
Abstract
Background
The chimney technique, fenestrated or branched endovascular aortic repair are endovascular options in patients with a juxtarenal, suprarenal or type IV thoraco-abdominal aneurysm. The chimney technique has specific advantages and disadvantages. A retrospective single center study was performed to describe the results.
Patients and methods
All consecutive patients in whom the chimney technique was used between 1th January 2011 and 31th December 2020 were included. We excluded patients who needed a revision of an existing EVAR and patients with a para-anastomotic aneurysm. Outcomes were reported in accordance with the reporting standards.
Results
38 Patients were included in the study, a total of 59 chimney grafts were deployed. At a median follow-up duration of 26.6 months, there were 9 patients with occlusion of the chimney graft. In 1 patient an iliac renal bypass was performed. In the other patients the renal function stabilized and no further therapy was necessary. All chimneys in the mesenteric arteries remained patent. Gutter endoleak was seen in 5 patients, 3 patients were successfully treated and in the other 2 patients the gutter endoleak disappeared spontaneously.
Conclusions
Conclusions should be drawn carefully as this is a retrospective non-comparative study. Results from 38 patients treated with the chimney technique are presented. Chimney graft occlusion rate was 15.3% at the end of follow-up. However, the majority (77.8%) of the occluded stents were self-expandable stents, stressing the importance of selecting the right devices.
Introduction
Juxtarenal and suprarenal aneurysms account for circa 15% of abdominal aortic aneurysms (AAA). Since standard endovascular aortic repair (EVAR) is not possible in these patients, other endovascular options for these patients have been explored: main endovascular options for these patients include fenestrated or branched EVAR (f/bEVAR) or the use of the chimney technique (ChEVAR).
Major disadvantage of f/bEVAR is that the manufacturing time is 4-8 weeks. Off-the-shelf branched devices exist, but not all patients meet the inclusion criteria for these stentgrafts. 1 When compared to standard EVAR, f/bEVAR is more complicated and time consuming.
The chimney technique can be used as an alternative when the procedure has to be performed urgently. Major drawbacks are the risk of gutter endoleak (EL), chimney stent occlusion and the need for upper extremity access. Gutter endoleak is the loss of aortic wall apposition between the endograft or chimney graft and can lead to type 1A EL and aneurysm rupture. 2 Chimney stent occlusion can occur due to compression of the stentgrafts, which are not designed to be deployed next to each other. Chimney stent occlusion can have major consequences such as (temporal) dialysis or acute mesenterial ischemia. Upper extremity access can also risk ischemic cerebrovascular event (CVA). A recent study reported a 4.6% incidence of CVA after complex EVAR.3,4
In this study we describe our experience with the chimney technique in a community hospital.
Patients and Methods
Patients
This study included all consecutive patients with a juxtarenal, suprarenal abdominal aortic aneurysm or type 4 thoracoabdominal aneurysm treated with the chimney technique between 1th January 2011 and 31th December 2020. Until recently f/bEVAR was not possible in our clinic. Patients in whom regular EVAR was not possible, were therefore considered for ChEVAR. Patients with an aneurysm neck <10 mm were considered for ChEVAR. For this study, we excluded patients with para-anastomotic aneurysms and patients who needed a revision of an existing EVAR. For the chimney technique to be performed, a proximal landing zone of >10 mm of healthy suprarenal or supramesenteric segment of aorta was necessary. Another prerequisite was adequate brachial access. We aimed at a minimal overlap between the endograft and adjacent chimney of approximately 20 mm.
A juxtarenal abdominal aneurysm was defined as an aneurysm extending up to, but not involving, the renal arteries, while a suprarenal abdominal aneurysm was defined as an aneurysm that extends up to the superior mesenteric artery.5,6 The Crawford classification was used to classify thoracoabdominal aneurysms. 7 The study was approved by the local ethics committee (University of Witten/Herdecke Nr. S-190/2022).
Procedure
All procedures were performed by vascular surgeons. Open and percutaneous access of the common femoral artery was used. Access for the chimney grafts included open and percutaneous approach of the left brachial or subclavian artery, depending on the number of chimney grafts. When 1 chimney graft was planned, percutaneous or open access of the brachial artery was used. When 2 or 3 chimney grafts were planned, the left infraclavicular subclavian artery was used. We always used open access of the subclavian artery. After access was gained, 5.000 IE heparin were administered intravenously. The subclavian or brachial access was then used to cannulate the target vessels. After cannulation with a 5F catheter, a 90 cm sheath was positioned in the target vessel and, after secure positioning, the chimney graft was introduced over a Rosen wire (Infiniti Medical, Malibu, Calif, USA). During the study period 4 stentgrafts were used: Viabahn (W.L. Gore and Assoc Inc, Flagstaff, AZ, USA), Advanta V12 (Atrium Medical/Maquet Cardiovascular, Hudson, USA), Lifestream (Bard Peripheral Vascular, Tempe, AZ, USA) and the BeGraft (Bentley Innomed GmbH, Hechingen, Germany). One mm oversizing was used for the chimney grafts, the diameter ranged from 5 to 7 mm. During the study period, no additional internal stenting of the chimney grafts was performed. We aimed to cover a minimum of 10 mm of the target vessel to achieve sufficient seal.
