
Abstract
Purpose:
Endovascular revascularization is the preferred treatment to improve perfusion of the lower extremity in patients with chronic limb-threatening ischemia (CLTI). Patients with CLTI often present with stenotic-occlusive lesions involving the infrapopliteal arteries. Although the frequency of treating infrapopliteal lesions is increasing, the reintervention rates remain high. This study aimed to determine the outcomes and patency of infrapopliteal endovascular reinterventions.
Methods:
This retrospective, multicenter cohort study of 3 Dutch hospitals included patients who underwent an endovascular infrapopliteal reintervention in 2015 up to 2021 after a primary infrapopliteal intervention for CLTI. The outcome measures after the reintervention procedures included technical success rate, the mortality rate and complication rate (any deviation from the normal postinterventional course) at 30 days, overall survival, amputation-free survival (AFS), freedom from major amputation, major adverse limb event (MALE), and recurrent reinterventions (a reintervention following the infrapopliteal reintervention). Cox proportional hazard models were used to determine risk factors for AFS and freedom from major amputation or recurrent reintervention.
Results:
Eighty-one patients with CLTI were included. A total of 87 limbs underwent an infrapopliteal reintervention in which 122 lesions were treated. Technical success was achieved in 99 lesions (81%). The 30-day mortality rate was 1%, and the complication rate was 13%. Overall survival and AFS at 1 year were 69% (95% confidence interval [CI], 55%–79%) and 54% (95% CI, 37%–67%), respectively, and those at 2.5 years were 45% (95% CI, 33%–56%) and 21% (95% CI, 11%–33%), respectively. Freedom from major amputation, MALE, and recurrent reinterventions at 1 year and 2.5 years were 59% (95% CI, 46%–70%) and 41% (95% CI, 25%–56%); 54% (95% CI, 41%–65%) and 36% (95% CI, 21%–51%); and 68% (95% CI, 55%–78%) and 51% (95% CI, 33%–66%), respectively. A Global Limb Anatomic Staging System score of III showed an increased hazard ratio of 2.559 (95% CI, 1.078–6.072; p=0.033) for freedom of major amputation or recurrent reintervention.
Conclusions:
The results of this study indicate that endovascular infrapopliteal reinterventions can be performed with acceptable 30-day mortality and complication rates. However, outcomes and patency were moderate to poor, with low AFS, high rates of major amputations, and recurrent reinterventions.
Clinical Impact
This multicenter retrospective study evaluating outcome and patency of endovascular infrapopliteal reinterventions for CLTI, shows that endovascular infrapopliteal reinterventions can be performed with acceptable 30-day mortality and complication rates. However, the short- and mid-term outcomes of the infrapopliteal reinterventions were moderate to poor, with low rates of AFS and a high need for recurrent reinterventions. While the frequency of performing infrapopliteal reinterventions is increasing with additional growing complexity of the disease, alternative treatment options such as venous bypass grafting or deep venous arterialization may be considered and should be studied in randomized controlled trials.
Keywords
Introduction
Endovascular revascularization is often performed in patients with chronic limb-threatening ischemia (CLTI) to restore blood flow to the lower extremity and foot.1,2 By increasing the perfusion of the lower limb with endovascular therapy (EVT), clinical symptoms, such as pain and nonhealing ulcers, can be improved, lowering the risks of major amputation and subsequent cardiovascular mortality.
With an aging population and the evolution of endovascular techniques, endovascular infrapopliteal reinterventions are increasingly performed. 3 Knowledge of the outcome of these reinterventions is therefore essential and may help in counseling patients who are scheduled for these procedures. Furthermore, it may help physicians in the decision-making process regarding the preferred treatment method to overcome infrapopliteal restenosis and reocclusions. Patients with CLTI frequently present with a complex multilevel arterial obstructive disease, including the infrapopliteal arteries. 4 Revascularization, specifically for infrapopliteal lesions, is primarily performed through percutaneous transluminal angioplasty (PTA).1,5,6 Various types of stents can also be used for the infrapopliteal disease if PTA alone is not sufficient.7 –9 Many studies report outcomes for different types of primary endovascular infrapopliteal revascularization and reveal high reintervention rates for all types of EVT, ranging from 11% to 30%, 10 and reintervention-free survival of only 15% to 26% after 5 years of follow-up. 11 However, the results of infrapopliteal endovascular reinterventions are underreported.
This study assessed the short-term and midterm outcomes and patency of endovascular infrapopliteal reinterventions in terms of technical success, mortality, complication, and survival rates. Moreover, freedom of amputation, major adverse limb event (MALE), and recurrent reinterventions at midterm follow-up were determined.
Materials and Methods
Study Design
This was a multicenter, retrospective cohort study of patients who underwent an infrapopliteal endovascular reintervention for CLTI in 1 of the 3 participating hospitals (ie, Maasstad Hospital Rotterdam, Martini Hospital Groningen, and the University Medical Center Groningen (UMCG)) in the Netherlands between March 2015 and April 2021. The study protocol was reviewed and approved by the institutional review board of the UMCG (IRB# 2018/024) and by the participating hospitals for local approval. The requirement for individual informed consent was waived due to the retrospective nature of the study. Study procedures were performed according to European privacy guidelines and according to the guidelines of the Declaration of Helsinki.
Patient Selection
Patients were eligible for inclusion if they were diagnosed with CLTI and underwent an infrapopliteal endovascular reintervention after a primary infrapopliteal intervention. Exclusion criteria were acute limb ischemia and absence of clinical, imaging, or procedural data. We screened all endovascular infrapopliteal endovascular interventions from March 2015 until April 2021 and selected all patients who underwent an infrapopliteal endovascular reintervention for CLTI.
