
Abstract
The country faces a shortage of healthcare professionals, yet today's average U.S. medical school graduate carries an enormous debt burden. with roughly $200,000 in education loans, interviewees explain, exciting decisions about specialty paths become struggles between passion and pragmatism.

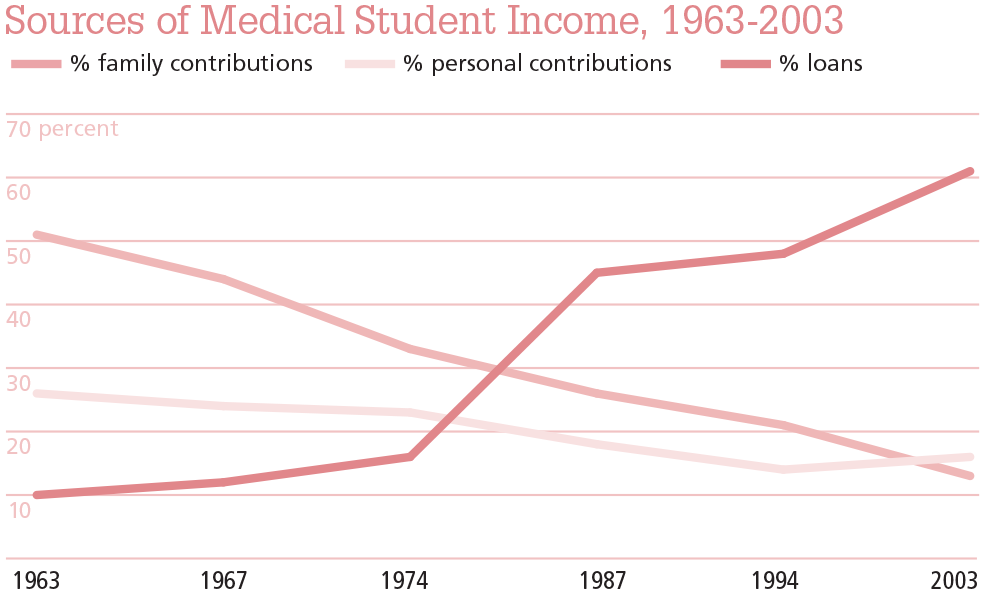
“I came in with undergrad debt that I still have, incurred $300,000-whatever dollars of debt for medical school. So, it’s huge. You would be foolish to not consider [debt]. What it really did is just push me away from [primary care] because there’s just no way that I can make a living to pay back my debt and have a good quality of life and be a family medicine doctor. And that, again, is the way our system is set up. Now, family medicine doctors just don’t make enough money.” As this fourth-year medical student entering residency for emergency medicine told us his story, we realized how very common it was: Cumulative debt for incoming physicians in the United States has ballooned in the last three decades (see Figure 1). Medical students at every stage of their education talked at length about the anxiety and precarity they felt when choosing a specialty. They didn’t want debt to figure into this decision, but like their fourth-year peer, they largely felt there was no ignoring the financial reality of their futures.
In this article, we share perspectives from our conversations with 33 medical students, situating their experiences within broader research in sociology and medicine and demonstrating the increased prevalence and complexity of medical school debt. In addition, we discuss how the accumulation of debt among new doctors contributes to a shortage of primary care physicians (including pediatricians) and potentially undermines physician well-being.
Educational debt affects physicians in multiple, varied, and unevenly distributed ways. For instance, pediatricians report relatively high job satisfaction, despite having some of the lowest incomes in the profession. But, as Aaron Carroll has demonstrated, fewer doctors appear to be pursuing pediatrics as a specialty in recent years, in line with projections for 2021 to 2036 which indicate a potential shortage of primary care physicians.
Sources: Jolly P. Medical School Tuition and Young Physician Indebtedness (Washington, DC: Association of American Medical Colleges; 2004. https://www.aamc.org/download/105366/data/mstuitionoriginal.pdf. Accessed March 22, 2011); Altenderfer ME, West MD. How Medical Student Finance Their Education: Results of a Survey of Medical and Osteopathic Students, 1963-1964 (Washington, DC: U.S. Department of Health, Education, and Welfare; 1965); Remund Smith LC, Crocker AR. How Medical Students Finance Their Education: Results of a Survey of Medical and Osteopathic Students, 1967-1968 (Washington, DC: U.S. Department of Health, Education, and Welfare; 1970); Crocker AR. How Medical Students Finance Their Education: Results of a Survey of Medical and Osteopathic Students, 1973-1974 (Washington, DC: U.S. Department of Health, Education, and Welfare; 1974).
