
Abstract
Abdominal aortic aneurysms (AAA) are most commonly observed in elderly male patients and are particularly rare in children. Among the pediatric population, they are usually diagnosed in the context of connective tissue disorders, genetic mutations, or vasculitis. The same is true of visceral arteries aneurysms. This case report describes the staged management of an 11-year-old patient presenting PIK3CA mutation and a 5.8 cm infrarenal AAA associated with bilateral common iliac arteries and multiple visceral aneurysms, the largest observed in the superior mesenteric artery (SMA = 3.2 cm). After careful evaluation, decision was made to first approach the most life-threatening lesion (the infrarenal AAA due to the large diameter) and the remaining aneurysms in secondary procedures, with special attention to the SMA aneurysm. The patient underwent a staged repair, with the first phase consisting of an aortobi-iliac graft with the distal anastomosis made at the left common iliac artery and right external iliac artery. The right hypogastric artery was ligated. The second procedure consisted of SMA aneurysm repair with a plication technique, as 7 branches were visualized coming off the aneurysm sac. Postoperative pathology analysis of the aortic and SMA aneurysms sac revealed vasculitis with a mixed inflammatory pattern and a COL3A1 gene heterozygote variant. He is currently in his 18th month after the last surgical intervention, receiving immunomodulatory therapy, with a planned follow-up by the interdisciplinary team to monitor the medications’ side effects and the diameter of the remaining visceral aneurysms.
Keywords
Introduction
Abdominal aortic aneurysms (AAA) are defined as an increment of 50% in the normal diameter of the vessel, which usually translates into a measurement above 3 centimeters (cm). Prior studies report the prevalence of this disease as being higher in men (3.9%–7.2%) than in women (1%–1.3%), 1 more specifically among white male patients older than 65 years who have ever smoked.1,2 Abdominal aortic aneurysm is described as the 10th cause of death in this demographic group, 3 and a study of risk factors analysis estimates the prevalence of the disease of being around 1 million people in the United States. 4
Abdominal aortic aneurysms are particularly rare in children, and are usually diagnosed in this age group in the context of connective tissue disorders, genetic mutations, infections (mycotic aneurysms), or vasculitis. 5 The same is observed for visceral arteries aneurysms. This case report describes our experience with the management of an 11-year-old patient presenting PIK3CA heterozygote mutation and a 5.8 cm infrarenal AAA associated with bilateral common iliac arteries and multiple visceral aneurysms (celiac trunk, superior mesenteric, hepatic, left gastric, and splenic arteries) who was also diagnosed with vasculitis with a mixed inflammatory pattern and a COL3A1 gene heterozygote variant.
Case Report Presentation
A 9-year-old asymptomatic male patient with an autism spectrum disorder was being followed by the Pediatric and Genetics teams due to a PIK3CA heterozygote mutation, which can be associated with overgrowth syndrome. The most significant findings observed during his evaluation were a lower limb discrepancy (right > left around 1.5 cm) and an intraosseous hemangioma in the left foot. No abdominal masses, pain, change in appetite or weight loss were observed in multiple evaluations. As part of this disease workup, the patient was initially submitted to an abdominal ultrasound that showed a 1.2 cm hepatic artery aneurysm, but no other aneurysms were identified at the time. Decision was made to follow-up this finding with an abdominal magnetic resonance imaging (MRI) within 1 or 2 years. The legal guardian of the patient has given informed consent for participation in this case report. This manuscript is included under the IRB protocol #22-1594.
