
Abstract
Katherine Beckett and Craig Reinarman on reducing overdose deaths.
The United States has the world’s highest rate of overdose deaths. According to the Centers for Disease Control, more than 100,000 Americans have died from overdose each year since 2021—more than from gun shots and car crashes combined. By 2023, scholars Alison Athey, Beau Kilmer, and Julie Cerel reported in the American Journal of Public Health (AJPH), one in four Americans knew someone who died by overdose. Over two-thirds of these fatalities—nearly 200 per day— involved synthetic opioids, mainly fentanyl, per the National Institute on Drug Abuse. And meth-related deaths and disease are spiking as new, even more powerful and toxic forms of methamphetamine flood the market (as reported in AJPH by researchers Rachel A. Hoopsick and R. Andrew Yockey in 2023).
There is significant debate about the best way to respond to this crisis. In recent years, drug policy has swung away from punitive drug-war tactics and toward public health-based harm reduction approaches. Harm reduction rests on the premise that while all drug use entails risks, attempts to eliminate it entirely have failed. Indeed, using punishment to try to deter drug use and eliminate illegal drug markets has itself caused significant harm, including by spurring the development of new synthetic drugs like fentanyl.
Some media outlets fuel public alarm, cultivating fear and heightening the desire to "get tough" on people who use drugs.
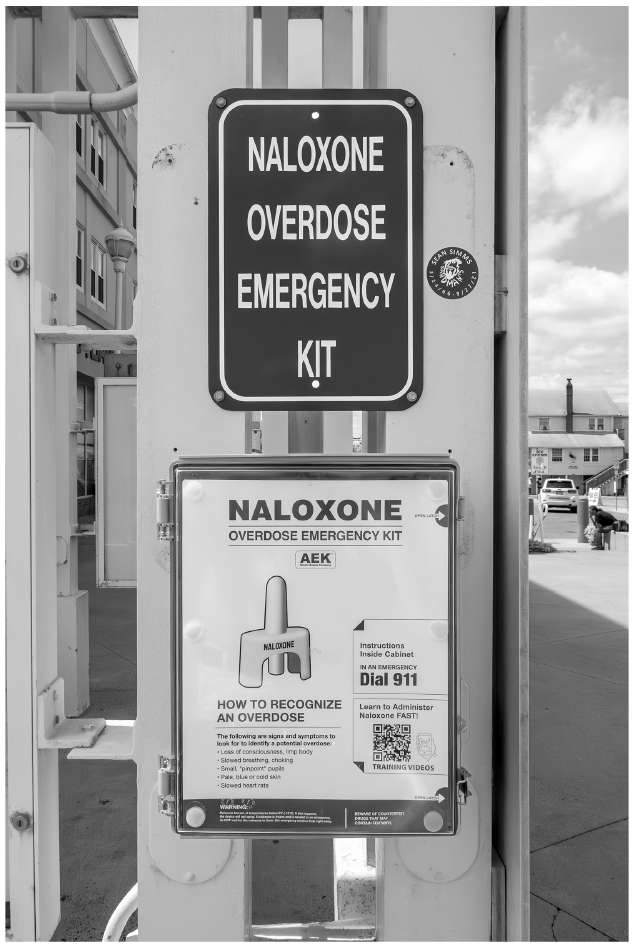
Advocates argue that since drugs cannot be made to go away, policy should focus on reducing the harms associated with their use. Harm reduction policies begin by “meeting drug users where they are,” without judgment, and helping them avoid some of the worst possible outcomes associated with continued drug use. Distributing naloxone, a medication used to reverse overdoses, for example, saves lives and helps to explain the recent downtick in overdose deaths. Similarly, providing sterile syringes to people who inject drugs has dramatically reduced the spread of HIV/AIDS and hepatitis C. Harm reduction approaches also include medicine-assisted treatment for opiate use disorder—maintaining dependent users on methadone, buprenorphine, or diamorphine (prescription heroin)—an approach that research shows is the most effective treatment available and reduces the risk of overdose by half.