During the study period different aortic stentgrafts were used; in most patients the Endurant stent graft system (Medtronic, Santa Rosa, Calif, USA) was used. We aimed at a proximal oversizing of 20 to 30%. The main body was introduced through the femoral access and the main body and chimney grafts were deployed simultaneously. We aimed to position the chimney graft 2 to 3 mm above the proximal covered stent of the aortic endograft. Completion angiography was performed to confirm the patency of all stents and to exclude endoleak. A selective angiography of the target vessel was performed before the sheath was removed.
Surveillance
A CT-angiography was performed before discharge, at 6 months, 12 months and annually thereafter. Patients with chronic kidney failure a CT-angiography was performed by a catheter placed in the aorta.
All patients received acetylsalicylic acid 100 mg daily and clopidogrel 75 mg daily for 6 weeks; thereafter patients were advised to take acetylsalicyl acid. Patients with preoperative oral vitamin K antagonists or novel oral anticoagulants were advised to take clopidogrel 75 mg daily for 6 weeks.
Outcomes
In accordance with consensus reporting standards, technical success was defined successful introduction and deployment of the device in the absence of surgical conversion or mortality, EL1 or EL3 or graft obstruction. 6 Clinical success was defined as successful deployment of the endograft without mortality, EL1 or EL3, graft infection or thrombosis, aneurysm expansion (diameter ≥5 mm or volume ≥5%), aneurysm rupture or conversion to open surgery. 6 Only patients without gutter EL or thrombosis of the chimney graft were considered as clinical successful in this study. Aneurysm related mortality was defined as death within 30 days of the procedure, death due to a primary or secondary procedure related to ChEVAR or death to aneurysm rupture. 6 Gutter endoleak was defined as a loss of continuous aortic wall apposition between the endograft or chimney grafts, or both and the aortic wall, with or without the persistence of blood flow in the aortic aneurysm (2). EL1A was defined as an incomplete seal at the proximal aortic attachment site. 5 Significant thrombus or calcifications was defined as circumferential thrombus or calcifications >50%. 8
For each patient the location of the sealing zone was determined. Zone 8 is located around the renal arteries, zone 7 around the superior mesenteric artery and zone 6 around the coeliac artery. 9
Acute kidney injury (AKI) was defined as an increase in serum creatinine ≥.3 mg/dl within 48 hours or an increase in serum creatinine ≥1.5 times baseline within the prior 7 days or urine volume <.5 mL/kg/h for 6 hours. 10 Chronic kidney was defined as an estimated glomular filtration rate (eGFR) < 60 mL/min, since urine tests with albumin to creatinine ratio were not available.
Statistics
Continuous variables were expressed as mean and standard deviation. Categorical data was expressed as number and percentages. A P-value <.05 was considered statistical significant. Kaplan-Meier charts were used to depict freedom from chimney graft occlusion and survival. Statistical analyses were performed using SPSS version 28 (SPSS Inc, Chicago).
Results
Patient and Aneurysm Characteristics
Demographics.
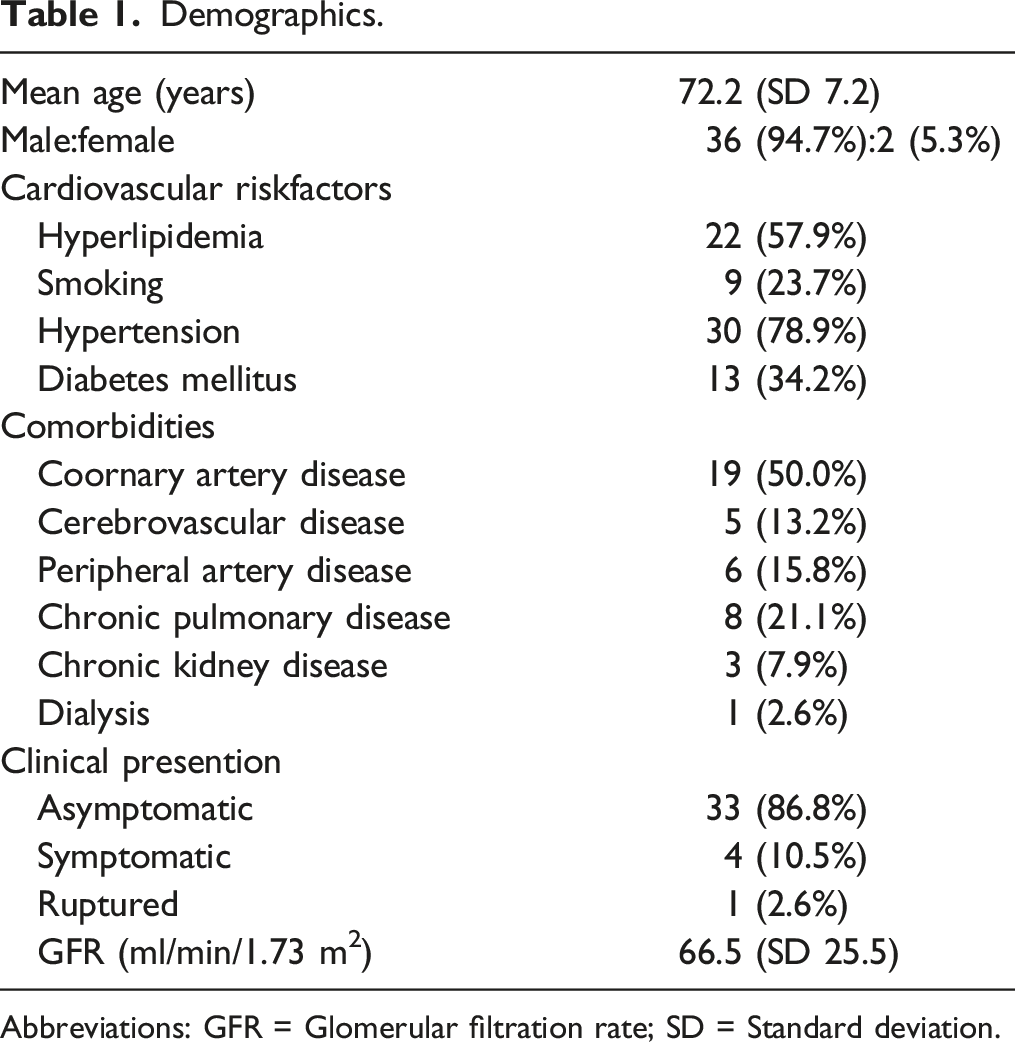
Abbreviations: GFR = Glomerular filtration rate; SD = Standard deviation.
