
Abstract
Background
Masson’s tumor, commonly referred to as intravascular papillary endothelial hyperplasia (IPEH), is an uncommon growth of endothelial cells within a vessel wall that is frequently assumed to indicate an abnormal resolution of thrombosis. IPEH is most typically found in the extremities however it is rare for IPEH to appear as a neck tumor. The issue with IPEH is that it could clinically, radiologically, and pathologically imitate some malignant neoplasms such as angiosarcomas creating a diagnostic challenge.
Case Report
We describe a 21-year-old male patient who presented with right anterolateral neck swelling for 12 months. Ultrasound revealed a 9.0 × 8.0 cm well-defined echogenic hyper-vascular lesion. The contrast computed tomography (CT) scan of the neck revealed an oval, well-defined subcutaneous mass, measuring 9 × 4.5 cm, situated over and separable from the right sternocleidomastoid muscle with no significant enhancement in the post-contract study. T1-weighted and T2-weighted MRI revealed a 10 × 9 × 7 cm well-defined subcutaneous lobulated lesion superficial to the sternocleidomastoid expanding upward to the Rt. side of the cheek and below to the suprasternal region, eliciting an intermediate signal in T1 and a heterogenous bright signal (mostly fluid) in T2 with low signal foci within the mass. The decision had been reached to entirely excise the lesion surgically with safety margins for histological evaluation. Histological examination indicated thrombosed variable-sized ectatic vascular spaces with papillary formations related to the thrombus, covered with a single layer of flat endothelium, and no features suggestive of malignancy. There was no recurrence at 18 months follow-up post-surgery.
Conclusion
Masson's tumor is a benign intravascular disease with an unclear origin and no confirmed inheritance pattern. Presentation of Masson’s tumor as a neck mass is incredibly uncommon. Masson's tumor lacks a distinct or distinguishing clinical and radiological appearance. Histopathologic examination is the sole definitive way for diagnosing the disease and the only tool for distinguishing it from angiosarcoma. Surgical excision is the best treatment for IPEH. Recurrence is extremely rare.
Keywords
Introduction
Masson's tumor, also known as intravascular papillary endothelial hyperplasia (IPEH), is a benign intravascular pathology that can resemble other benign tumors and even some types of malignancies. 1
French pathologist Pierre Masson first defined it as “vegetant intravascular hemangioendothelioma” in 1923. 2
IPEH is most typically found in skin and soft tissue, most commonly in the head, neck, and limbs. It accounts for about 2% of skin and subcutaneous tissue vascular tumors. IPEH has only been seen rarely in the oral cavity. 3
Although it is benign, IPEH may substantially influence health based on where it arises in the body. 4
IPEH often manifests in adulthood, however, there is no clear age, racial, or gender preference. 5 A low number of instances in children have been documented.
IPEH can emerge as a primary vascular lesion or as an addition to an existing vascular malformation. 6
Overall, the IPEH pathogenesis is unknown. According to several authors, it is either thrombosis with subsequent reactive endothelial growth or reactive endothelial proliferation with secondary thrombosis. 3 It could be an uncommon variety of thrombus organization, and in some situations, it could be related to prior trauma. 7
Despite it has a great prognosis, diagnosis can be difficult yet necessary because it might be clinically similar to other benign and malignant diseases that necessitate extra procedures, such as angiosarcoma and Kaposi's sarcoma. 7
Case Description
We describe the case of a 21-year-old male Egyptian patient, not known to have any medical illnesses of note, who was admitted to the vascular department of Al-Zahraa University Hospital in Cairo, Egypt, through a vascular outpatient clinic. He presented to the clinic with a 1-year history of painless, nontraumatic slowly growing, right anterolateral neck swelling.
The patient denied having dyspnea, dysphonia, dysphagia, weight loss, anorexia, or night sweats.
On physical examination, he had an 8 × 8 cm right anterolateral neck mass that was soft to firm, non-compressible, non-pulsatile, mobile, non-tender, and free of overlaying skin changes. The draining cervical lymph node examination came out negative, and the rest of the physical exams were normal. The swelling was initially assumed to be a subcutaneous lipoma (Figure 1). Masson tumor presented as Rt. Diffuse neck mass.
A complete blood count and peripheral blood smear revealed no abnormalities; erythrocyte sedimentation rate and viral serologies were both negative.
The palpable mass was visualized on sonography as a well-defined echogenic lesion measuring 9 × 8 cm, restricted to, and distended the lumen of a superficial vein. The existence of venous blood flowing proximal and distal to the swelling was established using pulsed Doppler scanning. However, a color Doppler examination of the mass indicated that it was hyper-vascular, with both venous and arterial flow patterns.
