
Abstract
Background:
Significant geographical variations exist in amputation rates and utilization of diagnostic and therapeutic vascular procedures before lower extremity amputations in the United States. The purpose of this study was to evaluate the rates of diagnostic and therapeutic vascular procedures in the year prior to amputation in a contemporary population and correlate with pathological findings of the amputation specimens.
Methods:
A retrospective analysis was conducted of non-traumatic amputations from 2011 to 2017 at a rural community hospital. We reviewed the proportion of patients undergoing diagnostic (ankle brachial index with duplex ultrasound, computerized tomography angiogram and invasive angiogram) and therapeutic (endovascular and surgical revascularization) vascular procedures in the year prior to amputation. Prevalence of tissue viability and osteomyelitis were evaluated in all amputated specimens and atherosclerotic vascular disease (ASVD) was evaluated in major amputations. We also analyzed primary amputation rates among different subgroups.
Results:
698 patients were included with 248 (36%) major amputations and 450 (64%) minor amputations. Any diagnostic procedure was performed in 59% of the major amputations and 49% of the minor amputations (P = 0.01). Any therapeutic revascularization procedure was performed in 34% of the major amputations and 28% of the minor amputations (P = 0.08). The pathology of major amputation specimens revealed severe ASVD in 57% and mild-moderate ASVD in 27% of specimens. Tissue viability was significantly higher in major amputations (90% vs 30%, P = 0.04) and osteomyelitis was significantly higher in minor amputations (50% vs 14%, P = 0.03). Primary amputations were performed in 66% of major amputations, 72% of minor amputations, 81% with mild to moderate ASVD and 54% with severe ASVD.
Conclusion:
Diagnostic and therapeutic vascular procedures appear under-utilized for patients undergoing lower extremity amputations at a rural community hospital. ASVD rates and tissue viability imply that revascularization could be of significant benefit to avoid major amputation.
Keywords
Introduction
Peripheral arterial disease (PAD) of the lower extremities is prevalent in approximately 8.5 million Americans and 1-3% of these patients progress to its most severe manifestation of critical limb ischemia (CLI). 1,2 PAD is the leading contributor of lower extremity amputations with more than 185,000 occurring annually in the United States. 3,4 Primary amputations, defined as without prior revascularizations, are associated with poor quality of life, increased mortality, and health care costs. 5 -9
The current guidelines from the American Heart Association/American College of Cardiology recommend that patients at risk for amputation undergo anatomic arterial testing and evaluation for revascularization. 10 However, large Medicare studies have shown a significant disparity in diagnostic and therapeutic vascular procedures performed prior to amputation. 11 -13 These studies also identified significant geographical variations in utilization of vascular studies and revascularization, with a high incidence of amputations occurring in certain regions in the United States. The state of Texas has one of the highest amputation rates, accounting for 9.2% of the total amputations in the United States, 14 at the same time revascularization rates had indeed been declining. 15 A previous population-based study from 2007–2009 observed a possible inverse relationship in low intensity of vascular care and subsequent amputations. 13 With recent advancements in medical therapy, revascularizations and reinforcement from vascular society guidelines, it was hypothesized that proportion of diagnostic and therapeutic revascularizations should be higher in contemporary practice. 16 -18
Non traumatic lower extremity amputations are presumed to be predominantly due to CLI, though the true prevalence and severity of atherosclerotic vascular disease (ASVD) remains unknown since vascular studies are not routinely preformed and primary amputation remains a common first line of treatment. There are only limited studies that have evaluated rates of ASVD and tissue viability in amputated specimens. 19,20
The purpose of this study was to 1) evaluate the utilization of diagnostic and therapeutic vascular procedures prior to major and minor amputation in a contemporary population at a community hospital with higher amputation rates and 2) correlate with pathological findings in the amputated specimen to gain a better insight into indications for amputation and potential value of revascularization in these patients.
Methods
A retrospective chart review was conducted on all patients who underwent lower extremity amputations at a rural community hospital in Texas from 2011 to 2017. Patients were identified using the Internal Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) and ICD-10 codes for amputation (Online Appendix I). Amputations related to a traumatic event or cancer were excluded from the study. Institutional review board approval for this study was obtained from the Western Institutional Review Board (Study #1180763) and the requirement for informed consent was waived.
Baseline Demographics
Charts were reviewed for baseline demographics including age, gender, race/ethnicity, and history of hypertension, hyperlipidemia, coronary artery disease, PAD, diabetes mellitus, smoking, obesity (body mass index >30), and chronic kidney disease (glomerular filtration rate ≤ 60 mL/min/1.73m2). Smoking was considered present if the patient was a current or former smoker. History of prior amputation and history of endovascular or surgical revascularizations greater than 1 year prior to the index amputation procedure were recorded. Clinical presentations including osteomyelitis, non-healing wound, and gangrene were also collected.