A multidisciplinary team of vascular surgeons and interventional radiologists determined the indication for an infrapopliteal reintervention based on clinical evaluation, including physical examination, duplex ultrasound imaging, ankle-brachial index, and computed tomography angiography (CT-A). CT-A was available in all patients before reinterventions and was used to determine the presence of a distal patent tibial target artery. Patient demographics, clinical information, imaging studies, and follow-up data were retrieved from electronic data files. All patients received treatment and follow-up according to the standard of care based on global vascular guidelines.1,12
Endovascular Procedure
Infrapopliteal endovascular reinterventions were performed under local anesthesia in an angiography suite. The procedures were primarily performed using antegrade percutaneous common femoral artery access. Retrograde tibial or pedal access was sought when antegrade passage of the occlusion was not possible. The primary treatment aim was to obtain continuous arterial runoff to the foot through at least 1 below-the-knee artery. If possible, runoff through multiple arteries was sought, which was to the discretion of the treating physician. Target lesions were treated with PTA and with additional stent placement in case of acute recoil, flow-limiting dissections, or >30% residual stenosis measured on angiography. 13 Technical success of the target lesion revascularization (TLR) was defined as <30% residual stenosis present on the completion angiogram examined by the performing interventionalist.14,15
All treated limbs were retrospectively classified according to the Global Limb Anatomic Staging System (GLASS). 1 Furthermore, the treated limbs were scored according to the TransAtlantic Inter-Society Consensus for Management of Peripheral Arterial Disease classification for infrapopliteal disease. 12 Both classifications were performed by 3 experienced vascular specialists from the 3 participating centers individually (B.F., C.G.V., and G.C.B.), and in all limbs, consensus was reached.
Outcome Measures
The technical success rate was assessed for each individual lesion. The outcome measures were the patients’ 30-day mortality rate and complication rate (any deviation from the normal postinterventional course), overall survival, amputation-free survival (AFS, an end point that combines the outcomes of mortality and major amputation), freedom from major amputation (above the ankle), freedom from MALEs (defined as above-ankle amputation or major reintervention [bypass, interposition/jump graft revision, thrombectomy/thrombolysis]), 16 and freedom from recurrent revascularization procedures (a reintervention following the infrapopliteal reintervention).
Statistical Analysis
