
Abstract
Purpose
To establish a non-invasive test method for the rapid detection of severe ischemia (SI) in the limbs in patients with peripheral arterial disease (PAD).
Methods
Between November 2019 and May 2021, 22 patients admitted for PAD to 2 hospitals agreed to participate in the study. All patients underwent a local heating load (LHL) test. SI was defined as at least 1 ankle-brachial index value of <.4 and/or transcutaneous oximetry value of <30 mmHg. The other cases were classified as mild-to-moderate ischemia (MMI). The LHL test was performed simultaneously with 15 minutes of heating and measurement by attaching a blood flow meter measuring probe combined with a warmer to the patient’s dorsal foot. Evaluation consisted of 200-s periods from the start of heating to 800 seconds. For each period, perfusion value (PV) was evaluated, and slope was calculated graphically based on linear regression as PV fluctuation per minute. Test accuracy was calculated using a receiver operating characteristic curve.
Results
Twenty-four limbs of 18 patients were finally evaluated; 4 patients (2 with missing data, 1 with collagen disease, and 1 with embolism) were excluded, with 13 and 11 limbs in the SI and MMI groups, respectively. The SI group showed a significantly lower slope value in the first 200 seconds and lower PV at 200 seconds and thereafter. From the slope value, it was possible to detect SI with 85% sensitivity and 73% specificity at 200 seconds. PV could be determined with higher accuracy in periods after 200 seconds, with 85% sensitivity and 82% specificity at 800 seconds.
Conclusions
Our non-invasive LHL test could be used as a rapid screening test to detect SI in limbs within 200 seconds, as well as a more accurate test to detect ischemia within 800 seconds.
Keywords
Introduction
Chronic limb-threatening ischemia (CLTI) represents the end stage of peripheral arterial disease (PAD) with chronic insufficient tissue perfusion at rest and ischemic pain in the foot, non-healing wound, or gangrene. It is also associated with a high risk of mortality, amputation, and impaired quality of life in patients with PAD. 1 In the Global Vascular Guideline, 1 the severity of limb threat should be assessed in all patients with suspected CLTI using the Wounds, Ischemia, and foot Infection (WIfI) classification stages. 2 It is, therefore, essential to assess CLTI in ischemia using objective hemodynamic tests.
Conventionally, the ankle–brachial index (ABI), toe–brachial index (TBI), and transcutaneous oximetry (tcPO2) have been indicated as objective tools for evaluating limb perfusion. However, ABI is not suitable for patients with ABI values >1.4 due to incompressibility that can result in falsely increased readings, 1 TBI is difficult to evaluate in patients with toe ulcers, and tcPO2 requires a test time of 15-20 minutes; therefore, we conducted a study using thermal load tests to complement conventional tests. Using the thermal load test, we previously reported the usefulness of a transient blood flow increase observed after removing a local heated warmer to detect severe limb ischemia using a laser speckle contrasting imaging device3,4 or a skin-attached probe of the laser flow meter. 5 These studies used a tcPO2 probe or an 8-mm diameter warmer as the local heating device on the dorsal foot for 20 minutes and observed the blood flow fluctuations for 15 minutes after the removal of the warmer. With this method, it is not possible to evaluate the fluctuations in blood flow during heating because the tcPO2 probe itself, which acts as the warmer, blocks the laser light used for measurement. These tests have a high accuracy; however, the long test time and procedure to remove the warmer remain major challenges with these techniques.
In this study, to perform a simple procedure with a short test time, we measured fluctuations in blood flow during heating by integrating the warmer with the probe of the blood flow measuring device. The purpose of this pilot study was to establish a non-invasive test method for detecting severe ischemic limbs corresponding to WIfI ischemia classification 2 grade 3 in patients with PAD by observing blood flow fluctuations during a local heating load (LHL) test. Furthermore, we evaluated the reduction in test time compared to that of the previous thermal load tests.3-5
Material and Methods
Patients and Study Protocol
Between November 2019 and May 2021, 22 patients admitted for PAD to our vascular surgery unit at Tokyo Medical and Dental University and Tsuchiura Kyodo General Hospital agreed to participate in the study and were enrolled through a convenience sampling. In April 2022, the LHL test was conducted on healthy adults included as a control group. All patients underwent an LHL test of the dorsal foot. PAD was diagnosed based on an ABI of <.9 or >1.4. 1 In addition, PAD was diagnosed when ABI could not be tested due to pain from lower limb ischemia. Patients with an axillary temperature of >37.0°C; inflammatory diseases, such as collagen disease; infectious diseases; and leg ischemia due to emboli were excluded. All protocols, surveys, and consent forms were approved by the Institutional Review Board of Tokyo Medical (reference number M2019-246) and Dental University Hospital and Tsuchiura Kyodo Hospital (reference number 447). Written informed consent was obtained from all patients.
Severe ischemia (SI) in this study was defined as at least 1 ABI value of ≤.39 and/or tcPO2 value of <30 mmHg, as these indicate grade 3 ischemic cases according to the WIfI ischemia evaluation classification.
