
Abstract
Objectives:
Comparative effectiveness of fenestrated endovascular aneurysm repair (FEVAR) and chimney graft endovascular aneurysm repair (ChEVAR) for juxtarenal aortic aneurysms (JAAs) remains unclear. Our objective was to identify and analyze the current body of evidence comparing the effectiveness of both techniques for JAA.
Methods:
We performed a systematic review and meta-analysis comparing the effectiveness of FEVAR and ChEVAR for JAA repair. We searched MEDLINE, EMBASE, and Cochrane Register for Controlled Trials from January 1, 1990, for randomized and non-randomized studies assessing outcomes of FEVAR and ChEVAR for JAA repair. Screening, data extraction, risk of bias assessment, and GRADE (Grading of Recommendations, Assessments, Development, and Evaluations) certainty of evidence were performed in duplicate. Data were pooled statistically where possible.
Results:
Nine retrospective cohort studies comparing the use of FEVAR and ChEVAR for juxtarenal aneurysm were included for meta-analysis. The FEVAR and ChEVAR arms of the meta-analysis consisted of 726 participants and 518 participants, respectively. There were 598 (86.8%) and 332 (81.6%) men in each arm. The mean diameter was larger in the ChEVAR arm (59 mm vs 52.5 mm). Both techniques had similar rates of postoperative 30-day mortality, 3.38% (8/237) versus 3.52% (8/227), acute kidney injury, 16.76% (31/185) versus 17.31% (18/104), and major adverse cardiac events, 7.30% (46/630) versus 6.60% (22/333). The meta-analysis supported the use of FEVAR for most outcomes, with significant advantage for technical success (odds ratio [OR]: 3.24, 95% CI: 1.24–8.42) and avoidance of type 1 endoleak (OR: 5.76, 95% CI: 1.94–17.08), but a disadvantage for spinal cord ischemia (OR: 10.21, 95% CI: 1.21–86.11), which had a very low number of events. The quality of evidence was “moderate” for most outcomes.
Conclusion:
Both endovascular techniques had good safety profiles. The evidence does not support superiority of either FEVAR or ChEVAR for JAA.
Clinical Impact:
While lack of equipoise has hampered the design of randomised trials of open versus endovascular repair of juxtarenal aortic aneurysms, concern about the durability of endovascular repair highlights the need for stronger evidence of the comparative efficacy of endovascular techniques. This review performed meta-analysis and evidence appraisal of recent data from large observational studies comparing fenestrated and chimney techniques, using a comprehensive outcome set. Superiority of either intervention could not be established due to differences in participants’ baseline risk in each study arm. However, data suggests that both techniques are safe and suitable for use when indicated.
Introduction
Abdominal aortic aneurysms that extend close to <10 mm, but do not involve the visceral arteries are most commonly called juxtarenal aortic aneurysm (JAA). 1 They account for approximately 15% of abdominal aortic aneurysms (AAAs) worldwide.2,3 The anatomical complexities of JAAs make open repair more technically difficult. The higher likelihood of prolonged suprarenal clamping and/or revascularization of the visceral vessels during open repair for this population is associated with increased risk of perioperative complications, postoperative renal impairment, and mortality.4–6
Unfortunately, the short neck (<10 mm) of JAAs rarely facilitates durable proximal sealing during standard endovascular aneurysm repair (EVAR). 7 Two endovascular techniques developed to circumvent this problem are fenestrated endovascular aneurysm repair (FEVAR) and chimney graft endovascular aneurysm repair (ChEVAR). Both techniques aim to extend the proximal sealing zone above the renal arteries while maintaining perfusion of visceral and/or renal arteries. FEVAR is technically challenging and requires meticulous planning and custom graft production, which often precludes its use in the urgent setting. In comparison, the ChEVAR technique is often available off-the-shelf in emergent cases but can be prone to junctional endoleaks. Overall, durability is uncertain for all endovascular repairs that involve visceral vessels. 8
The comparative effectiveness of FEVAR and ChEVAR for repair of JAAs remains unclear and has become an important issue as the prevalence of endovascular operations increase. In 2016, Li et al 9 published a systematic review comparing the benefit and harm of FEVAR and ChEVAR for JAA repair. The body of evidence they presented was not formally assessed for risk of bias, nor were analyses powerful enough to make conclusions about comparative effectiveness of the techniques. A 2018 review by Caradu et al 10 included participants with pararenal aneurysms in their analysis, which is a more vague term only sometimes referring to JAAs. They used the Cochrane Risk of Bias 2.0 tool 11 to assess the non-randomized studies in their review. Differences in definitions and reporting of complex juxtarenal neck anatomy (eg, pararenal vs juxtarenal) may influence the results of comparative studies, which will hopefully be clarified by the UK-COMPASS study. 12 Patel et al 6 also compared FEVAR and ChEVAR in a recent network meta-analysis that included pararenal aneurysm. In recent years, there have been several large-scale observational studies13–15 and developments in endovascular repair with lower profile devices, steerable sheaths, and new bridging stents with 3 or 4 visceral vessels now being stented more commonly than before. Herein, we describe a systematic review and meta-analysis to compare the clinical benefit and harm of FEVAR and ChEVAR for repair of JAAs in adults.