Data were analyzed using SPSS 23 statistical software (IBM Corp, Armonk, NY, USA). Patient and procedural characteristics are presented as means and standard deviations or as medians and 25th and 75th percentiles for continuous variables according to data distribution and as counts and percentages for categorical variables. Kaplan-Meier (KM) analyses were performed to determine the overall survival, AFS, freedom from major amputation, freedom from MALE, freedom from recurrent reintervention, and freedom from major amputation or recurrent reintervention. In the KM analysis, follow-up ended at the date of the diagnosis of the event or at the date of the last follow-up visit. All KM curves were terminated at 2.5 years so that the numbers at risk were not <10. Survival estimates are given with a 95% confidence interval (CI). Univariable and multivariable Cox regression proportional hazard models were used to determine the association between risk factors with AFS and freedom from major amputation or recurrent reintervention. The included number of variables was limited to 1 per 10 events; anatomical factors and patient-related risk factors were chosen. For all statistical analyses, a p value of ≤0.05 was considered statistically significant.
Results
The study included 81 patients. In the 81 patients, 87 limbs underwent an endovascular infrapopliteal reintervention. Six patients underwent an endovascular reintervention in both limbs, which were performed on different days. An overview of the patient characteristics at the time of the endovascular reintervention is presented in Table 1.
Patient Characteristics at the Time of Infrapopliteal Reintervention.
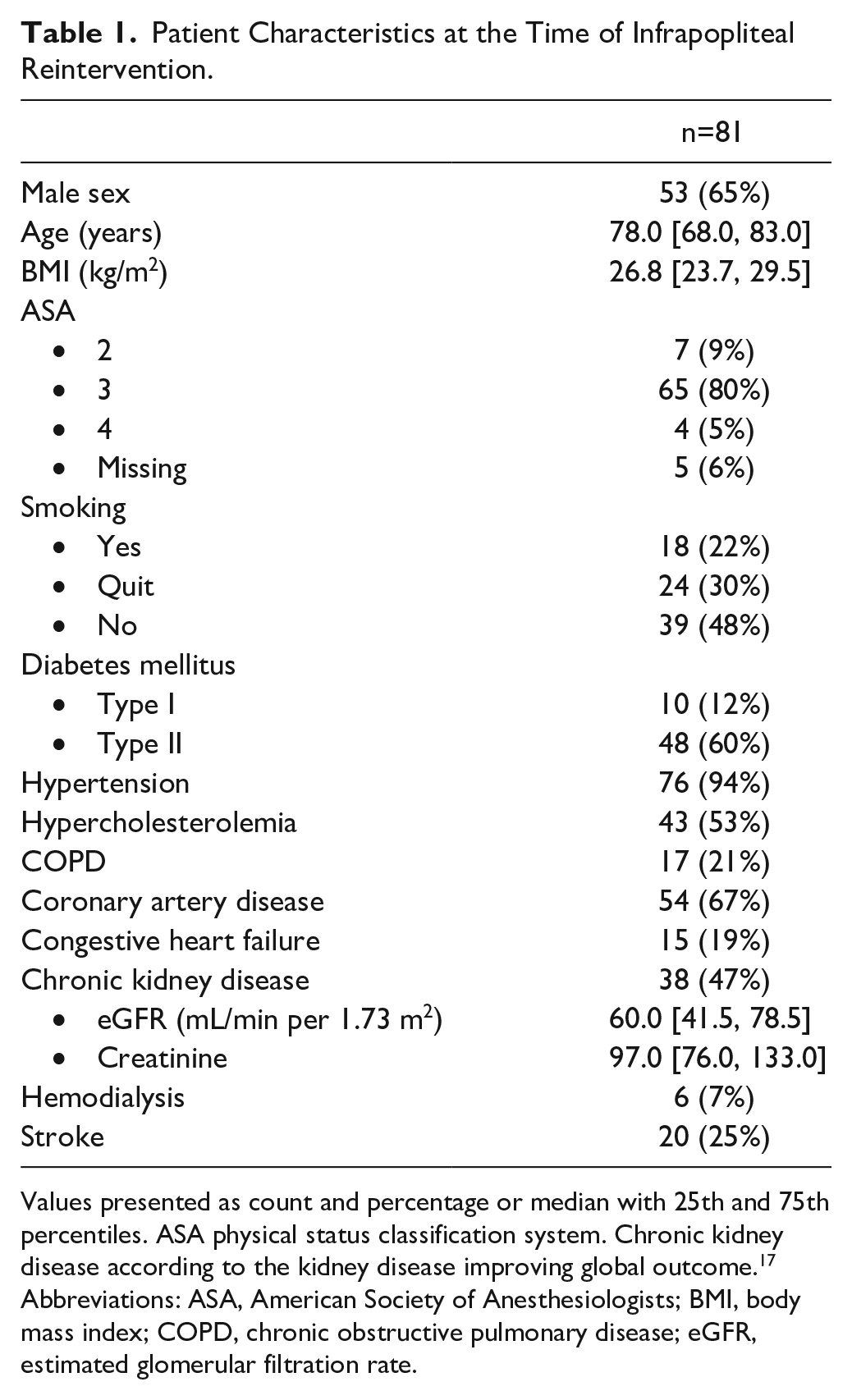
Values presented as count and percentage or median with 25th and 75th percentiles. ASA physical status classification system. Chronic kidney disease according to the kidney disease improving global outcome. 17
Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; COPD, chronic obstructive pulmonary disease; eGFR, estimated glomerular filtration rate.
Procedural Characteristics
Table 2 reports the procedural characteristics of the infrapopliteal reinterventions performed in this study. Of the 87 limbs that underwent a reintervention, 80 (92%) were classified as Fontaine IV. During the reintervention, TLR (according to the primary treated lesion) was performed in 59 limbs (68%), and in 15 limbs (17%), TLR was combined with endovascular treatment of an additional infrapopliteal lesion. Reintervention in 13 limbs (15%) was performed in an infrapopliteal artery other than the one with the target lesion of the primary endovascular procedure, however in the same limb. An example of angiograms before and after the revascularization of a single lesion treated is shown in Supplementary Figure 1. The primary endovascular interventions were performed to treat 132 infrapopliteal lesions. These lesions were treated with either PTA (88%) or PTA with stent placement (12%). The median time between primary intervention and reintervention was 4.6 months (25th and 75th percentile, 1.4 and 8.1 months, respectively).
Preprocedural and Procedural Characteristics.
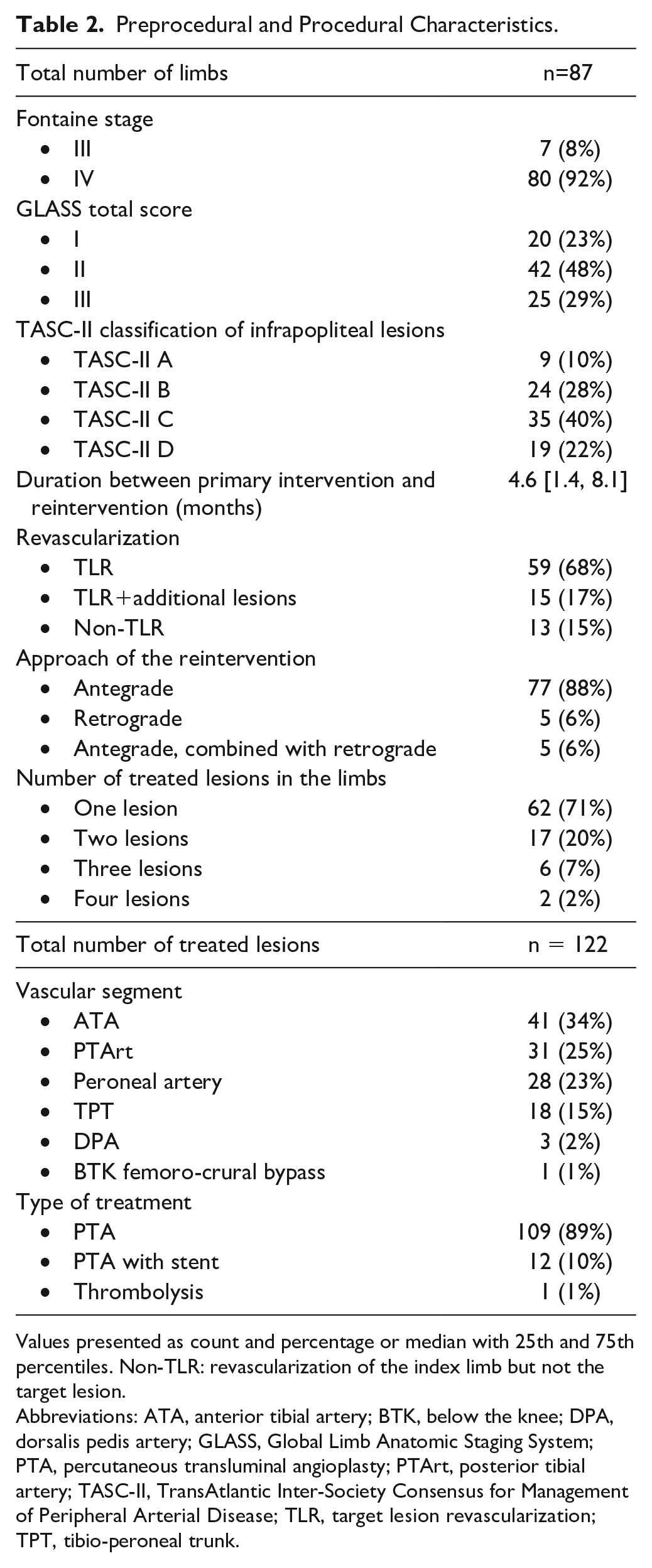
Values presented as count and percentage or median with 25th and 75th percentiles. Non-TLR: revascularization of the index limb but not the target lesion.