2
Mild-to-moderate ischemia (MMI) includes cases arrived at after excluding limbs with SI from among those diagnosed with PAD. The severity classification procedure used in this study is shown in Figure 1. We first classified the limbs according to the Rutherford category based on the clinical findings.
6
Limbs classified as Rutherford categories 1-3 were assessed for severity using the ABI test only. If the ABI could not be measured due to ABI being >1.4 or lower limb pain, the tcPO2 test was used. Limbs classified as Rutherford categories 4-6 were evaluated by using 2 tests: ABI and tcPO2. ABI was measured using the Doppler method,
1
with the patient placed in the supine position. If the Doppler sound could neither be detected in the dorsalis pedis artery nor the posterior tibial artery, the ABI value was set to zero. TcPO2 was measured according to the instructions specified in the user manual of the monitoring device (TCM400™, Radiometer Medical, Inc, Copenhagen, Denmark). Flow chart of the severity classification procedure in this study.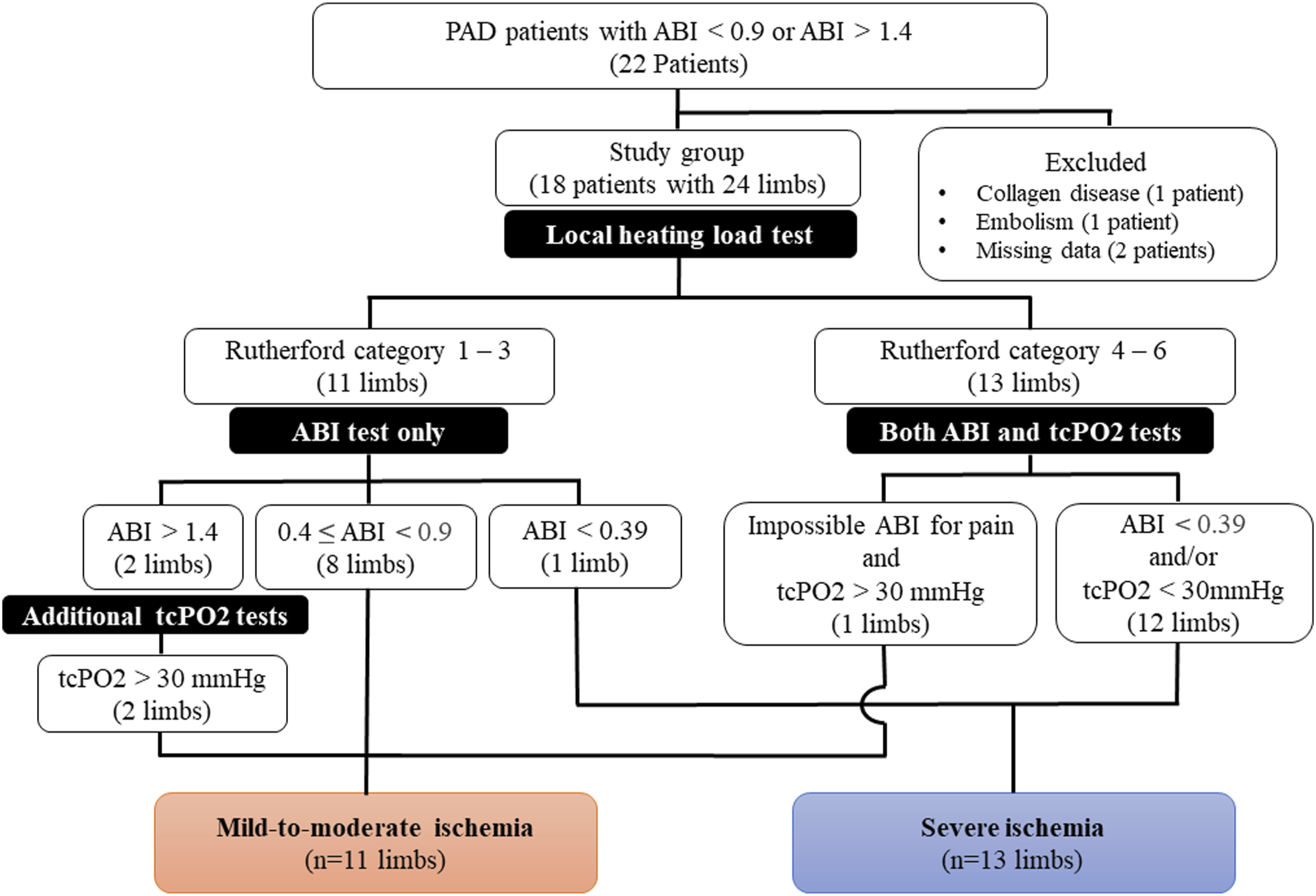
Measurements
We measured the blood flow fluctuation during local heating by combining the warmer and the probe of the blood flow measuring device into a single unit. For the warmer, we used a medical electric moxibustion device for local hyperthermia therapy (Shouki E09-04 TM, Zeniryoki Co., Ltd., Fukuoka, Japan). The heating part of the warmer had a diameter of 8 mm that adheres to the skin and was composed of a transparent glass plate that allowed laser light to pass through. The warmer was heated to 48°C by intermittently radiating it with far infrared rays with a wavelength of 8-10 μm for 30 seconds (heating for 15 seconds, off for 15 seconds) in 1 cycle. We then measured the tissue blood flow through the transparent glass plate by fixing the probe and warmer at a certain distance and by adjusting the intensity of the laser light from the probe of the fiber optic blood flow meter (Omegaflo-lab, Omegawave, Inc, Tokyo. Japan; Figure 2A). Local heating load