Materials and Methods
Search Strategy and Selection Criteria
We conducted a systematic search for randomized and non-randomized studies comparing the benefits and harm of FEVAR and/or ChEVAR techniques for adults with JAA. The search was carried out and reported as per Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines. 16 The search strategy utilized a combination of the terms and acronyms for “juxtarenal aortic aneurysm,” “snorkel graft,” “fenestrated graft,” “zenith graft,” and “chimney graft”. We searched MEDLINE, EMBASE, and Cochrane Central Register of Controlled Trials (CENTRAL) from January 1, 1990 (year of first reported endovascular aneurysm repair) to July 9, 2023. Our search was restricted to English language records only. The references of all relevant records were searched manually for additional relevant studies.
We included original studies that presented comparisons of at least 5 participants with JAA treated with FEVAR or ChEVAR. Authors must have explicitly described the participants as having juxtarenal aneurysms. Studies describing only complex (involvement of renal and/or mesenteric arteries) or pararenal aneurysms (where the renal arteries originate from the aneurysmal aorta, but the level of the superior mesenteric artery is not aneurysmal) were excluded to reduce indirectness. In our review, treatment with unlicensed grafts, off-the-shelf or physician-modified grafts, hybrid procedures, and bailout procedures were excluded. Reviews and case studies were also excluded.
Data Collection
At least 2 of the authors (T.B., T.R., T.M., and G.F.) independently screened the titles and abstracts of each citation, reviewed full texts, extracted data, and assessed risk of bias using Covidence online software. 17 Discrepancies were resolved by discussion among reviewers until consensus was reached. We extracted information regarding study design, country, setting, funding source, conflicts of interest, population characteristics, intervention characteristics, and relevant health outcomes.
Outcomes
The outcomes of interest for this study were determined a priori to the systematic literature search. The primary outcomes were technical success (as reported by authors), 30-day mortality, and acute kidney injury. Secondary outcomes of interest were target vessel occlusion, aneurysm-related mortality, avoidance of type 1 endoleak, avoidance of type 2 endoleak, avoidance of type 3 endoleak, reintervention, major adverse cardiac event, stroke, spinal cord ischemia, lower limb ischemia, compartment syndrome, and access site complications.
Data Analysis and Quality Assessment
Pooled analysis of participant and operation characteristics was performed across all included studies. This was presented as percentages and mean (SD). A meta-analysis of associations reported in the 2-armed comparative studies was performed using the Mantel-Haenszel method. We measured the effect magnitude by calculating odds ratios (ORs) and corresponding 95% CIs, using a fixed-effects model. The analysis was completed using Cochrane’s Review Manager Version 5.3 software for reviews. 