
Abstract
Participating in out-of-home (OOH) activities has been shown to benefit health in older adults. This scoping review aimed to describe the nature of the literature on OOH activities and health in community dwelling older adults, and the operationalization of OOH activity and health-related variables. We followed the Joanna Briggs Institute guidelines. Four databases were searched; studies were selected through title/abstract and full-text screening; and data on study characteristics, sample, and OOH activity and health-related variables were extracted, and summarized descriptively. Sixty articles were identified. There was a considerable focus on leisure and social activities (78% and 75%, respectively) but no predominant health-related outcome was identified. Few studies analyzed sex/gender and/or racial differences (25% and 2%, respectively). Future studies may include systematic reviews focused on health outcomes associated with social and leisure OOH activities; as well as gender-based and/or race-based differences in OOH and health relationships.
Introduction
Population aging is a global phenomenon. Nearly every country in the world faces a rapid expansion of the older adult population, and the aging population is projected to live longer than previous generations (United Nations, 2019). A significant issue facing clinicians, policy makers, and researchers is how best to foster health and well-being across an increasingly longer lifespan, and how to support older adults wishing to age in place. Integral to this issue is understanding the role of out-of-home (OOH) activities in the health of older adults.
Longer and more frequent time spent out of home are associated with better physical health, improved cognitive function decreased depression, and reduced mortality rates in community dwelling older adults (Chow et al., 2014; Harada et al., 2016, 2017; Inoue et al., 2006). The concept of being out of home shares similarities with the concept life-space mobility that refers to the spatial area in which a person operates during their daily life activities. Life-space mobility extends from in-home mobility to the ability to move and travel in the individual’s immediate surroundings and to distant locations (Baker et al., 2003). Poor life space mobility in older adults is associated with depression, reduced cognitive functioning, and poor quality of life (De Silva et al., 2019; Polku et al., 2015; Rantakokko et al., 2016). It has been suggested that a larger life-space provides more opportunities to engage with society through access to societal amenities (Polku et al., 2015), which may explain its health-related benefits.
One possible explanation for these benefits may lie in the types of activities performed when leaving the house, and their potential implication on health and well-being. Community dwelling older adults reported that the primary purpose for going out was for exercise, shopping, and social activities (Chow et al., 2014; Davis et al., 2011). It is likely that at least some of the health benefits from being out of the home are related to what people do, rather than the act of going out. There is a growing body of literature that shows positive health outcomes for physical exercise, social and leisure activities in older adults (Brajša-Žganec et al., 2011; Kimura et al., 2017; Rebelo-Marques et al., 2018); however, the specific contribution of OOH activities to health is not well understood. Frühauf et al. (2016) found that outdoor exercise showed greater affective improvements compared to indoor exercise in adults with depression. Hambrook et al. (2020) suggests that community-based physical activities (e.g., in gym or senior center) may have unique health-related benefits, such as enhanced independence and social connectedness.
The question remains as to the types of OOH activities that may benefit specific aspects of health and well-being. This study takes the first step toward shedding light on this question, by identifying and summarizing the empirical literature on the relationship between different types of OOH activities that older adults are engaging in, and health-related outcomes. A fundamental understanding of the potential effects of OOH activities on health and well-being is especially important to the fields of occupational therapy and occupational science as it will inform occupation-based treatments that could benefit older adults. This knowledge gap was noted by participants attending the American Occupational Therapy Foundation (AOTF) Planning Grant Collective (PGC) in 2019 focused on advancing research to support aging in place (Rodakowski et al., 2021).
Consequently, we undertook a scoping review to describe the empirical literature on the relationship between participation in OOH activities and health outcomes in community dwelling older adults. The two core concepts of this review, “OOH activities” and “health” were operationalized broadly, to capture the full breadth of the literature. OOH activities were operationalized as activities that required the individual to leave their home, even if performing an activity in close proximity to the home (e.g., gardening in home garden). To operationalize health, we used the World Health Organization’s (2021) definition of health as not just the absence of disease, but rather complete physical, mental and social well-being. We used health and health-related domains described in the International Classification of Functioning, Disability and Health (World Health Organization, 2001), and included concepts related to body function and structures (e.g., physical, emotional, cognitive functions); well-being, daily function, social engagement, and so on.
This scoping review aimed to assist in developing a research question for a systematic review, by identifying specific OOH activities and health-related variables that are consistently studied. Consistent with the purpose of this scoping review, we did not summarize or synthesize the finding on the effectiveness of participation in specific OOH activities on health. The research question was: What OOH activity and health-related concepts are examined in the literature that explored the relationship of OOH activities with health in older adults living in the community? The specific aims were to (a) describe the nature of the literature that examines the relationship between OOH activities and health-related outcomes (i.e., study design, time and location, sample characteristics); (b) describe and classify the types of OOH activities examined in relation to health outcomes; and (c) describe and classify the types of health-related outcomes used as dependent variables.