Since the 1990s, harm reduction policies have spread to dozens of countries around the globe. Their effectiveness is now widely recognized, including by the World Health Organization, the American Medical Association, the American Public Health Association, the Centers for Disease Control, and the National Academy of Sciences. To be sure, harm reduction policies do not reduce all of the harm and violence associated with illicit drug markets. Nor do they provide a solution to the marginalization and dispossession that underlie the most destructive forms of drug misuse. But they can, and do, reduce the disease and death caused by illicit drugs.
Despite their clear benefits, pundits and politicians have blamed harm reduction policies for the rise in overdose deaths and the apparent increase in public drug use. Even where there is broad support for harm reduction principles, efforts to open harm reduction services (such as syringe exchange facilities) in particular places often trigger neighborhood opposition and support for tougher alternatives. Some media outlets fuel public alarm and encourage a return to drug-war tactics, flooding the zone with images of people openly smoking fentanyl on city streets, homeless encampments in which used syringes crunch underfoot, and hard drug users shooting up on sidewalks. Together with related coverage of brazen smash-and-grab robberies and rampant shoplifting, these stories cultivate fear and heighten the desire to “get tough” on people who use drugs.
From this perspective, the renewal of drug-war tactics is a badly needed (and all but inevitable) corrective to harm reduction policies run amok. A recent New York Times headline, for example, declared “Liberal Berkeley’s Toughened Stance on Homeless Camps Is a Bellwether.” Such stories tend to reiterate false claims about the efficacy of criminal sanctions, but many voters are once again receptive to more punitive approaches to the drug crisis. Progressive district attorneys in San Francisco, Oakland, and Los Angeles—proponents of alternatives to arrest—have been voted out in recall initiatives. Last November voters also ousted the Mayor of San Francisco who, despite her conversion to tougher law-and-order drug policies, was unable to make much of a dent in her city’s drug problems. Similarly, a strong majority of California voters recently passed Proposition 36, which reinstated penalties for drug possession and other non-violent crimes. In 2024, Oregon voters, too, repealed Measure 110, a bold experiment in drug decriminalization that they had supported by a significant margin just a few years earlier.
Distributing naloxone, a medication used to reverse overdoses, as Ocean City, Maryland does, is an example of a harm reduction strategy that saves lives (helps to explain the recent downtick in opiate overdose deaths).
iStockPhoto.com // Alexander Farnsworth
the debate over stigma
In short, the overdose crisis, the apparent increase in outdoor drug use, and media coverage of these challenges has sparked opposition to reforms like harm reduction. Some observers have even called for the re-stigmatization of drug use. In their view, some public health education and outreach strategies that seek to avoid stigmatizing people who use drugs have gone too far. Such campaigns encourage people who use drugs not to feel shame, but rather to take more control of their health by using with other people rather than alone, employing safer modes of ingestion, and seeking treatment.
Prominent critics have argued that by withholding moral judgment, such messages signal society’s approval of dangerous drug use and weaken the coercive incentives needed to induce people to get help and quit using drugs. In their view, addiction is unlike other diseases because the people who suffer from it do not necessarily want to be cured. The solution, they believe, is to re-stigmatize drug use, both to deter it and to pressure people who use drugs into treatment.
We agree that public health messaging should take care not to romanticize drug use, especially in the fentanyl era. It’s also worth noting that these critics are calling for the re-stigmatization of a behavior (drug use) rather than the people who use drugs. Yet it’s not at all clear that we actually can stigmatize drugs without also stigmatizing the people who use them.
The call for re-stigmatization also ignores ample evidence that people who use drugs already experience tremendous stigma. Experimental studies such as those discussed by Finelle in Substance Abuse (2018), for example, show that exposure to images of people who use drugs elicits strong, negative emotions, including disgust. Survey research confirms that most people hold negative beliefs and stereotypes about people who use drugs. As reported by addiction experts Anthony Cazalis, Laura Lambert, and Marc Auriacombe in Drug and Alcohol Dependence Reports in 2023, these perceptions and attitudes are widespread even among health care professionals (some of whom are unwilling to work with people with opioid use disorder and many of whom believe that the condition is solely the responsibility of the individual patient).