Abbreviations: ATA, anterior tibial artery; BTK, below the knee; DPA, dorsalis pedis artery; GLASS, Global Limb Anatomic Staging System; PTA, percutaneous transluminal angioplasty; PTArt, posterior tibial artery; TASC-II, TransAtlantic Inter-Society Consensus for Management of Peripheral Arterial Disease; TLR, target lesion revascularization; TPT, tibio-peroneal trunk.
Technical Success and Mortality and Complication Rates of Infrapopliteal Reinterventions
Of the 122 lesions treated in 87 limbs, technical success was obtained in 99 lesions (81%). In the 23 lesions (19%) in which technical success was not obtained, it was not possible to pass the stenosis or occlusion with any wire in 15 lesions, a residual stenosis of >30% remained after several attempts of PTA without the possibility to deploy a stent in 4 lesions, there was no outflow artery present distal from the lesion in 3 lesions, and the EVT was terminated early because of chest pain and dyspnea in 1 case.
The 30-day mortality rate was 1%. One patient died of an unknown reason 12 days after the reintervention and 6 days after discharge. The 30-day complication rate was 13% (11 of 87 limbs). Four procedure-related complications occurred. In 2 cases, there was postprocedural bleeding of the puncture site; in 1 case, there was migration of the Angio-Seal (Terumo, Somerset, NJ, USA) that occluded the superficial femoral artery, for which the patient underwent an exploration for removal of the Angio-Seal; and in 1 case, there was a false aneurysm at the puncture site. Another 7 complications occurred within this cohort: five cases of infection in ≤30 days, including urinary tract infections (n=2), pneumonia (n=1), cellulitis (n=2), and 2 cases of transient renal dysfunction, without the need for dialysis.
The 30-day readmission rate for disease progression was 18% (16 of 87). These readmissions were indicated because of deterioration of ulceration and necrosis for which an additional revascularization (n=2), minor amputation (n=8), or major amputation (n=6) was needed.
Outcomes and Patency After Infrapopliteal Reinterventions
The median follow-up duration after the endovascular reintervention was 292 days (25th and 75th percentile: 136 and 727 days, respectively). Twenty-six patients (32%) died during follow-up. The causes of death were unknown in 14 patients, cardiac failure in 4 patients, urosepsis or pneumosepsis in 2 patients, multiple organ failure in 2 patients, malignancy in 2 patients, stroke in 1 patient, and a rupture of the aortic arch in 1 patient. Estimated patient survival at 1 year and 2.5 years was 69% (95% CI, 55%–79%) and 54% (95% CI, 37%–67%), respectively (Figure 1). The estimated AFS at 1 year and 2.5 years was 45% (95% CI, 33%–56%) and 21% (95% CI, 11%–33%), respectively (Figure 1).
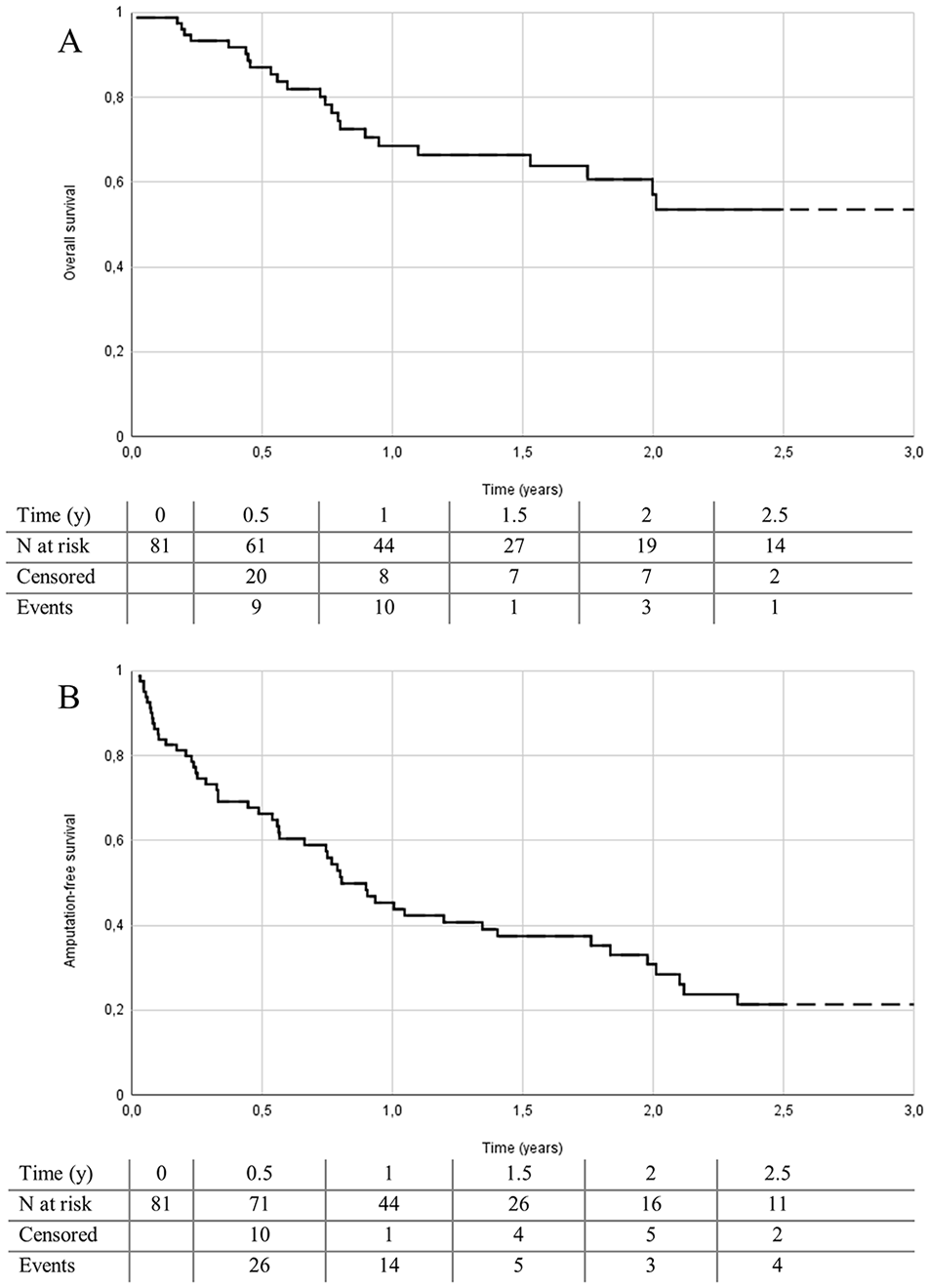
Kaplan-Meier analysis for overall patient survival (A) and amputation-free survival (B) after endovascular infrapopliteal reintervention. Standard error at 2.5 years was 7.8% for overall survival and 5.7% for amputation-free survival.