Method
We conducted this scoping review in accordance with the Joanna Briggs Institute (JBI) scoping review methodology (Peters et al., 2020) and the PRISMA Extension for Scoping Reviews (PRISMA-ScR; Tricco et al., 2018). Scoping reviews are the process of mapping the existing literature on a topic area (Levac et al., 2010), and are conducted to explore the breadth or depth of the literature, map and summarize research evidence, identify knowledge gaps in the literature, and inform future research (Tricco et al., 2016). As in the current study, scoping reviews are particularly appropriate when the literature is complex and/or heterogeneous (Peters et al., 2020). A research protocol was developed a-priori, and included the research question, aims, eligibility criteria, search strategy, and screening procedures, as outlined below.
Eligibility Criteria
We developed eligibility criteria to identify quantitative studies that presented an analysis of the relationship between at least one OOH activity and at least one health-related outcome in community-dwelling older adults. The criteria are outlined in Table 1. As per the JBI scoping review methodology, the “concepts” in this review are OOH activities and health-related outcomes. A paper describing an activity that can be performed both in and out of home (e.g., gardening, volunteering, exercising), was included only if explicitly describing the activity as being performed OOH. The “participants” are older adults; and the “context” is the community. The “evidence sources” were limited to quantitative studies published in English in peer-reviewed journals. To ensure the most up to date scientific literature were identified, we limited our search to articles published in the previous 10 years. We excluded intervention studies because we were interested in OOH activity that were available and utilized by older adults in their real-world environments and daily lives rather than contrived activity tied to an experimental context.
Operational Definitions of Eligibility Criteria.
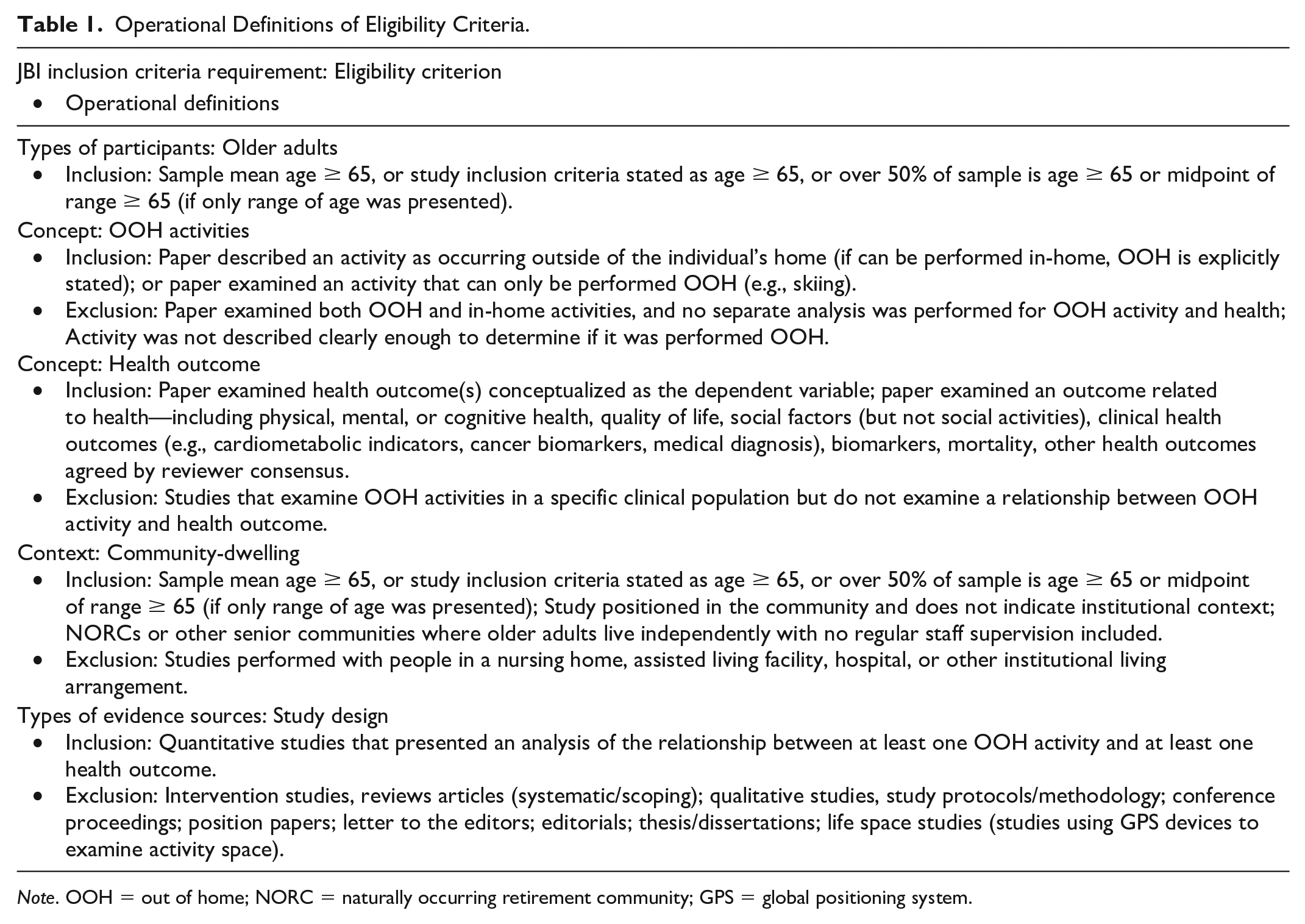
Note. OOH = out of home; NORC = naturally occurring retirement community; GPS = global positioning system.