test. (A) We measured the blood flow fluctuation during local heating by combining the medical electric moxibustion device as a warmer and the probe of a blood flow measuring device into a single unit. (B) The slope (PU/min) parameter was defined as the value of the blood flow fluctuations per minute during heating and obtained graphically from the linear regression in the 4 periods every 200 seconds from the start of local heating. Perfusion values (PVs) were recorded at rest and every 200 seconds from the start of heating.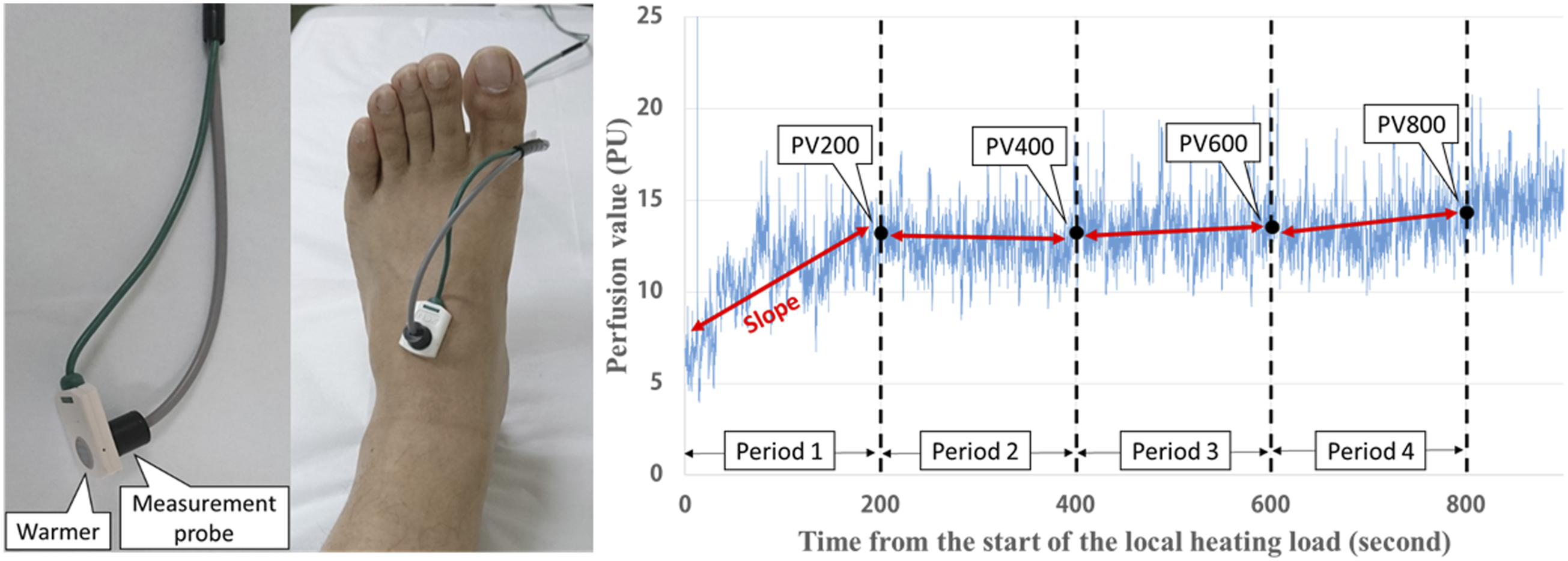
The LHL test was conducted at room temperature (21°C-25°C). The patient remained at rest in the supine position for 15 minutes. We attached the measuring probe combined with the warmer to the flat skin on the patient’s extensor digitorum brevis and extensor hallucis brevis in the proximal part of the dorsal foot (Figure 2A). This part is located slightly outside the dorsalis pedis artery. First, we measured the perfusion value at rest before heating with the same probe. At the same time, as the LHL was started by the warmer, the blood flow fluctuation was measured throughout for 15 minutes using the probe of the blood flow meter.
Data Analysis
Blood flow meter data can be expressed as arbitrary perfusion units (i.e., perfusion units [PU]) as a relative value corresponding to mL/min/100 g. 7 To evaluate the findings of the LHL test, 2 perfusion parameters were defined: slope (PU/min) and perfusion value (PV). The slope was calculated as the value of the blood flow fluctuation per minute during heating based on linear regression of the blood flow fluctuations plotted over time in an arbitrary period (Figure 2B). The slope was calculated for 4 200-s periods from the start of LHL: Period 1 (1-200 seconds), Period 2 (201-400 seconds), Period 3 (401-600 seconds), and Period 4 (601-800 seconds). The PV parameter was measured every 200 seconds from the start of LHL as PV200, PV400, PV600, and PV800. PV was calculated as the median value for 20 seconds before and after the evaluation time.