Amputations
Lower extremity amputations were divided into 2 cohorts based on the level of amputation: major or minor. Major amputations were defined as transection occurring proximal to the tarsometatarsal joint which included transtibial, below-the-knee and above-the-knee amputations. Minor amputations were defined as transection occurring distal to the tarsometatarsal joint which included toe(s), transmetatarsal, Chopart, and Lisfranc amputations. The first amputation, either major or minor, that a patient received during the study period was classified as the index amputation. Any subsequent amputation(s) in the same patient were excluded from this analysis.
Diagnostic and Therapeutic Vascular Procedures
Hospital medical records were reviewed to collect information regarding any vascular procedures in the year prior to the index amputation. The diagnostic vascular procedures collected included duplex ultrasound with or without ankle brachial index (DUS+/-ABI), computed tomography angiography (CTA) and invasive diagnostic peripheral angiogram. Therapeutic procedures included surgical and endovascular revascularization attempts.
Pathology Examination
The pathology of each amputation specimen was routinely examined and reported by pathologists within this institution. Information was collected regarding viability of tissue margins, osteomyelitis, and ASVD.
Absence of necrosis or gangrene, with presence of nucleoli by microscopy was defined as viable tissue at the proximal margin. Presence of necrosis, gangrene and absence of nucleoli by microscopy was defined as non-viable tissue. The presence or absence of osteomyelitis by microscopy was also collected.
Histopathology was routinely examined in major amputation specimens at the proximal margins. The entirety of the vessels was not consistently probed or examined at this institution. The presence and severity of ASVD was determined by the atherosclerotic burden described in the histopathology report. Severity of ASVD was described as none, mild to moderate, or severe. If there was no intimal narrowing, then ASVD grading was none. Mild to moderate ASVD was reported as 10% to 90% luminal narrowing. Severe ASVD was reported to be greater than 90% luminal narrowing or complete occlusion of the vascular lumen. Presence of ASVD was not consistently reported in the minor amputation specimens and therefore not reported in this study.