Search Strategy
We collaborated with a medical librarian to develop and execute the search strategy across four databases (PubMed, Web of Science, CINAHL, and Embase). Prior to commencing the review, the research team conducted preliminary searches to develop a list of search terms that best fit the research purpose and that were commonly used in each database. The search terms and Boolean operators were as follows: ([health OR social isolation OR loneliness OR quality of life OR physical functional performance] AND [activities of daily living OR activity patterns OR activity engagement OR daily living OR activities OR social activity OR leisure activity OR social participation OR hobbies OR recreation] AND [older adult OR elderly OR aged OR senior OR pensioner] AND [neighborhood OR community OR communities OR out of home]). The search strategy for each of the four databases is presented in Supplemental Appendix A. Searches were executed between September 26 and October 1, 2019. Covidence, a systematic review management software (Veritas Health Innovation, 2016), was used to deduplicate citations, screen titles and abstracts and full-texts while tracking reasons for exclusion. We used Covidence to produce the study flow diagram (Figure 1), as required by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Moher et al., 2009).
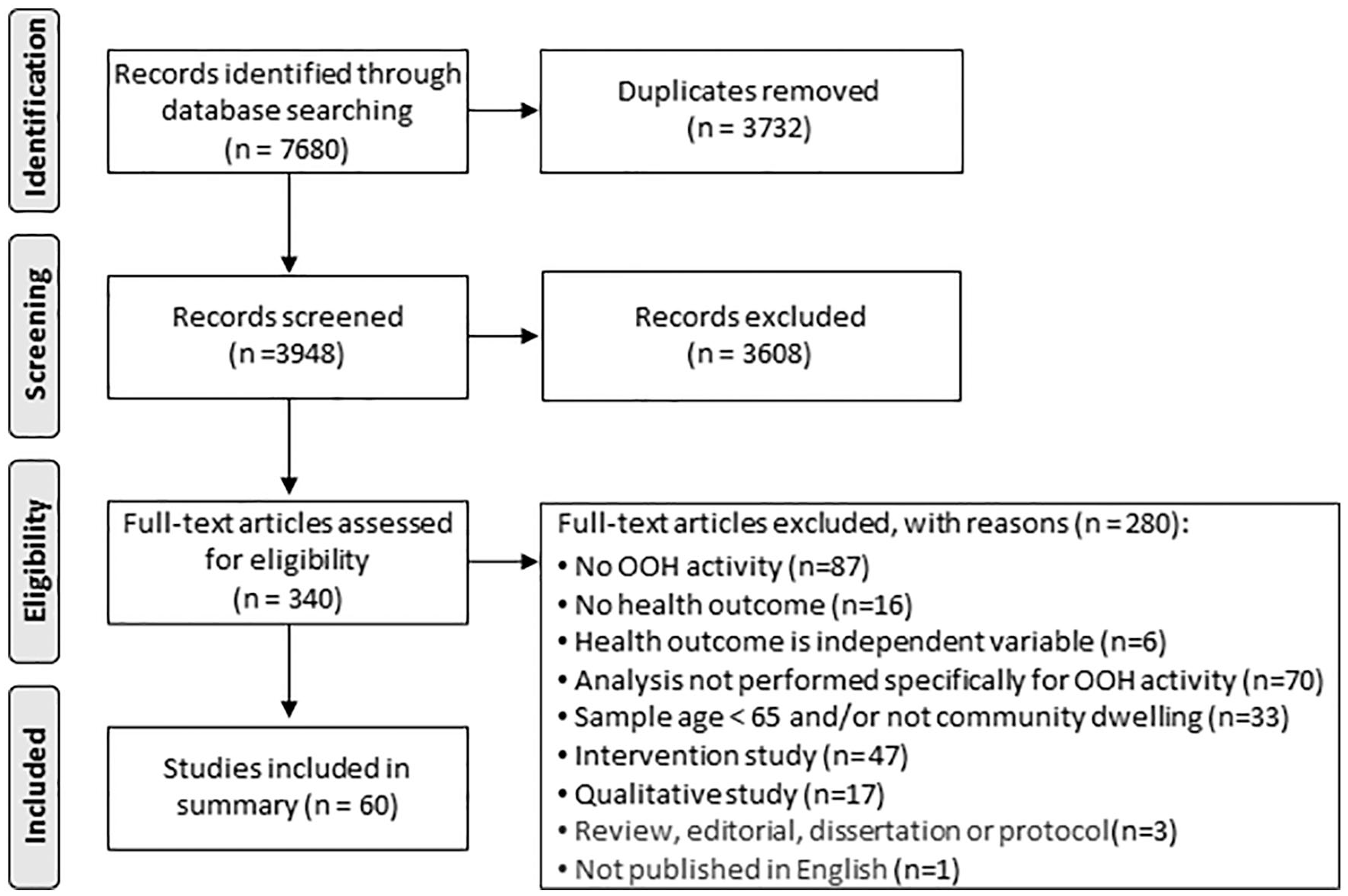
PRISMA diagram.
