
Abstract
Introduction
Stroke is 1 of the leading causes of disability and death worldwide. Endovascular therapy with mechanical thrombectomy in acute stroke patients allows the treatment of cases with large vessel occlusion stroke. 1 Approximately 20% of ischemic strokes are due to atherosclerotic carotid stenosis, and about 6% of patients receiving endovascular stroke treatment require additional emergency treatment of the carotid artery for adequate stroke therapy.2,3 Carotid artery stenting (CAS) is the most common treatment option for concomitant carotid stenosis. 4 Even though current data are limited to rather small retrospective studies and prospective randomized studies are lacking, data in the literature suggest that carotid artery endarterectomy (CEA) can also be a valuable treatment option in these patients: CEA can be helpful in gaining access in stroke patients with non-passable high-grade ICA stenosis. 5 It has also been shown that emergency CEA instead of carotid artery stenting with dual antiplatelet therapy (DAPT) reduces the risk for subsequent intraparenchymal hemorrhage after thrombectomy.6-8
In our institution, we perform emergency CEA in stroke patients in our angiography suite in the same anesthesia session as the thrombectomy to avoid transportation to the operating room. A major limitation of this approach is the lack of neuromonitoring during the surgical procedure, which implies the risk of unnoticed ischemia during surgery.9,10
The aim of our study was to investigate whether CEA in the emergency stroke setting without neuromonitoring is associated with a risk for additional infarctions that are not explained by the initial stroke.
Methods
Clinical Procedures
Clinical patient selection and procedures have been reported previously.5,6,11 In short, our workflow is as follows: The rescue coordination center informs the neurologist in charge about a possible stroke and its predicted time of arrival directly by phone. Depending on the severity of reported symptoms, the neurologist already contacts the neuroradiologist and anesthesiologist on call. At hospital arrival, the neurologist confirms the stroke symptoms and severity as well as cardiopulmonary stability by a focused clinical examination and furthermore initiates the patient’s direct transport to the CT suite. Acute stroke patients in our institution receive emergency cranial computed tomography (CCT), CT angiography (CTA) and CT perfusion (CTP) using a mathematical deconvolution approach and a maximum slope approach for calculation of perfusion parameters (Somatom Definition AS, Siemens Healthineers, Forchheim, Germany). If the neurologist makes the decision for intravenous thrombolysis, it is directly administered in the CT suite without waiting for CT angiography and CT perfusion, which are routinely performed next. Patients, who present within a time window of 4.5 hours after symptom onset receive intravenous thrombolysis in the absence of contraindications. 12 Patients with extended or unknown time windows receive intravenous thrombolysis based on non-contrast CT scans as well as CT perfusion exams and/or MRI. 13 Given eligibility and interdisciplinary neurological-neuroradiological treatment decision to perform endovascular stroke therapy, the patient is transferred to the angiography suite immediately after CT imaging. The majority of endovascular procedures are performed under general anesthesia and parallel workfow with the interventionalist performing the groin puncture while the anesthesiologist intubates the patient. During thrombectomy, systolic blood pressure is kept above 160 mmHg and is lowered once revascularization is achieved. All common thrombectomy techniques such as stent-retriever thrombectomy, ADAPT (A Direct Aspiration First Pass Technique) and combined approaches such as SAVE (Stent-Retriever Assisted Vacuum-Locked Extraction) and Solumbra (use of a stent retriever with concomitant distal aspiration) are established in our clinic. 14 We implemented an interdisciplinary consensus in our hospital to perform thrombectomy with general anesthesia and to avoid CAS whenever possible and to perform CEA in the same anesthesia session in our angiography suite either before or after thrombectomy whenever necessary. For this, we notify our vascular surgery team, which is available 24/7, whenever 1) surgical access to the occlusion site is needed because access to the occlusion site via femoral or radial/brachial access is expected to be difficult and to take longer than 45 minutes or 2) CAS and DAPT should be avoided in a case of high-grade ICA stenosis. The vascular surgery team is then on hold in our angiography suite and performs the necessary procedure in the same anesthesia session before or after thrombectomy. Medical management during hospital stay and rehabilitation are performed following relevant guidelines and clinical standards. All cases are entered into our local stroke registry and are evaluated and discussed in interdisciplinary teams at regular intervals.
Surgical Procedure
According to our standard operating protocol, 1 dose of antibiotics is given prior to incision and 3000 IE of heparin are given prior to carotid clamping. No modifications of medical treatment are made for surgery; hence, intravenous thrombolysis is continued during surgery. During carotid cross-clamping a mean arterial pressure of 100 mmHg is being maintained. In cases of contralateral carotid occlusion, a temporary inta-arterial shunt (LeMaitre Vascular, Sulzbach, Germany) is routinely inserted during carotid clamping. In cases of non-stenotic contralateral carotid artery and a good collateralization through the circle of Willis, shunt insertion is not mandatory in our institution if eversion thrombendarterectomy is the surgeon`s preference and the procedure can be performed with a short (<20 minutes) clamping time. An eversion or conventional carotid thrombendarectomy with bovine patch plasty (Lamed, Oberhaching, Germany) are performed, depending on the carotid anatomy and on the surgeon`s preference. On completion, an angiography of the carotid reconstruction and of the intracranial vessels is routinely performed, and the neck incision is closed following drainage insertion.
Patients
Data for this study were based on our prospectively maintained stroke registry that was launched and approved in the context of the ENDOSTROKE registry trial (ClinicalTrails.gov NCT1399762).15,16 This retrospective analysis was approved by our local ethics board, allowing us to use all patient data without explicit consent.
Our hospital is a tertiary stroke center with a coverage for approximately 1.2 million inhabitants. For this analysis we included all consecutive patients with occlusions in the anterior circulation who received thrombectomy together with emergency CEA either before or after thrombectomy between June 2013 and November 2020. Of 1257 patients, who received thrombectomy due to occlusion in the anterior or posterior circulation, 54 consecutive patients were found to undergo vascular surgery in the acute setting. To homogenize our patient population, we excluded 3 patients with CEA between 24-72 hours after thrombectomy and 2 patients who received emergency CEA with the same anesthesia team directly after thrombectomy, but in the surgical ward. Two further patients were excluded from analysis as they received emergency stenting as well as emergency CEA during hospitalization. This left 47 patients to be included in our study.