KM curves for freedom from amputation and freedom from MALE are shown in Figure 2. Estimated freedom from major amputation at 1 year and 2.5 years was 59% (95% CI, 46%–70%) and 41% (95% CI, 25%–56%), respectively. Estimated freedom from MALE at 1 year and 2.5 years was 54% (95% CI, 41%–65%) and 36% (95% CI, 21%–51%), respectively. Freedom from recurrent reintervention and freedom from amputation or recurrent reintervention are shown in Figure 3. Estimated freedom from recurrent reintervention at 1 year and 2.5 years was 68% (95% CI, 55%–78%) and 51% (95% CI, 33%–66%), respectively. Estimated freedom from a major amputation or recurrent reintervention at 1 year and 2.5 years was 42% (95% CI, 30%–53%) and 22% (95% CI, 11%–36%), respectively.
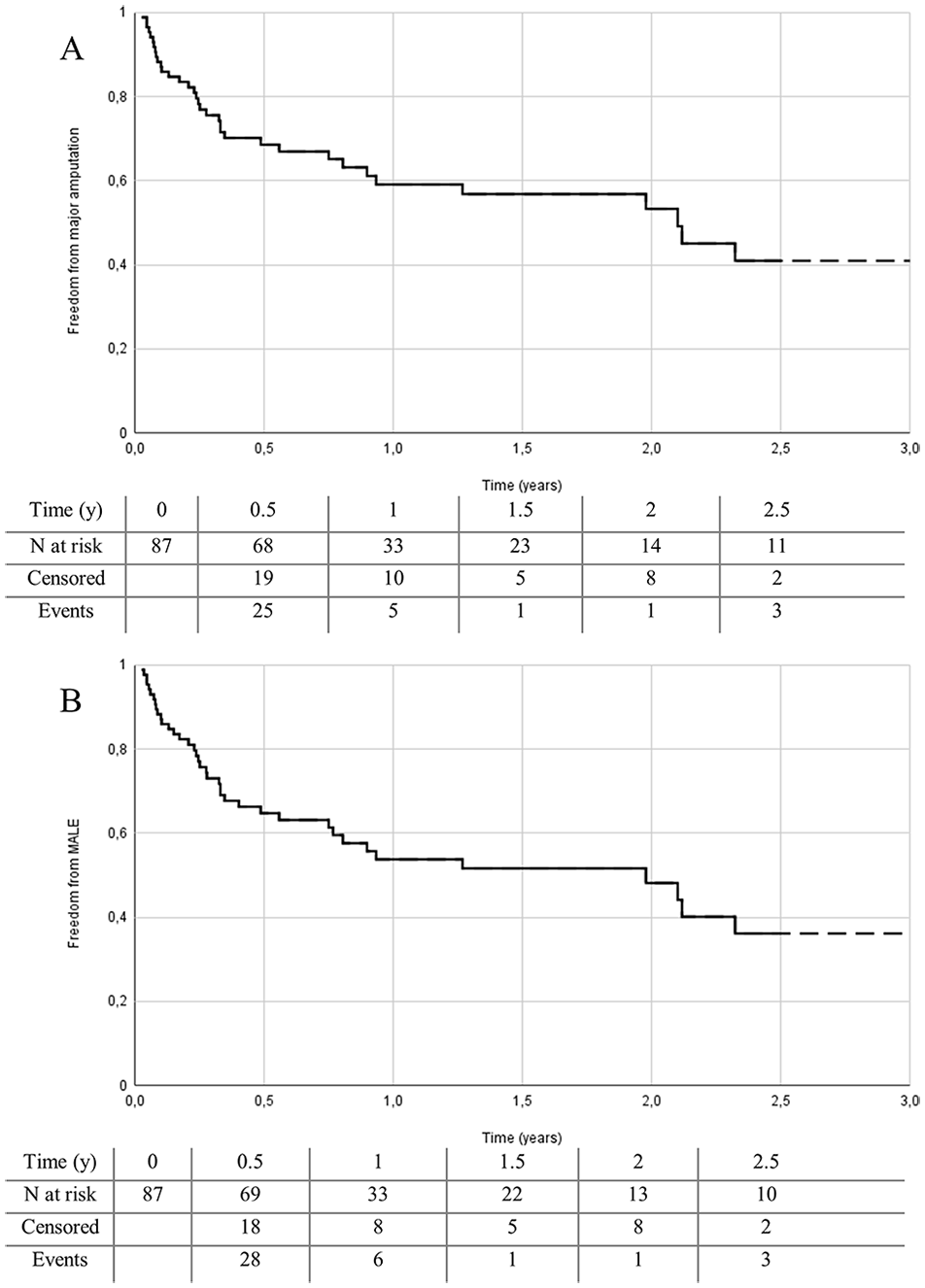
Kaplan-Meier analysis for freedom from major amputation (A) and freedom from major adverse limb events (B) for limbs after endovascular infrapopliteal reintervention. Standard error at 2.5 years was 8.1% for freedom from major amputation and 7.8% for freedom from major adverse limb events.
