
Abstract
Endovascular repair has gained acceptance for the treatment of arterio-ureteral fistula (AUF). However, data on associated postoperative complications are relatively scarce. We report the case of a 59-year-old woman with an external iliac artery (EIA)-ureteral fistula treated by endovascular stentgraft placement. Hematuria resolved after the procedure; however, occlusion of the left EIA and migration of the stentgraft into the bladder occurred 3 months postoperatively. Endovascular repair is a safe and effective method for the treatment of AUF, but it needs to be carefully followed. Extravascular migration of a stentgraft is a rare but possible complication.
Introduction
Endovascular stentgraft treatment has gained acceptance for the treatment of arterio-ureteral fistula (AUF). However, data on associated postoperative complications are relatively scarce. We herein report a rare case of stentgraft migration into the bladder after endovascular treatment of AUF. Written informed consent was obtained from the patient for the potential future use of patient information and images for research purposes.
Case Report
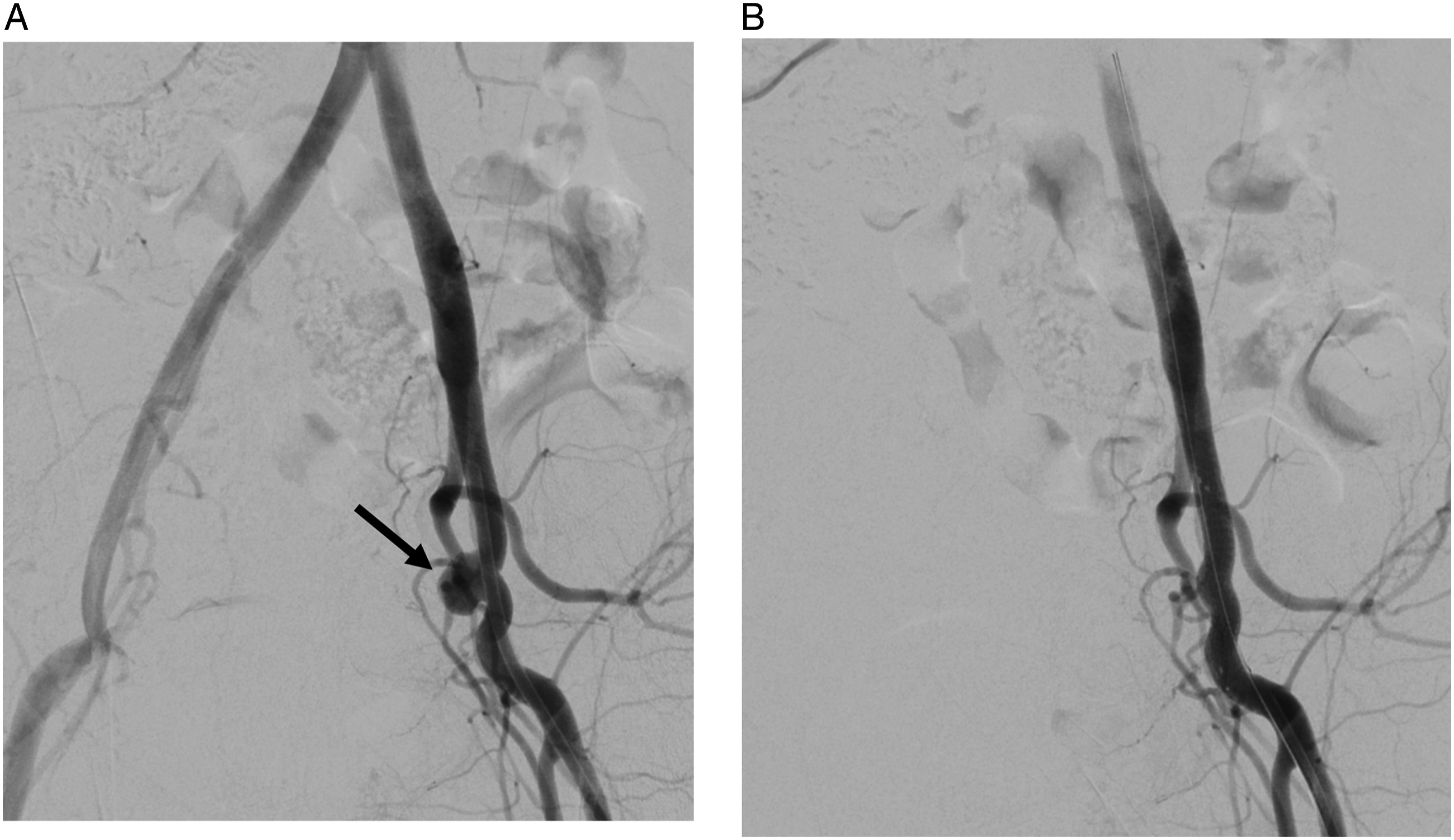
A 59-year-old woman presented to the emergency department with massive hematuria. The patient had a history of cervical cancer, which was treated by primary surgery and radiation therapy 16 years previously. Her clinical course after the treatment of cervical cancer was complicated by subsequent radiation proctitis, radiation cystitis, and adhesive intestinal obstruction. The laboratory findings on admission showed a hemoglobin level of 7.2 g/dL, a white blood cell (WBC) count of 10990/μL, and a C-reactive protein (CRP) level of 1.95 mg/dL. Computed tomography (CT) revealed a pseudoaneurysm in the left external iliac artery (EIA) adjacent to the ureter near the bladder (Figure 1), suggesting an AUF. The patient underwent urgent placement of an 8-mm×50-mm Viabahn stentgraft (W. L. Gore and Associates, Inc; Flagstaff, AZ, USA) in the left EIA (Figure 2). The device was chosen from among available off-the-shelf products and it was oversized by 20% compared with the diameter of the EIA. Both the proximal and distal landing zone lengths were approximately 20 mm. Her hematuria resolved after the procedure. The patient was also suspected of having an entero-vesical fistula because the presence of intravesical air was observed on CT. However, other investigations did not confirm its presence. The postoperative course was uneventful and the patient was discharged home on oral levofloxacin (500 mg once daily). As an antithrombotic therapy, aspirin (100 mg once daily) was given. At 2 months after the procedure, the