Analysis
To assess whether there were additional infarctions due to the surgical procedure, we assessed initial preinterventional CT imaging as well as postinterventional and follow-up imaging. Initial cranial CT, CT perfusion maps, and CT angiograms were analyzed with regard to already infarcted areas, cerebral perfusion evoking tissue at risk, and vessel anatomy including the collateralization in the circle of Willis (CoW). Tissue at risk was defined as any non-infarcted area with increased perfusion times (time-to-peak, mean-transit-time, or time-to-drain parameters) on deconvolution perfusion maps (VPCT, Siemens Healthineers, Forchheim, Germany). Post-interventional and follow-up imaging were analyzed with regard to the initially expected infarction size and new infarction, which was not explained by the initial stroke upon admission.
Clinical, procedural, and imaging data included among others baseline characteristics (such as age, sex, and initial stroke size) and an extended set of variables (such as duration of the procedures, use of an arterial shunt, and minimum arterial pressure during the anesthesia). In patients, in whom the duration of the surgical procedure was not documented consistently, we estimated the duration using anesthesia logs and imaging data.
Primary outcome parameters were the occurrence of additional ipsilateral and/or contralateral infarctions that were not explained by the initial stroke as well as final infarction size according to the Alberta Stroke Program Early CT Score (ASPECTS). 17
Secondary outcome parameters were the occurrence of parenchymal hemorrhage (defined as PH1 and PH2 according to the European Australasian Acute Stroke Study, ECASS) and the rate of good clinical outcome after 90 days according to the modified Rankin Scale (mRS 0-2).18,19 We also analyzed the independent impact of the presence or absence of a complete CoW, collateral ICA stenosis, and the use of an intraoperative shunt on our outcome parameters in a multivariable analysis.
All imaging analyses were performed by 2 experienced neuroradiologists who were blinded to each other. A reference standard for statistical analyses was obtained in a consensus reading.
Statistics
Parametric variables are indicated as mean±standard deviation (SD) and non-parametric variables are indicated as median and interquartile range (IQR). For comparison of these variables we used a Student’s T test or a Mann–Whitney U test after testing for normal distribution with a Shapiro-Wilk test. Nominal variables were tested with Fisher’s exact tests and χ2 tests, depending on sample size. Multivariable analysis was performed with a linear logistic regression test with backward elimination, indicating the regression coefficient (r) and 95%-confidence intervals (CI). P values under the α-level of .05 were defined as significant. All statistical analyses were performed with SPSS 27 software.
Results
Overview of All Patients. All Values are Given as Medians Unless Specified Otherwise.
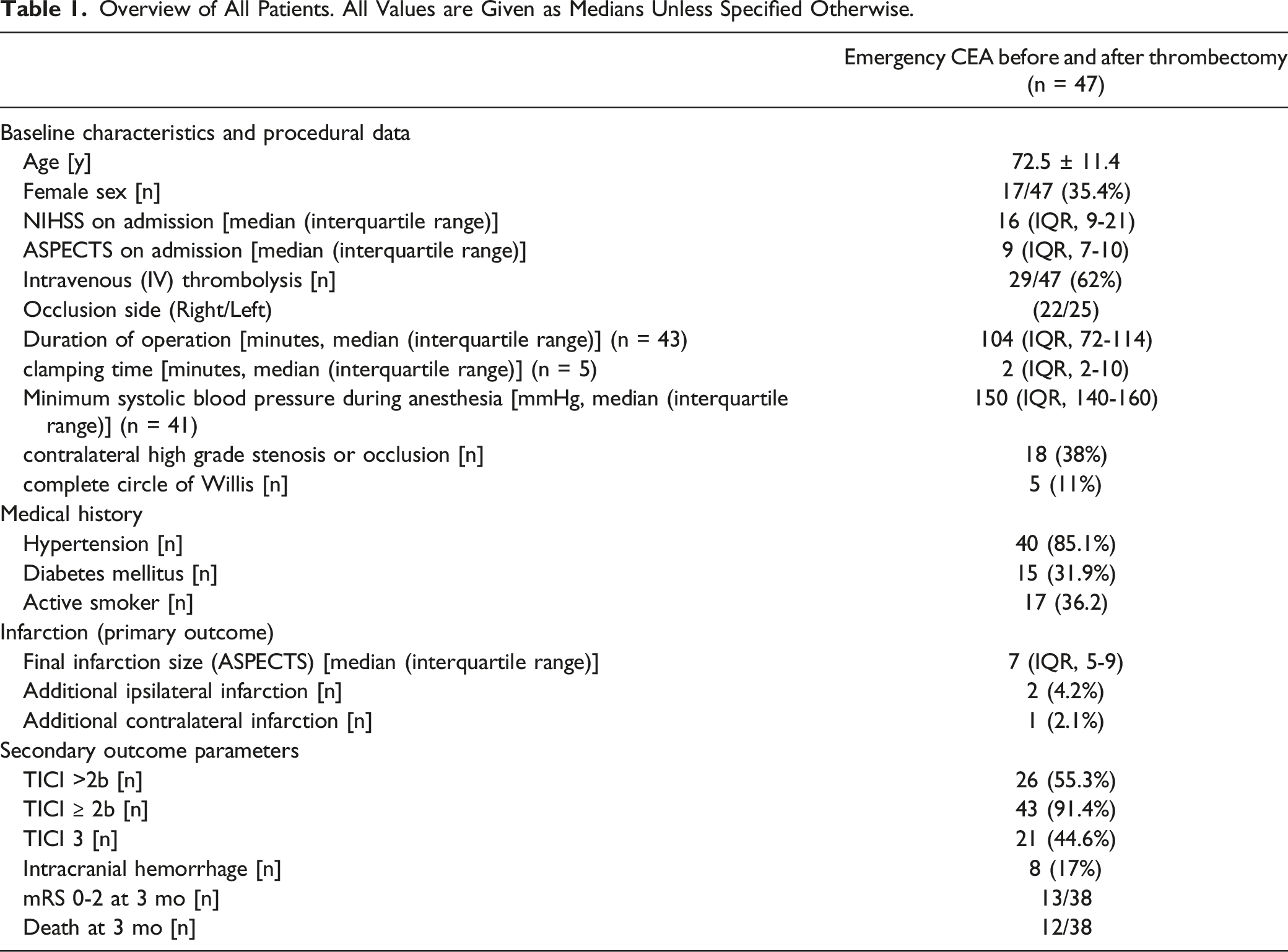
Of the 47 patients with CEA, 12 (26%) patients received CEA before thrombectomy because of difficult access route or because passage of the carotid artery was not possible, and 35 (74%) patients received CEA after thrombectomy because a high-grade residual stenosis had remained.