Primary and Secondary Amputation
Primary amputation was defined as patients who underwent amputations without any revascularization attempt. Secondary amputation was defined as patients who underwent amputations after a revascularization attempt.
Statistical Analysis
XLSTAT (2018; Data Analysis and Statistical Solution for Microsoft Excel. Addinsoft, Paris, France) software was used for data collection and statistical analysis. Values presented are n (%) or mean ± standard deviation. P-values for quantitative variables are from the Mann-Whitney U test. P-values for qualitative variables are from the Chi-square test or the Fisher’s exact test (if theoretical frequencies were < 5).
Results
Figure 1 is a flow diagram demonstrating the selection of patients. A total of 989 records were identified for lower extremity amputations during 2011-2017. From these records, 270 patients who had repeat amputations were excluded. There were 719 identified with index amputation, of these, 21 patients were excluded due to trauma related (n = 18) or cancer related (n = 3) amputations. A total of 698 patients with index amputations were included in the final study with 248 (36%) major amputations and 450 (64%) minor amputations.
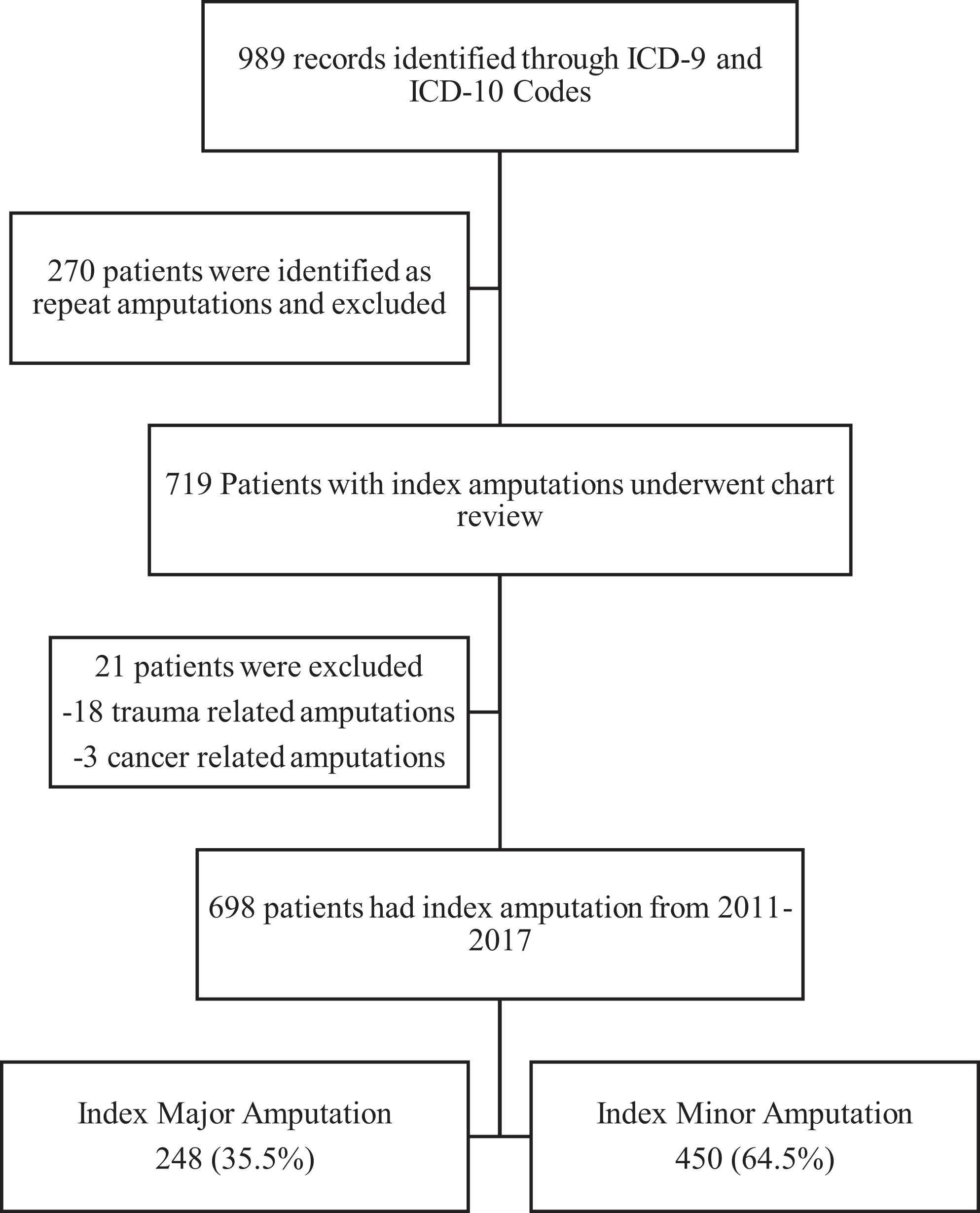
Flow diagram of study selection.
Baseline Characteristics
Baseline characteristics of major and minor amputation patients are described in Table 1. Patients undergoing major amputations had higher prevalence of PAD (57% vs 37%, P < 0.0001), prior amputation (29% vs 22%, P = 0.036), prior endovascular revascularization (25% vs 14%, P < 0.0001), prior surgical revascularization (16% vs 2%, P < 0.0001) and more often presented with gangrene (52% vs 42%, P = 0.013). Patients undergoing major amputations had a lower prevalence of diabetes mellitus (65% vs 79%, P < 0.0001), osteomyelitis (9% vs 29%, P < 0.0001) and wound at presentation (90% vs 97%, P < 0.0001).
Patient Baseline Demographics.
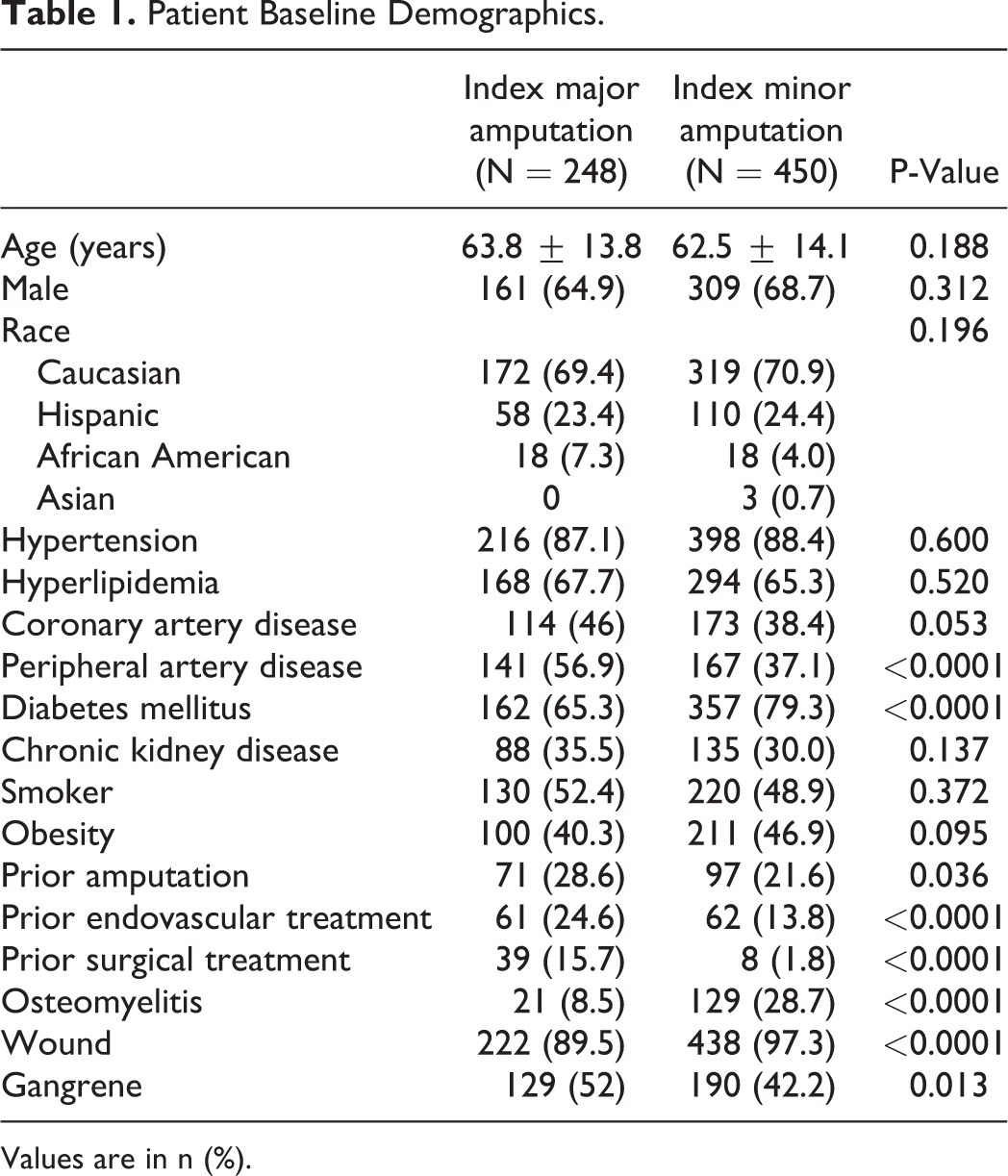
Values are in n (%).