18 Heterogeneity among included studies was assessed for each outcome, using the I2 statistic. Subgroup analyses were attempted to test whether indication for aneurysmal repair (elective vs urgent or emergent) modified the effect of FEVAR compared with ChEVAR for the outcome set. However, a small number of trials contributed to the subgroup for elective cases only (2 trials, 719 participants). The remaining studies included a combination of elective, urgent, or emergent cases, making it difficult to isolate the effect of indication. For these reasons, we deemed the subgroup analysis to be invalid and underpowered. As such, the analysis is not presented in this article.
The risk of bias of each non-randomized study included in our meta-analysis was rated using the risk of bias in non-randomized studies of interventions (ROBINS-I) tool. 19 No randomized studies were identified by our systematic search. The quality of evidence for all studies included in the meta-analysis was assessed using The Grading of Recommendations, Assessments, Development, and Evaluations (GRADE) approach, 20 which was used to present the quality of evidence in this review.
Results
Search Results
A total of 5924 records were screened for inclusion. The full texts of 457 articles were retrieved and 9 studies (1244 total participants) met inclusion criteria for the meta-analysis (Figure 1). Our systematic search did not identify any randomized studies meeting our inclusion criteria.
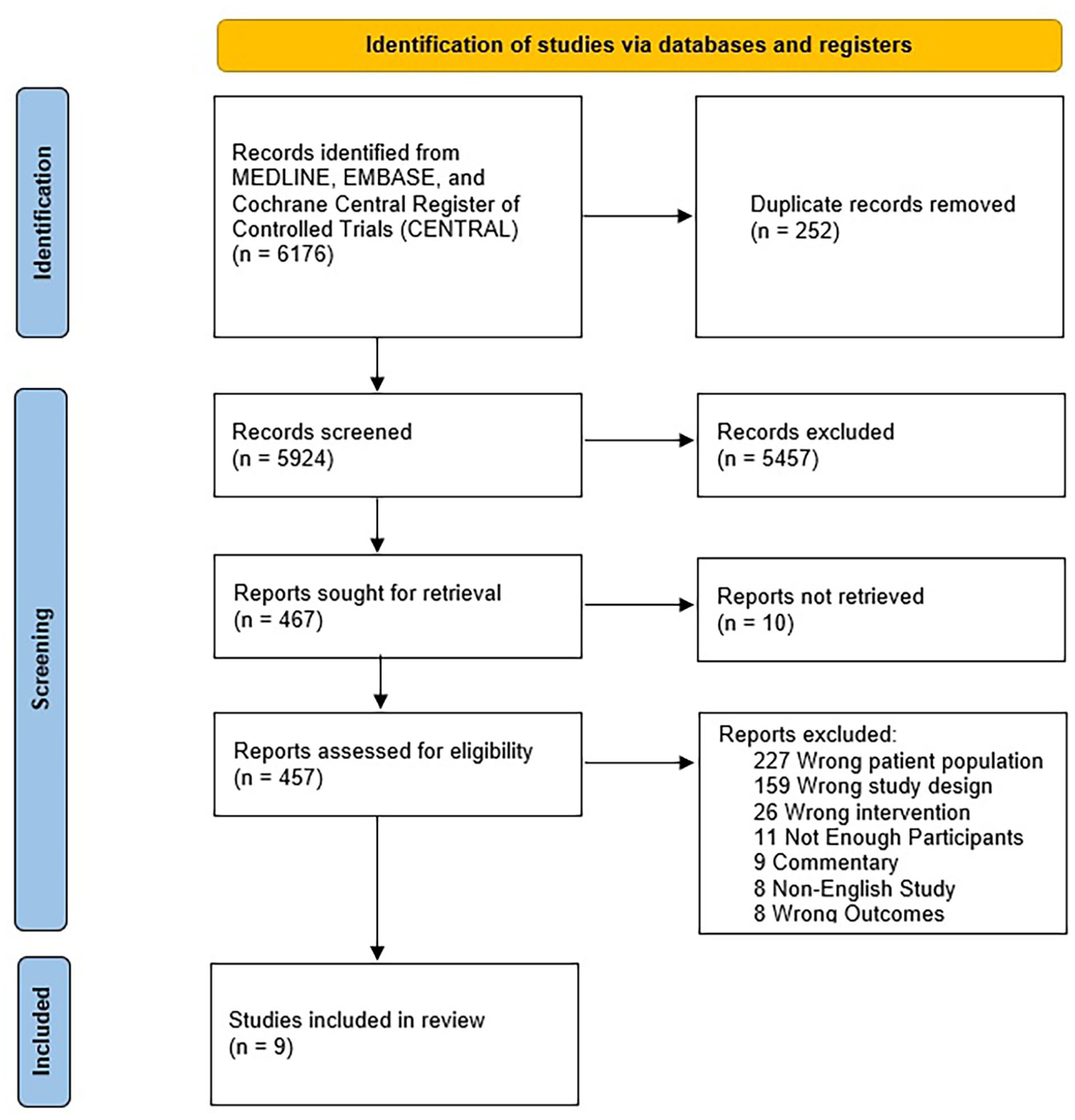
A PRISMA diagram of studies comparing FEVAR and ChEVAR for repair of juxtarenal aortic aneurysms. A total of 6176 records were returned from the search. There were 457 full texts assessed for eligibility. Of these, 9 were included in the meta-analysis. ChEVAR, chimney endovascular aortic repair; FEVAR, fenestrated endovascular aortic repair; PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses.
Included Studies
There were nine retrospective cohort studies included in the meta-analysis.21–29 Study characteristics for these are summarized in Table 1. There were 6 European studies, 2 American studies, and 1 Asian study. The FEVAR and ChEVAR arms consisted of 726 participants and 518 participants, respectively. There were 630 (2.28 vessels per patient) and 518 (1.84 vessels per patient) target vessels reported in each arm, respectively, although this does not include Steffen et al, 29 which did not report the number of target vessels. Steffen et al 29 and Lee et al 25 included only elective cases, whereas other studies in this review included elective and urgent or emergent cases. The mean length of follow-up was 53.82 months in the FEVAR arm and 55.43 months in the ChEVAR arm. There were 598 (86.8%) and 332 (81.6%) men in each arm (p<0.93), excluding Taneva et al, 28 which did not report the number of males. The mean (SD) age of those undergoing FEVAR and ChEVAR repair was 71.89 (4.59) years and 75.00 (7.19) years, respectively (p<0.001). There were significant differences observed in mean aneurysmal diameter (52.59±3.34 mm vs 59.16±9.08 mm, p<0.001) but not mean neck length (3.73±5.56 mm vs 4.52±5.16 mm, p=0.31) between arms.
Study Characteristics of Included Studies (N=9) Reporting Data on ChEVAR and FEVAR for Repair of Juxtarenal Aortic Aneurysm.