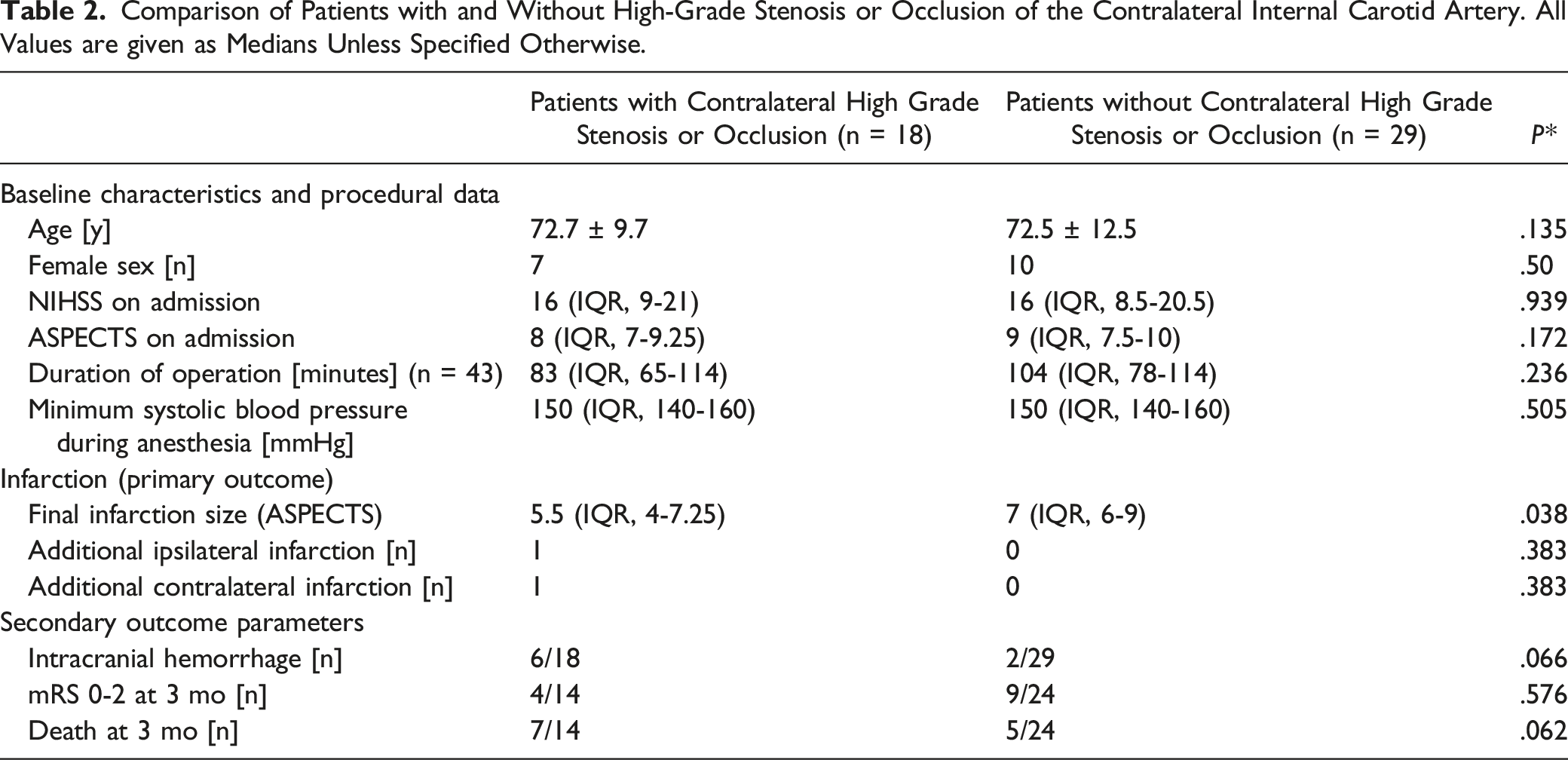
Comparison of Patients with and Without High-Grade Stenosis or Occlusion of the Contralateral Internal Carotid Artery. All Values are given as Medians Unless Specified Otherwise.