Preoperative Evaluation
Twenty months after the abdominal ultrasound, an MRI was performed and detected multiple abdominal fusiform aneurysms: infrarenal abdominal aortic aneurysm - IRAAA (diameter: 6.1 cm), right and left common iliac arteries (2.5 cm and 2.1 cm, respectively), superior mesenteric artery (SMA = 3.2 cm), multiple dilations in distal SMA branches (up to .9 cm), hepatic artery (1.3 cm), celiac artery (1.3 cm), and left gastric artery (1.1 cm) aneurysms. At this point, the patient was referred to Vascular Surgery. A chest, abdomen, and pelvis computerized tomography angiography (CTA) was then performed for surgical planning (Figure 1(A)) and normal thoracic aorta was observed as well as normal supra-aortic trunks. Centerline measurements of the aneurysms are listed as follow: infrarenal aorta (diameter: 5.8 cm), right and left common iliac arteries (2.7 cm and 2 cm respectively), SMA (3.2 cm), multiple dilations in distal SMA branches (up to 0.9 cm), right hepatic artery (1.6 cm), celiac artery (1.4 cm), left gastric artery (1.3 cm), and splenic artery (1.2 cm). The right hepatic artery branched off the SMA and the left hepatic artery branched off the celiac artery. At least 7 vessels branched off directly from the SMA aneurysm sac, therefore the surgical planning carefully considered this anatomical detail to avoid compromising bowel viability. (A) 3D reconstruction image of the preoperative CTA showing the 5.8 cm IRAAA, the bilateral common iliac aneurysms, the 3.2 cm SMA aneurysm (white asterisk), and the right hepatic artery aneurysm. (B) Intraoperative anterior view of the IRAAA associated with aneurysms in both common iliac arteries. (C) Anterior view, after repair using a Dacron 12 × 6.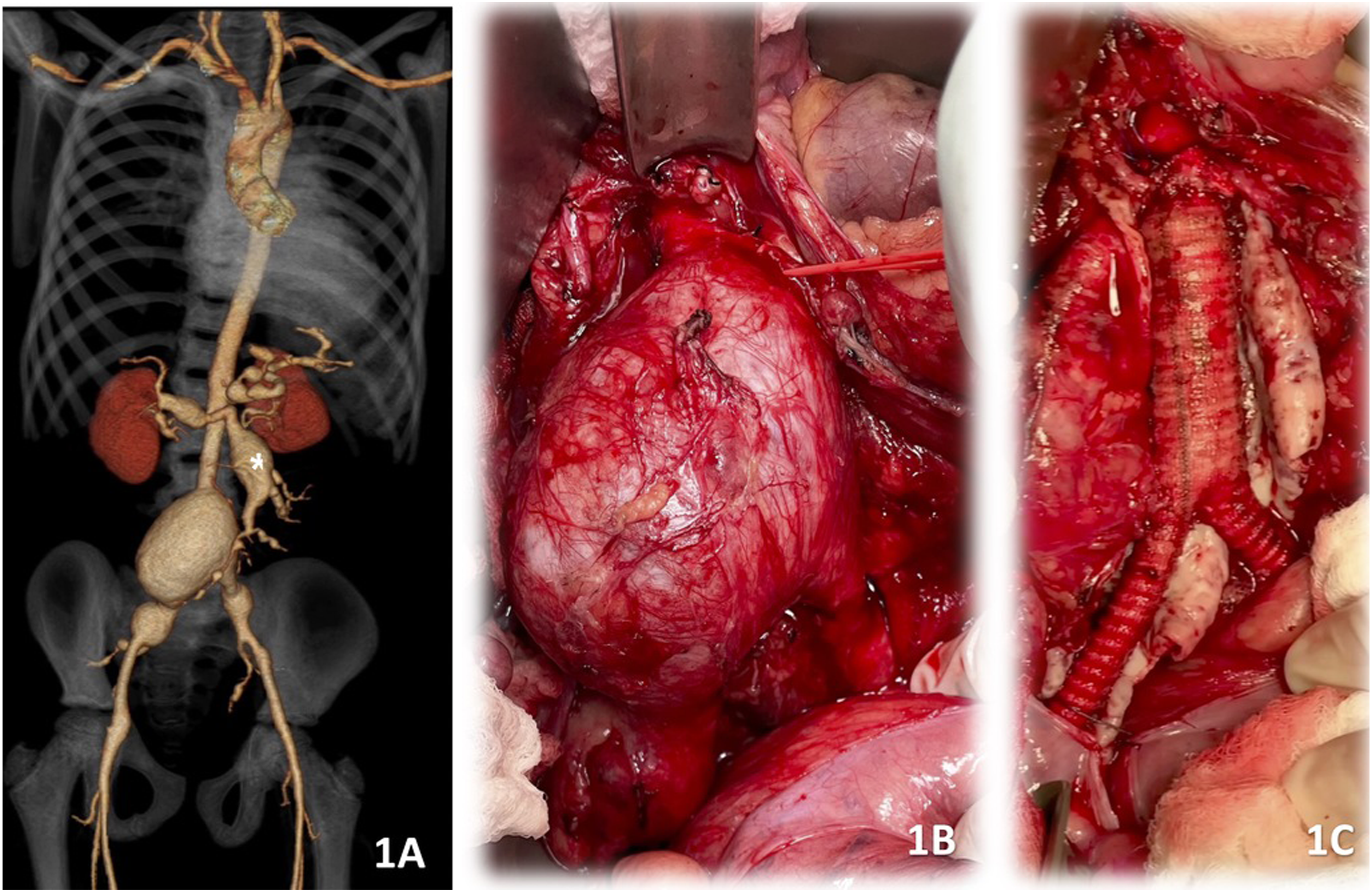