Source: Reproduced from S. Ryan Greysen, Candice Chen, and Fitzhugh Mullan. 2011. “A History of Medical Student Debt: Observations and Implications for the Future of Medical Education,” Academic Medicine 86.
These trends prompt an unnerving question: Will the doctor see you now? Family care physicians and pediatricians, among other primary care providers, comprise our healthcare system’s first line of defense. Given that we don’t have enough of these professionals to make medical care more widely and equitably accessible in the United States, anything that contributes to the shortage must be investigated. And so, amid the undoubtedly complex factors that have created this care gap, we delved deeply into educational debt.
Medical students don’t want debt to figure into their career decisions, but they largely feel they can’t ignore financial pressures.
iStockPhoto // Drazen Zigic
residency placements and the supply of physicians
A 2019 Association of American Medical Colleges (AAMC) News Brief speculated that, if more medical schools waived tuition for students who would require loans—or even for all students—more medical school graduates would pursue primary care. The rationale was that aspiring physicians who carried less debt (or none at all) would find earning potential a less salient factor in their residency specialty decisions. After all, an article in U.S. News & World Report indicated that, in 2022, U.S. medical students graduated with an average debt burden of more than $200,000 (and that’s without counting any debt they might still have from their undergraduate education). Providing partial support for this hypothesis, a study examining residency choice among medical school students from 2010 found that debt influenced residency choice among public (though not private) medical school graduates. A more recent study found evidence that high levels of educational debt and considerations of future income discouraged many osteopathic medical students from pursuing primary care. Our interviews with medical students at a private allopathic (that is, traditional western) medical school provide further evidence that debt influences residency choice. We also observe widespread skepticism regarding the potential for the small handful of medical schools now offering free tui-tion—whether to some students or to all—to produce enough graduates to meet existing primary care needs.
Projections from 2021 to 2036 indicate a future shortage of primary care physicians on the magnitude of 20,000 to 40,000 unfulfilled roles (if medically underserved populations accessed health care at the same rate as more privileged communities, the projected gap would be even greater). Within the broader field of primary care, pediatrics recently experienced an alarming drop in residency placements—according to a recent American Medical Association (AMA) News Brief, the residency fill rate in pediatrics fell from 97% in 2023 to 92% in 2024. Family medicine has similarly experienced shortages; per MedScape, only 88% of family medicine residency positions were filled in the 2024 Match.
debt and residency decisions
A systematic review published in 2023 indicates that the majority of medical students use loans to pay for at least a portion of their medical education. The same study reports that medical school debt is a significant source of stress and anxiety for medical residents and that it influences decisions to pursue medical subspecialties other than primary care. Debt appears to deter the pursuit of academic medicine (that is, work in medical centers where physicians train prospective physicians and do research in addition to treating patients—positions that typically come with prestige but comparatively lower incomes), and it appears to decrease the likelihood that a physician will seek further training after residency.
Similar patterns have been observed within medical specialties. A 2020 study of emergency medicine residents suggests that debt reduces the likelihood of male residents seeking academic careers, such as faculty positions or academic fellowships. Family medicine residents with high debt are less likely to seek work in a government organization, and those with high debt or very high debt are less likely to pursue academic careers or geriatric fellowships. Taken together, research warns that high educational debt burdens may exacerbate shortages of academic, geriatric, and primary care physicians. Loan forgiveness programs are too few and too narrow to reverse these trends on their own.
debt horizons and anxiety
Our study draws on qualitative interviews with 33 medical students at a private allopathic medical school in the Midwest. We included students across all four years of medical school, oversampling students in their third and fourth years (we conducted 8 interviews with first- and second-year students and 25 interviews with third- and fourth-year students). We took this approach because we wanted to include as many students with clinical experience (typically completed during the second two years of the program) as possible while also gaining the perspectives of first- and second-year students. In the interviews, we asked a range of questions about students’ experiences with and perspectives on their medical education. We also included an elicitation element in our interviews in which we shared excerpts from a classic sociological text on medical education in the 1950s (sociologist Howard S. Becker and colleagues’ Boys in White), then asked students to compare their own experiences to those described by medical students from a prior generation. This process led interviewees to reflect on elements of the institutional environment that had changed or persisted over time.