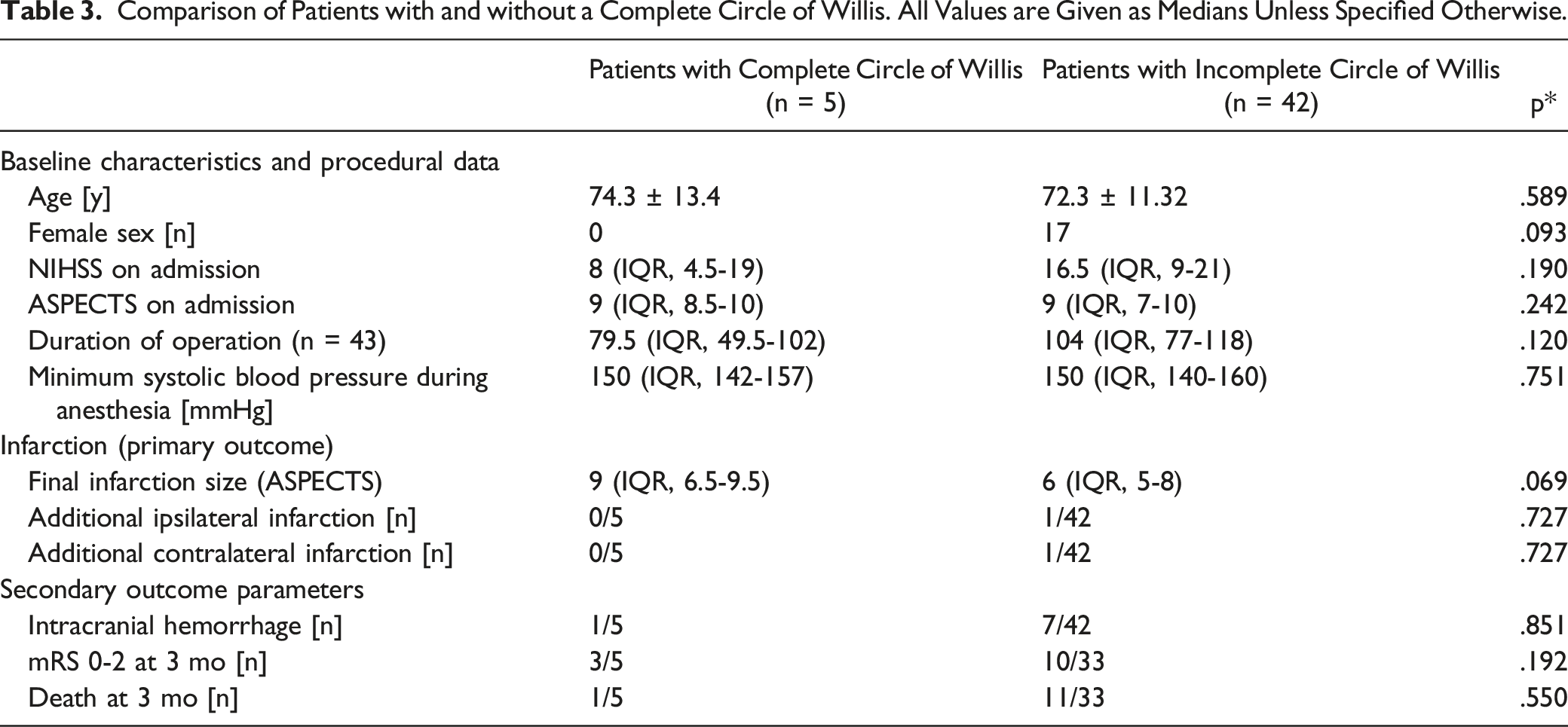
Comparison of Patients with and without a Complete Circle of Willis. All Values are Given as Medians Unless Specified Otherwise.
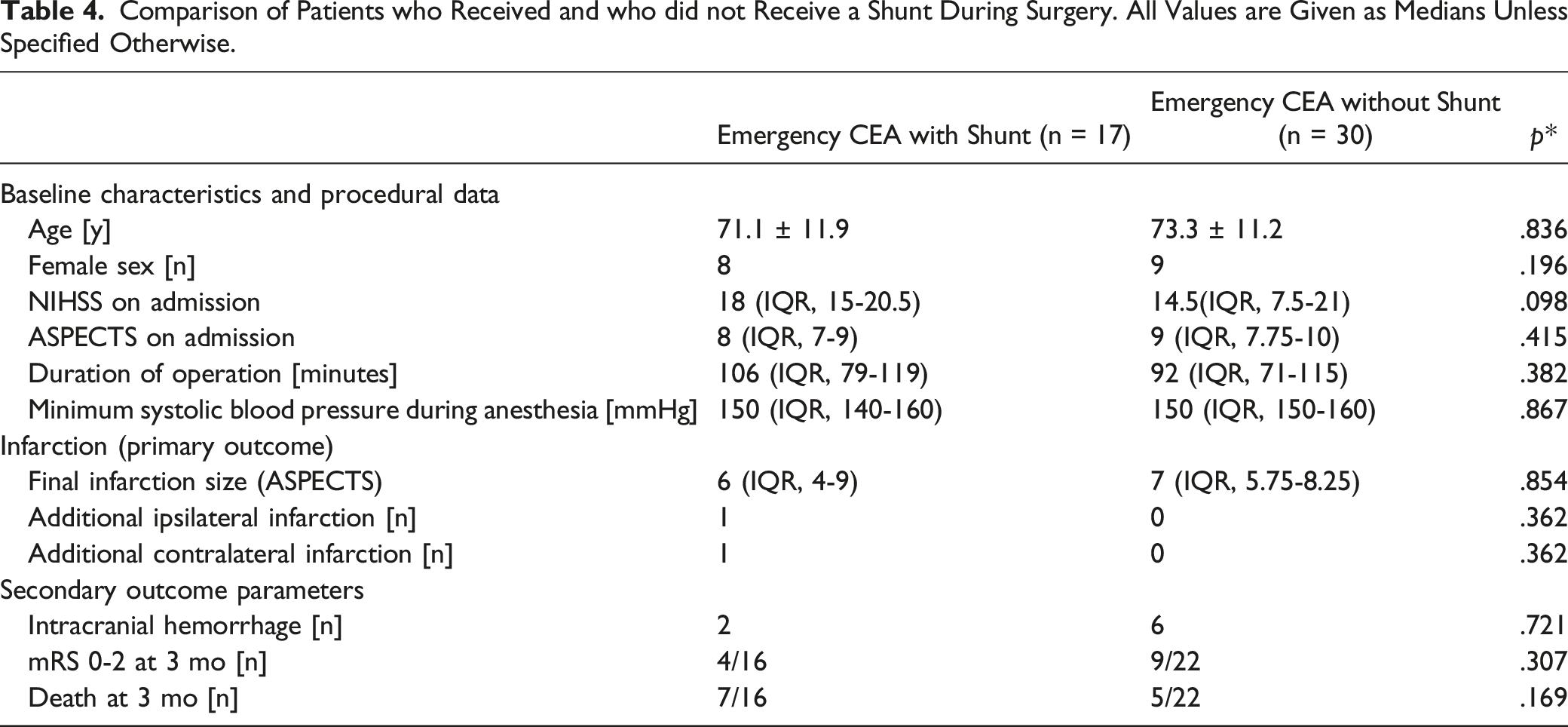
Comparison of Patients who Received and who did not Receive a Shunt During Surgery. All Values are Given as Medians Unless Specified Otherwise.