Diagnostic Vascular Procedures
Figure 2 demonstrates the proportion of diagnostic vascular procedures performed in the year prior to major and minor amputations. Among the patients with major amputations 59% had at least one diagnostic procedure compared to 49% for patients undergoing minor amputations (P = 0.013). There was no difference in DUS+/-ABI between major and minor amputations (P = 0.973). CTA was performed in 31% of major amputations and 14% in minor amputations (P < 0.0001). Invasive diagnostic angiography was performed in 29% of patients in the year prior to major amputation and 28% in the year prior to minor amputation (P = 0.909).
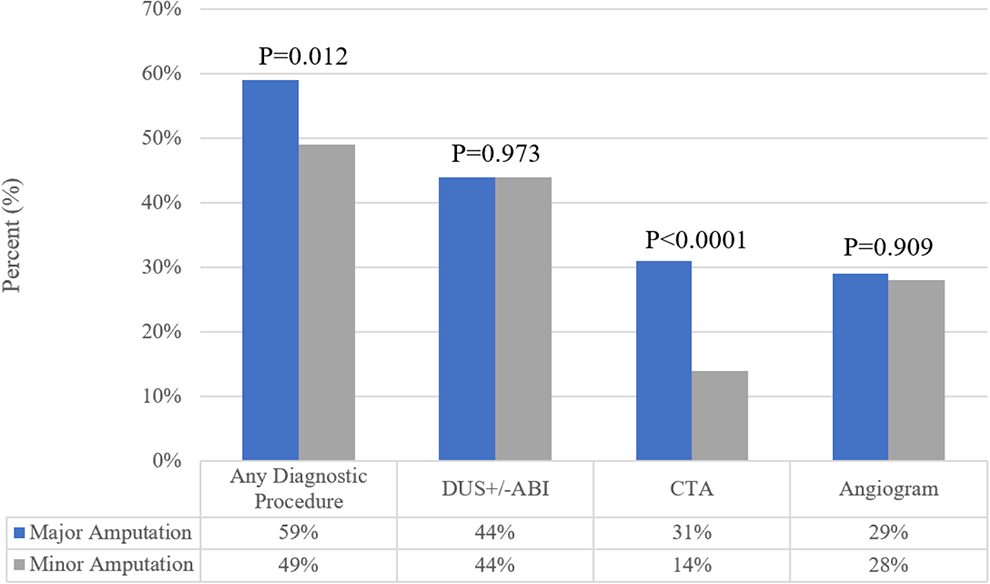
Bar graph demonstrating the rates of diagnostic vascular procedures prior to major or minor amputation.
Revascularization
Figure 3 demonstrates the rates of therapeutic revascularizations in the year prior to major and minor amputations. Rates of any revascularization was 34% in major amputations and 28% in minor amputations (P = 0.081). Endovascular revascularization rates were similar before major and minor amputations (25% vs. 26%, P = 0.941). Surgical revascularization was higher in major amputation compared to minor amputation (12% vs. 2%, P < 0.0001).