Quickly, the current medical students brought our attention to the rise in the cost of (and therefore debt from) attending and completing medical school. Especially among students in the latter half of their medical training—the ones closest to choosing their professional paths—the prospect of future debt repayment loomed large. Like the student quoted in the opening of this piece, few medical students would prefer to make this big career decision on the basis of salary, yet many feel they must. Evelyn, a third-year student who estimated her current debt load at about $600,000 from college, graduate school, and medical school combined, was straightforward: “The debt is suffocating, to be honest. And then it’s also really frustrating, because I knew I wanted to do hema[tology], right? So, for several months, I’ve been saying, ‘Okay, I need to decide between adults or kids….’ And when I made my list of pros and cons, one of the things that I put towards the bottom of the list, but still on the list, is that adult [hematology] pays way more money. Adults pay about $150,000 a year more....” In choosing a medical specialty, Evelyn advised, “It’s not worth making your entire decision on money. But I do think realistically you should make it a factor.”
Other medical students shared similar sentiments. One fourth-year student described the educational debt as “insane,” while another lamented that there was a certain amount of stigma associated with having to consider cumulative debt: “I think it’s on most people’s minds, but it’s a little bit taboo to talk about. Because we need to be ‘all for the patient’.. We’re not here for the money.” That jibes with a study by Mary Dunn and Candace Jones, who reported that medical students identified concern for their patients as the primary motivation behind their chosen career paths—perhaps even those students felt nervous to admit to their debt repayment woes.
As medical students begin to look toward their futures, educational debt can limit their imaginations.
iStockPhoto // Jacob Wackerhausen
Of course, debt does not affect all medical students equally. William Cull and colleagues found, for instance, that nearly a quarter of pediatricians reported over $150,000 in debt, but nearly 30% had no debt at all (the authors note that these data are from people who completed residency between 2002 and 2004; both the prevalence and the magnitude of educational loans have increased since then). Our interviews reveal how this socioeconomic inequality plays out among medical students such that even those students not directly affected by debt feel its effects second-hand. Bianca, a third-year medical student, expressed concern about others discovering her lack of debt. She confirmed that the interview was confidential before sharing, “I am very fortunate where my parents are helping me out [financially] with med school. And I truly think that if they weren’t—I don’t know [if] I could have gone into medicine, because the thought of having $200,000 to $300,000 in debt is very scary to me. So, I was very fortunate in that I didn’t really have to worry about that in my decision-making.”
Especially among students in the latter half of their medical training the prospect of future debt repayment loomed large.
Making a similar point, third-year student Tiffany explained how she saw debt impacting her friends’ decision-making: “I know I’ve had experiences with med students [who] originally really wanted to do something like family medicine... But then, like later on, they’re like, ‘Oh my God, like, I’m going to have so many debts.’ Like, ‘I think I should do anesthesiology.’“ Henry, also in his third year, told us, “With the rise in student debt that everyone has,… it’s very hard to stick with those values that brought you into medicine in the first place. ‘I need to pay off my debt. How am I going to do that?’ Make more money. ‘What specialties make more money?’ And I feel like, over time, money has become more of an issue for students. And some students might not go into the specialty they like the most or they feel like they belong to, but they go into something else because the compensation is better. ... I think that leads to some unhappy doctors.”
Far from the only factor affecting shortages in primary care and pediatrics, debt nonetheless seems to disincentivize students’ pursuit of both specialties.
iStockPhoto // PeopleImages
Henry’s prediction that selecting a specialty “because the compensation is better... leads to some unhappy doctors” appears to be borne out in the existing research literature. For instance, a 2011 article published in the Journal of the American Medical Association concluded, “Higher levels of educational debt were associated with lower QOL [quality of life] and higher rates of burnout.”
Our research suggests that debt interferes with the pursuit of passion for many medical students.
Similarly, another student noted, “People are coming out of school with hundreds of thousands of dollars in debt and, um, they’re worried about that debt, you know. So, I think that money comes up in conversation but usually only with like good friends or people that you trust.” He explains how the subject of money and debt is typically reserved for close friends and trusted peers. As Bianca, the debt-free student mentioned above, observed, those without medical school debt may feel uncomfortable about their relatively privileged status as debt becomes increasingly normalized.
Perhaps counterintuitively, given the documented shortage of primary physicians discussed above, research shows that physicians working in primary care and pediatrics are often happy with their careers. Although they don’t make as much money as, say, surgeons, they still earn six figures per year. Moreover, most medical students insist they did not choose their career path for the money in the first place, instead framing the choice as a pursuit of “passion” (a widespread goal among college-educated professionals beyond the medical profession, according to sociologist Erin Cech).