Primary Outcome
Final stroke was smaller than tissue at risk in 31 of 47 (66%) patients. There were only 2 patients with new infarction in an originally unaffected territory: in 1 patient with occlusion in the middle cerebral artery, there was new infarction in the previously unaffected ipsilateral anterior cerebral artery territory. As shown on the angiography images this was due to embolization during thrombectomy. In another patient with occlusion in the middle cerebral artery, there was new infarction in the previously unaffected ipsilateral anterior cerebral artery territory. As shown on the angiography images this was also due to embolization during thrombectomy. In both cases the reason for these embolic events remained unclear, though. The second patient, whose detailed case description is given in Figure 1, also suffered from additional contralateral border-zone infarction (Figure 1). These 2 patients belonged to a group of 9 of 18 (50%) patients with stenosis or occlusion of the contralateral ICA and contralateral perfusion deficits evoking additional tissue at risk. This patient had acute occlusion of the right MCA and a concomitant proximal high-grade ICA stenosis. In addition to the expected right-hemispheric infarction, this patient also suffered from a left-sided infarction in the border zone of the anterior and middle cerebral artery territories, because there was a pre-existing chronic occlusion of the left ICA, with the left hemisphere being mainly perfused via the anterior communicating artery. A 64 year-old male patient with acute ischemic stroke due to embolic occlusion of the right middle cerebral artery (MCA) and concomitant occlusion of the internal carotid artery (ICA). Initial CT scan (A and B) shows edema due to acute infarction in the right insular and frontal lobe (a: arrow). There is also infarction in the left frontal lobe (A: arrowhead). There are no signs of infarction in the apical layers (B). CT angiography (C and D) reveals occlusion of the right MCA bifurcation (C: arrow). There is also a high-grade stenosis with thrombotic aggregates at the origin of the right ICA (D: arrow). Despite this, the right ICA is perfused (D: arrowheads). There is chronic occlusion of the left internal and common carotid arteries (d: thin arrow). Perfusion imaging (E) shows that there is a perfusion deficit in the right MCA territory (e: arrow), but also in the left border zone between the middle and anterior cerebral artery territories (time to drain parameter; E: arrowhead). Normal cerebral blood volume (CBV) and blood flow (CBF) in the left hemisphere (E) suggest that the deficit is compensated. While a high caliber right posterior communicating artery (not shown) contributes to perfusion of the right hemisphere, a low caliber left posterior communicating artery (not shown) implies that perfusion of the left hemisphere depends on other collaterals, especially on the wide anterior communicating artery. Initial angiography (F and G) shows occlusion of the proximal right ICA (F: arrow) with only delayed and faint contrast in the subsequent right ICA via cervical collaterals (G: arrow). There is also faint contrast in the left anterior and middle cerebral artery (G: arrowheads), indicating that the right ICA supplies the left hemisphere via the anterior communicating artery. DSA after thrombectomy and carotid artery endarterectomy (H-J) shows that the proximal ICA is reconstructed (H) and arterial perfusion is restored (I). While there is arterial perfusion even in the left anterior and middle cerebral artery (I: arrowheads), the border zone between the left anterior and middle cerebral arteries remains insufficiently supplied in the parenchymal phase (J: arrow). A shunt was used during surgery. Minimum systolic arterial pressure during surgery was 140 mmHg. On follow-up CT after 10 days (K), there is infarction in the right hemisphere (also in the right anterior cerebral artery territory due to embolism during cerebral thrombectomy), but also in the border zone of the left hemisphere, with final infarction and initial perfusion deficit matching well (f: arrowhead and k: arrowheads).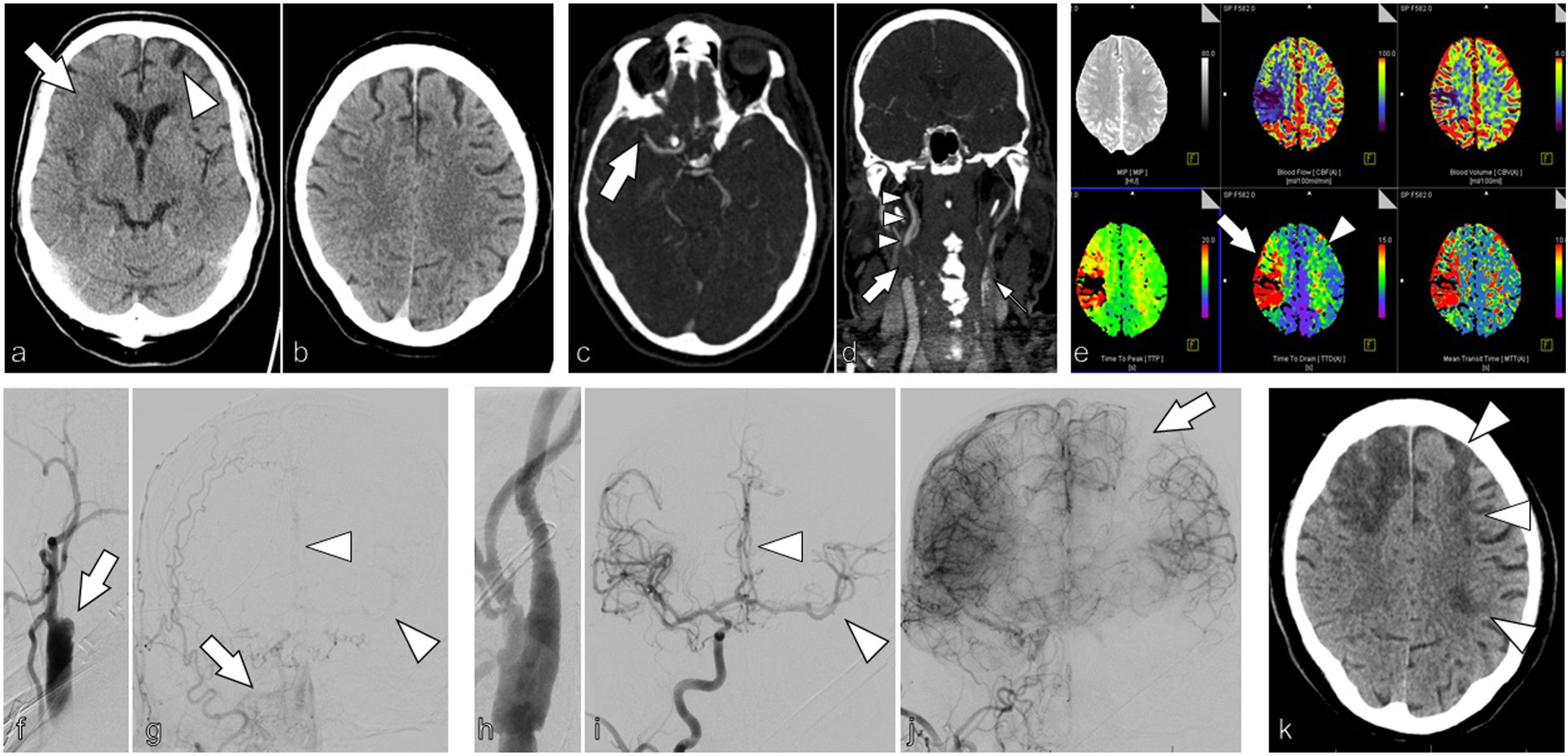
Secondary Outcome
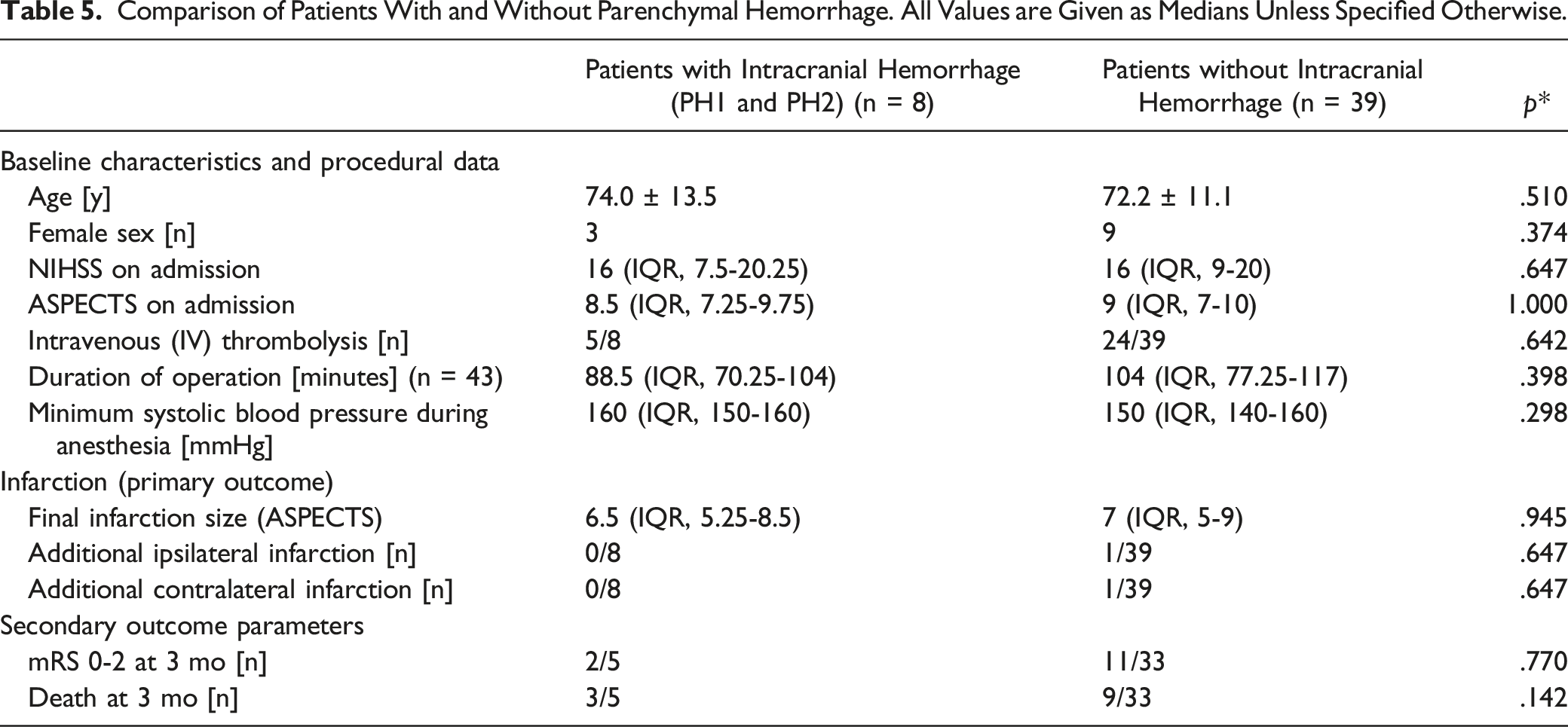
Comparison of Patients With and Without Parenchymal Hemorrhage. All Values are Given as Medians Unless Specified Otherwise.