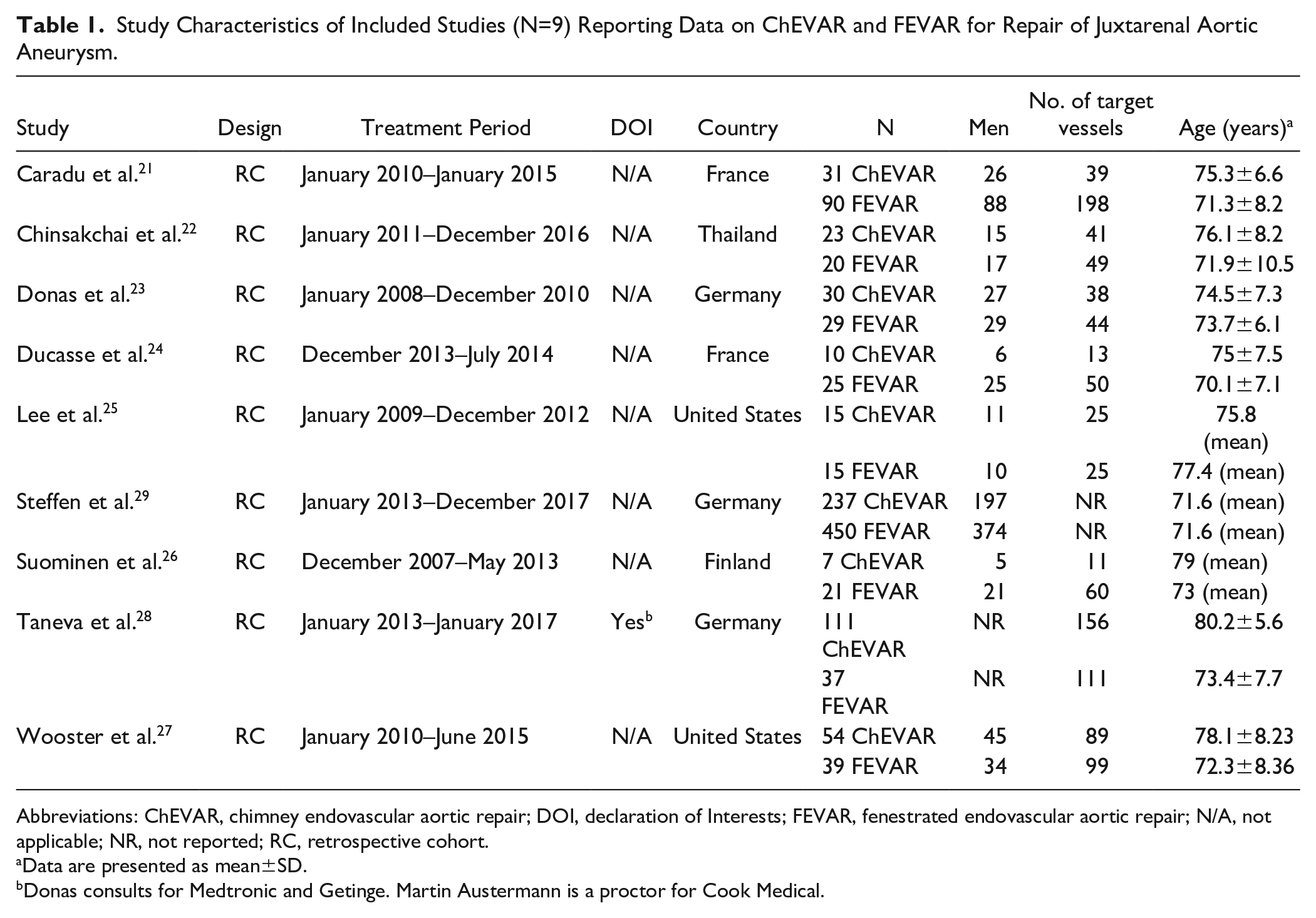
Abbreviations: ChEVAR, chimney endovascular aortic repair; DOI, declaration of Interests; FEVAR, fenestrated endovascular aortic repair; N/A, not applicable; NR, not reported; RC, retrospective cohort.
Data are presented as mean±SD.
Donas consults for Medtronic and Getinge. Martin Austermann is a proctor for Cook Medical.
Reporting of comorbidity data was inconsistent between studies (Table 2). The most prevalent comorbidities in the FEVAR and ChEVAR arms were hypertension (81.46% vs 81.43%, p=0.99), hyperlipidemia (51.98% vs 52.11%, p=0.98), coronary artery disease (52.08% vs 54.26%, p=0.72), and smoking history (59.91% vs 76.10%, p<0.001). Participants in the FEVAR arm were more likely to be obese (61.74% vs 41.05%, p<0.002) and less likely to have chronic obstructive pulmonary disease (COPD; 29.52% vs 38.43%, p<0.03) and prior aortic surgery (8.18% vs 27.90%, p<0.001). No statistically significant differences were observed in the prevalence of renal insufficiency (20.62% vs 19.31%, p=0.78), cerebrovascular disease (11.49% vs 8.42%, p=0.44), diabetes mellitus (17.56% vs 15.00%, p=0.53), hostile abdomen (17.78% vs 19.35%, p=0.85), and peripheral arterial disease (16.00% vs 10.00%, p=0.65). Malignancy data were not reported in the included studies.
Comparison of Pooled Participant Characteristic Data for Repair of Juxtarenal Aortic Aneurysm Using FEVAR and ChEVAR.
