directed work activities and QoL of the adults with ADHD population, promoting their health and preventing the development of secondary difficulties.
Supplemental Material
sj-doc-1-otj-10.1177_15394492231159902 – Supplemental material for Work-MAP Telehealth Metacognitive Work-Performance Intervention for Adults With ADHD: Randomized Controlled Trial
Supplemental material, sj-doc-1-otj-10.1177_15394492231159902 for Work-MAP Telehealth Metacognitive Work-Performance Intervention for Adults With ADHD: Randomized Controlled Trial by Nufar Grinblat and Sara Rosenblum in OTJR: Occupational Therapy Journal of Research
Supplemental Material
sj-docx-2-otj-10.1177_15394492231159902 – Supplemental material for Work-MAP Telehealth Metacognitive Work-Performance Intervention for Adults With ADHD: Randomized Controlled Trial
Supplemental material, sj-docx-2-otj-10.1177_15394492231159902 for Work-MAP Telehealth Metacognitive Work-Performance Intervention for Adults With ADHD: Randomized Controlled Trial by Nufar Grinblat and Sara Rosenblum in OTJR: Occupational Therapy Journal of Research
Footnotes
Acknowledgements
We thank all who participated for their cooperation and interest in the study and the National Insurance Institute of Israel for their support. We especially thank all the academic and therapeutic experts whose knowledge and experience helped shape the Work-MAP program (Dr. Yael Fogel, Rami Gertler, Dr. Yael Goldfarb, Dr. Liat Hen-Herbst, Dr. Gili Hoter Ishay, Dr. Maya Huber, Dr. Liron Lamash, Neta Mril, Ruth Shoham, Sara-Orit Torem, Tal Tzameret, and Dr. Naomi Vurembrand) and the people with ADHD for sharing their experiences, insights, and suggestions during the program development.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Insurance Institute of Israel (grant no.: 46006).
Research Ethics and Patient Consent
The research was approved by the Ethics Committee for Human Subject Research of the Faculty of Social Welfare and Health Sciences, University of Haifa (approval no.: 032/17). The procedures followed were in accordance with the institution’s ethical standards and consistent with the revised (2000) Helsinki Declaration.
Trial Registration
This trail has been registered through ClinicalTrails.gov (identifier: NCT05270226).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.