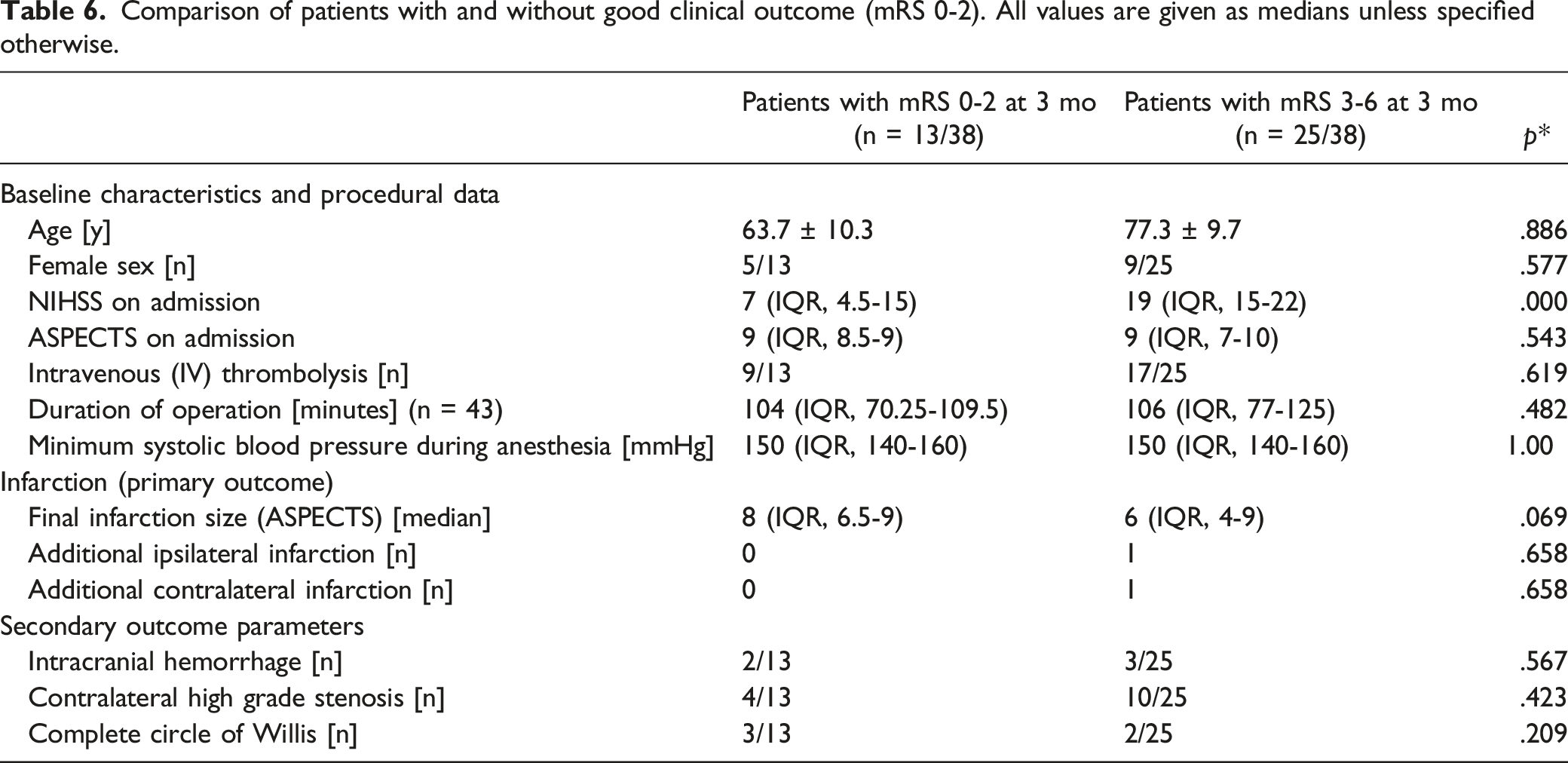
Comparison of patients with and without good clinical outcome (mRS 0-2). All values are given as medians unless specified otherwise.
In univariate analyses, final infarction size was significantly larger in patients with stenosis or occlusion of the contralateral ICA (P = .038; Table 2); CoW anatomy and the use of a shunt during surgery had no significant impact on our primary and secondary outcome parameters (Tables 3 and 4). Logistic regression revealed that contralateral stenosis or occlusion was independently associated with final infarction size (P = .042; r = -1.48; CI = -2.9 - .54), whereas CoW anatomy (P = .121; r = -.49; CI = -2.0 -.06) and use of a shunt during surgery (P = .516; r = 1.84; CI = -2.9-.54) were not.
Discussion
Our concern that emergency CEA without neuromonitoring could lead to new infarctions was not confirmed. Definite infarction was smaller than tissue at risk in two-thirds of patients. Only 2 patients had an unexpected infarction in a previously unaffected territory, which was not necessarily due to surgery: 1 patient with MCA occlusion suffered from embolism in the previously unaffected ipsilateral anterior cerebral artery caused during endovascular thrombectomy. The other patient also had MCA occlusion and suffered from embolism in the previously unaffected ipsilateral anterior cerebral artery (also caused during endovascular thrombectomy), but also from contralateral border-zone infarction (Figure 1). This clinical course is worth mentioning (Figure 1), because it is conceivable that the additional surgery resulted in decompensation of an already insufficient perfusion of left hemisphere. However, the poor left-hemispheric perfusion in angiography, the good match between final left-sided infarction and initial perfusion deficit in the left border zone, the use of a shunt during surgery and the high minimum systolic arterial pressure of 140 mmHg during surgery, imply that it is at least equally possible that the left-sided stroke was due to the overall poor collateral situation and could have occurred even without our doing.
20
A similar case (Figure 2), which did not result in such infarction, implies that we can neither prove nor rule out that our intervention resulted in this outcome. In conclusion, 9 of 18 patients with high-grade contralateral stenosis or occlusion had contralateral perfusion deficits and only 1 of these patients had contralateral infarction that was potentially but not definitely attributable to our intervention. An 81 year-old female patient with acute ischemic stroke due to embolic occlusion of the right common carotid artery (CCA) and internal carotid artery (ICA). There are no signs of infarction on the initial CT scan (A). CT angiography (B and C) shows thrombotic occlusion of the right CCA (B and C: arrow) and contralateral high-grade stenosis of the left ICA (B: arrowhead). Perfusion imaging (D) shows that there is a perfusion deficit in the right MCA territory (D: arrow) and in both border zones between the middle and anterior cerebral artery territories (D: arrowheads). Because it was not possible to reach the CCA via a femoral access, we performed carotid endarterectomy (CEA) with extraction of large clots from the CCA. After CEA, a DSA (E) via a sheath in the CCA (e: arrow) shows multiple residual clots in the right ICA (E: arrowheads). After thrombectomy in the ICA, normal perfusion is restituted (F). On follow-up CT after 9 days (G), there is no infarction. MRI after 16 days shows faint diffusion restriction with a hemodynamic pattern in the right border zone between the middle and anterior cerebral artery territories (H: arrowheads) but no infarction in the left hemisphere.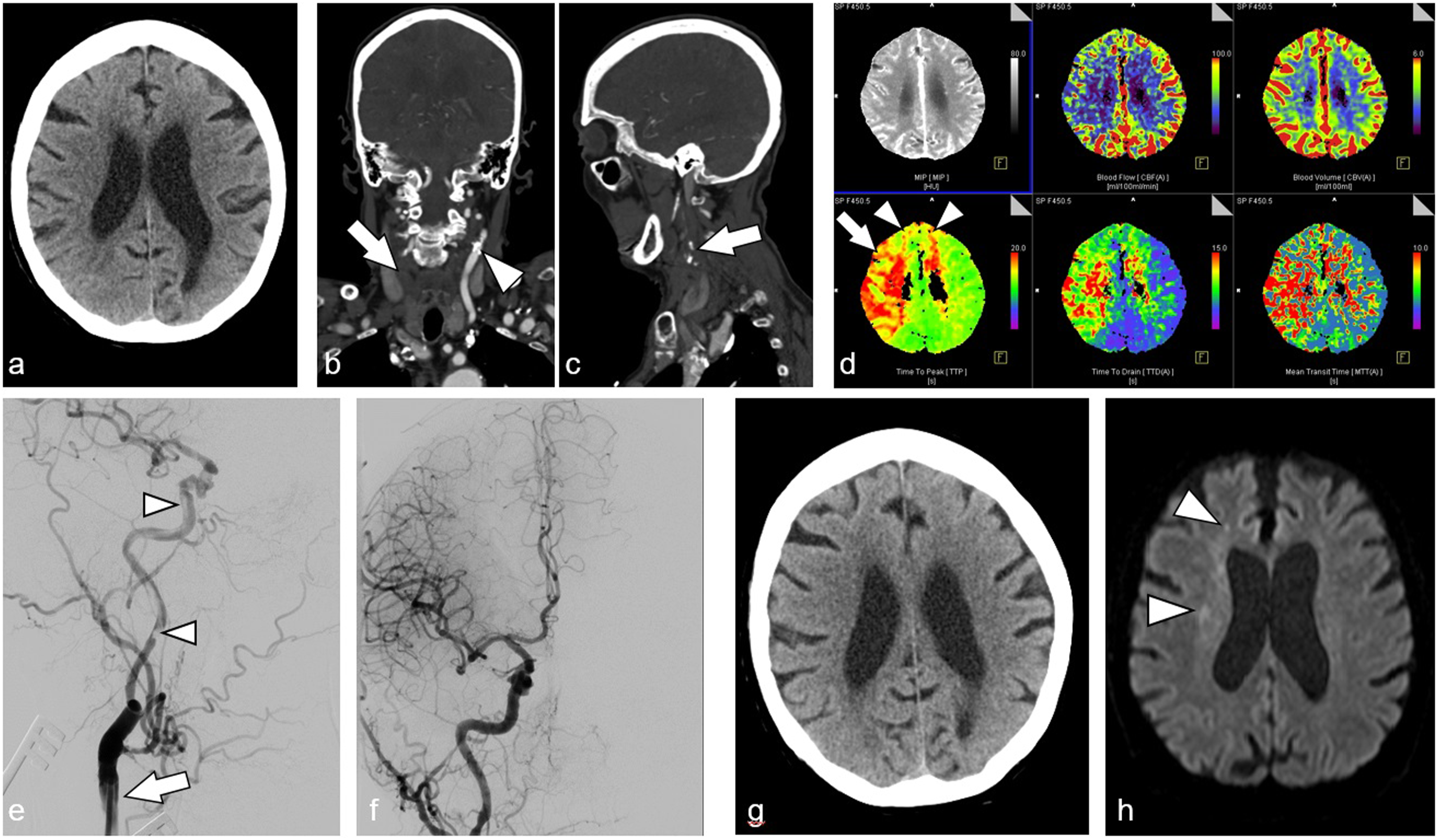