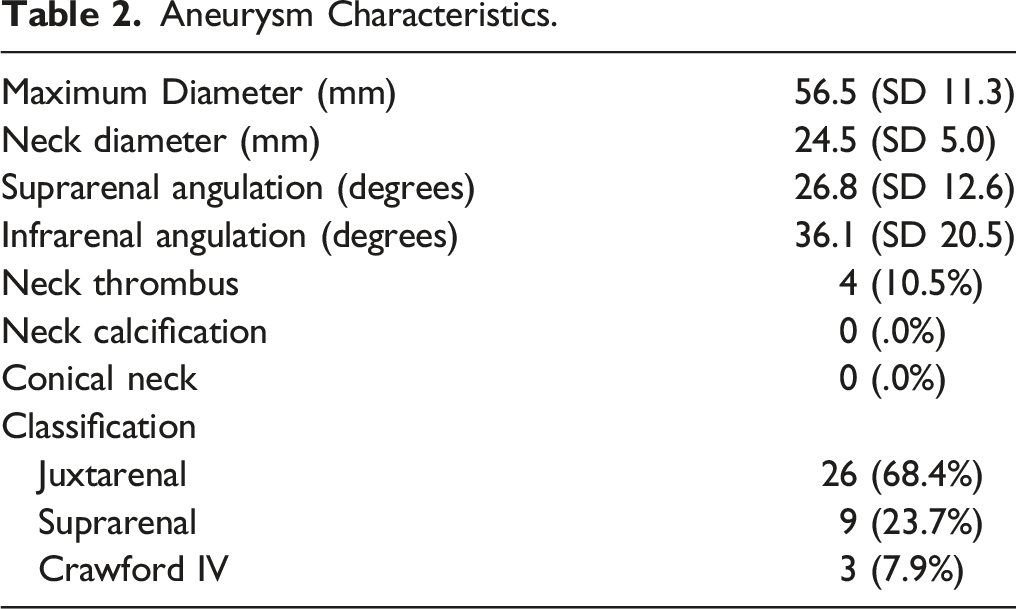
Aneurysm Characteristics.
Details of the Procedure.
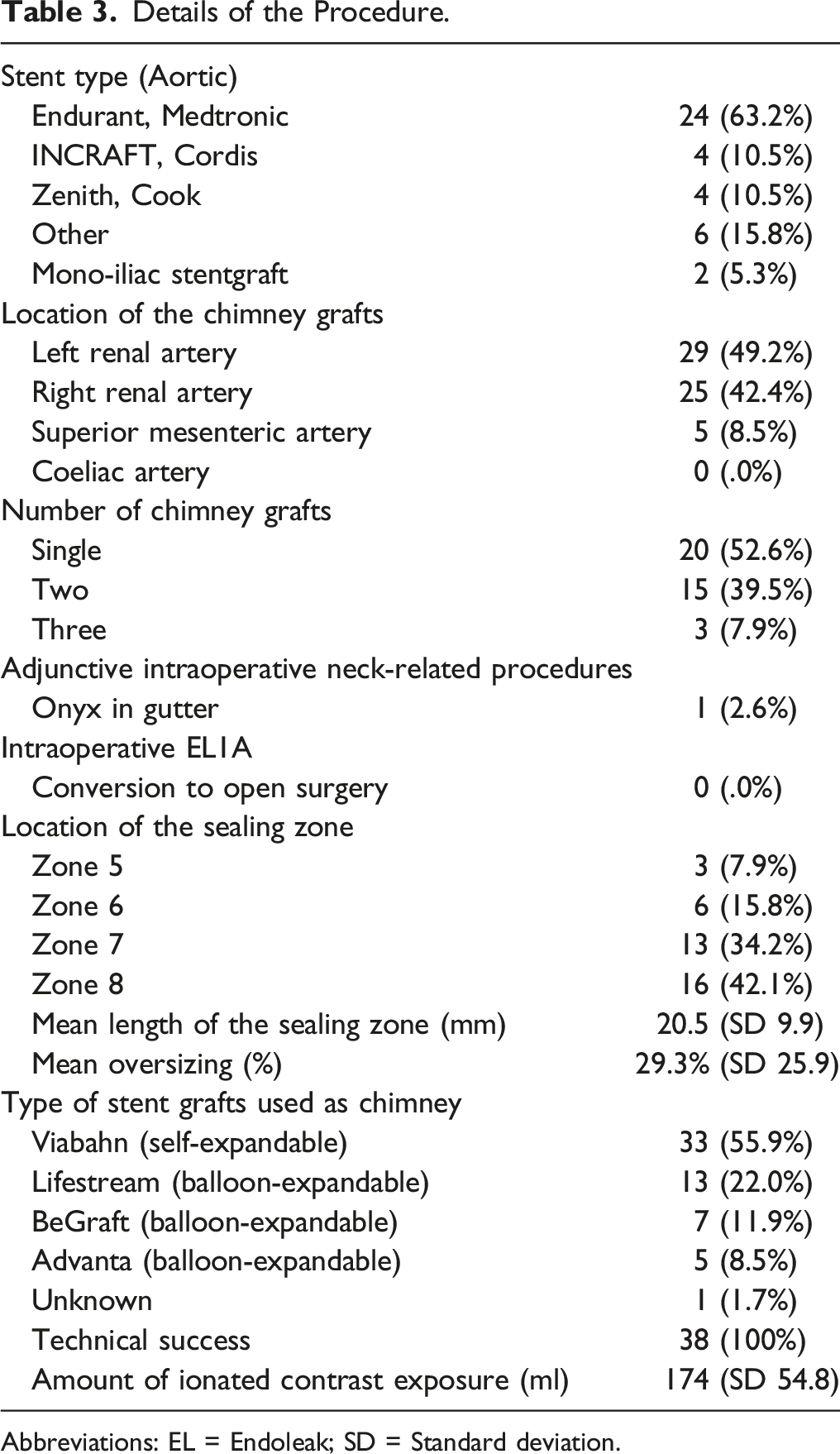
Abbreviations: EL = Endoleak; SD = Standard deviation.
In most patients the new sealing zone was located in segment 8 (42.1%) or segment 7 (34.2%). Mean length of the new sealing zone was 20.5 mm. 13 Lifestream stents (22.0%), 33 Viabahn stents (55.9%), 7 BeGraft stents (11.9%) and 5 Advanta stents (8.5%) were used. In 1 patient the manufacturer of the stentgraft was not mentioned (1.7%).
Chimney Graft Occlusion in the Early Postoperative Phase
Outcome.
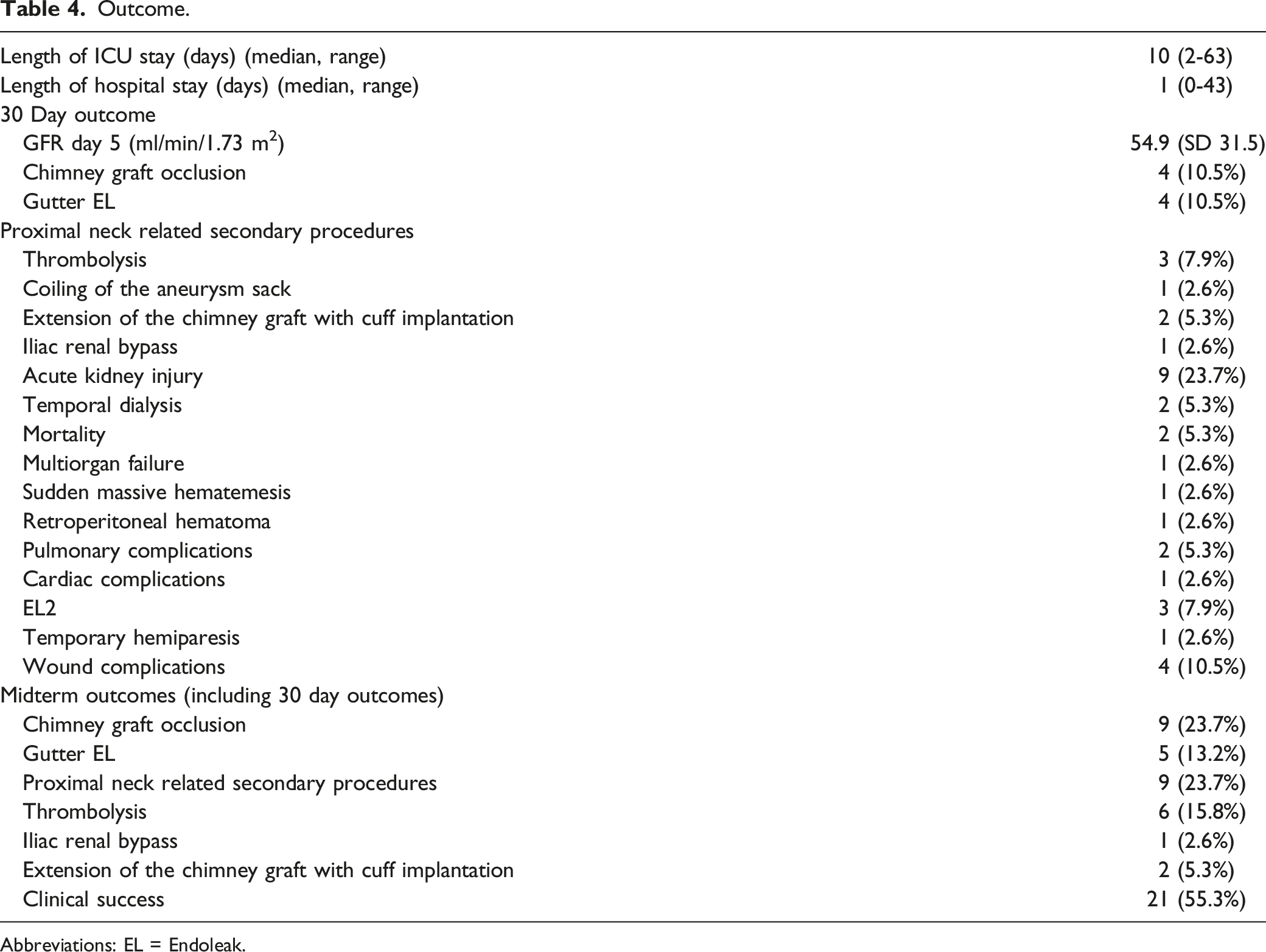
Abbreviations: EL = Endoleak.
Gutter Endoleak in the Early Postoperative Phase
In 4 patients gutter endoleak was seen in the first 30 days. 1 Patient was successfully treated with coiling of the aneurysm sac. Two patients were successfully treated with extension of the chimney grafts and cuff implantation. In 1 patient no treatment was performed and the EL disappeared spontaneously.
Renal Function in the Early Postoperative Phase
During the first 30 postoperative days, there were 9 patients with acute kidney injury according to the KDIGO guidelines, 2 patients needed temporal dialysis, none of the patients needed permanent dialysis. None of these patients had an occluded chimney graft. 10 The cause for the temporal dialysis was a renal hematoma in 1 patient, probably due to wire perforation during the procedure. In the other patient a coronary angiography was necessary during the early postoperative period, because of a NSTEMI. For this patient the cause of the temporal dialysis was probably the iodinated contrast. The remaining 7 patients had a relatively high exposure to iodinated contrast: 211 mL instead of the mean 174 mL.