Source of Evidence Selection
Article screening was performed in two stages, using the eligibility criteria outlined above, defined a priori. We screened titles and abstracts of all records, followed by screening of the full texts of studies deemed as potentially relevant. In both stages, screening was performed independently by two of the five reviewers, and disagreements were resolved through discussion or by a third reviewer (SR or HF).
Data Extraction
A charting form was developed by SR and HF and piloted on five articles by all five authors. Minor changes were made before finalizing the form. Data from all the included studies was extracted by two reviewers and discrepancies were resolved through discussion with a third reviewer (SR or HF). Data points extracted for analysis included: (a) study characteristics (author, year, study location, study design, sample); (b) operationalization of OOH activity variable(s); and (c) operationalization of health-related outcome variable(s).
Data Coding
We classified OOH activity variables into occupational categories defined by the Occupational Therapy Practice Framework (OTPF; American Occupational Therapy Association [AOTA], 2020). We used occupations categories, that describe activities performed OOH: instrumental activities of daily living (IADLs), health management, education, work, play, leisure, and/or social participation (AOTA, 2020). When applicable, OOH activities were classified into sub-categories as defined in the OTPF (e.g., IADLs—driving or shopping; social participation—family participation or friendships). Some OOH activities were classified using more than one category. For example, group cultural activities were classified as both social and leisure activities. If an article included more than one type of activity, we classified the article into multiple categories. The classification of health-related outcomes was made using a list of categories composed by SR for this study, based on outcomes used in the included studies. For both OOH activities and health-related outcomes, SR classified the activities, and HF confirmed all the classifications.
Data Summary
The data were summarized descriptively to describe study and sample characteristics (aim 1); OTPF classifications of OOH activities (aim 2); and classification of health-related outcomes (aim 3).
Results
The search resulted in 7,680 articles obtained. After removing 3,732 duplicates, we screened the titles and abstracts of 3,948 articles, and excluded 3,608 articles. We conducted a full text screening of the remaining 340 articles, resulting in the exclusion of 267 articles for reasons outlined in the PRISMA diagram (Figure 1). We extracted data from the remaining 60 articles. The full list of references for the 60 papers can be found in Supplemental Appendix B.