In elective CEA cases, great care must be taken not to endanger the patient. Common concerns are contralateral high-grade stenosis and insufficient intracranial collateralization. 21 Therefore, the indication for elective CEA is strict, the procedures are short, and protective options such as shunts and neuromonitoring are used to avoid infarctions.10,22 In acute stroke, however, a hemodynamically relevant stenosis or occlusion needs to be treated as fast and as efficiently as possible. Notably, contralateral ICA stenosis (>60%) and chronic occlusion were present in 18 of 47 (38%) patients. In these patients, final infarction size was significantly larger than in patients without stenosis or occlusion of the contralateral ICA. We surmise that contralateral stenosis or occlusion results in larger infarctions by impairing collateral supply to the affected territory. Even though our study lacks a control cohort of patients without surgery, data in the litrature suggest that contralateral stenosis has a negative impact regardless of additional procedures such as CAS or CEA: Maus et al compared straight-forward thrombectomy stroke patients with and without contralateral stenosis (>50%) and found that contralateral stenosis was independently associated with significantly larger infarctions (176 cm3 vs 11 cm3; P < .001) and unfavorable outcome (93% vs 65%; P = .003). 14 This suggests that a complete CoW should have a protective impact on outcome, which was shown to be the case in some studies, but which was not the case in our study and the study of Seifeld-Held et al.23-25 Because most patients in our cohort had an incomplete circle of Willis, more comprehensive studies are needed to develop a full picture of this issue. Regarding intraoperative shunting, our results do not speak for or against its use, especially because the use of a shunt was not randomized but at the surgeons’ discretion in our study. This is indeed a limitation of this study. This accords with the literature, which is non-conclusive: While a shunt does not appear to be absolutely necessary when collaterals and cerebral perfusion are good, the use of a shunt is recommended in the presence of contralateral carotid occlusion and suboptimal collateralisation.9,26,27
Limitations
Limitations of this study are its retrospective nature, its limited sample size, and the fact that it lacks a control cohort of patients without surgery. Furthermore, the use of a shunt during surgery was not randomized but at the surgeons’ discretion.
Conclusion
Emergency surgery in the angiography suite without neuromonitoring does not appear to be associated with an increased risk for additional infarction in selected patients, even though 38% of patients had stenosis or occlusion of the contralateral ICA, and 89% of patients had an incomplete CoW. Only in 1 patient we cannot determine with certainty, whether contralateral infarction was due to our thrombectomy and/or surgery or whether it would have occurred also without our doing.
Footnotes
Authors’ contributions
Principal author: author #1; Conception and design: all authors; Acquisition of data: all authors; Analysis and interpretation of data: all authors; Critically revising the article: all authors.
Declaration of Conflicting interest
Author #2: Consultancy: Stryker. Payment for Lectures: Bracco, Medtronic, Siemens, Stryker. Payment for Development of Educational Presentations: Bracco, Codman, Medtronic, Phenox, Siemens. Other authors: none.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics statement
Data for this study were based on our stroke registry after obtaining ethical approval from our local ethics board with number EK 335/15.