
Abstract
Optimal Medical Therapy (OMT) has been the accepted mode of treatment for uncomplicated Type B Aortic Dissection (uTBAD). There is growing evidence that despite the short-term benefits of OMT, patients suffer deleterious consequences in the long-term with OMT alone. Thoracic Endovascular Aortic Repair (TEVAR) along with OMT has emerged as an alternative option for patients with uTBAD. This study evaluates the available literature for TEVAR + OMT as an alternative to OMT for treatment of uTBAD. In addition, issues related to TEVAR as a treatment for uTBAD are discussed.
Keywords
Introduction
According to the Society for Vascular Surgery (SVS) and Society for Thoracic Surgeons (STS) reporting standards, complicated Type B Aortic Dissection (cTBAD) refers to a dissection with evidence of rupture or end-organ malperfusion. Patients without evidence of rupture or end-organ malperfusion are deemed as uncomplicated Type B Aortic Dissection (uTBAD). A subset of uTBAD is considered high-risk which include: refractory pain, refractory hypertension, or high-risk radiographic features. Another important factor is presenting chronicity. The definitions outlined in the SVS/STS reporting standards are maintained in this manuscript (hyperacute <24 hours, acute 1-14 days, subacute 15-90 days, and chronic >90 days). 1 This manuscript reviews the current understanding of uTBAD management.
Optimal medical therapy (OMT) is a management strategy to reduce aortic wall stress with aggressive blood pressure and heart rate control. Beta-blockers are most utilized, and vasodilators are a possible adjunctive option. In addition, medical therapy aims to control the acute pain. As a general rule, the goal heart rate should be < 70 beats/min and the systolic blood pressure should be < 120 mmHg. 2 Thoracic endovascular aortic repair (TEVAR) has emerged as the primary treatment of cTBAD over OMT and open surgery due to improved short and long-term outcomes.2,3 There are however significant risks with TEVAR including stroke (2.9%), 4 spinal cord ischemia (5%), 5 access site complications (2.8%), 6 and retrograde type A dissection (1.7%).3,7 Advancements in graft technology and operator experience have reduced these risks, but remain a consideration.