Statistical Analysis
Data are presented as medians with 25th and 75th percentiles for continuous variables and as percentages for categorical variables. To compare numerical data between the 2 groups, the Mann–Whitney U test was used for unpaired groups. Receiver operating characteristic (ROC) curves were plotted to evaluate the diagnostic value of the slope and PV in detecting severe limb ischemia with an ABI ≤.39 and/or a tcPO2 < 30 mmHg. The slope was calculated using a single linear regression model. Statistical significance was set at P < .05. The effect size was considered moderate or large if the r values were .3≤r<.5 or ≥.5, respectively, according to the Mann–Whitney U test. All statistical analyses were performed using SPSS software (version 20.0, IBM Corp, Armonk, NY, USA).
Results
Patient Characteristics
Patient Characteristics.
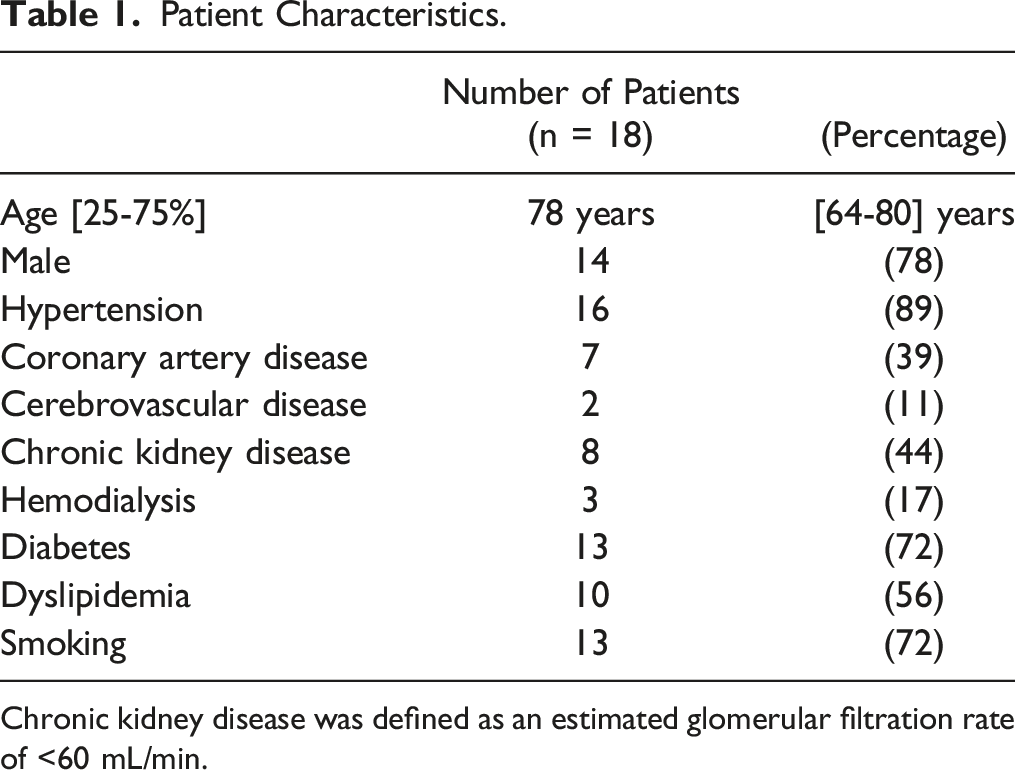
Chronic kidney disease was defined as an estimated glomerular filtration rate of <60 mL/min.
The Rutherford Category and the ABI and tcPO2 Values in Each Group.