Treatment – Stage 1: AAA and Iliac Arteries Aneurysm Repair
After careful evaluation, decision was made to first approach the most life-threatening lesion (the infrarenal AAA due to the large diameter) and the remaining aneurysms in secondary procedures, with special attention to the 3.2 cm SMA aneurysm.
By the age of 11, the patient underwent transabdominal open surgical repair with a bifurcated Dacron graft (12 × 6 millimeters). The proximal anastomosis was made in an end-to-end fashion in the infrarenal aorta (Figure 1(B) and (C)); the distal anastomosis were also made in an end-to-end fashion between the limbs of the Dacron graft and right external iliac artery and left common iliac artery. The right hypogastric artery was ligated because the right common iliac artery aneurysm compromised the iliac bifurcation. Specimens of the aortic aneurysm wall were sent to pathology and genetics analysis. The patient had an uneventful hospital course and was discharged home on the seventh postoperative day.
The histopathological evaluation reported diminished elastic laminae, intimal and medial fibrosis, and calcification compatible with aortitis with mixed inflammatory pattern. The findings were not befitting of Takayasu aortitis, and the lack of involvement of the aortic arch and subclavian arteries further argues against this diagnosis. These features were indicative of a systemic inflammatory/rheumatologic condition and the evaluation suggested the patient would benefit from immunomodulatory therapy. The genetic analysis identified a COL3A1 gene heterozygote variant of uncertain significance.