Traditionally, uTBAD are treated medically and only select patients receive TEVAR. However, as we follow these patients, it has become a point of contention if medical therapy alone is adequate for all patients with uTBAD. Here, we will explore what is known about OMT and TEVAR + OMT for treatment of uTBAD.
Results
There is limited research into treatment of aortic dissection and specifically very few randomized clinical trials evaluating treatment strategies. A core challenge to aortic dissection studies is that aortic dissections are a rare event with incidence of 3.5 per 100,000 persons per year. 8 Enrolling a significant number of patients in this setting generally requires a multi-institutional or international study. The International Registry of Acute Aortic Dissections (IRAD) database was established in 1996 to gather data from a consortium of institutions and attempt to answer some key questions about aortic dissections.
Evidence for OMT
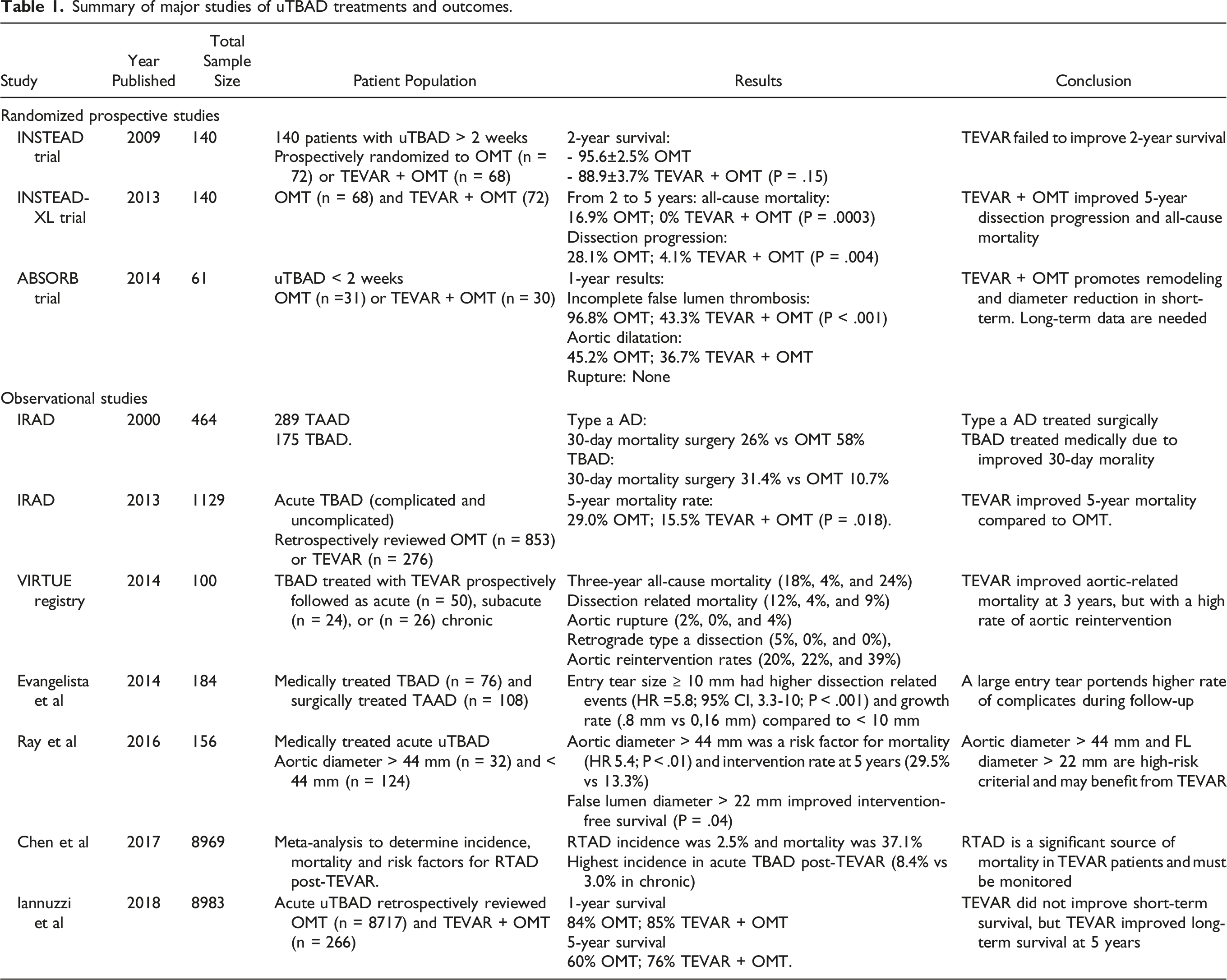
Initial evidence for OMT originated from the IRAD database published in the Journal of American Medical Association in 2000. In 175 TBAD patients, medical therapy resulted in a 30-day mortality of 10.7% compared to 31.4% in surgically treated patients. Of note, this study was completed in the era of open surgical management of TBAD, 9 as the first published report of TBAD with TEVAR was published in 1994. 10 The Investigation of Stent Grafts in Aortic Dissection (INSTEAD) trial, published in Circulation in 2009, cemented the paradigm of medical therapy only for TBAD. This study included 7 centers across Germany, France, and Italy and was the first to randomize patients with uTBAD for > 2 weeks to OMT or TEVAR + OMT. The group was able to enroll 140 patients, OMT (n = 72) or TEVAR + OMT (n = 68). The 2-year survival rates did not differ between groups (95.6 ± 2.5% OMT vs 88.9 ± 3.7% TEVAR + OMT, P = .15) with a 2.8% spinal cord injury rate for TEVAR patients. Additionally, the authors highlight that relatively few OMT patients (n = 11) required TEVAR due to continued aortic expansion. Lastly, 3 patients were converted to open surgery, showcasing the role of open surgery as a last resort (discussed in later section). 11 Based on these studies, the recommended treatment for uTBAD was OMT and close surveillance.