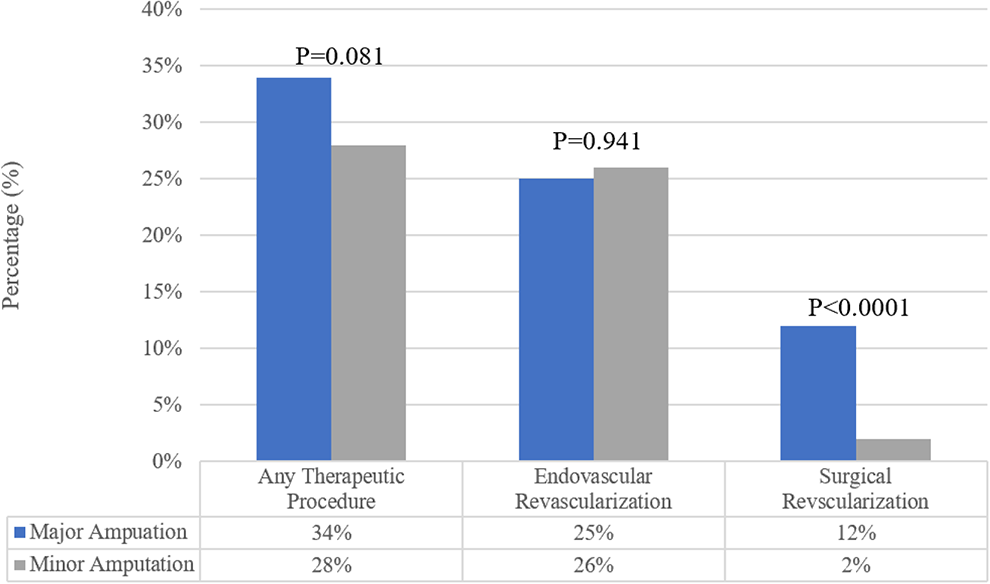
Bar graph demonstrating the rates of therapeutic vascular interventions prior to major or minor amputations.
Pathology
The reported pathology findings among major and minor amputations are described in Table 2. Among major amputations, severe ASVD was seen in 57%, mild-moderate in 27%, and no ASVD in 13%. Tissue viability at margins on the amputated specimens were seen in 90% of the major amputations compared to 30% in the minor amputations (P = 0.042). Osteomyelitis was seen in only 14% of the major amputations compared to 50% of the minor amputation specimens (P = 0.032).
Different Pathological Specifics of the Major and Minor Amputations.
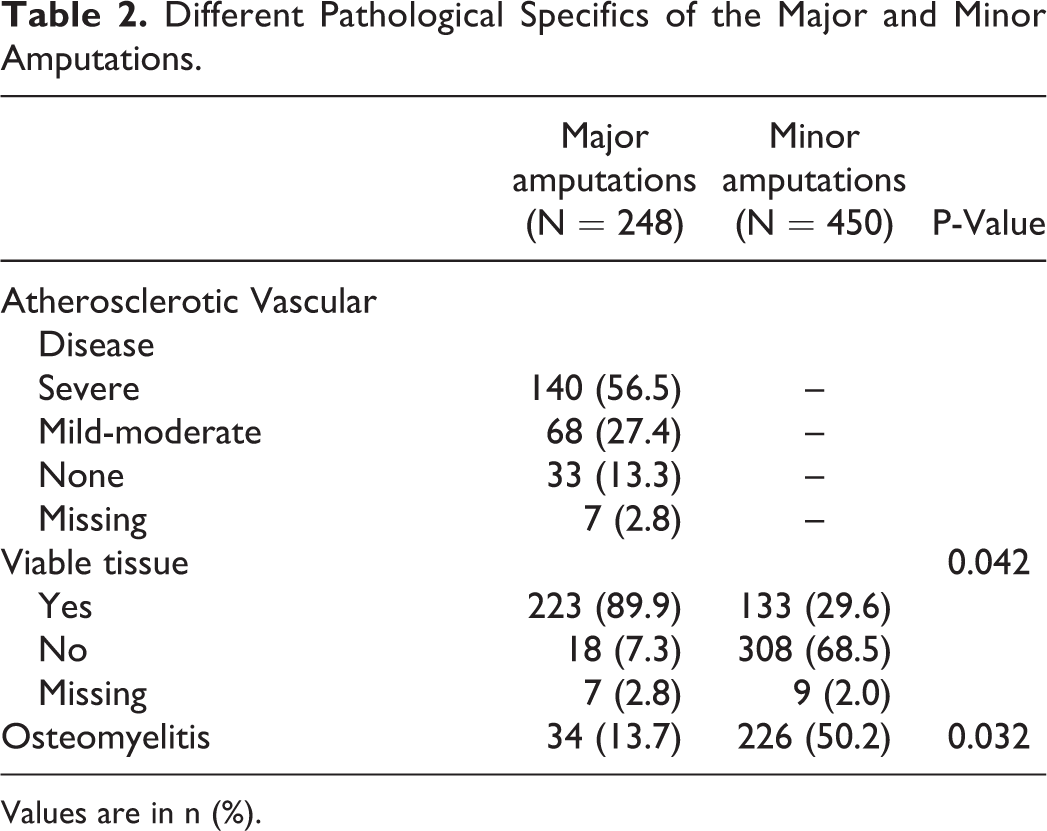
Values are in n (%).
Table 3 compares the difference between diagnostic vascular procedures and revascularization procedures based on severity of ASVD identified by pathology. Severe ASVD had a higher probability of having any diagnostic vascular procedures (P < 0.0001) and any therapeutic revascularizations (P < 0.0001) compared to mild to moderate ASVD.