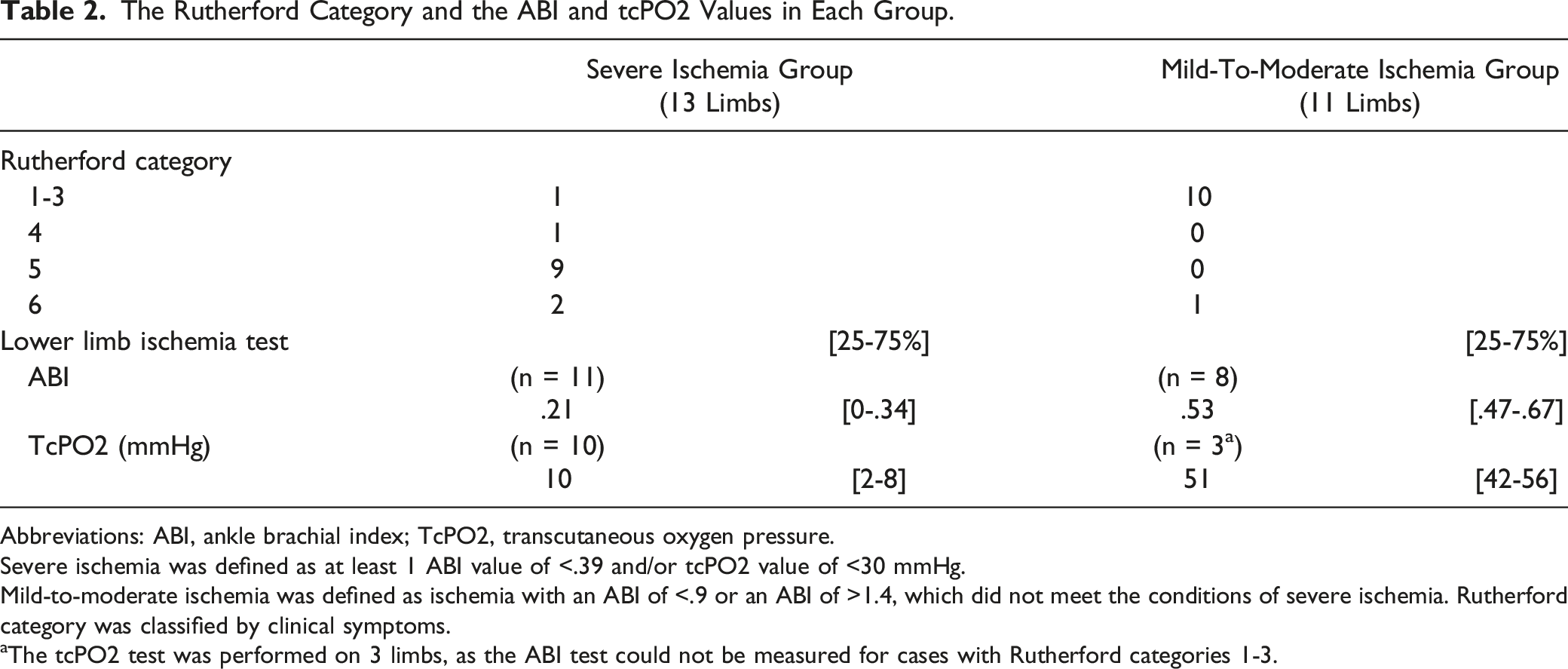
Abbreviations: ABI, ankle brachial index; TcPO2, transcutaneous oxygen pressure.
Severe ischemia was defined as at least 1 ABI value of <.39 and/or tcPO2 value of <30 mmHg.
Mild-to-moderate ischemia was defined as ischemia with an ABI of <.9 or an ABI of >1.4, which did not meet the conditions of severe ischemia. Rutherford category was classified by clinical symptoms.
aThe tcPO2 test was performed on 3 limbs, as the ABI test could not be measured for cases with Rutherford categories 1-3.
Local Heating Load Test
Comparison of Slope and Perfusion Value Parameters Between the Severe Ischemia, Mild-to-Moderate ischemia, and control groups in each period and at the evaluation time.
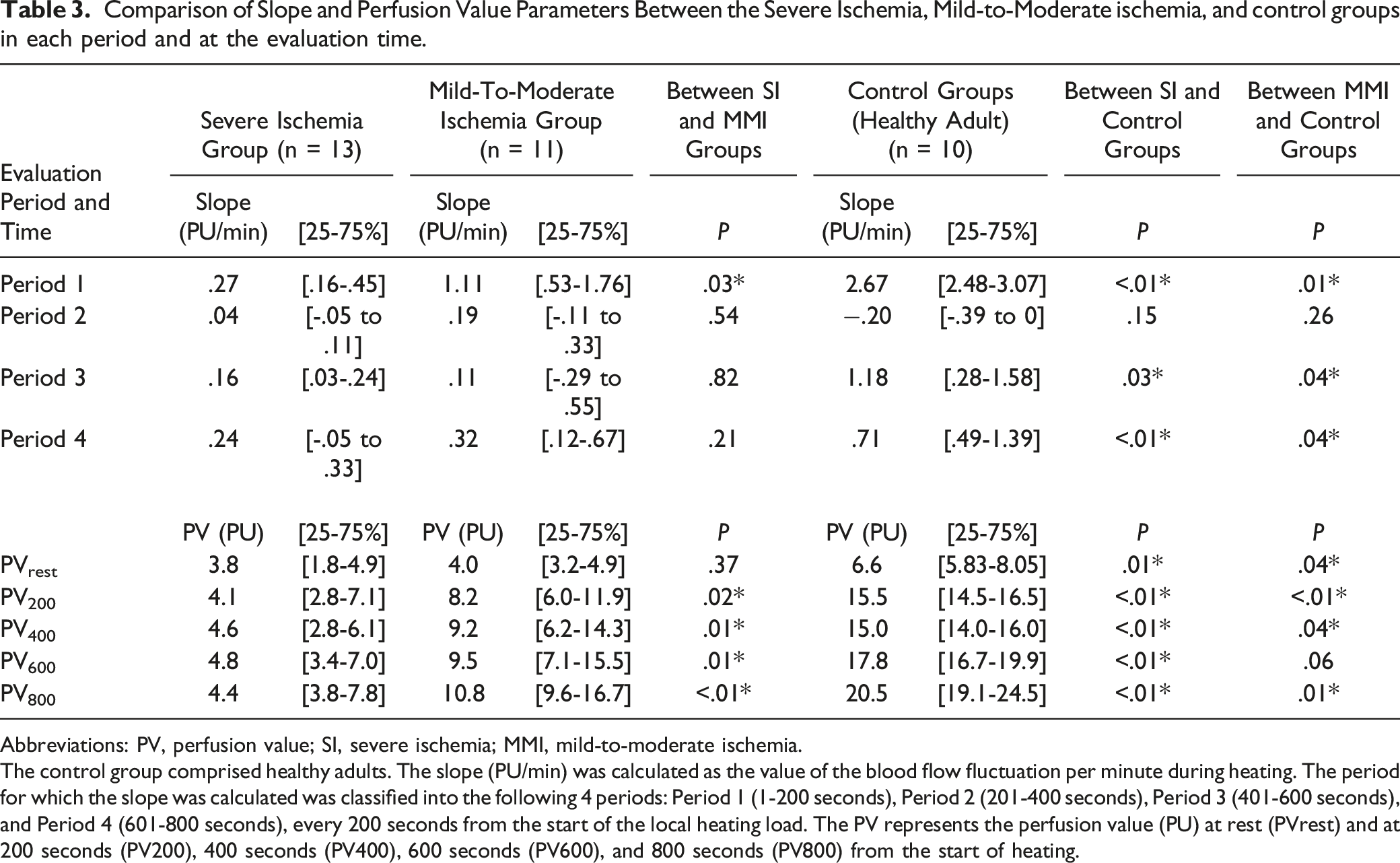
Abbreviations: PV, perfusion value; SI, severe ischemia; MMI, mild-to-moderate ischemia.