Study Characteristics
Study characteristics are presented in Table 2. Of the 60 studies included, 24 (40%) were performed in Japan, and an additional seven (12%) were performed in other countries in East Asia. Only two studies were performed in South America, and one in Africa. Our search was limited to studies performed from 2010 onward and identified 23 (38%) studies performed in the 5 years between 2010 and 2014, and 37 (62%) over the next 5 years. Sample sizes of the included studies varied significantly, ranging from 83 (Barcelos-Ferreira et al., 2013) to over 300,000 (Jeong et al., 2019) participants. All but three articles reported the sex or gender distribution of their sample, but only 15 (25%) studies included an analysis of sex or gender differences in regard to the relationship between OOH activities and health. Only 11 (18%) studies reported the race or ethnicity of their samples, and only one (Fitchett et al., 2013) examined racial differences in the relationship between OOH activities and health.
Study Characteristics.
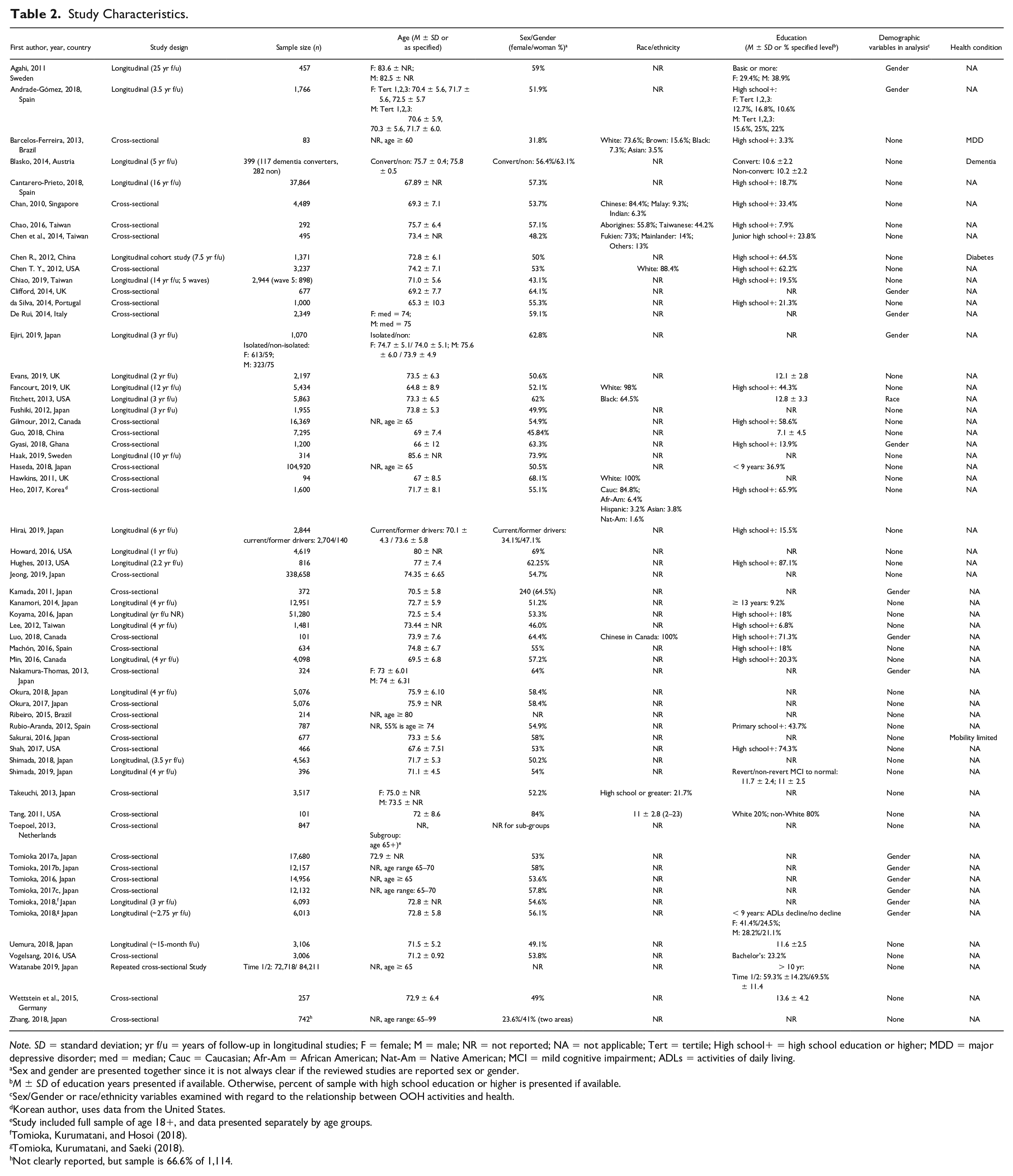
Note. SD = standard deviation; yr f/u = years of follow-up in longitudinal studies; F = female; M = male; NR = not reported; NA = not applicable; Tert = tertile; High school+ = high school education or higher; MDD = major depressive disorder; med = median; Cauc = Caucasian; Afr-Am = African American; Nat-Am = Native American; MCI = mild cognitive impairment; ADLs = activities of daily living.
Sex and gender are presented together since it is not always clear if the reviewed studies are reported sex or gender.
M ± SD of education years presented if available. Otherwise, percent of sample with high school education or higher is presented if available.
Sex/Gender or race/ethnicity variables examined with regard to the relationship between OOH activities and health.
Korean author, uses data from the United States.
Study included full sample of age 18+, and data presented separately by age groups.
Tomioka, Kurumatani, and Hosoi (2018).
Tomioka, Kurumatani, and Saeki (2018).
Not clearly reported, but sample is 66.6% of 1,114.
Out-of-Home Activity Variables
There was substantial variability in the types and number of OOH activities utilized in the included studies. The OOH variables are presented in Table 3, and further detailed in Supplemental Appendix C. Thirteen studies (21.7%) examined the relationship of health to a single OOH activity category, with some only examining a single type of activity such as visiting friends and relatives (Chen et al., 2014); religious services (Fitchett et al., 2013) or driving (Hirai et al., 2019). Most of the studies (n = 47, 78.3%), however, included multiple OOH activities, often within more than one activity category.