Guidelines for medical therapy for aortic dissection have been released by multiple cardiovascular societies across the globe with the goal of reducing aortic wall stress to promote aortic remodeling and false lumen thrombosis. In 2010, 10 international medical societies came together to publish guidelines on the diagnosis and management of thoracic aortic disease. 12 The suggested medical management of an acute thoracic aortic dissection is to obtain a goal heart rate < 60 bmp and SBP between 100-120 mmHg with intravenous beta-blockers, if not contraindicated. Non-dihydropyridine calcium channel blocking agents should be used as alternatives for rate control when beta-blockers are contraindicated. If systolic blood pressures continue to remain above 120 mmHg, it was recommended to start angiotensin-converting enzyme inhibitors and/or other vasodilators. It is often difficult to reach these targets with beta-blockers alone, and frequently multiple antihypertensive agents are initiated. These blood pressure parameters were echoed in the European Society of Cardiology recommendations for acute TBAD, which were published in 2014. 13 In addition, pain management is another essential component of acute TBAD treatment. Uncontrolled pain releases a sympathetic surge that elevates blood pressure and heart rate. Pain also induces patient anxiety which has a similar effect on vitals. Intravenous opiates, such as morphine sulfate, is the recommended choice to decrease pain in acute TBAD. 12
Numerous retrospective studies have analyzed the best medical therapy for chronic TBAD, but no large-scale RCT currently exists. Genoni et al initially showed the benefit of beta-blocker therapy (n = 51) compared to other antihypertensives (n = 20) in 71 patients with chronic TBAD. This study showed beta-blockers resulted in lower rates of increased aortic diameter (12% vs 40%, P = .002) and dissection-related surgery (28% vs 45%, P = .002). 14 In contrast, other recent studies have shown success with ACE inhibitors/angiotensin receptor blockers 15 and calcium channel blockers 16 compared to beta-blockers. Currently, beta-blockers are first line in the treatment of heart rate and blood pressure control for acute and chronic TBAD when not contraindicated, and ACE inhibitors/ARBs/CCB may be used as adjunctive agents to help reduce aortic shear wall stress and tension and support aortic remodeling. In summary, while the pharmacological management of uTBAD is currently suggested by expert opinion, the level of evidence is weak. 17
Evidence of TEVAR + OMT
While medical therapy was established as the standard of care for uTBAD from the results of IRAD database and the initial results of the INSTEAD trial, in 2013, the 5-year data of the INSTEAD-XL were published with surprising results. In 140 patients (TEVAR + OMT = 72, OMT = 68), TEVAR + OMT improved aorta-specific mortality (6.9% vs 19.3%; P = .04), dissection progression (27.0% vs 46.1%; P = .04), and trended towards improved all-cause mortality (1.1% vs 19.3%; P = .13) after 5 years follow-up. More importantly, the authors modified their initial recommendation from OMT to TEVAR + OMT due to improved late outcomes. 18
This was followed by the publication of the 20-year results from the IRAD database in 2018. The results of this study provided additional insight into the contemporary management of TBAD. Interestingly, the overall in-hospital mortality for TBAD remained 13%, which had not changed significantly over the study period. One third of this cohort presented as cTBAD, and OMT was the overall majority treatment modality ranging from 75% to 57%, while there was an increase in endovascular management during this time period from 7% to 31%. 19 Further insights from retrospective data in the IRAD (OMT = 853, TEVAR + OMT = 276) showed excellent short-term outcomes from medical therapy for uTBAD, but similarly to the INSTEAD trial, the long-term outcomes were poor with overall survival < 50%. Aneurysmal degeneration was as high as 60%. Moreover, TEVAR was protective with a lower mortality over 5 years compared to OMT alone. 19
For acute uTBAD, the Acute Dissection Stent Grafting or Best Medical Treatment (ADSORB) trial compared OMT to TEVAR + OMT. In this study, 31 patients were randomized to the OMT group and 30 patients to the OMT + TEVAR group. In a composite endpoint of false lumen thrombosis, aortic dilatation, and rupture, TEVAR + OMT was significantly more effective than OMT at 1-year. The results showed that the false lumen size had decreased in the TEVAR group at one year (P < .001), while in the OMT group it increased. Additionally, the overall transverse aortic diameter in the TEVAR group decreased at 1 year, while it remained stable in the OMT group. 20 While the trial was underpowered to assess mortality, these results suggest that TEVAR promotes aortic remodeling. Li Wei et al performed a similar prospective trial that evaluated 45 patients treated with OMT to 45 patients treated with OMT + TEVAR, and showed greater 1-year (75.6% vs 91.1%) and 2-year (66.7% vs 86.7%) survival rates in the OMT + TEVAR group (P < .05), with no difference in early complications. 21
Observational studies report similar favorable outcomes for TEVAR in acute uTBAD. Iannuzzi et al compared 8717 patients treated with OMT to 266 patients who underwent TEVAR in the California Office of Statewide Hospital Planning Development database. The results of their study found that TEVAR patients had similar 1-year survival to those treated with OMT (85% vs 84%), but improved 5-year survival (76% vs 60%, P < .01). 22
To define the optimal window for TEVAR repair, a multicentered, prospective trial called the VIRTUE Registry was performed to compare mid-term outcomes after TEVAR in acute (<15 days), subacute (15-92 days), and chronic (>92 days) phases of TBAD. 23 At 3-years, dissection related mortality was 12%, 4%, and 9% and aortic reintervention rates were 20%, 22%, and 39%, respectively. Moreover, the true lumen was significantly expanded after TEVAR, and the amount of false lumen area reduction was greater in acute and subacute groups compared to the chronic group. These findings support a treatment window for beneficial remodeling to include the acute and subacute phases. A metanalysis of 8969 total TBAD patients determined that TEVAR performed in the acute phase consisted of the highest rate of Retrograde Type A Dissection (RTAD) at 8.4% (26/309) compared to 3% (10/325) in chronic dissection. 24 Thus, it is reasonable to postpone TEVAR to the subacute phase in uTBAD when feasible. The optimal timing of intervention is critical and if possible, should be performed in the subacute phase of the dissection.