The control group comprised healthy adults. The slope (PU/min) was calculated as the value of the blood flow fluctuation per minute during heating. The period for which the slope was calculated was classified into the following 4 periods: Period 1 (1-200 seconds), Period 2 (201-400 seconds), Period 3 (401-600 seconds), and Period 4 (601-800 seconds), every 200 seconds from the start of the local heating load. The PV represents the perfusion value (PU) at rest (PVrest) and at 200 seconds (PV200), 400 seconds (PV400), 600 seconds (PV600), and 800 seconds (PV800) from the start of heating.
Receiver Operating Characteristic Curve
Receiver Operating Characteristic Curves of the Slope and Perfusion Value for Discrimination of Severe Limb Ischemia in Each Period and at the Evaluation Time.
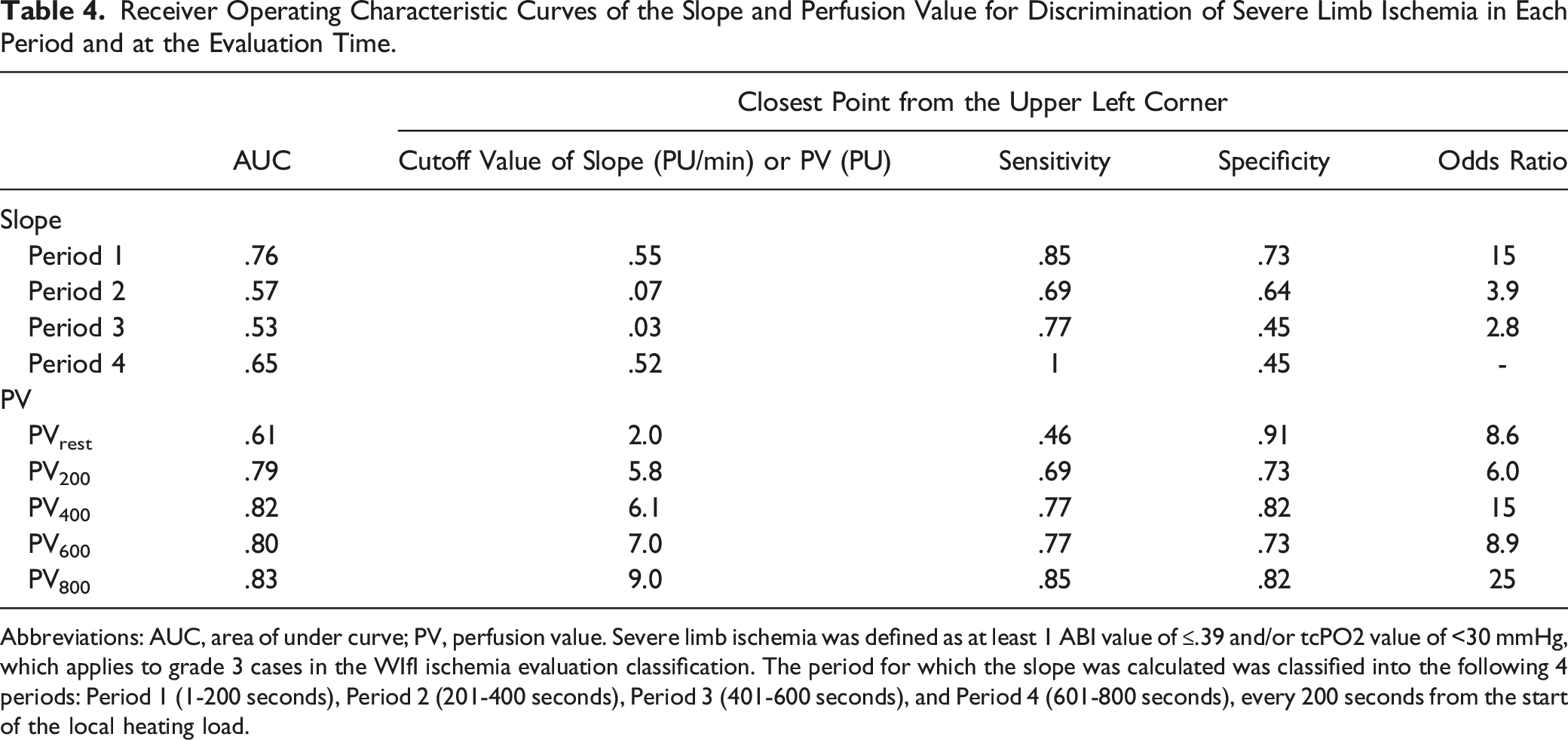
Abbreviations: AUC, area of under curve; PV, perfusion value. Severe limb ischemia was defined as at least 1 ABI value of ≤.39 and/or tcPO2 value of <30 mmHg, which applies to grade 3 cases in the WIfI ischemia evaluation classification. The period for which the slope was calculated was classified into the following 4 periods: Period 1 (1-200 seconds), Period 2 (201-400 seconds), Period 3 (401-600 seconds), and Period 4 (601-800 seconds), every 200 seconds from the start of the local heating load.