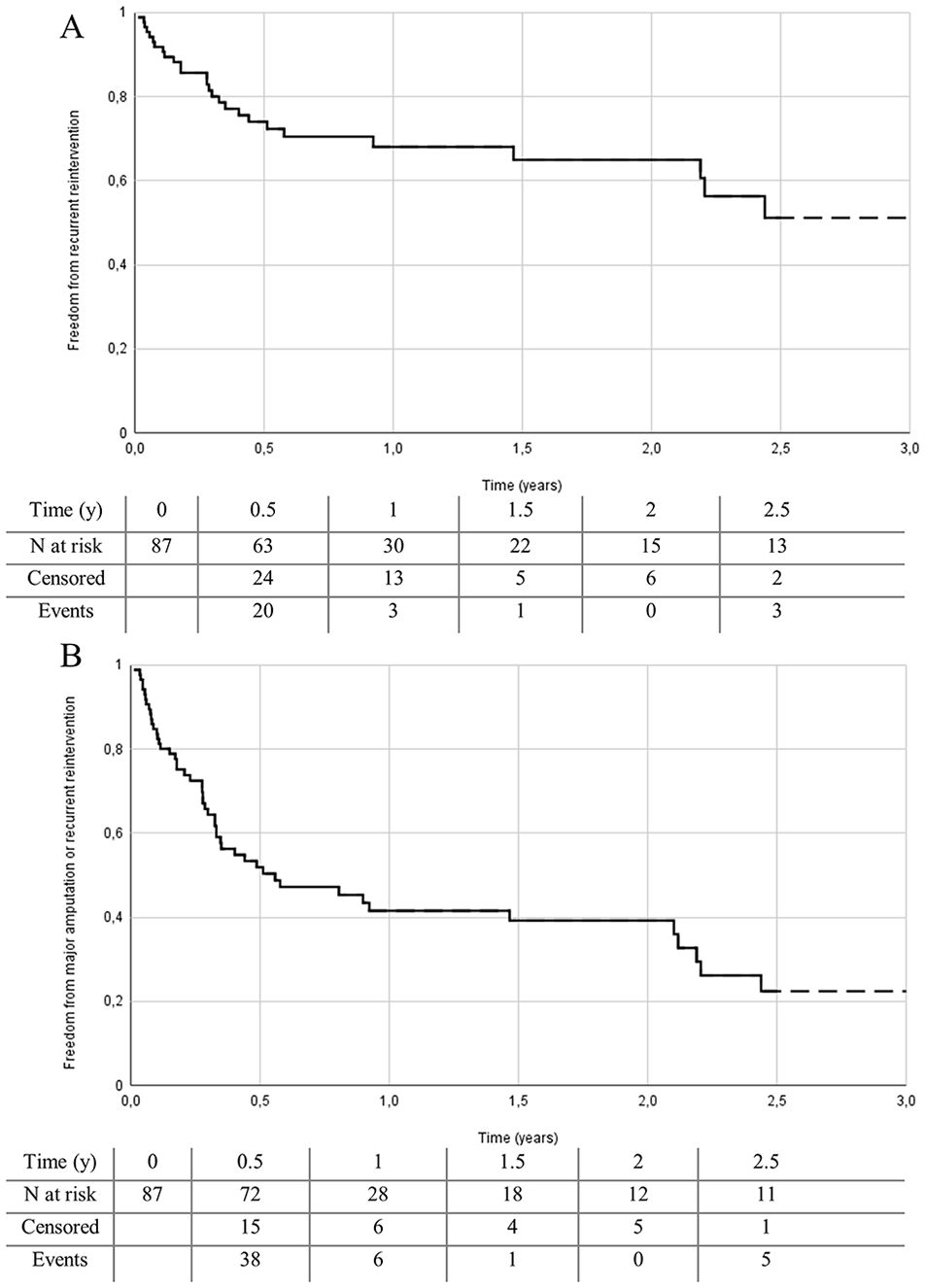
Kaplan-Meier analysis for freedom from recurrent reintervention (A) and freedom from major amputation or recurrent reintervention (B) for limbs after infrapopliteal endovascular reintervention. Standard error at 2.5 years was 8.7% for freedom from recurrent reintervention and 6.7% for freedom from major amputation or recurrent reinterventions.
The univariable hazard ratios for the analyzed risk factors for AFS and freedom of major amputation or recurrent reintervention are shown in Table 3. The univariable Cox proportional hazard model showed no statistically significant association between risk factors and AFS. The univariable Cox proportional hazard model for freedom from major amputation or recurrent reintervention showed an increased hazard ratio of 2.559 (95% CI, 1.078–6.072; p=0.033) for a GLASS score of III. A multivariable Cox proportional hazard model could not be fitted while there was only 1 significant variable in the univariable hazard model.
Univariable Cox Proportional Hazard Model for Amputation-Free Survival and Freedom From Major Amputation or Recurrent Reintervention After Endovascular Infrapopliteal Reintervention.