Diagnostic and Therapeutic Procedures for Patients Identified to Have Atherosclerotic Vascular Disease (ASVD) by Pathology.
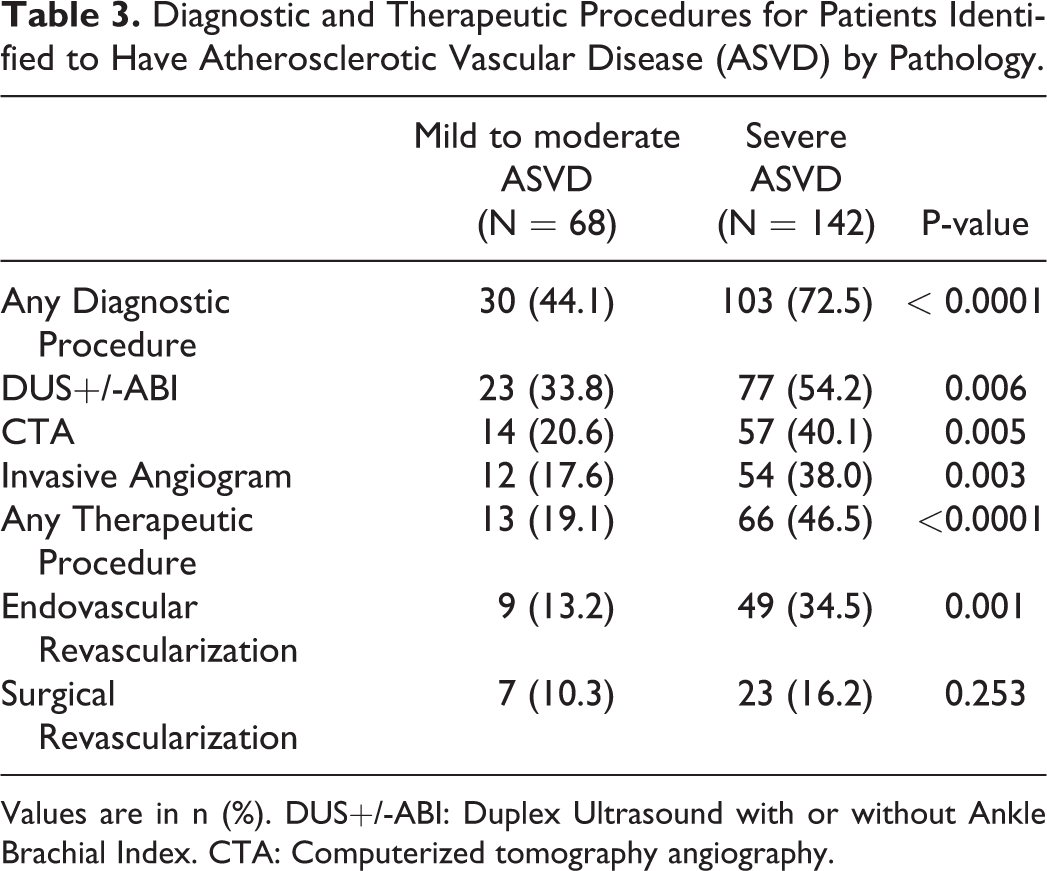
Values are in n (%). DUS+/-ABI: Duplex Ultrasound with or without Ankle Brachial Index. CTA: Computerized tomography angiography.
Primary and Secondary Amputations
Figure 4 demonstrates primary and secondary amputation rates in the subgroups based on level of amputation and degree of ASVD. Among patients with major amputations, 66% of patients received primary amputation and 34% received secondary amputation. Among patients with minor amputations, 72% received primary amputation and 28% received secondary amputation. In patients with severe ASVD, 54% had primary amputations and 46% had secondary amputations. In patients with mild to moderate ASVD, 81% had primary amputations and 19% had secondary amputations.