OOH-Activity Variables Examined in Included Studies.
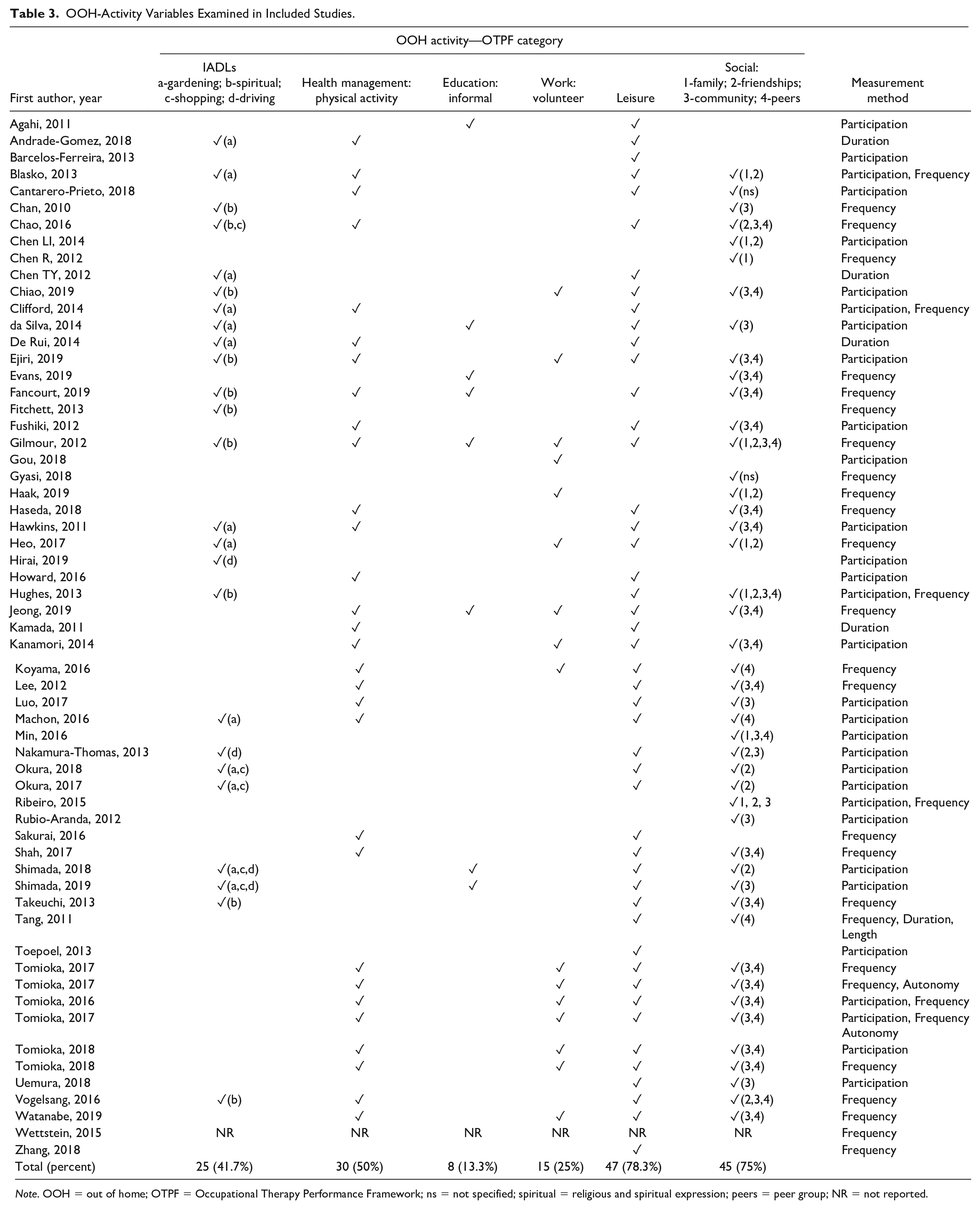
Note. OOH = out of home; OTPF = Occupational Therapy Performance Framework; ns = not specified; spiritual = religious and spiritual expression; peers = peer group; NR = not reported.
The most commonly examined occupational categories were OOH activities related to leisure (n = 47, 78.3%) and social participation (n = 45, 75%). OOH health management activities were assessed in 30 (50%) of the studies, all of which described OOH physical activities. OOH IADLs were examined in 25 (41.6%) of the studies, that included IADLs of gardening (n = 13), religious and spiritual expression (n = 10), shopping (n = 5), and driving (n = 4). Volunteer work and informal education OOH activities were assessed in 15 (25%) and eight (13.3%) studies, respectively. None of the included studies examined OOH activities related to play.
Different studies measured OOH activity in different ways. Thirty-one (51.7%) of the studies assessed whether or not the participants were engaged in the OOH activity currently, or over a defined period of time, and presented the participation in OOH activities as either “yes” or “no.” The same number of studies examined frequency of participation over a given time, but in many of the studies this was dichotomized into two or more categories, such as frequent or infrequent participation (see Supplemental Appendix C). Only five (8.3%) studies examined the duration of participation over a specific period of time, and only two (3.3%) examined autonomy as a characteristic of OOH activities. Eight (13.3%) of the studies used more than one measurement method (e.g., both participation and frequency).
Health-Related Outcomes
There was also considerable variability in the types of health-related outcome used, as presented in Table 4. We identified health-related outcomes related to mental health (n = 16, 26.7%), cognitive function (n = 13, 21.7%), everyday function (e.g., basic or instrumental activities of daily living; n = 10, 16.7%), physical function (n = 9, 15%), specific health conditions (n = 9, 15%), general health status (n = 7, 11.7%), quality of life (n = 7, 11.7%), social function (n = 6, 10%), and mortality (n = 5, 8.3%). There was a wide variability in the standardized measures used to examine health-related outcomes within the same category. For example, five studies used the Center for Epidemiologic Studies Depression Scale (CES-D; Lewinsohn et al., 1997) to measure depression, while four others used the Geriatric Depression Scale (GDS; Yesavage et al., 1983). Most of the studies (n = 49, 81.7%) examined a single health-related outcome, and 11 (18.3%) examined multiple health-related outcomes, ranging from two to five.
Health-Related Outcome Variables Examined in Included Studies.