Numerous studies show that TEVAR promotes aortic remodeling, which may be the mechanism behind improved long-term outcomes compared to OMT alone. In fact, the INSTEAD trial showed aortic remodeling was observed in 91.3% of patients with TEVAR vs 19.4% of those who received OMT. 11 Moreover, TEVAR was shown to increase the true lumen percent area and concomitantly decrease the false lumen area in the thoracic aortic segment with effect down to the aortic bifurcation. 25 Likewise, Aoki et al introduced TEVAR (n = 26) for patients with a narrow true lumen (<50% of aortic diameter) and showed true lumen expansion up to 90% at 6 months without any significant perioperative complications. 26
The question then remains as to whether all patients with uTBAD should undergo TEVAR and which factors portend favorable outcomes with TEVAR, which some recent publications have sought to identify. Evangelista et al demonstrated that an entry tear ≥ 1 cm was associated with worse cumulative survival and higher incidence of dissection-related events in medically managed TBAD. 27 Another study showed partial thrombosis of the false lumen was associated with higher 3-year mortality rates in uTBAD patients on OMT alone. 28 In addition, Ray et al showed that aortic diameter > 44 mm or false lumen diameter > 22 mm was associated with decreased survival, while Matsushita et al showed that a ratio of false lumen to true lumen diameter > 1 on admission imaging predicted long-term incidence of aortic events for uTBAD patients.29,30
Summary of major studies of uTBAD treatments and outcomes.
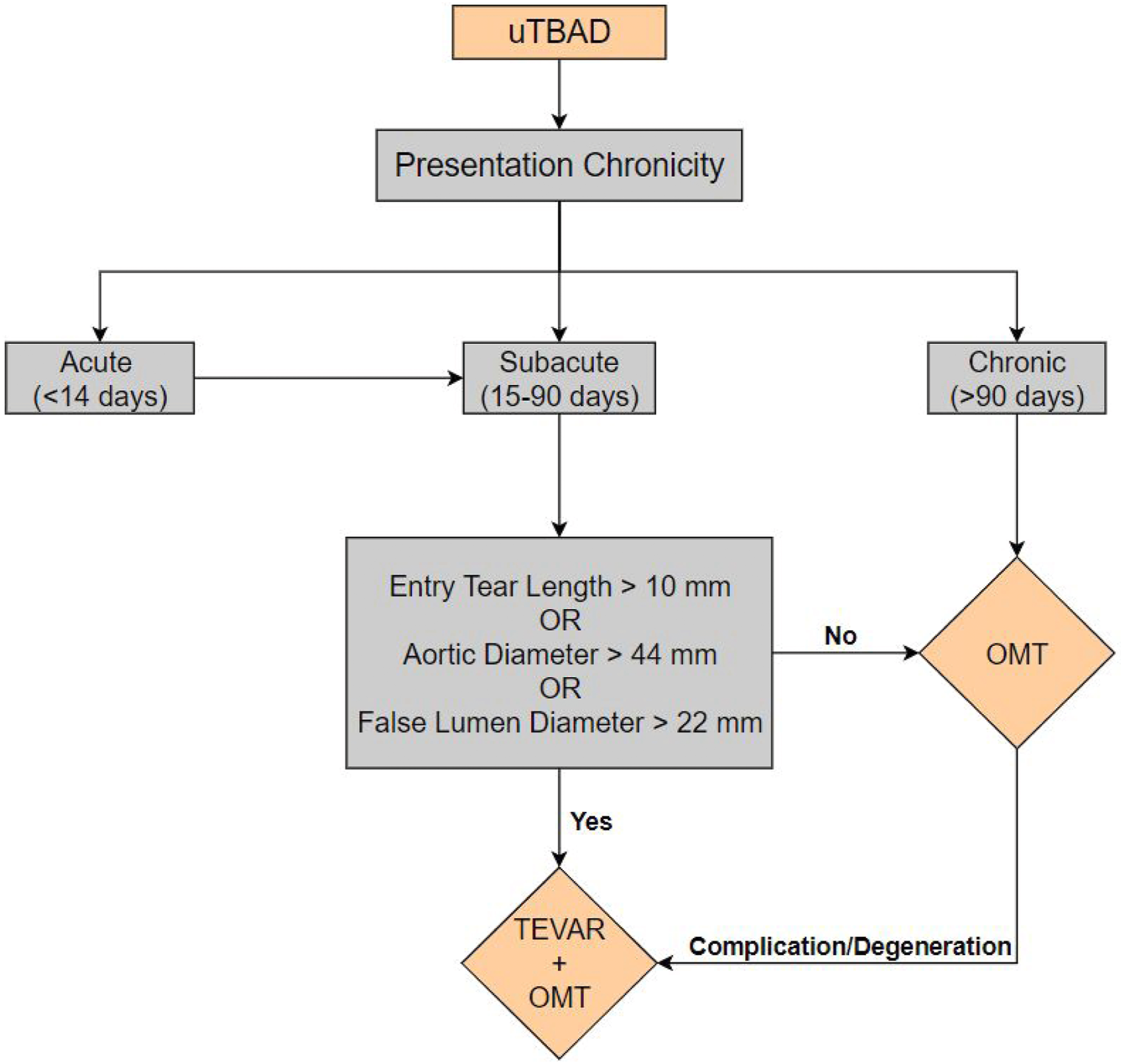
Algorithm for treatment of uTBAD with TEVAR + OMT vs OMT alone.
Limitations and Problems with TEVAR for uTBAD
TEVAR has possible complications that must be considered in the decision between medical therapy and TEVAR. In addition to access site complications, one devastating risk of TEVAR includes spinal cord injury and stroke which has been reported to be as high as 2.5-5%, and a major cause of morbidity and mortality. 5 Another procedure related complication includes stent graft-induced new entry (SINE) tears which are associated with an elevated mortality of 26.1%, and occurred in 22/650 TEVAR patients in one study (3.4% incidence). 