CT angiography revealed a well-defined rounded Rt. Cervical subcutaneous mass lesion of soft tissue density measuring 9 × 4.5 cm extending upwards to the angle of the mandible, showing multiple foci of dense calcifications with no significant enhancement in the post-contract study, the mass is seen separable from the underlying Rt. Sternocleidomastoid muscle. There were no feeding vessels seen emerging from the carotid or subclavian vessels.
T1-weighted and T2-weighted magnetic resonance imaging (MRI) was conducted, showing a ×109 × 7 cm well-defined subcutaneous lobulated lesion superficial to the sternocleidomastoid extending superiorly to the Rt. Side of the check and inferiorly to the suprasternal region, eliciting intermediate signal in T1, and inhomogenous bright signal (mostly fluid) in T2 with low signal foci within the mass (Figure 2 left and right Axial T2 sequence showing 10 × 9 × 7 cm Rt (Left). Neck mass elicits an inhomogeneous bright signal with low signal foci within the mass. Coronal T2 sequence showing the craniocaudal extension of the noted hyperintense mass (right).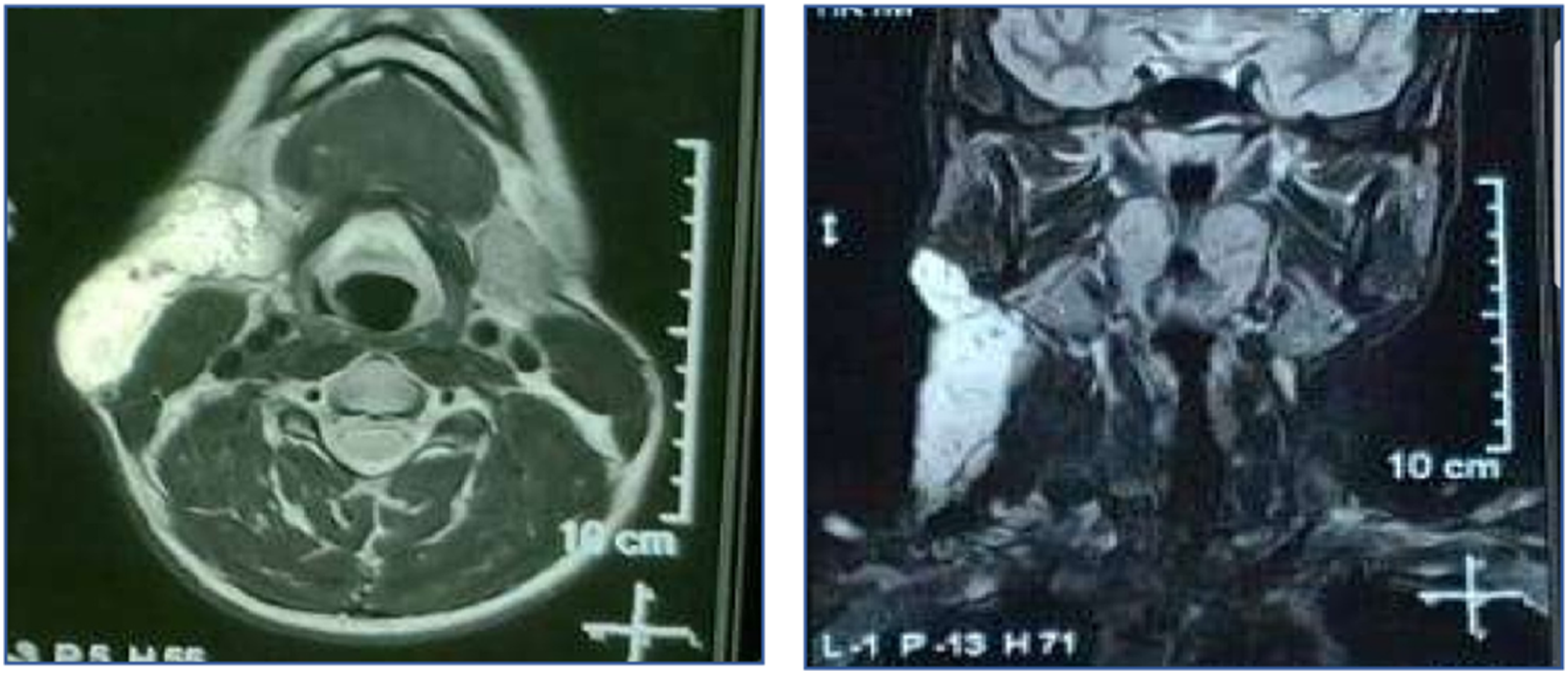
The diagnosis was not definitive at this point therefore an ultrasound-guided biopsy was planned to evaluate for possible malignancy, but the results were ambiguous.