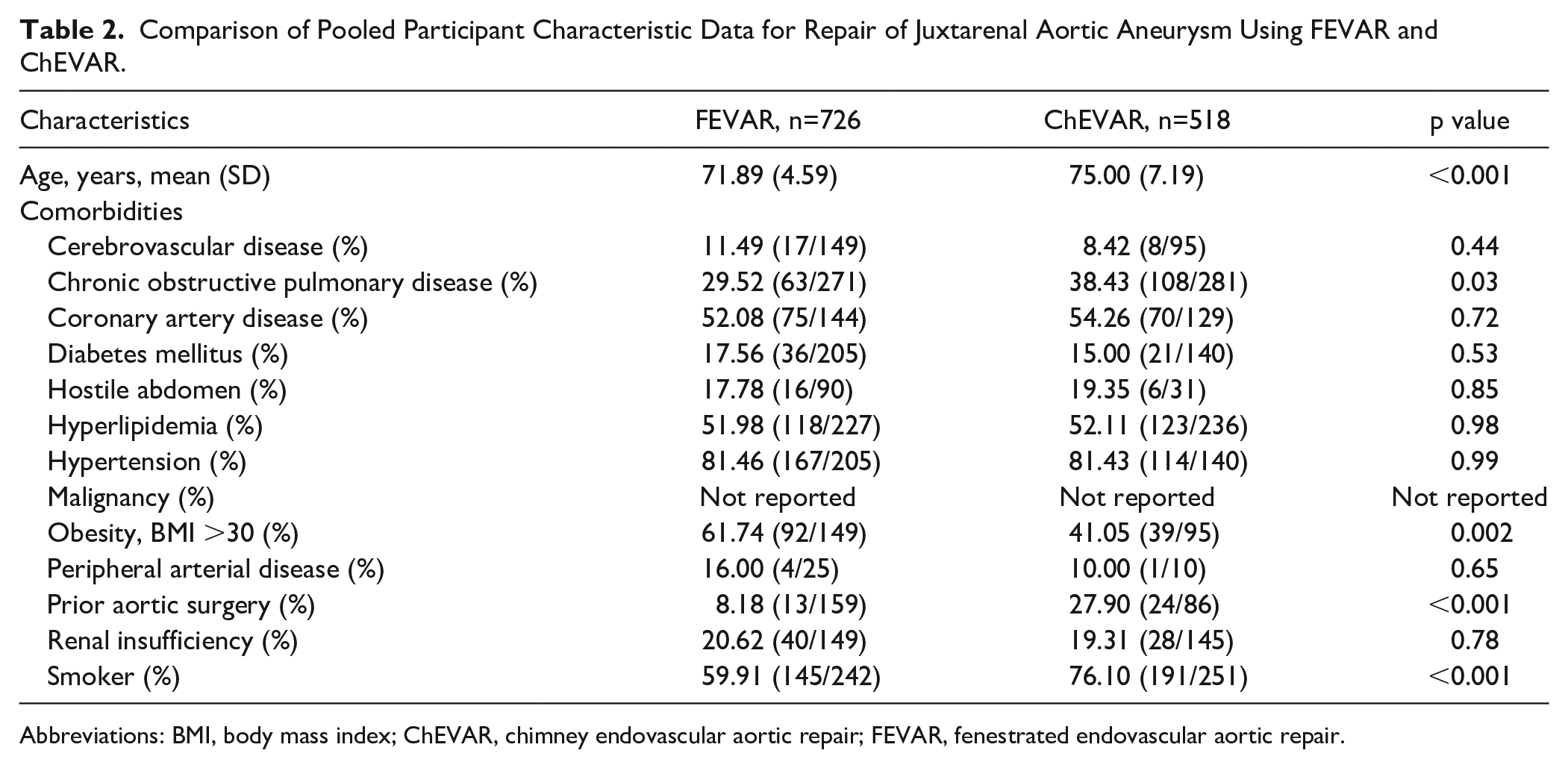
Abbreviations: BMI, body mass index; ChEVAR, chimney endovascular aortic repair; FEVAR, fenestrated endovascular aortic repair.
The operation characteristics for both study arms are presented in Table 3. Participants in the FEVAR arm experienced significantly longer mean operation times (212.17±84.44 min vs 174.68±62.88 min; p<0.001), fluoroscopy times (69.85±58.65 min vs 56.34±32.55 min; p=0.007), and higher contrast doses (132.18±51.60 mL vs 94.30±26.39 mL; p<0.001). Mean blood loss was not reported consistently in all included studies and no significant differences were detected between the FEVAR and ChEVAR arms (482.43±213.11 mL vs 583.37±734.21 mL; p=0.33).
Comparison of Pooled Operation Characteristics for Repair of Juxtarenal Aortic Aneurysm Using FEVAR and ChEVAR.
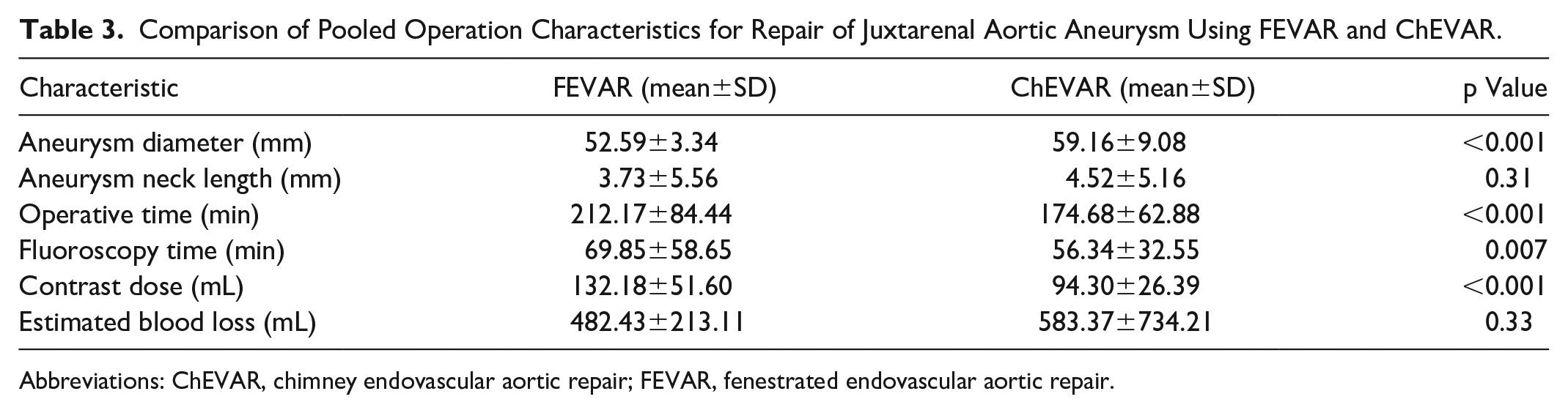
Abbreviations: ChEVAR, chimney endovascular aortic repair; FEVAR, fenestrated endovascular aortic repair.