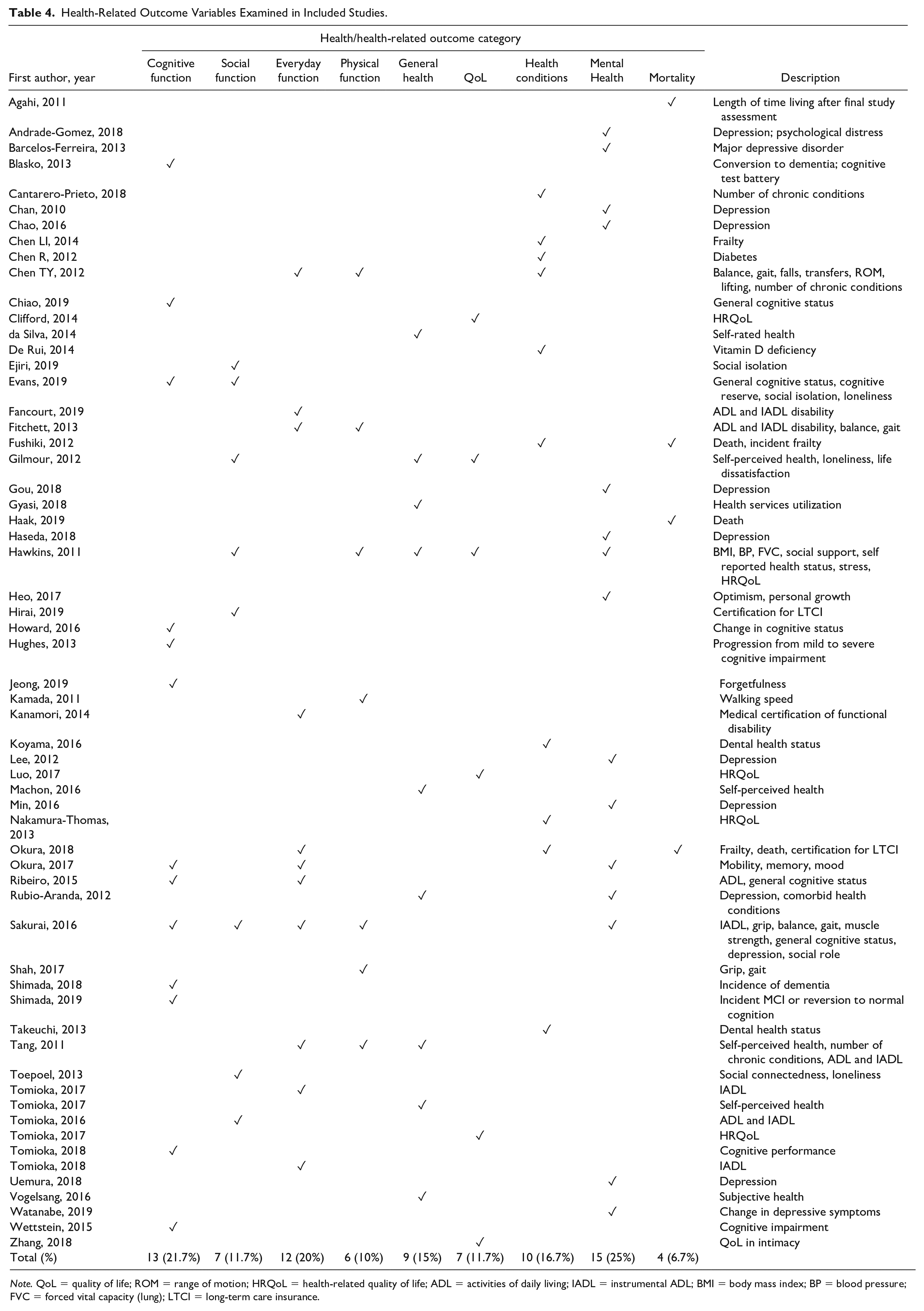
Note. QoL = quality of life; ROM = range of motion; HRQoL = health-related quality of life; ADL = activities of daily living; IADL = instrumental ADL; BMI = body mass index; BP = blood pressure; FVC = forced vital capacity (lung); LTCI = long-term care insurance.
Discussion
This scoping review aimed to describe the nature of the literature that examined the relationship between OOH activities and health-related outcomes in community dwelling older adults; and describe and classify the types of OOH activities and health-related outcomes examined in this literature. The results suggest an increase in research on the topic with 62% of articles included in this review being published in the previous 5 years. The increase in scholarship on the topic and the geographic distribution of studies suggests a global interest in better understanding the relationship between OOH activities and health. This interest may be inspired by the concept of healthy aging, presented and defined by the World Health Organization as “the process of developing and maintaining the functional ability that enables well-being in older age” (Beard et al., 2016, p. 28). Although not limited to OOH activities, the World Health Organization suggests that older adults’ engagement in valued activities within their communities is a core factor in healthy aging (Beard et al., 2016).
Nature of the Literature
Japanese scholars produced the highest number of studies of any country represented in the dataset. A dynamic driving this finding is the creation of several large cohort studies in various community settings across the country that have been heavily analyzed with attention to social activities and health. The analysis of large aging-based data sets in China and Japan is in turn shaped by research questions regarding social capital, and within that focus, social participation, which includes OOH activities (Liu et al., 2019). The preponderance of Asian research in our findings does, however, raise a question regarding the generalizability of these studies to older adult populations in the western world, especially in the absence of cross-cultural comparative studies examining differences in OOH-activity. An anecdotal example of such cultural differences is that while the main reason for leaving the house among older adults in Taiwan was for physical exercise in local parks (Chow et al., 2014), in Great Britain the main purpose was shopping (Davis et al., 2011). Further research is warranted to examine cultural differences in relation to OOH activities and health-related outcomes.