Treatment – Stage 2: SMA Aneurysm Repair
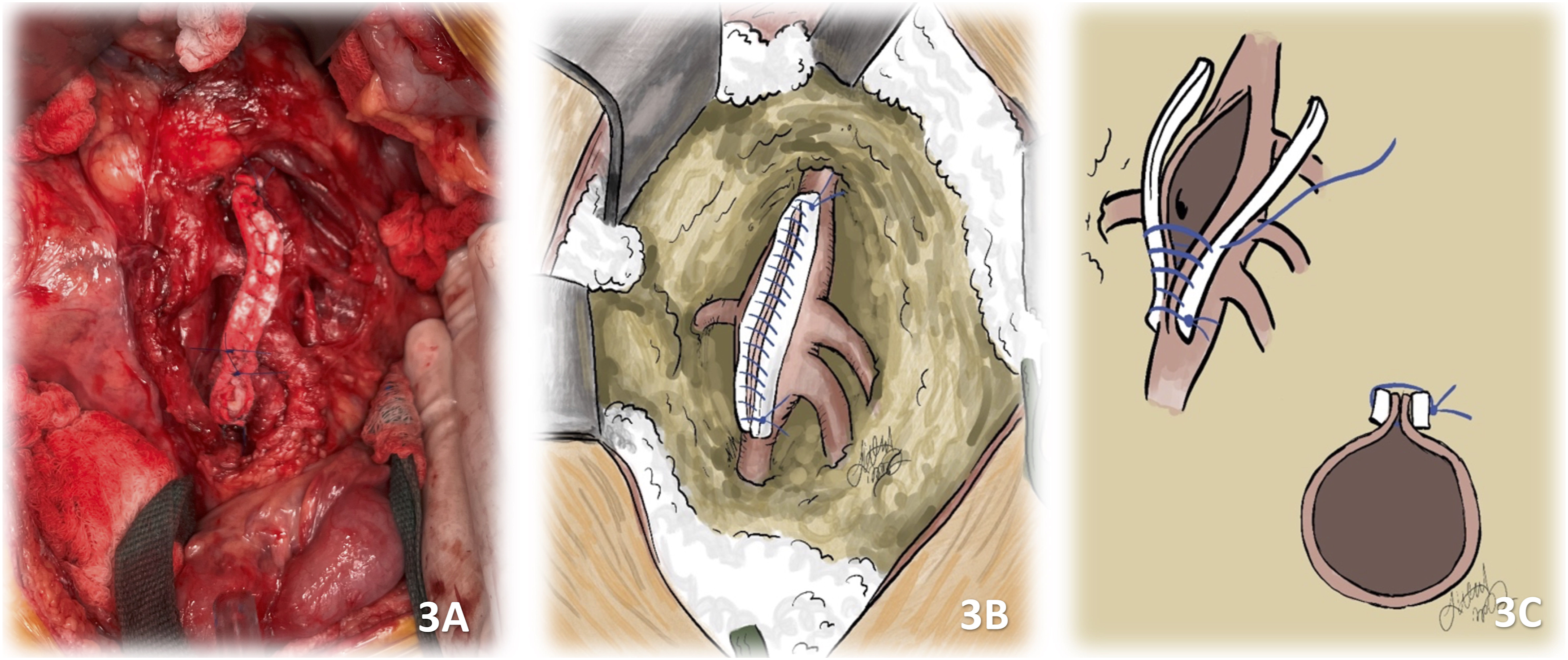
A 3-month follow-up CTA showed unchanged visceral aneurysms. Five months after the first procedure, the patient was fully recovered. The most concerning lesion at this time was the SMA aneurysm due to the size (3.2 cm) and complexity (multiple vessels branching off the aneurysm sac). Due to the risk of bowel ischemia, it was decided to repair the aneurysm with a plication technique. At operation, which was performed through transabdominal approach, 7 branches were visualized coming off the aneurysm sac, The aneurysm was plicated using PTFE felt strips and continuous prolene suture (Figure 2(A) to (D); 3(A) to (C)). All the branches were preserved. No bowel ischemia was visualized intraoperatively. Fragments of the SMA aneurysm wall were sent to pathology analysis and the findings were very similar to the ones described for the IRAAA (vasculitis