Meta Analysis
Data from the nine comparative studies were extracted and pooled for meta-analysis.21–29 Forest plots for outcomes of interest are presented in Figures 2A–O. The effect estimates and evidence appraisal judgments are summarized in Supplemental Table S2. No data for the outcomes “lower limb amputation” and “compartment syndrome” were reported in the included studies and so the corresponding forest plots are not presented herein. Substantial and moderate heterogeneity were present in the analysis for outcome “acute kidney injury” (I2 Statistic = 46%), respectively (Figure 2I). The definition of acute kidney injury reported by study authors varied considerably, so analysis of these data in particular should be interpreted with caution. We included the following definitions in our analysis: “acute kidney injury (any stage),” “Increase in serum creatinine by ≥1.5 times the pre-op measurement,” “renal impairment,” “renal failure,” “contrast induced nephropathy,” and “≥25% reduction in eGFR.”
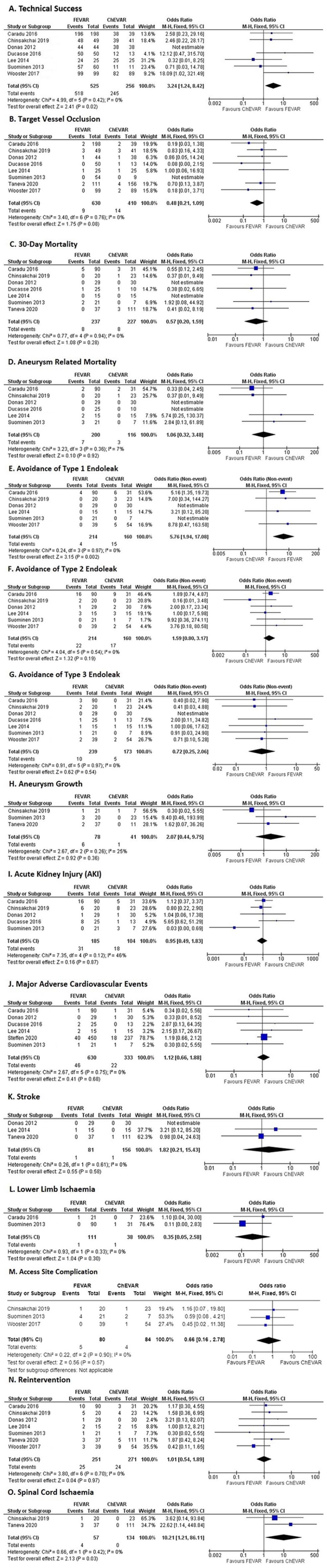
Forest plots for comparison of outcomes of FEVAR and ChEVAR for repair of juxtarenal aortic aneurysm. The outcomes of interest presented are as follows: (A) Technical success, (B) target vessel occlusion, (C) 30-day mortality, (D) aneurysm-related mortality, (E–G) avoidance of type 1 to 3 endoleak, (H) aneurysm growth, (I) acute kidney injury, (J) major adverse cardiac event, (K) stroke, (L) lower limb ischemia, (M) access site complication, (N) reintervention, and (O) spinal cord ischemia. ChEVAR, chimney endovascular aortic repair; FEVAR, fenestrated endovascular aortic repair.
The effect estimates from our meta-analysis support the use of FEVAR over ChEVAR with respect to the following outcomes: technical success (OR: 3.24, 95% CI: 1.24–8.42), target vessel occlusion (OR: 0.48, 95% CI: 0.21–1.09), 30-day mortality (OR: 0.57, 95% CI: 0.20–1.59), avoidance of type 1 endoleak (OR: 5.76, 95% CI: 1.94–17.08), avoidance of type 2 endoleak (OR: 1.59, 95% CI: 0.80–3.17), acute kidney injury (OR: 0.95, 95% CI: 0.49–1.83), lower limb ischemia (OR: 0.35, 95% CI: 0.05–2.58), and access site complication (OR: 0.66, 95% CI: 0.16–2.78).
In comparison, the use of ChEVAR was supported by effect estimates for the following outcomes: aneurysm-related mortality (OR: 1.06, 95% CI: 0.32–3.48), avoidance of type 3 endoleak (OR: 0.72, 95% CI: 0.25–2.06), aneurysm growth (OR: 2.07, 95% CI: 0.44–9.75), major adverse cardiac events (OR: 1.12, 95% CI: 0.66–1.88), stroke (OR: 1.82, 95% CI: 0.21–15.43), reintervention (OR: 1.01, 95% CI: 0.54–1.89), and spinal cord ischemia (OR: 10.21, 95% CI: 1.21–86.11).
The certainty of evidence (Supplemental Table S2) surrounding these comparisons was “moderate” for 3 outcomes (technical success, aneurysm-related mortality, and avoidance of type 1 endoleak), “low” for 6 outcomes (30-day mortality, target vessel occlusion, avoidance of type 2 endoleak, avoidance of type 3 endoleak, reintervention, lower limb ischemia, and access site complication), and “very low” for all remaining outcomes. The risk of bias assessments for each study are summarized in Table 4. Generally, there was inadequate control of confounders (eg, age, comorbidities, prior surgery, and neck angulation) and selection bias due to the comorbidity profile of the participants and indication for ChEVAR in emergent settings. The overall risk of bias for all studies was “serious”.