Another noteworthy finding is the limited analysis of sex and gender-based and/or race and ethnicity-based differences in OOH and health relationships. As gender and race have been found to influence occupational choices and meaning of occupations (Beagan & Saunders, 2005; Galvaan, 2012) future studies should include sub analyses to examine how gender and race influence the selection and meaning of OOH activities and how those relate to health.
Types of Out-of-Home Activities
Our results suggest the literature on OOH activities and health primarily focused on OOH social and leisure activities (75% and 78% of studies, respectively), as well as physical exercise (50% of the studies). There is abundance of research to support the association of these types of activities with health-related outcomes (Brajša-Žganec et al., 2011; Christie et al., 2017; Kelly et al., 2017; Moritani, 2015), as well as a growing body of research that shows that being out of home supports health in aging (Chow et al., 2014; Harada et al., 2016, 2017). However, studies that examine the added value of engaging in such activities OOH are sparse. With the growing research and clinical interest in non-pharmacological interventions that promote positive health outcomes through lifestyle behaviors (Kelly et al., 2017), more research is needed to understand the mechanisms through which OOH activities affect health-related outcomes.
The vast majority of the studies identified in the review examined OOH activities in terms of frequency of participation (as a dichotomous or continues measure). We found a striking paucity of literature that examined autonomy, and no research on other aspects of occupational experience, defined as the subjective qualities that individuals associate with their occupations, such as personal meaning, pleasure, choice, and balance (Atler et al., 2016; Hammell, 2009). Occupational scientists have argued that the occupational experience related to an activity is fundamental to well-being, rather the participation per se (Atler et al., 2016; Hammell, 2009). We identified a need for research on OOH activities and health in aging to be expanded to examine concepts related to occupational experience.
Health-Related Outcomes
We found a wide range of health-related outcomes that were examined in this literature, with no one predominant health-related outcome being explored. However, mental health outcomes, mainly depressive symptoms, were most frequently queried. This is not surprising given the known contribution of depression to adverse outcomes in later life (Fiske et al., 2009). The heterogeneity of the health-related variables, as well as their diverse operationalization may be a reflection of the multifaceted and inter-related nature of health in aging, and the lack of consensus in regards to its definition and measurement (Sholl, 2021).
Study Limitations
This study has several limitations. First, we limited this review to quantitative studies and excluded qualitative studies that may have contributed understandings regarding how and why some OOH activities could be health promoting. We also excluded articles written in languages other than English, which shaped the study data set, analysis, and interpretation of results.
Conclusions and Implications and Future Research
The results of this review suggest the relationship between OOH activity and health is complex, spanning a wide range of circumstances, activities, and health-related outcomes. A future systematic review may focus on health-related outcomes of the more prevalent conceptualization of OOH activities identified in the literature, namely frequency of performance of social and/or leisure activities. Our findings do not inform a clear direction for the focus of a systematic review with regard to specific health outcomes.
There was also a lack of assessment of OOH activities beyond frequency of activity participation. Future research could shed light on the most therapeutic and transformative OOH activities, as well as why, how, for whom (which populations), and under what conditions they contribute to positive outcomes. Moreover, including additional attention to the role of social determinants of health such as gender bias and racial discrimination would not only improve inferences about OOH activities and health, but it would enhance the role of occupational therapy in addressing population health (Braveman, 2016).
Supplemental Material
sj-docx-1-otj-10.1177_15394492211023192 – Supplemental material for Out-of-Home Activities and Health in Older Adults: A Scoping Review
Supplemental material, sj-docx-1-otj-10.1177_15394492211023192 for Out-of-Home Activities and Health in Older Adults: A Scoping Review by Shlomit Rotenberg, Heather Fritz, Tracy Chippendale, Catherine Lysack and Malcolm Cutchin in OTJR: Occupation, Participation and Health
Supplemental Material
sj-docx-2-otj-10.1177_15394492211023192 – Supplemental material for Out-of-Home Activities and Health in Older Adults: A Scoping Review
Supplemental material, sj-docx-2-otj-10.1177_15394492211023192 for Out-of-Home Activities and Health in Older Adults: A Scoping Review by Shlomit Rotenberg, Heather Fritz, Tracy Chippendale, Catherine Lysack and Malcolm Cutchin in OTJR: Occupation, Participation and Health
Supplemental Material
sj-docx-3-otj-10.1177_15394492211023192 – Supplemental material for Out-of-Home Activities and Health in Older Adults: A Scoping Review
Supplemental material, sj-docx-3-otj-10.1177_15394492211023192 for Out-of-Home Activities and Health in Older Adults: A Scoping Review by Shlomit Rotenberg, Heather Fritz, Tracy Chippendale, Catherine Lysack and Malcolm Cutchin in OTJR: Occupation, Participation and Health
Footnotes
Acknowledgements
The authors wish to thank the American Occupational Therapy Foundation for funding the PGC in 2019, where this research team came together, and Wendy Wu for her assistance in conducting the review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
This is a scoping review study that did not involve human or other participants, and therefor did not require ethics approval.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.