Chimney Graft Occlusion During the Follow-Up Period
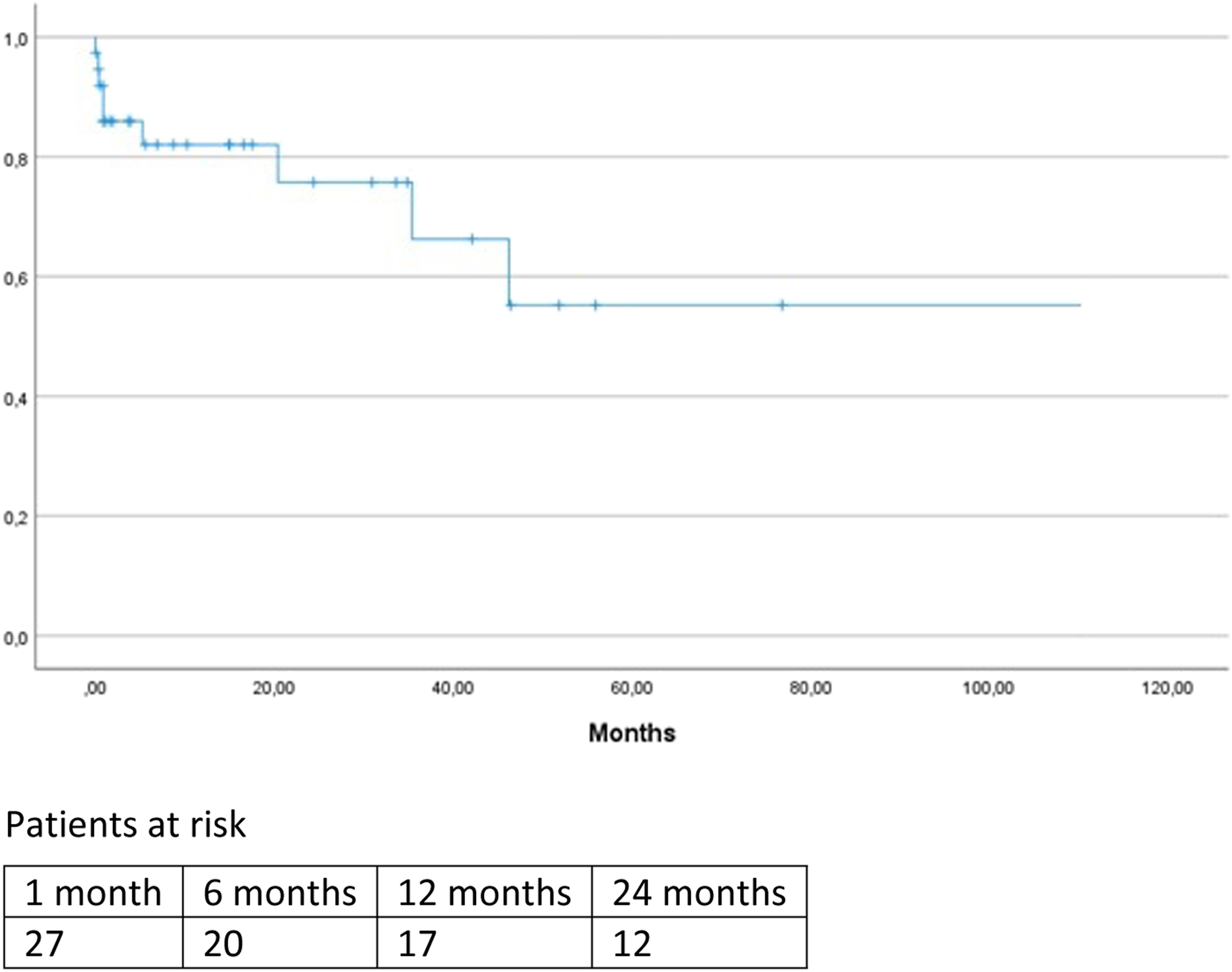
During the follow-up period 5 additional patients presented with a chimney graft occlusion, Figure 1. In all patients a renal infarction was seen on CT-angiography. Attempts to salvage the chimney graft was made in 3 patients but catheterization failed in all patients. Renal function stabilized in all 3 patients and dialysis was not necessary. Mean GFR decreased from 59.0 (SD 25.2) to 40.2 (SD 19.4) in the patients with late occlusion of the chimney graft.
Gutter Endoleak During the Follow-Up Period
Median follow-up was 26.6 months. During this period 1 additional patient presented with a gutter EL, because of a poor general condition, no secondary procedure was performed. This patient is still alive with a stabile diameter of the aneurysm sack. Clinical success was 55.3%.
Aneurysm Related Mortality
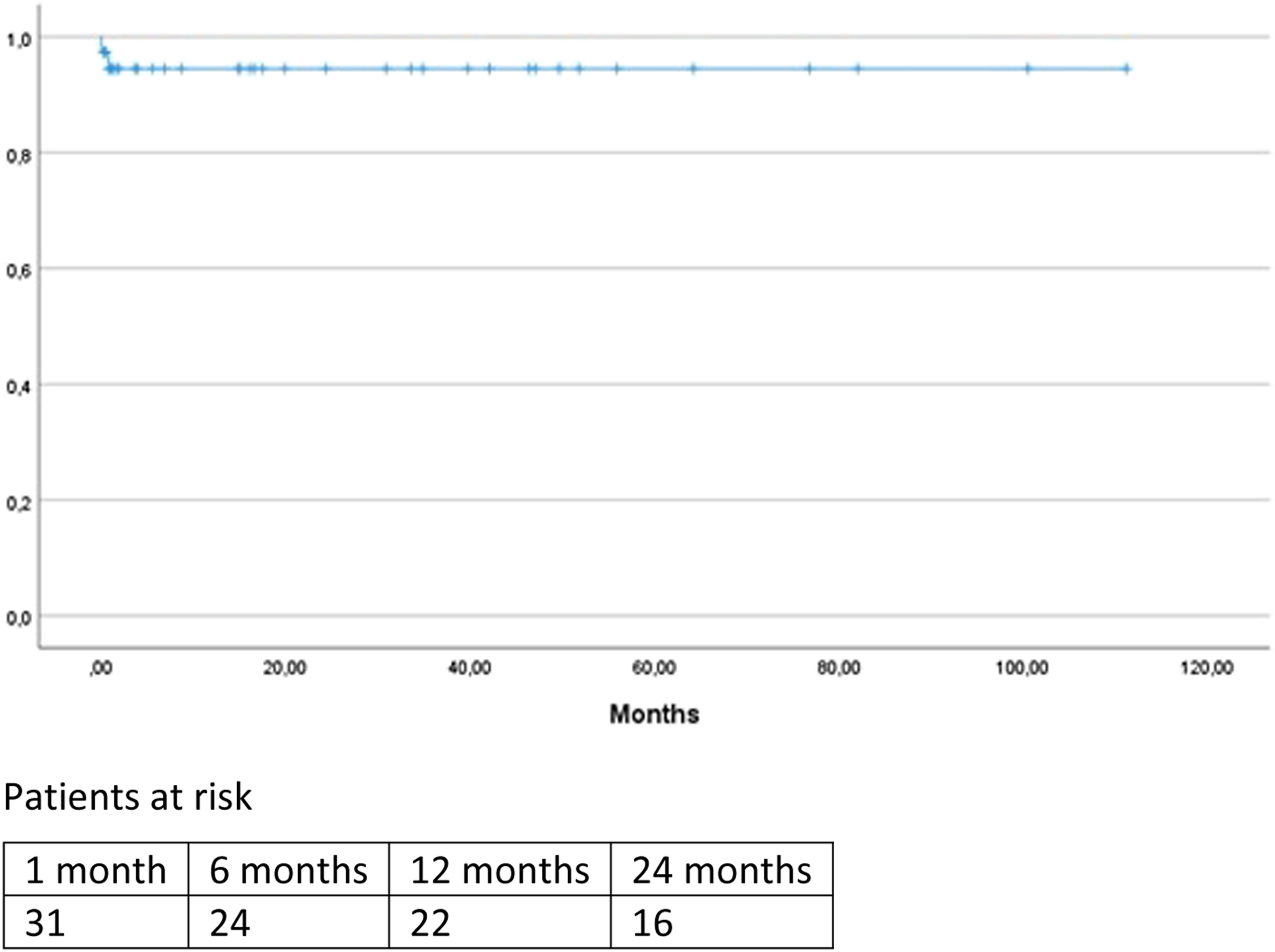
Aneurysm related mortality and occlusion of the chimney graft are depicted in Figure 2 and 3. There were 2 cases of aneurysm-related mortality, both were patients who died during hospital admission. The first patient had multiple comorbidities and died because of multi-organ postoperatively and care was withdrawn. The other patient died as a result of sudden massive hematemesis; the cause of the hematemesis was unclear and autopsy was not