This means that the stigma experienced by people who use drugs remains both deep and pervasive. Research further shows that this stigma compounds drug-related harm. For example, many people who use drugs identify stigma and discrimination as barriers to seeking treatment, as shown by Kathleen A. Crapanzano and colleagues in Substance Abuse and Rehabilitation (2018). Stigma also breeds isolation, encourages less safe ways of using drugs, and pushes people who use drugs to the margins of society where moderating conventional norms lose sway. When stigmatization results in a criminal record, it shrinks opportunities for drug users to return to the fold. Plus, there’s little evidence that stigma is an effective prevention strategy. The United States conducted a century-long drug policy experiment to see if more stigma, shame, and imprisonment would turn the tide. They didn’t.
Perhaps the best argument against re-stigmatization comes from the anti-smoking movement, which cut the prevalence of tobacco use by roughly half. Stigmatization was not the main driver of the marked decline. Instead, beginning with the U.S. Surgeon General’s 1964 report, the anti-smoking campaign was rooted in science-based public health education, informing people of real risks without overt judgment or the threat of arrest. This campaign took nicotine addiction seriously, understanding that smoking is more than a matter of free choice. Anti-smoking policies restricted sales, eliminated mass advertising, used taxation to increase prices, and shrunk the spaces where smoking is permitted (not long ago there were ashtrays on every restaurant table!). Tools for quitting smoking were made widely available, with nicotine gum and transdermal patches sold in supermarkets without a prescription. By contrast, in the United States, medicine-assisted treatment for opiate dependence has been restricted to specially licensed physicians and clinics and is still disallowed by some treatment providers and drug court judges.
the deeper causes of the crisis
The idea that recent harm reduction-informed public health messaging is responsible for the worsening drug crisis ignores the harm stigma causes. It also ignores the deeper causes of the crisis, including the impact of the powerful synthetic drugs now saturating global supply chains. In the United States and elsewhere, fentanyl is increasingly hidden in other illicit drugs, and while many long-term opioid users would prefer heroin, fentanyl has largely replaced it on the illicit market. In Canada and parts of Europe, nitazenes—synthetic opioids even more powerful than fentanyl—are wreaking havoc. New, more potent and toxic forms of methamphetamine also cause significant harm. As top U.S. Drug Enforcement Agency officials concluded in their 2024 National Threat Assessment, “The shift from plant-based drugs, like heroin and cocaine, to synthetic, chemical-based drugs, like fentanyl and methamphetamine, has resulted in the most dangerous and deadly drug crisis the United States has ever faced.”
"Long-term and transformational change will require addressing the structural factors that fuel dangerous drug use."
iStockPhoto.com // Nicola Colombo
Social dislocation, dispossession, and desperation amplify the damage done by these new and more potent synthetic drugs. The overdose epidemic cannot be understood apart from its social context: growing inequality, widespread housing precarity, underfunded mental health care, the absence of universal health care, and decades-long attacks on government’s capacity to assist people in need. These structural factors help to explain why the U.S. overdose death rate is, by a significant margin, the highest in the world.
Neither stigmatization nor criminalization addresses these structural drivers of drug-related harm. Harm reduction policies and individualistic public health strategies don’t either. Simply providing clean syringes or reversing an overdose and leaving people to return to their unchanged life circumstances helps keep them alive, but it is not enough. Long-term and transformational change will require addressing the circumstances that fuel dangerous drug use.
Still, of the current options, a multifaceted approach that leverages harm reduction measures—backed by key investments and programmatic changes—could meaningfully reduce drug-related harm. Along with medication-assisted treatment, diversion and deflection initiatives that provide an alternative to jail as well as long-term emotional and social support for people with behavioral health challenges have been found to be enormously helpful, as reported by harm reduction scholars Seema L. Clifasefi, Heather S. Lonczak, and Susan E. Collins in Crime and Delinquency in 2017. Adequately funded Housing First programs that provide low-barrier housing and intensive case management support for people experiencing mental health challenges and substance use disorder also dramatically reduce harm and unsheltered homelessness. And measures that increase access to affordable housing, including units that are open to people with criminal records and who use drugs, are clearly needed.
Even if these and other evidence-based approaches are scaled up, though, increasingly dangerous drugs will continue to pose real challenges and cause real harm. Tougher public health messaging will not fix this. The destruction fentanyl and other synthetic drugs now wreak cannot be curtailed by further stigmatizing some of the most vulnerable people in our communities. The drug crisis cannot be resolved without also addressing the broader conditions from which it springs.