with mixed inflammatory pattern). The patient had an uneventful hospital course and was discharged home on the sixth postoperative day. (A and B): Anterior intraoperative view of the SMA aneurysm sac. (C and D): Anterior view of the SMA aneurysm sac prepared for the plication procedure. Illustrations 2 B and D by Dr. Jacob Claude Wood. (A and B): SMA aneurysm sac after the plication. (C): schematic illustration of the plication technique. Illustrations 3 B and C by Dr. Jacob Claude Wood.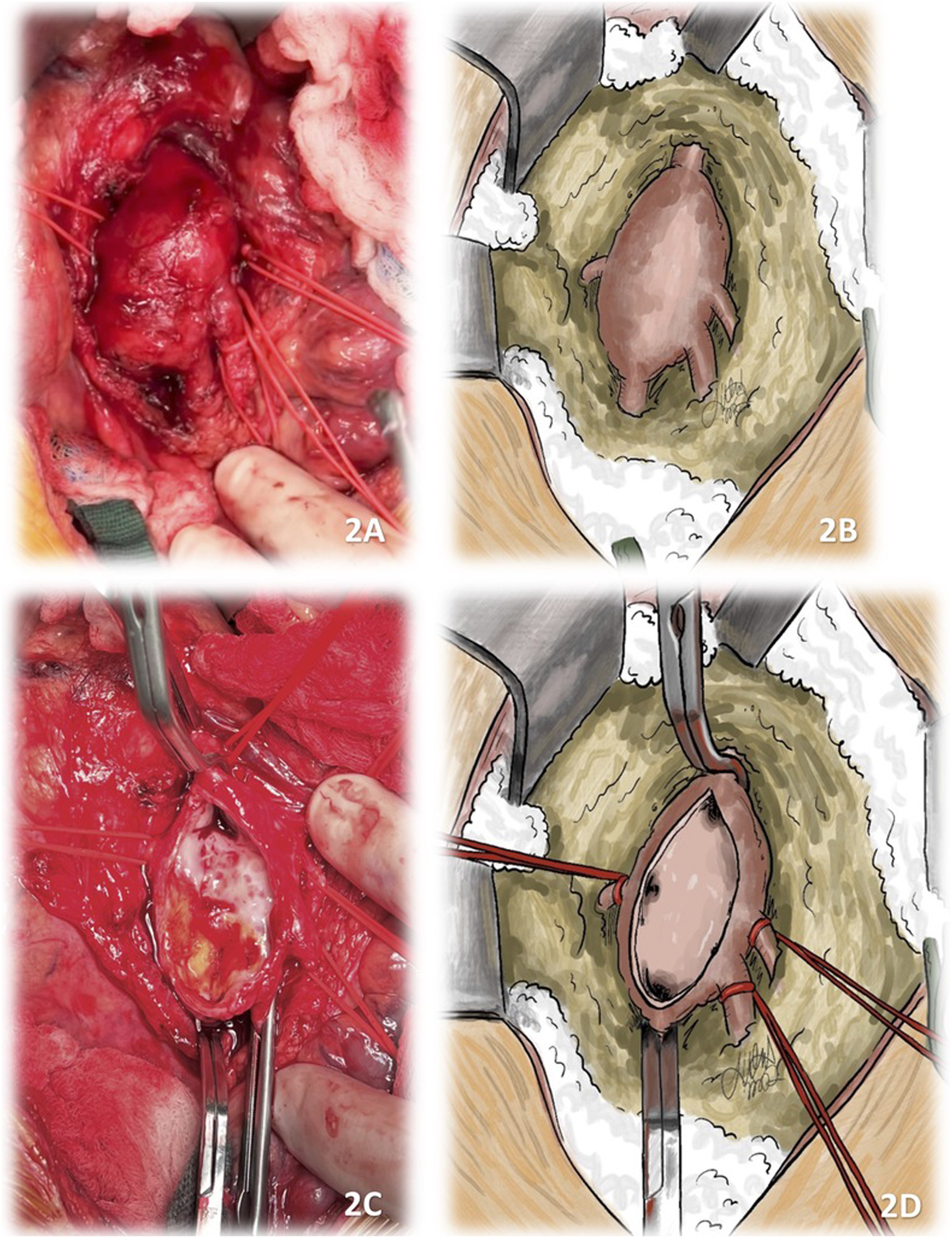
Follow-up
At 1-month follow-up, the patient was without complaints with normal return of bowel function and activities. A new MRI was performed, showing no complications related to both repairs performed. The Pediatric Rheumatology team initiated the patient on immunomodulatory therapy with Methotrexate and Infliximab 2 months after the second operation, and he is currently on these medications.