performed. There were no patients who died of aneurysm rupture or because of reinterventions. Freedom from aneurysm-related mortality. Freedom from chimney graft occlusion. Freedom from occlusion of balloon-expandable vs self-expandable chimneys.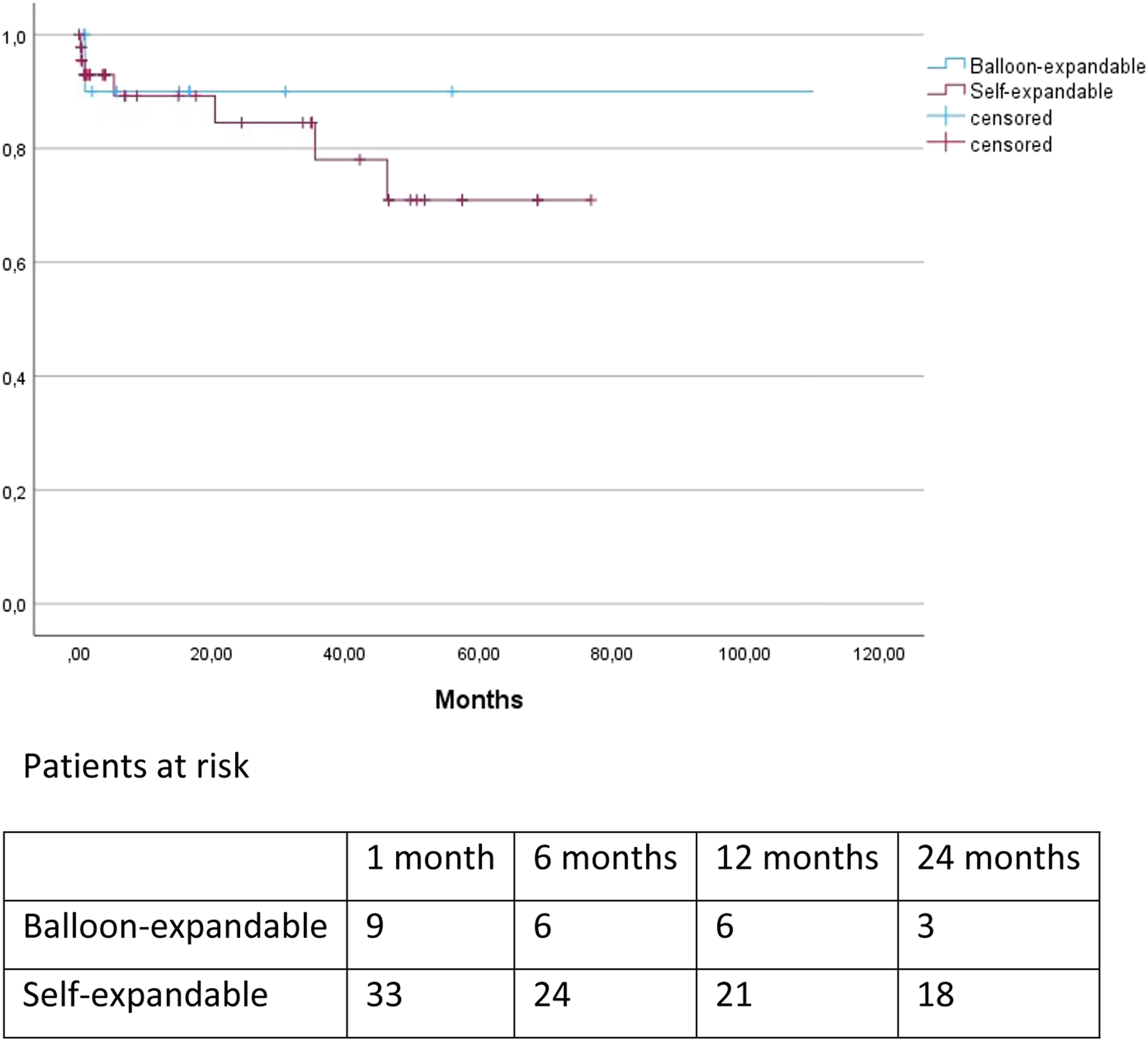
Discussion
ChEVAR was originally reported as a “bailout” after inadvertent renal artery coverage during EVAR. 11 However, due to high technical success rates and excellent short term outcomes, this technique evolved into a primary treatment strategy. Important complications after ChEVAR are gutter EL and risk of chimney graft occlusion. In contrast to f/bEVAR, the chimney grafts are positioned between the aortic wall and the aortic stentgraft. The gaps between the aortic wall, stentgraft and chimney graft can lead to a gutter endoleak and this may be the origin of EL1A. Oversizing was considered to minimize the risk of gutter EL. The ideal amount of oversizing remains unclear, but appears to be 30-40%.12–14
Technical success was 100% in this patient cohort. However, there were 4 chimney graft occlusions in the first 30 days and a 5 more during the follow-up period. Most chimney graft occlusion occurred in the first year of the study period. When compared with other studies, this is a relatively high chimney graft occlusion rate.15,16 A possible explanation could be that in the first years of the study mainly Viabahn stentgrafts were used. At this moment, there is no consensus as to which stentgraft should be used as chimney graft.17–20 Although, recently the Radiant balloon-expandable stent (Medtronic, Santa Rosa, Calif, USA) in combination with the Endurant II/IIs (Medtronic, Santa Rosa, Calif, USA) was approved for ChEVAR. 