patient presented with fever and fatigue. The laboratory findings at this point showed a hemoglobin level of 9.7 g/dL, a WBC count of 14310/μL, and a CRP level of 13.17 mg/dL. CT suggested a colo-vesical fistula and also showed diffuse stenosis of the left EIA (Figure 3). The diagnosis of rectosigmoid-vesical fistula was subsequently confirmed by means of colonoscopy, and the patient underwent transverse colostomy. CT performed 1 month later showed occlusion of the left EIA and migration of the distal part of the stentgraft into the bladder (Figure 4). The patient remained free from recurrent hematuria and did not exhibit lifestyle-limiting symptoms of limb ischemia. Considering her poor nutritional status and frailty, intervention for stentgraft migration was not performed. The patient died 6 months later from complications of complex entero-vesical fistula. An autopsy was not performed. (A) Axial and (B) coronal computed tomography images showing a pseudoaneurysm (arrow) in the left external iliac artery adjacent to the ureter near the bladder. (A) Intraoperative angiogram showing a pseudoaneurysm in the external iliac artery (arrow). (B) Angiogram obtained after stentgraft placement showing the disappearance of the pseudoaneurysm. Right anterior oblique maximum intensity projection computed tomography image at 2 months postoperatively showing stenosis of the left external iliac artery. (A) Axial and (B) coronal computed tomography images at 3 months postoperatively showing migration of the stentgraft (arrowhead) into the bladder.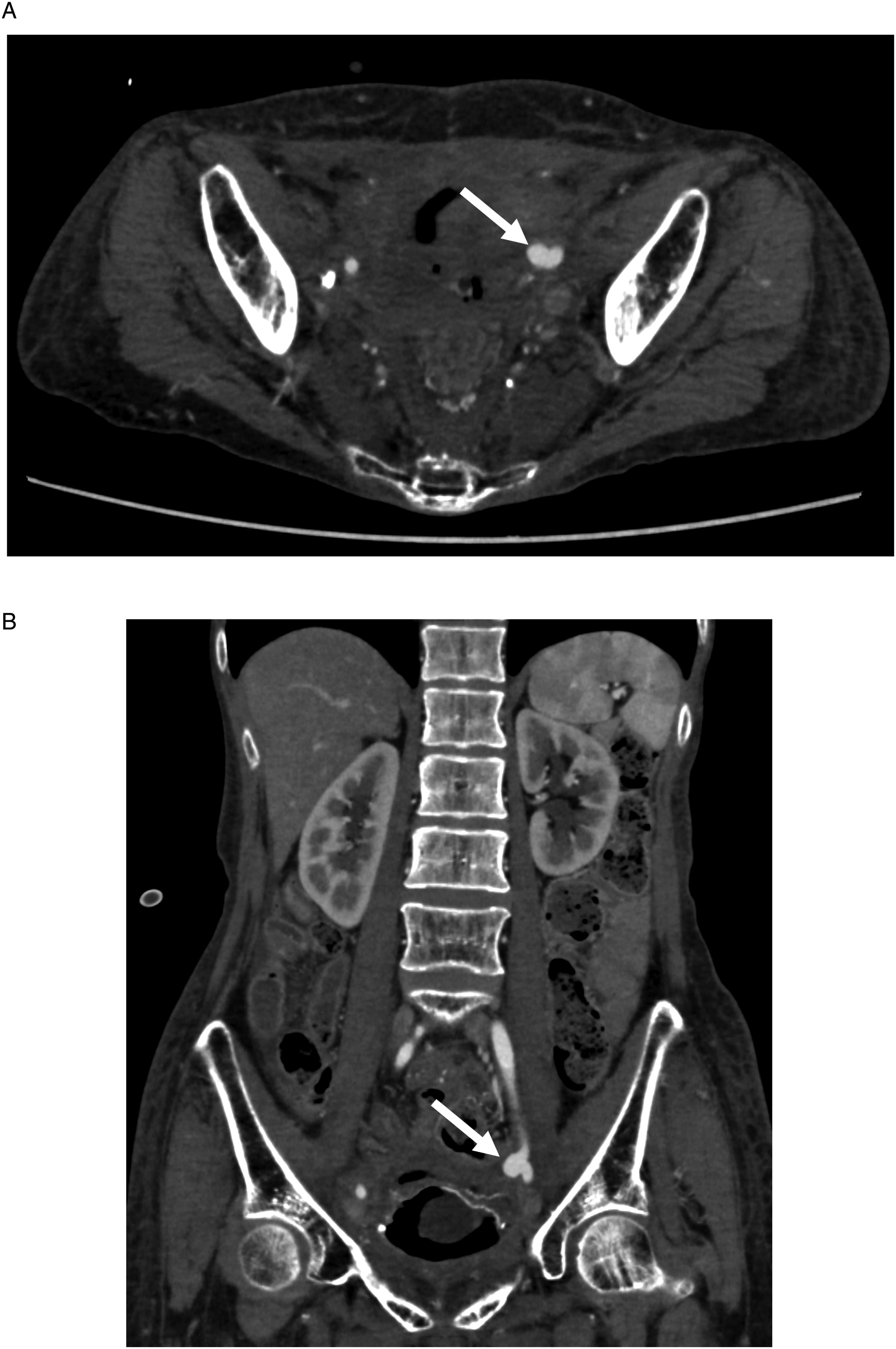


Discussion
AUF is a rare condition that can cause life-threatening massive hematuria. It usually occurs between the mid-to distal ureter and part of the iliac artery as a complication of indwelling ureteral stent placement, pelvic radiation therapy, or pelvic oncologic or vascular surgery. 1
For many years, open surgical reconstruction or direct repair of the involved segment of the artery combined with urologic treatment has been the standard treatment. In the last 2 decades, endovascular treatment has become the preferred treatment for AUF due to decreased early morbidity and mortality in comparison to conventional open repair.2,3 Endovascular treatment of AUF usually consists of stentgraft placement with/without internal iliac artery embolization. The advantages of the endovascular approach include avoidance of possible complications associated with open repair in a scarred operative field and the immediate control of hemorrhage in an unstable patient.
Despite these early advantages, there is currently little data on the mid- and long-term results of endovascular treatment of AUF.