31 Another study reported a SINE incidence of 7.9% in 1415 TEVARs, and all but one patient were successfully treated with endovascular management. 32 A significant complication of TBAD repair with TEVAR is retrograde type A aortic dissection (RTAD), which can lead to a catastrophic outcome. In 9894 TEVARs, RTAD was identified in 168 patients (1.7% incidence) with an elevated mortality rate of 33.6%. 7
In addition to short-term complications, long-term complications should also be considered, as endoleaks and type R entry flow have been reported to occur in 5-30% of TEVARs.33-35 Endoleak is a common occurrence that can be managed conservatively and observed for expansion but may also require intervention to prevent further degeneration of aorta leading to rupture. Endoleaks tend to prevent remodeling of the aorta. Type II endoleak can arise from the left subclavian artery (LSA), but can also be caused by intercostal and bronchial arteries. Type II endoleak from the LSA should be treated with embolization of the LSA at the time of initial operation if feasible. 36 A subsequent carotid LSA bypass may be necessary depending on patient symptoms. Sac embolization is another technique that can be used for type II endoleaks. Options to address Type R entry flow from a distal exit tear to prevent the progression of uTBAD include knickerbocker technique, Candyplug technique and Direct False Lumen embolization. The knickerbocker technique was developed to occlude the false lumen by rupturing the dissection membrane with a stent-graft. In one study of 16 patients, the knickerbocker technique had a success rate of 94%, and 9/12 patients showed aortic remodeling. 37 Another option is the Candy-Plug Technique which entails occlusion of the false lumen with an endovascular plug. In a study of 18 patients, this technique had a success rate of 100% and favored aortic remodeling as well. 38 Lastly the direct embolization can be achieved using large coils, plugs or a combination. 39 These techniques have yet to be tested in a large-scale, and require further investigation into their role in uTBAD treatment.