But our research suggests that debt interferes with the pursuit of passion for many medical students. Those who are debt-free have more freedom to pursue the fields they feel passionately about, unencumbered by the fear of repaying debt. (It may even be the case that many physicians in primary care and pediatrics who report high levels of satisfaction belong to this privileged group). Other graduates opt for more lucrative specialties—not because they are greedy, but because they are concerned about paying off their loans. In making such a choice, they may be pursuing fields that do not represent their primary intellectual interests, and as Henry hypothesized above, that can make for “some unhappy doctors.” But it takes a combination of factors to interact to produce “happy doctors,” according to the students we spoke with. For instance, to thrive in pediatrics or primary care, one must first have a passion for their chosen specialty—which is not a given.
Solutions for the combination of high medical school debt burdens and looming primary care shortages are elusive. As a policy idea, debt relief has received limited public support. Some medical schools have moved to free tuition, such as John Hopkins University and New York University, though even these bold reforms do not entirely eliminate costs for medical students, nor are they likely to impact the broader medical labor market so long as the majority of schools continue to charge high tuition. The good news is that people who enter primary care and pediatrics often enjoy rewarding careers. However, debt may deter aspiring physicians from pursuing these specialties in the first place, and those who enter despite carrying debt may experience debt-related stress down the road.
Although physicians occupy a privileged position in society, there is substantial inequality within the profession. For instance, sociologist Tania Jenkins shows how status hierarchies emerge informally among physicians in ways that reflect doctors’ training backgrounds: Jenkins finds that U.S.-trained MDs occupy a privileged position relative to international medical graduates and osteopathic doctors. All of our medical students were USMDs, the high-status subgroup of physicians, though our data reveal that differences in debt and familial wealth may be a source of inequality within this privileged group.
Additionally, while certainly not the only factor affecting shortages in primary care, debt appears to play a central role in disincentivizing the pursuit of this specialty. In fact, the previously cited bimodal distribution of debt burden among early/ mid-career pediatricians, for example, provides some evidence for both of these contributing factors (i.e., familial wealth and debt burden). While many new pediatricians had to borrow to finance their entire higher education (i.e., undergrad and medical school), just as many enter pediatrics with no debt at all.
As has been established by other scholars, access to familial wealth can create and maintain status hierarchies among physicians. Our study suggests an additional benefit to such familial wealth: to some extent, it allows medical students to more freely choose their passion for their specialty. The same data indicate, for instance, that those who had to borrow to cover the cost of their education began to feel enormous pressure to start paying off their debt as the end of medical school approached. For some, this pressure manifested as reluctance (or outright refusal) to select a specialty with extended residency training or a required post-residency fellowship, both of which come with comparatively poor compensation. For others, the pressure constituted an injunction to pursue a high-paying specialty that would enable them to pay off their debt quickly. Policymakers, accrediting bodies, medical professional associations, and administration in higher education institutions would be well served to seek novel ways of reducing cumulative debt for students in the medical field should they aim to adequately stock the future pipeline with primary and pediatric care doctors.
recommended resources
Aaron E. Carroll. 2024. “Why Doctors Aren’t Going into Pediatrics,” The New York Times, July 1. An op-ed written by a doctor and public health expert, this piece discusses the challenge of primary care shortages, especially in pediatrics.
William L. Cull et al. 2017. “A Study of Pediatricians’ Debt Repayment a Decade after Completing Residency,” Academic Medicine 92. Published in one of the premier journals on medical education, this article documents some of the impact of debt for physicians.
Mary B. Dunn and Candace Jones. 2010. “Institutional Logics and Institutional Pluralism: The Contestation of Care and Science Logics in Medical Education, 1967-2005,” Administrative Science Quarterly 55. The authors explain that, despite facing multiple institutional pressures, physicians still cite care for patients and the science of medicine as their professional motivating forces.
Tania M. Jenkins. 2020. Doctors’ Orders: The Making of Status Hierarchies in an Elite Profession. Columbia University Press. In her groundbreaking book, Jenkins explores how the informal dynamics of status hierarchies among physicians play out in residency training.
Colin P. West, Tait D. Shanafelt, and Joseph C. Kolars. 2011. “Quality of Life, Burnout, Educational Debt, and Medical Knowledge among Internal Medical Residents,” Journal of the American Medical Association 306(9). An insightful piece for those interested in the complex relationships between incoming physicians’ debt and their quality of life.