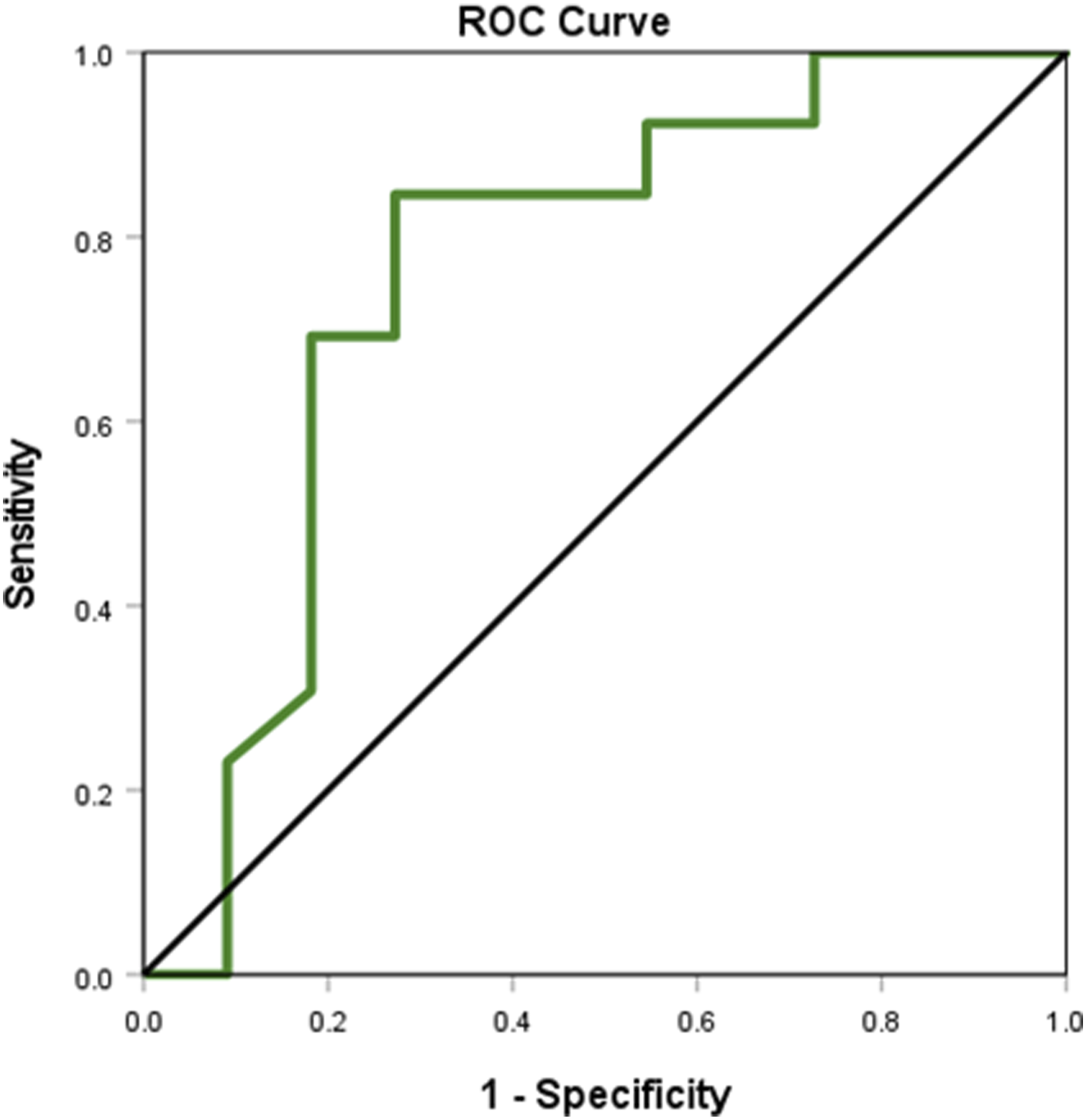
Receiver operating characteristic curve for the slope parameter in the first 200 seconds. Receiver operating characteristic curve by the slope parameter to detect severe limb ischemia in the period from the start of local heating to 200 seconds.