In 2021, Simon et al 4 described 17 cases of AUF treated by endovascular treatment and reviewed 152 previously reported cases. They reported that the major complications specific to endovascular treatment included recurrence of hematuria, stentgraft occlusion, and infection. The incidence of these complications was 11.8%, 5%, and 3.6%, respectively. Secondary radical treatment including open arterial reconstruction, although not indicated in the present case because the patient was deemed unfit for open surgery, should therefore be considered for some cases. Extravascular migration of a stentgraft after the treatment of AUF is very rare, with only 1 case reported in the literature. Liang et al 5 reported the case of a patient who developed migration of a stentgraft into the bladder 18 months after the treatment of an AUF. They reported that thrombosis of the stentgraft preceded the migration by 6 months and that the patient was asymptomatic when stentgraft migration was detected on CT.
Although rare, there are several reports describing extravascular migration of stentgrafts placed for visceral artery disease. Tipaldi et al 6 reported 5 cases of extravascular migration of stentgrafts after endovascular treatment of visceral artery aneurysms or pseudoaneurysms, including 4 cases of hepatic or splenic artery pseudoaneurysms that formed in association with pancreatic surgery. The authors hypothesized that the most probable predisposing cause of this rare phenomenon was the loss of vessel wall integrity caused by an inflammatory microenvironment.
In the present case, diffuse stenosis of the EIA proximal and distal to the stentgraft was observed on CT 2 months after stentgraft placement, and stentgraft migration occurred 1 month later.
There are several potential explanations for these unusual findings in the present case, including (1) potential vascular damage from radiation therapy or severe perivascular inflammation may have caused diffuse stenosis of the EIA, leading to stentgraft thrombosis. Radiation-induced arterial stenosis is a late complication that can occur 10 years or more after radiotherapy. 7 (2) The fistula in the present case involved the distal ureter close to the bladder. Thus, a large fistula may have been created directly to the bladder that allowed the stentgraft to pass through.
In conclusion, endovascular treatment has become the mainstay of treatment for patients with AUF due to its improved short-term outcomes; however, it needs to be carefully followed. Extravascular migration of a stentgraft is a rare but possible complication, especially in patients with severe perivascular inflammation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.