Data from IRAD reported an in-hospital mortality of 31.4% for patients treated with open surgical repair (OSR) for TBAD which has been largely supplanted by TEVAR. 9 Many argue that mortality in the contemporary era has improved with proper patient selection, better intensive care, and referral to high-volume centers. 40 Data from IRAD and a systemic review put the current in-hospital mortality from 7.5%-13.0% for OSR.41,42 OSR remains an option under certain circumstances such as chronic TBAD with aneurysmal degeneration despite TEVAR, anatomy unsuitable for TEVAR, impending rupture, and connective tissue disease. One study retrospectively reviewed OMT, TEVAR, and OSR for chronic TBAD and reported 7 cases where OSR was required post-TEVAR with a 3-year survival of 85.7%. 43 Thus, OSR remains a viable option in select patients.
In summary, since the first TEVAR for TBAD 23 years ago, there has been a significant increase in the number of patients with TBAD treated with TEVAR. The increasing numbers of TEVAR in uTBAD will be associated with some short term and long-term issues that may require secondary intervention. The patients who have TEVAR should have close surveillance with follow up imaging after TEVAR repair at 1 months, 6 months, and annually thereafter is recommended. 17
Discussion
The controversy of OMT vs TEVAR + OMT for uTBAD is difficult to address, and this manuscript highlights the current lack of large-scale data in uTBAD management. Current literature suggests an individualized approach to uTBAD with specific clinical and anatomic indications for TEVAR. From these studies, an uTBAD treatment algorithm was developed for optimal patient outcomes (Figure I).
In an era where healthcare costs are figured into the value of care in addition to the less certain long-term efficacy of newer costly devices, rigorous study is required to balance cost and the currently limited data on TEVAR benefit. Importantly, patient specific factors, which are often ignored in the equation of healthcare delivery should be considered in the treatment of aortic dissection. Factors to consider include patient understanding, socioeconomic status, addiction, and compliance with medical treatment. Often patients are noncompliant with blood pressure medications for financial, psychiatric, or physiologic reasons. In addition, many patients with TBAD are lost to follow-up, which could make OMT a less effective choice for long-term management and outcomes. 44 Physicians must consider the patient and their condition holistically and use best data available to determine the optimal course of treatment.
The understanding of uTBAD management is currently limited to small, randomized studies or retrospective data. A much larger multi centered randomized control trial of uTBAD with long term follow-up is required to determine the role of TEVAR on long-term outcomes. All uTBAD patients including high-risk features would be randomized to OMT or TEVAR + OMT in the acute or subacute phase (day 1-90) of dissection and followed for all-cause mortality, aortic-related mortality, malperfusion, new aortic tear requiring intervention, retrograde aortic dissection, conversion to TEVAR, and readmission for BP control or pain control. A subgroup analysis could be performed on patients converted to TEVAR, chronicity (acute vs subacute) and patients with high-risk features to assess many of the hypothesis summarized in this manuscript. The IMPROVE-AD (Improve Outcomes in Vascular Disease-Aortic Dissection) trial was designed to address this controversy and is expected to begin enrolling patients in the coming year.
Despite the recent guidelines released by the Society for Thoracic Surgeons and American Association for Thoracic Surgery as well as guidelines that are being written by Society for Vascular Surgery, it is clear that the level of evidence for treatment of uTBAD is weak and based on a few trials with limited data set. We need a multicenter randomized trial comparing OMT to TEVAR + OMT. A RCT would require significant funding and extensive collaboration, but would answer many of our questions in regards to treatment of uTBAD.
Conclusion
Although there is growing evidence that uTBAD should not be treated with OMT alone, the evidence for intervention, the quality of evidence, and the criteria for intervention is sparse. It is clear however that TEVAR will play a growing role in the treatment of uTBAD in the future. Current evidence seems to indicate that patients with entry tear greater than 1 cm in diameter, and false lumen diameter greater than 22 mm, and total aortic diameter greater than 44 mm have improved outcomes with TEVAR + OMT and should be considered for treatment. However, it is clear that further evidence-based studies are needed in this realm to determine treatment with TEVAR + OMT. We recommend a randomized multicentered longitudinal study to evaluate the safety and efficacy of these two treatment modalities.
Footnotes
Declaration of Conflicts of Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors claimed the following potential conflict of interest in regard to research, authorship and/or publication of this article: Babak Abai is a consultant for Cook Biomedical and Endologix.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.