Of the 23 limbs, excluding 1 limb that could not be evaluated due to contrast agent allergy, 13 limbs showed obstruction of the dorsalis pedis artery (8 in the SI group and 5 in the MMI group). Within the dorsal pedis artery occlusion subgroup, the sensitivity and specificity for detecting the SI group calculated by the ROC curve for typical parameters were .88 and .60 for the slope of Period 1, .75 and 1.0 for the PV200, and .88 and .80 for the PV800, respectively.
Discussion
In this study, the SI group showed significantly lower slope values than the MMI group during the period from the start of LHL to 200 second, and lower PV at 200 seconds and thereafter. According to the ROC curve, the slope was able to detect SI with a sensitivity of 85% and a specificity of 73% at 200 seconds. Regarding PV, the test accuracy tended to increase over time after 200 seconds and was the highest at the final evaluation time of 800 seconds. In the thermal load test that we reported earlier, the test had a high accuracy with a sensitivity of 78.7%, specificity of 96.2%, and AUC of .91. 3 However, after local heating, the test itself takes >30 minutes,3-5 whereas the conventional tcPO2 test takes approximately 15 to 20 minutes. On the basis of our findings, we speculate that our non-invasive LHL test could be used as a rapid screening test for patients with suspected severe limb ischemia. For rapid screening, the slope and PV can be evaluated within 200 s, and for more accurate results, PVs can be evaluated within 800 seconds.
The slope value was the highest in Period 1, dropped sharply in Period 2, and then gradually increased. In previous reports that evaluated blood flow fluctuations after local heating of the upper limb, the first peak was reached approximately 200 seconds after the start of heating, and a gradual increase was observed thereafter. 8 These blood flow fluctuations are very similar to the results from our LHL test. It is commonly believed that the skin blood flow response to the LHL is mediated by at least 2 independent phases: the initial rapid phase is predominantly mediated by local sensory nerves, and the late phase is mediated predominantly by locally produced chemical factors, such as nitric oxide.9,10
The group defined here as SI corresponds to cases with stage 3 ischemia according to the WIfI classification. 2 This is a very serious ischemic condition that corresponds to tcPO2 of <30 mmHg and ankle pressure of 50 mmHg (70 mmHg in patients with ulcers), which is the standard criterion of critical limb ischemia (CLI) according to the Trans-Atlantic Inter-Society Consensus II classification that was announced in 2007. 11 With this level of CLI, arterioles, namely resistant blood vessels, are maximally dilated to reduce vascular resistance for ensuring blood flow to the ischemic site. 12 Therefore, it is presumed that a poor reserve capacity for vascular response to LHL slightly increases the blood flow. Conversely, the cases in the MMI group, namely claudication limbs, such as Rutherford category 1-3 ischemic cases, are presumed to have sufficient reserve capacity to respond to increased blood flow by LHL in a resting state. Therefore, it is believed that differences in the ischemic status between the SI and MMI groups appear as differences in blood flow fluctuation during the LHL test, rather than as differences in PV at rest.
This study has certain limitations. First was the small sample size. Nevertheless, our study demonstrated that the LHL test can provide a quantitative assessment of ischemic lower limbs. Second, this study did not include patients with any fever, such as those with systemic infection. These patients may show increased skin blood flow at rest, and the effects of LHL may be diminished in such cases. Third, the coronavirus disease epidemic in Japan may have affected patient selection due to study suspension, prevented hospital visits/admissions for PAD, and reduced motivation for patients to participate in the study. However, this is a pilot study on the use of the LHL test for detecting severe ischemic limbs. Further research with larger sample sizes, including patients with fever, is therefore needed to resolve these limitations.
Conclusion
We have made it possible to evaluate blood flow fluctuation during LHL by combining a warmer device and a blood flow measurement probe into a single unit. In the non-invasive LHL test, severe limb ischemia, corresponding to grade 3 in the WIfI ischemia classification system, could be detected based on the slope parameter with a high accuracy, 85% sensitivity, and 73% specificity at 200 seconds after the start of local heating. Furthermore, SI could be detected with higher accuracy after 200 seconds using the PV parameter. Thus, we believe that our non-invasive LHL test could be used as a rapid screening test as well as a more accurate test for patients with suspected severe limb ischemia. For rapid screening, the slope and PV can be evaluated within 200 seconds, and for more accurate results, PVs can be evaluated within 800 seconds.
Footnotes
Acknowledgments
The authors are grateful to Dr. Yoshinori Inoue (Ambulatory Vascular Surgical Clinic Tokyo) for his kind support for this research.
Author Contributions
S.K. conceived and designed the study and performed the analysis and prepared the manuscript. S.K. and Y.Y. collected and interpreted the data. All authors performed the research, discussed the results, and contributed to the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.