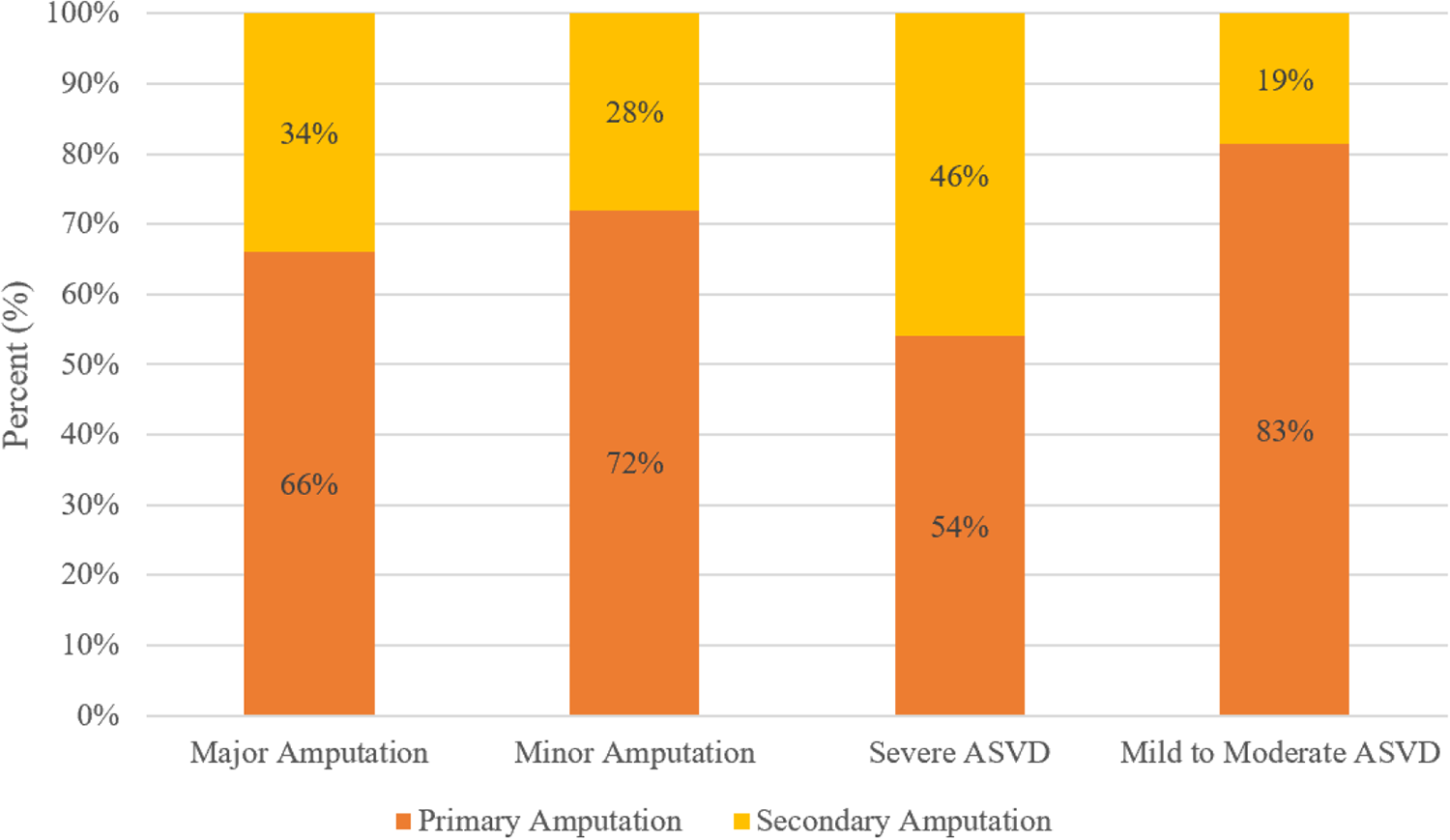
Primary and secondary amputation rates based on the subgroups of major amputation, minor amputation, and degree of atherosclerotic vascular disease (ASVD).
Discussion
The main findings of this study were 1) only 59% of patients undergoing major amputations and 49% of patients undergoing minor amputations received any diagnostic vascular evaluations in the year prior to amputation, 2) only 34% of the patients undergoing major amputations and 28% of the patients undergoing minor amputations received any therapeutic vascular interventions in the year prior to amputation, and 3) pathology of major amputated specimens demonstrated that any degree of ASVD was identified in 84% and viability of the tissue margins were identified in 90% of specimens, whereas pathology in minor amputated specimens more often identified osteomyelitis.
Non-invasive vascular studies are likely the first evaluation to be performed for CLI patients and should result in subsequent referral to a vascular specialist for revascularization, as it is the preferred initial therapy for CLI. 21,22 Although the optimal amount of pre-amputation arterial testing is not yet defined, not performing arterial evaluation undoubtedly contributes to loss of opportunity for limb salvage, as well as the potential to convert a major amputation to a minor amputation. Indeed, small studies have demonstrated favorable 1-year survival and amputation-free survival with the use of aggressive screening and revascularization programs in patients facing amputation. 23 Unfortunately, this study demonstrates that a significant proportion of patients still did not undergo any diagnostic or therapeutic vascular procedures in the year prior to amputation, resulting in a high rate of primary amputations in the contemporary era.
There is a myriad of potential reasons for lower pre-amputation vascular evaluation and treatment in this real-world community hospital experience. Late clinical presentations for CLI is one potential reason, as 95% of patients presented with a wound, 46% with gangrene and 21% with osteomyelitis, and these limbs may have been presumed to be non-salvageable. The scarcity of dedicated vascular specialty care in this area could be contributing to this disparity as well. Most importantly, this institution did not have a multi-disciplinary team which could have caused direct referral for primary amputation with the intention for “permanent cure,” as opposed to a group discussion of all treatment options and methodical diagnosis and assessment prior to choice of therapy.