The decision had been made to excise the lesion completely with safety margins for histological assessment. An incision was made across the medial side of the SCM, cutting through fat and the platysma muscle separating deeply to reach the carotid sheath. The sheath vessels are exposed after carefully incising the sheath. The internal and external carotid arteries, as well as the internal jugular veins, are all controlled. Intraoperatively, the mass was composed of diffuse anastomosing channels of dilated vessels occupying the subcutaneous space of the anterolateral aspect of the neck, superficial to the sternomastoid muscle, extending to the submandibular space and not infiltrating the skin or the deep muscles. The mass was excised completely anterior to the SCM. The incision was extended posteriorly to allow excision of the lesion in the posterior triangle of the neck. Bleeding was adequately controlled (Figure 3). The blood loss was about 300 mL. A drainage tube was fitted following surgery. The patient recovered quickly without complications. Post-complete excision of the Rt. cervical Masson tumor (left). After 18 months of follow-up, there was no recurrence of the Masson tumor (right).
The histopathology report came consistent with Masson’s tumor which presented as a thrombosed variable-sized anastomosing dilated vascular spaces with intravascular papillary formations related to the thrombus. The papillae had a fibrous pedicle covered by flattened endothelium. The lesion showed no infiltrative behavior or cellular features indicating malignancy.
The patient was followed at 6, 12, and 18 months with no evidence of recurrence (Figure 3 (right)).
Discussion
Pierre Masson originally described IPEH in 1923. He introduced the term “vegetant intravascular hemangioendothelioma” to describe an intravascular papillary growth in the lumen of an inflammatory hemorrhoidal plexus in a 68-year-old man. 8
The term “intravascular papillary endothelial hyperplasia” (IPEH), coined by Clearkin and Enzinger 9 in 1976, is now the most often used because it emphasizes the disease's non-neoplastic nature.
IPEH pathophysiology is unknown, however, it appears to be complex. Although 30% of instances have been linked to triggers such as trauma or vascular anomalies (eg, hemangiomas, vascular malformations), the majority of cases have unexplained origins. 10 There is no established inheritance pattern.
Based on the etiology, IPEH is divided into three forms, the primary form, also known as the “pure” form, occurs in a dilated vessel, the most prevalent form, also known as the “mixed” form; occurs in conjunction with a thrombus in a context of an already present lesion, such as a hemangioma, or arteriovenous malformation, and the third form which is a relatively rare extravascular variant that appears in hematomas following trauma. 11
IPEH appearing as a neck mass is unusual, with nearly ten cases recorded in the literature. 12
IPEH is minimally heterogeneous in MRI T1-weighted imaging due to the blood vessels and thrombi within the tumor, and postcontrast T1-weighted scans show heterogeneous enhancement that could indicate a malignant lesion as low-grade angiosarcoma. 13
Because there are no clinical or imaging-specific features sufficient to direct the diagnosis of Masson’s tumor and to distinguish it from malignant tumors such as angiosarcomas, a histological description of the lesion is required as the therapy approach and prognosis are different. 14
The only conclusive diagnostic tool of IPEH is histopathologic evaluation. IPEH has fully intravascular papillae comprised of connective tissue and coated by endothelial cells, with organizing thrombi. The lesion does not destroy the vascular wall or invade surrounding tissues. Furthermore, IPEH lacks tissue necrosis and malignant cytological characteristic. 15
Immunohistochemistry is not advisable in the diagnosis of IPEH since it fails to distinguish it from angiosarcoma. 16
Total surgical excision with safety margins to avoid recurrence is the best treatment for IPEH. Cases of IPEH recurrence have been recorded in cases of inadequate surgical excision. 17
Because IPEH has prominent vascularization, intraoperative neurophysiologic monitoring and control of bleeding are essential. 13 Eventually, We could list the clinical significance of this study as follow: (i) IPEH appearing as a neck mass is unusual, with nearly ten cases recorded in the literature. (ii) Because there are no clinical or imaging-specific features sufficient to direct the diagnosis of Masson’s tumor and to distinguish it from malignant tumors such as angiosarcomas. (iii) Preoperative procedures like sclerotherapy to decrease intraoperative bleeding is limited because the preoperative diagnosis is not conclusive. CT findings sometimes did not reveal any feeding vessel to embolize. (iv) There should be more work to definitely diagnose the disease preoperatively and to try other methods of treatment like radiotherapy.
Conclusion
Masson's tumor is a benign intravascular pathology with an unidentified etiology and no known genetic pattern. Masson's tumor presenting as a neck lump is extremely rare. Masson's tumor does not have a unique clinical appearance. The diagnosis is frequently ambiguous on MRI. Histopathologic examination is the only definite approach to diagnosing the disease and the only way to differentiate it from angiosarcoma. The most effective treatment for IPEH is surgical excision. Recurrence is extremely uncommon.
According to ICH- good clinical practice, Declaration of Helsinki, and World Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent and consent for publication including the patient’s data and photographs were obtained from the patient.
Organization Guidelines
The Research ethics committee of the Faculty of Medicine for Girls, Cairo, Al-Azhar University (FMG-IRB) approved this study.