ROBINS-I Summary of Risk of Bias for Non-Randomized Studies Comparing FEVAR and ChEVAR for Repair of Juxtarenal Aortic Aneurysms.
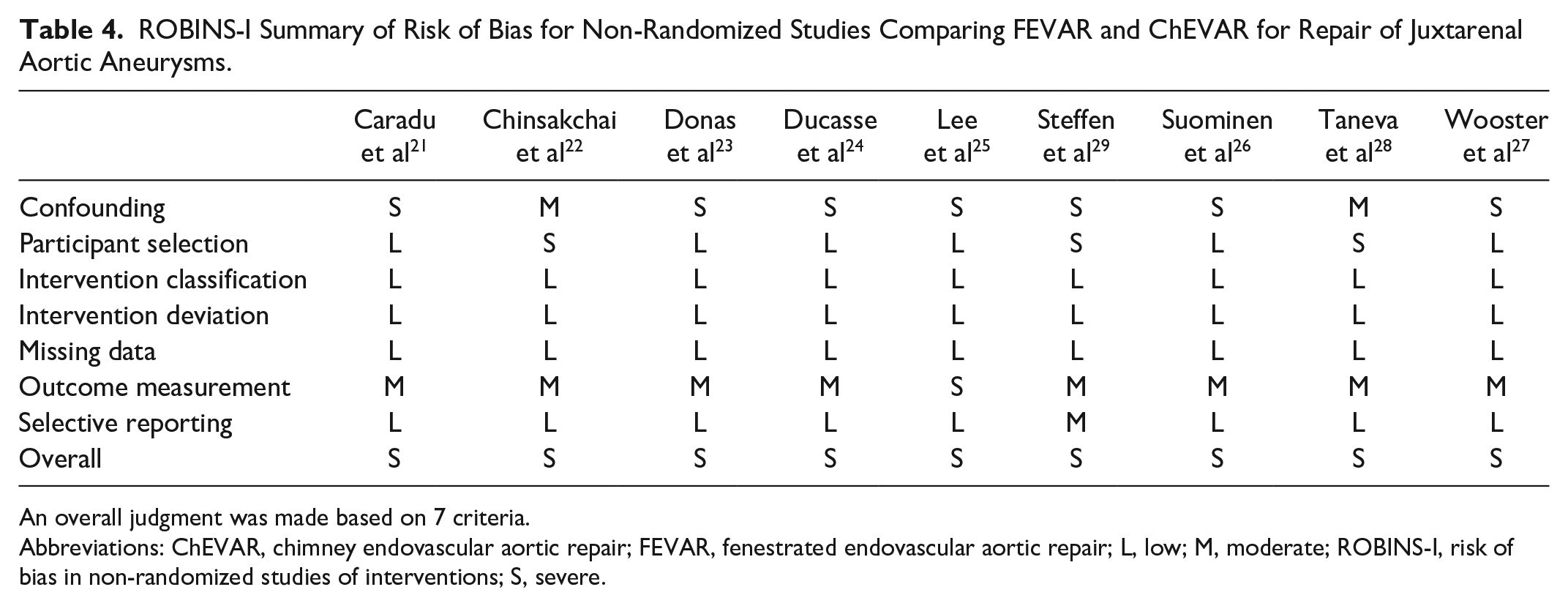
An overall judgment was made based on 7 criteria.
Abbreviations: ChEVAR, chimney endovascular aortic repair; FEVAR, fenestrated endovascular aortic repair; L, low; M, moderate; ROBINS-I, risk of bias in non-randomized studies of interventions; S, severe.
Discussion
The Society of Vascular Surgery (SVS) states in its AAA clinical practice guidelines that “fenestrated, branched, and chimney or snorkel grafts have expanded the range of complex aortic anatomy potentially treatable by EVAR.” 30 Although the SVS guidelines do not make a recommendation for a specific procedure, the European Society of Vascular Surgery (ESVS) guidelines do make a recommendation based on weak evidence that patients with JAA should be considered for open repair or complex endovascular repair, when indicated by patient status, anatomy, local routines, team experience, and patient preference. 1 In this review, we compared the use of FEVAR and ChEVAR in adults with JAA. Lack of equipoise has hampered the design of randomized trials in this area, despite the need being well-documented.9,10,31 As a result, only observational studies were included in the analyses.
There were differences in the comorbidity profile of participants in the FEVAR and ChEVAR arms. Those receiving ChEVAR were older in age and had higher rates of smoking, COPD, and prior aortic surgery. Only the rate of obesity was higher in the FEVAR arm. Comorbidity data were reported inconsistently across included studies, but analysis of available data suggests that those receiving ChEVAR were more sick. In this study, FEVAR outcomes were more favorable despite significantly greater operation times, fluoroscopy times, and contrasts doses, likely because, on average, these patients had more vessels stented and smaller aneurysms than the ChEVAR arm. Furthermore, patients presenting acutely were more likely to have received ChEVAR as FEVAR stents are not readily available off-the-shelf. 31 This may have profoundly influenced the comorbidity profiles, aneurysm characteristics, as well as decision-making. In that respect, participants undergoing the ChEVAR procedure could be expected to have larger aneurysms and worse clinical outcomes compared with FEVAR. Therefore, it was unsurprising that the significant relative effects in this meta-analysis supported the use of FEVAR over ChEVAR. Existing meta-analysis have been unable to show significant difference in effects, typically because of the relatively small number of participants, 9 inclusion of complex aneurysms,5,6,10 and limited outcome sets.5,6 They generally yielded point estimates that favored FEVAR, with the exception of Caradu et al, 10 which was an older study that included pararenal aneurysms.