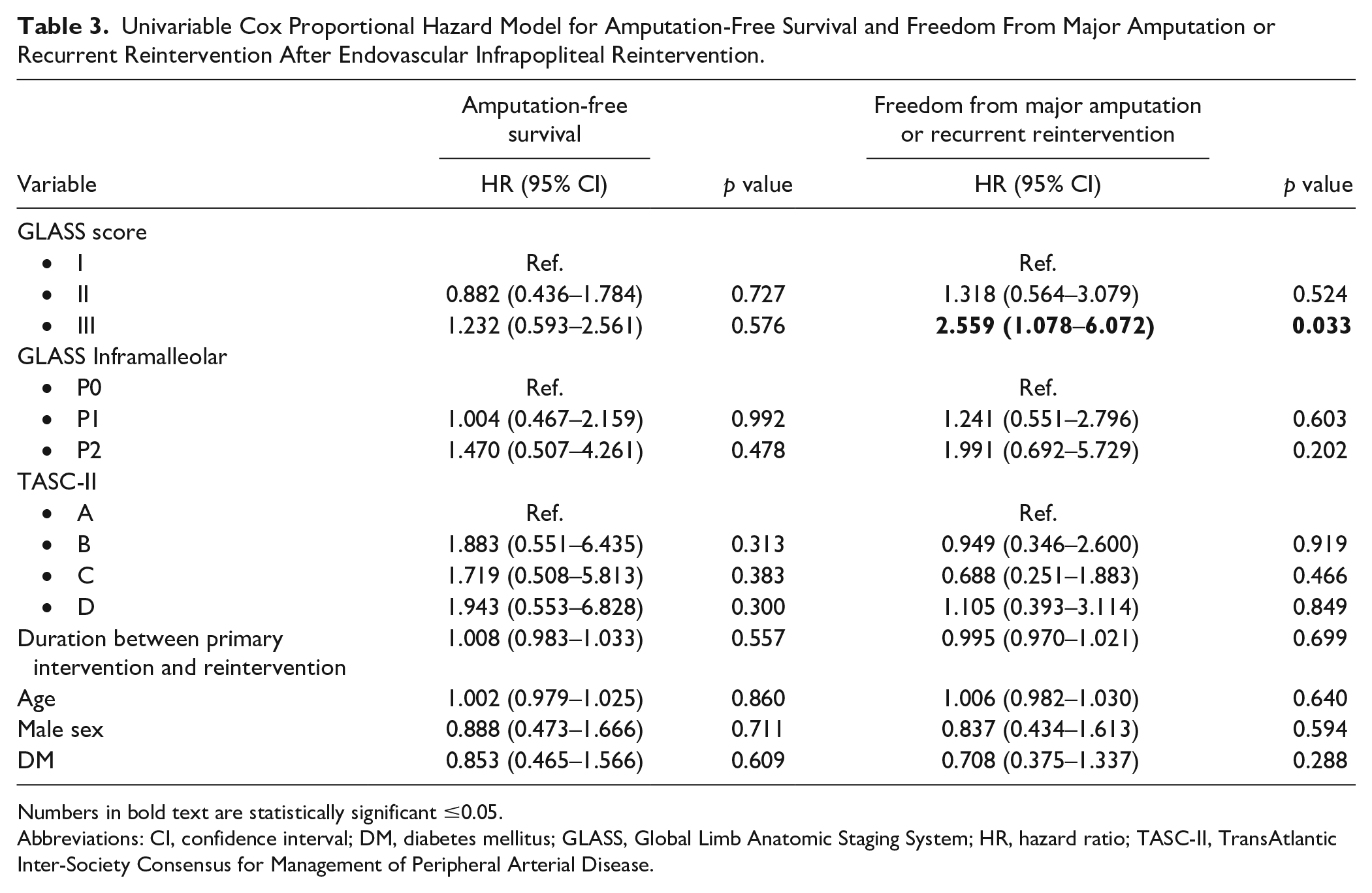
Numbers in bold text are statistically significant ≤0.05.
Abbreviations: CI, confidence interval; DM, diabetes mellitus; GLASS, Global Limb Anatomic Staging System; HR, hazard ratio; TASC-II, TransAtlantic Inter-Society Consensus for Management of Peripheral Arterial Disease.
Discussion
This retrospective multicenter study evaluated the outcomes and patency of endovascular infrapopliteal reinterventions for patients with CLTI. Technical success, 30-day mortality, and morbidity were acceptable; however, the outcomes of the infrapopliteal reinterventions were moderate to poor, with low rates of AFS and a high need for recurrent reinterventions.
In the literature, studies focusing on the outcomes of infrapopliteal reinterventions are scarce. One previous study on infrapopliteal reinterventions found an increased risk of amputation in CLTI patients on dialysis. 18 Furthermore, to determine the effect of the frequency of infrapopliteal reinterventions, Kobayashi et al 19 described worse outcomes, in terms of wound healing, limb salvage, and AFS, for patients requiring 3 or more reinterventions.