One year after the procedure, the patient underwent an MRA (Magnetic Resonance Angiography), which revealed that both repairs were intact and a new 8 mm left renal artery aneurysm. He is currently in his 18th month after the last surgical intervention, receiving immunomodulatory therapy. As a long-term plan, he will continue to be followed by the interdisciplinary team to monitor the medications side effects and the diameter of the remaining visceral aneurysms (annual chest, abdomen and pelvis MRA or CTA).
Discussion
We report a rare case of vasculitis and COL3A1 gene heterozygote variant in a child with PIK3CA mutation presenting with multiple arterial aneurysms, sparing the thoracic aorta and the supra-aortic trunks. Arterial aneurysms are extremely rare in the pediatric population, especially presenting as a multi-vessel disease as in the patient described in this report.
The PIK3CA heterozygote mutation diagnosed in this case is usually related to a spectrum of symptoms called PROS (PIK3CA-related overgrowth spectrum), which include disorders such as Klippel-Trenaunay syndrome, CLOVES syndrome, isolated lymphatic malformation, hemi-hyperplasia, among many others. 6 The most common vascular findings usually compromise the venous, lymphatic, and capillary systems, 7 but spare the arterial vessels. The lower limbs length discrepancy and the intraosseous hemangioma diagnosed in this patient can be associated with this mutation. However, we believe this is the first patient with a PIK3CA mutation that presents with such extensive arterial disease described in the literature. It is not possible to clearly determine the contribution of this genetic component in this severe clinical presentation, especially in the context of the inflammatory disease and collagen gene variant diagnosed postoperatively.
Considering vasculitis in the pediatric population, 8 a large variety of disorders such as Behcet’s disease, 9 Takayasu disease, 10 polyarteritis nodosa, 11 and Kawasaki disease 12 are associated with arterial aneurysms compromising the aorta, supra-aortic trunks, pulmonary, coronary, and visceral arteries. The final pathology analysis of both aortic and SMA aneurysm fragments described a vasculitis of mixed inflammatory pattern. At first, the multidisciplinary team considered Takayasu disease as the main hypothesis, but the lack of a granulomatous component or the typical adventitial fibrosis seen in this condition counted against this diagnosis. Involvement of the thoracic aorta or supra-aortic trunks is also expected in this disease but was not observed in this case. For the management of arterial aneurysms, immunomodulatory therapy, surgical repair, or a combination of these 2 approaches are indicated for vasculitis cases, depending on the size of the lesions and extension of the disease.13,14
Inherited conditions such as Ehlers-Danlos, Marfan syndrome, 15 Loeys-Dietz syndrome, 16 and tuberous sclerosis 17 are also described in literature in association with arterial aneurysms, many of them particularly involving the aorta. For these cases, treatment is based on surgical repair alone, and close follow-up with imaging is required for life. In these pathologies, the preferred approach is open surgical repair over endovascular procedures, as the progressive degeneration of the aorta provoked by these diseases could compromise the proximal and distal sealing zones of endovascular devices. Endovascular procedures are also not good options for children because with growth, stents or endoprosthesis could be dislodged and lose the proximal and distal seals. In this patient, a COL3A1 gene heterozygote variant of uncertain significance was identified, which is one of the genes that can be implicated in the Ehlers-Danlos syndrome vascular type. Therefore, the presence of this variant associated with the described vasculitis and the PIK3CA syndrome could have jointly contributed to the aggressive manifestation of the vascular degeneration seen in this patient.
Conclusion
The management of complex aortic and visceral aneurysms in the pediatric population is challenging but possible with a multidisciplinary team. Staged open-repair strategy for extensive disease compromising multiple arteries demonstrated to be successful and durable, especially in those cases with challenging anatomy. Immunomodulator therapy can be extremely important for disease control, particularly in patients with vasculitis. Life-long follow-up with imaging allows the healthcare team to observe further degeneration of the vessels and anticipate complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article:
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board information
Name of the IRB Chairperson by the time of the approval of the Research protocol #22-1594: Penny Gordon-Larsen, Vice Chancellor for Research at UNC Chapel Hill