The only statistically significant findings of the meta-analysis were for the outcomes “technical success,” “avoidance of type 1 endoleak,” and “spinal cord ischemia” (Figure 2A, E, and O). The outcomes “technical success” and “avoidance of type 1 endoleak” supported the use of FEVAR over ChEVAR. The outcome “spinal cord ischemia” supported use of ChEVAR but was based on a small number of events in the FEVAR arm only. It should be interpreted with caution. The higher number of type 1 endoleaks observed in the ChEVAR arm may be related to the procedure’s reliance on stent placement alongside the aortic wall and parallel to the main graft. Unlike FEVAR, this has the potential to produce gutter endoleaks, particularly when more than 2 vessels require repair. There were also possible anatomical differences that may have influenced the number of type 1 endoleaks, such as participants in the ChEVAR arm having larger aneursyms. Furthermore, FEVAR is less compatible with very angulated necks and therefore these aneurysms may be underrepresented in the FEVAR arm.
The outcome set from this review should be further investigated in future randomized or observational studies, as per existing protocols. 12 Although the meta-analysis in this study yielded minimal statistically significant findings, the absolute number of complications (in particular deaths, endoleaks, and reinterventions) for both arms in the meta-analysis was small and supports both interventions as being safe. Neither intervention can be established as being superior due to inherent differences in the risk profile between arms (ie, comorbidities, aneurysm characteristics, and indication). These factors should be investigated in future study. Until off-the-shelf fenestrated grafts become widely available, there will likely remain a role for ChEVAR, given its acceptable safety profile and suitability for emergent scenarios. Other promising alternatives for urgent aneurysm repair include physician-modified endografts (PMEGs) and inner endograft branches. The PMEGs have been used for years but require the skills for planning modifications to the endograft and modifying measurements, and a willingness to accept any legal consequences of modification. Branched endografts are relatively new but may have limitations in the context of narrow aortic lumens. It was not assessed as an independent comparator in Patel’s recent network meta-analysis. 6 As both options evolve and increase in usage, they should be compared with FEVAR and ChEVAR to develop clinical guidance. Finally, open aneurysm repair should also be considered for suitable (younger, low-risk) patients due to relatively higher perioperative mortality4,6 and improved midterm outcomes4,5 when compared with FEVAR in recent studies.
This review was strengthened by its detailed literature search, comprehensive list of outcomes, and appropriate use of evidence appraisal. There are also limitations to this study. First, no randomized studies were included in the meta-analysis, which reduced the quality of evidence. Evidence was graded as “low” or “very low” for most comparisons. Second, many studies failed to report important outcome data. Finally, the lack of consistency in the reporting of “juxtarenal,” “pararenal,” and “complex” aneurysms made it difficult to screen records for inclusion and extraction of data. The terms are used sporadically in the literature, often without accompanying definitions. 1 This may have led to indirectness and missed participants in this review. Efforts to agree upon more precise definitions of aortic anatomy or standardized reporting practices will lead to better quality comparative data. 32
Conclusions
This contemporary review compared the safety and efficacy of FEVAR and ChEVAR for management of JAA in adults. The results suggest that both procedures are safe and can be used when appropriate. The meta-analysis for the outcomes “technical success” and “avoidance of type 1 endoleaks” supports FEVAR as being more effective; however, superiority of either intervention cannot be established due to inherent differences in the baseline risk between arms. This challenges ESVS AAA Guidelines’ recommendation that FEVAR should be the preferred treatment option when feasible. 1 For the purposes of improving shared decision-making and in the absence of a prospective randomized trial, the UK-Complex Aneurysm Study (COMPASS) will seek to clarify the roles of open repair, endovascular techniques, and nonoperative management in this patient cohort. 12
Supplemental Material
sj-docx-1-jet-10.1177_15266028241231171 – Supplemental material for Systematic Review and Meta-analysis of Fenestrated and Chimney/Snorkel Techniques for Endovascular Repair of Juxtarenal Aortic Aneurysms
Supplemental material, sj-docx-1-jet-10.1177_15266028241231171 for Systematic Review and Meta-analysis of Fenestrated and Chimney/Snorkel Techniques for Endovascular Repair of Juxtarenal Aortic Aneurysms by Tejan Baldeh, Tomás Reilly, Tayyaub Mansoor, Gerard Feeney, Mekki Medani, Michael A. Moloney and Eamon G. Kavanagh in Journal of Endovascular Therapy
Supplemental Material
sj-docx-2-jet-10.1177_15266028241231171 – Supplemental material for Systematic Review and Meta-analysis of Fenestrated and Chimney/Snorkel Techniques for Endovascular Repair of Juxtarenal Aortic Aneurysms
Supplemental material, sj-docx-2-jet-10.1177_15266028241231171 for Systematic Review and Meta-analysis of Fenestrated and Chimney/Snorkel Techniques for Endovascular Repair of Juxtarenal Aortic Aneurysms by Tejan Baldeh, Tomás Reilly, Tayyaub Mansoor, Gerard Feeney, Mekki Medani, Michael A. Moloney and Eamon G. Kavanagh in Journal of Endovascular Therapy
Footnotes
Authors’ Note
Early results were presented as a poster at the Joint Annual Scientific meeting of the Irish Vascular Society and Northern Ireland Vascular Society, on Saturday November 6, 2021.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.