A study by Schmidt et al 20 offers an analysis reflecting the outcome of infrapopliteal reintervention by presenting the secondary patency (patency of the target lesion after treatment of a reocclusion) in a cohort of patients receiving endovascular retrograde tibioperoneal access. Secondary patency of infrapopliteal lesions was 63% at 1 year and 50% at 2 years. 20 This finding is in line with the secondary patency of 60% in a cohort of de Athayde Soares et al. 21 However, the repeat reintervention rate alone is a poor outcome measure for these patients because many of them received amputation and the primary goal of EVT is to improve limb perfusion and thereby avoid amputation. 22
Other studies that have examined reinterventions for the infraingunial arterial disease also found good 30-day outcomes.23,24 Shannon et al 24 compared the outcomes of endovascular reinterventions with those of a bypass surgery after prior failed EVT, recommending endovascular reintervention when anatomy is suitable because of low 30-day major adverse cardiac events. However, Paraskevas and Geroulakos 25 question this recommendation while failing to address the long-term patency and amputation rates. 24 The uncertainty about the patency of endovascular reinterventions may be a reason to consider a bypass surgery. 25
Considering the high need for recurrent reinterventions after an EVT in combination with poor AFS, other treatment options might be considered. The previously mentioned bypass surgery after a prior failed EVT is an alternative treatment option for patients with infrapopliteal CLTI. The most recent guideline for CLTI recommends open surgical revascularization with an autologous vein graft in patients with an infrainguinal disease, in consideration of Wound, Ischemia, and foot Infection (WIfI) and GLASS classification, especially in high-risk patients with advanced complexity of the disease or after prior failed endovascular attempts. 1 Long-term clinical outcomes specifically for an infrapopliteal bypass after a prior EVT has been investigated, with different conclusions. Although “endovascular first” is a common approach in infrainguinal disease, performing a bypass surgery after EVT might have worse outcomes compared with an initial bypass, as was found in the Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL-1) trial for infrainguinal disease. 26 This is in contrast to 2 retrospective studies on infrapopliteal disease, not showing worse outcomes for infrapopliteal bypass after prior EVT compared to patients who primarily underwent a bypass surgery.17,27 Therefore, performing a bypass surgery after a failed EVT should definitely need to be considered for patients with infrapopliteal CLTI in case a vein is available, with attention to the anatomical features such as GLASS classification and using shared decision-making for these often complex and multimorbid patients.1,28 The combined outcome of major amputation and recurrent reintervention was associated with a high GLASS score in this study. The GLASS score describes a complexity of the anatomic pattern of the disease, which may be the reason for worse patency rates of endovascular reinterventions resulting in low freedom from a major amputation or recurrent reintervention. However, these GLASS scores were not used in the decision-making while patients were included from 2015, and the GLASS classification was proposed by the global vascular guidelines in 2019. 1 For study purposes, the GLASS scores were determined retrospectively for all patients. The upcoming outcomes of the Best Endovascular versus Best Surgical Therapy in Patients With Critical Limb Ischemia (BEST-CLI) trial should provide us with more definitive evidence on the optimal treatment strategy. 29
Alternative treatment options can be considered in addition to EVT and bypass surgery. One example is percutaneous deep venous arterialization, which provides perfusion of the limb indicated for patients with the so-called no-option CLTI. 30 A recent study investigating the efficacy of percutaneous deep venous arterialization showed acceptable technical success and promising rates of AFS and limb salvage rates and that it may be an alternative to arterial infrapopliteal reinterventions. 31 Besides this, even though the mortality rate is high after primary amputation, amputation might be considered as a treatment option in light of the low AFS of 21% after 2.5 years. 22 In addition, the low overall survival of 54% of patients after 2.5 years of follow-up emphasizes again CLTI patients suffer from an end-stage cardiovascular disease. Therefore, providing best medical treatment is of utmost importance to improve clinical outcomes and survival.
The findings of this investigation complements those of earlier studies, showing poor long-term outcomes of patients with CTLI requiring reinterventions. Literature on several treatment options have been explored; however, uncertainty remains on the best therapy for these patients. While safety and technical success seems preserved, long-term limb salvage and survival is poor. If the debate is to be moved forward, randomized trials are needed to provide more definitive evidence on the treatment of patients with reoccurrence of the infrapopliteal disease.
Limitations
This study is limited by its retrospective nature and the small number of included patients. Owing to the retrospective character, selection bias is likely; for example, missing patients with CLTI who were not offered a reintervention were treated with bypass surgery, amputated primarily, or treated conservatively. Furthermore, we did lose patients during follow-up, leading to an increased uncertainty of survival outcomes. However, the standard error remained below the prespecified precision of 10% for the KM analysis. The clinical information on severity of disease was limited to Fontaine classification; Rutherford’s classification or WIfI classification could have been better to distinguish minor tissue loss from major loss or determine the presence of infection. In addition, 13 limbs underwent a reintervention for a lesion other than the primarily treated lesion, which leads to a heterogeneous cohort. The small cohort prevented us from identifying individual risk factors for relevant outcome measures such as amputation. Another study limitation is the lack of a proper control group.
One of the drawbacks in determining the technical success of revascularization is that it is mainly limited to the target lesion. A possible better way to assess whether an EVT will lead to improved limb perfusion is to determine technical success together with the presence of the number of runoff arteries with uninterrupted flow to the foot circulation. Another option is to perform tissue perfusion measurements before and after the EVT to determine treatment success. To date, however, no perfusion measurement technique has been implemented on a wide scale due to the lack of validity and reliability. 32
Conclusions
Endovascular infrapopliteal reinterventions can be performed with acceptable 30-day mortality and complication rates; however, outcome and patency at 2.5 years in the follow-up are moderate to poor, with a low AFS and high rates of major amputations and recurrent reinterventions.
Supplemental Material
sj-tiff-1-jet-10.1177_15266028221147457 – Supplemental material for Outcomes and Patency of Endovascular Infrapopliteal Reinterventions in Patients With Chronic Limb-Threatening Ischemia
Supplemental material, sj-tiff-1-jet-10.1177_15266028221147457 for Outcomes and Patency of Endovascular Infrapopliteal Reinterventions in Patients With Chronic Limb-Threatening Ischemia by Simone F. Kleiss, Patricia A. H. van Mierlo-van den Broek, Cornelis G. Vos, Bram Fioole, Gijs C. Bloemsma, Debbie A. B. de Vries-Werson, Reinoud P. H. Bokkers and Jean-Paul P. M. de Vries in Journal of Endovascular Therapy
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.