21 Self-expandable stentgrafts, such as the Viabahn, are flexible and kink resistant, but lack radial force when compared to balloon expandable stentgrafts. Radial force is especially important when using the chimney technique. In our study 7 of 9 chimney occlusions occurred in a self-expandable stentgraft (77.8%), thus underscoring the necessity of choosing the appropriate chimney graft. The number of chimneys did not seem to influence the risk of chimney stent occlusion in our study, since 5 occlusions occurred in the group with 1 chimney and 4 in the group with 2 chimneys.
Another explanation for the relative high incidence of chimney graft occlusion in our patient cohort could be the use of suprarenal fixation. Almost all aortic stentgrafts used in our study population had a suprarenal fixation. As described in the method section the chimney graft was placed 2-3 mm above the covered fabric, thereby the chimney graft could be compressed by the suprarenal crown. In the majority (6 of 9 patients with an occlusion of the chimney graft) the proximal end of the chimney graft was located under the proximal end of the suprarenal crown.
Late onset EL1A is an uncommon complication after EVAR, with an incidence of 1-5%.22–24 It is associated with continued sac expansion and risk of rupture.25,26 There are studies which suggest that primary EL1A, defined as EL1A at the completion angiography, has a more mild course when compared to late onset EL1A. 27 O’Donnell et al. described a patient cohort of 1484 procedures, the incidence of EL1A at the completion angiography was 2.9% (43 patients), of which 16 (1.1%) EL1A persisted at 1 months and 6 patients (.4%) at 1 year. The authors concluded that early EL1A can be safely observed. This may also hold true for gutter EL. 28 In the current study 5 patients presented with gutter EL. Three were successfully treated, the gutter EL disappeared in 1 and 1 patient refused treatment due to poor general condition. No patient died because of aneurysm rupture during the study period. These results are in concurrence with other studies and support the hypothesis that the natural history of gutter EL may be relatively benign.13,19 A systematic review reported an early gutter or type IA EL of 13% and a relatively low risk of late EL (2%). 27 In our study most patients with gutter EL had 2 or more chimneys (4 of 5 patients). This finding is not supported by other studies.13,29
Because of encouraging short- and midterm results f/bEVAR is now increasingly used in Europe and the United States. F/bEVAR remains a technical challenge and f/bEVAR may be more costly than ChEVAR. Off-the-shell devices are available, but are not suited for all patients. 1 The main conclusion of most systematic reviews comparing f/bEVAR and the chimney technique is that f/bEVAR is associated with more re-interventions (mainly EL and target vessel related), less target vessel occlusion and less EL1.30,31 The chimney technique is associated with a high rate of technical success, but also a higher rate of aneurysm-related mortality. 32 It should be kept in mind however that the chimney technique is more often used in patients symptomatic or ruptured aneurysms, because off-the-shelf fEVAR are only available in the last years.
Limitations
There are 2 major limitations. First, this is a non-comparative retrospective study and, secondly, the number of included patients is relatively small. Due to the retrospective nature of the study, bias cannot be excluded. Since these are the outcomes of a small community hospital, the number of patients is small, but, in our opinion, reflect common day practice. Most procedures took place in the first years of the study period, therefore a relatively large number of patients were treated with a self-expandable stentgraft, which may have contributed to the high rate of chimney grafts occlusion.
Conclusions
In this retrospective study, results from 38 patients treated with the chimney technique are presented. Chimney graft occlusion rate was 15.3% at the end of follow-up. The majority of the occluded stents were self-expandable stents, thereby underscoring the necessity of appropriate choice of stentgraft. Also, it should be avoided that the proximal part of the chimney graft ends at the level of the suprarenal crown. ChEVAR should be used with caution in elective patients with suprarenal or juxtarenal aneurysms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: D.H. is a proctor for Boston Scientific. The other authors declare that there is no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.