This is the first study, to our knowledge, evaluating histopathology and prevalence of ASVD (major amputation), tissue viability and osteomyelitis in all patients undergoing lower extremity amputations. Our findings of higher prevalence of ASVD and viability among major amputation specimens help validate the argument that vascular studies should be pre-requisite before any major amputation. Even among pathologically proven ASVD patients, the diagnostic and therapeutic revascularization procedures are significantly underutilized. In addition, the high percentage of patients with major amputations and tissue viability at proximal margins implies that revascularization may have been able to convert at least a subset of these patients to minor amputation.
Compared to major amputations, tissue viability was only 30% at the amputated margins and presence of osteomyelitis was identified in 50% of the minor amputation specimens. These findings could partially justify primary minor amputation as the initial treatment option without prior vascular evaluation. However, pre-amputation vascular evaluations even when considering minor amputation would give more comprehensive understanding of the vasculature, which is a critical component in wound healing. In addition, it is likely that vascular evaluation could have avoided repeat, more proximal, amputations in this patient population (270 repeat amputations observed in this study—which were excluded from this analysis).
Patients with extensive wounds, severe concomitant infections, and patients with limited life expectancy may benefit from primary amputation. 24 In addition, patients with prior failed revascularization attempts or extremely challenging vascular anatomy may eventually require primary or secondary amputation. There could be similar patients who received amputations in this study, nevertheless, primary amputation rate of 54% even in patients with severe ASVD could have been decreased with aggressive revascularization strategies. In carefully selected patients with either revascularization approach, the rate of primary amputations can be reduced to as low as 10% as previously demonstrated. 25,26
The absence of claudication symptoms, under recognition that a given wound may have arterial etiology, limitations of different noninvasive imaging modalities, limited access to advanced vascular specialists and underutilization of modern revascularization options are some of the potential barriers to proper vascular evaluation before amputations, and may have led to the very high rate of primary amputation in this study. In addition, community awareness to avoid late presentation is a large factor, especially in rural communities. Also, multiple point of care entry such as emergency departments, primary care clinics, specialty clinics, wound care centers, podiatry offices and inpatient facilities may result in lack of coordination of care for CLI patients, and inadvertent direct referral to surgeons for amputation. To achieve a coordinated care pathway, national guidelines and consensus documents support the establishment of CLI/Limb Salvage teams. These teams could not only increase the rates of pre-amputation vascular evaluations and revascularizations, but also decrease the potential delay for futile revascularization attempts. 23,26 In other words, they are key to both evaluation and case selection for revascularization versus amputation. Further research is needed to assess and validate the impact of CLI teams in rural areas.
Limitations
This is a single center retrospective study and results may not be generalizable, but these findings can give insight into the potential barriers at similar hospitals with high amputation rates. This study does not provide definite reasons for reduced vascular procedures, as they were multifactorial and not documented. There is a possibility that we underestimated the amount of non-invasive studies (DUS+/-ABI) preformed as some could have been performed at an outside facility. We searched extensively in our medical records to avoid this confounding factor and the low percentage of angiography reassures our numbers could be accurate. Our pathology reports evaluated only the proximal margins of amputated specimens and 10-90% stenosis was reported as mild to moderate. However, this liberal definition would have more likely underestimated the prevalence of ASVD in this population.
Conclusion
This study demonstrates that primary amputation rates remain high in a large rural community hospital and that pre-amputation diagnostic and therapeutic procedures appear to be significantly under-utilized overall and even among patients with proven ASVD. Establishment of CLI multidisciplinary teams and hospital level protocols may improve pre-amputation vascular evaluations and revascularization rates in order to attempt to reduce primary and secondary amputation rates and improve morbidity, mortality and health care costs in rural communities.
Supplemental Material
SUPPLEMENTAL_MATERIAL - Utilization Rates of Diagnostic and Therapeutic Vascular Procedures Among Patients Undergoing Lower Extremity Amputations in a Rural Community Hospital: A Clinicopathological Correlation
SUPPLEMENTAL_MATERIAL for Utilization Rates of Diagnostic and Therapeutic Vascular Procedures Among Patients Undergoing Lower Extremity Amputations in a Rural Community Hospital: A Clinicopathological Correlation by Joji J. Varghese, Bailey Ann Estes, Brad J. Martinsen, Zsuzsanna Igyarto, Jihad Mustapha, Fadi Saab and Srihari S. Naidu in Vascular and Endovascular Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Brad J Martinsen—Employed by and owns stock in Cardiovascular Systems, Inc.; Zsuzsanna Igyarto—Employed by and owns stock in Cardiovascular Systems, Inc.; Jihad Mustapha—Consulting agreements with Boston Scientific (BSc), Cardiovascular Systems, Inc (CSI), Bard Peripheral Vascular (BPV), Terumo Medical, and Philips; Fadi Saab—Consulting agreements with Boston Scientific (BSc), Cardiovascular Systems, Inc (CSI), Bard Peripheral Vascular (BPV), Terumo Medical, and Philips.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Institutional support from Hendrick Medical Center, Abilene, Texas 79602.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.