
Abstract
How HIV treatment, fertility fears, and western values have confounded traditional beauty ideals in Botswana.
THOR, Flickr CC
“If you say someone is fat, it should be a compliment.” Gorata, a 22-year-old university student in Gaborone, Botswana tells me. She went on to describe how, when she was younger, if somebody was called fat, it meant that they were fit, they looked like they would have healthy children. She continues, “you always knew that a fat cow meant a healthy calf, but today things are different…. you want to be modern, you want to wear stylish clothing, be thin and beautiful, and you worry less about the cows.”
Like many young urban, educated women, Gorata is negotiating what it means to be healthy and attractive in contemporary Botswana where HIV has long been a part of everyday life and anti-retroviral therapies (ARVs) have transformed what it means to have a healthy body. She describes how even as a child she would watch the “Miss Tourism,” “Miss University,” “Face of Africa,” and the “Queen Esther International” pageants on television. Back then, she says sadly, the contestants were role models, but “as you get older, you are faced with the problems, the paradox…. If you have HIV, you cannot be beautiful, women with HIV or AIDS are not beautiful, so even if you are thin, people will suspect you, and if you get too fat, they will also know you have HIV.”
Today, Gorata and others like her are forming conceptions of health and beauty against a backdrop of a three-decades-old HIV/AIDS epidemic and a constant influx of intervention programs. I first met Gorata at the 2010 “Miss HIV Stigma-Free” beauty pageant. She was hopeful that she might be “discovered” as a potential model. I attended as a guest of the event organizers and interviewed Gorata and ten of her friends as part of a larger ethnographic study on perceptions of public health strategies in Botswana. After the pageant, I spent two months with these young women who agreed to talk to me about growing up in an “ARV era” and an “AIDS culture” in which HIV has always been part of their lives and an HIV-free generation is now possible. Organizations such as PSI (Population Services International) and the U.S. Centers for Disease Control were the first to introduce beauty pageants equating a positive HIV status with contemporary global concepts of attractiveness and wealth, but it’s increasingly common for domestic and foreign HIV/AIDS prevention organizations to sponsor events for Tswana youth that combine a focus on healthy, safe sex with Western ideals of beauty and modernization.
The Context of HIV/AIDS in Botswana
Botswana is a prime example of how an effective and committed government can lead a country out of an enormous health crisis. In the past two decades, the country’s overall rate of HIV infection has declined from over 40% to approximately 18%, and the rate of transmission from mothers to infants is now practically zero. ARVs are available for free to any citizen who tests HIV positive, and there are young people who have been HIV positive since birth and lead relatively normal adult lives with the help of the medicines. Still, infection rates have plateaued, remaining especially high among those living in urban and more developed areas of the country and those with the greatest access to health care resources, higher standards of living, and more economic resources in general. The latest data show that HIV prevalence rates for both sexes were highest among the 40-44 age group at 40.6%. Statistics indicate that women, in general, have a higher HIV prevalence rate (the exception is among those aged 50-64, where women’s HIV positive rate is slightly lower than their male counterparts, 22.9 and 21.7%). But education and information abound and, in the past decade, from billboards to t-shirts, messages about knowing one’s status and striving for a stigma-free society are ubiquitous.
Modern Tswana women are caught between western discourses of fatness and obesity as “bad” markers of ill-health and the more traditional and powerful cultural beliefs that fatness and obesity are signs of health, wealth, prestige, and reproductive fitness.
Since 2002, Botswana’s government has implemented its extremely effective anti-retroviral policy that provides long-term medication to infected people. ARVs treat HIV and, while they do not kill or cure the virus, they can prevent the growth of the virus and improve longevity and quality of life. Many businesses support ARV treatment for employees and one dependent spouse, and, if HIV positive individuals are not employed, the government will subsidize their care. ARVs are so successful that they have mitigated the need to voluntarily disclose HIV status and even made a dent in the stigma of being HIV positive. Most strikingly, ARVs are seen as “restoring” health, increasing caloric intake and essentially bringing individuals back to a healthy weight (or higher). People on ARVs gain weight quickly and generally return to a physically “fitter” and “fatter” state.
One of the greatest impediments to successful HIV/AIDS prevention programs, is inattention to the gender complexities of Tswana culture. While a focus on male involvement in HIV/AIDS prevention has been gradually increased, for a variety of social and biological reasons, women remain at greater risk of infection. They have less access to resources and are situated at the crossroads between traditional and more modern gender roles and expectations. This is where beauty pageants and cultural norms have come into conflict. Modern Tswana women are caught between western discourses of fatness and obesity as “bad” markers of ill-health and the more traditional and powerful cultural beliefs that fatness and obesity are signs of health, wealth, prestige, and reproductive fitness.
Kopano Matlhape had three-month-old Tyrone circumcised as part of an HIV prevention campaign in Botswana.
CDC Global, Flickr CC

Complicating the scene is the fact that, in a country plagued by HIV/AIDS, looking “too thin” may mean being seen as having the “slimming” disease (a euphemism for AIDS) and looking “too heavy” could make others think you’re trying to hide your HIV status by taking ARVs. While awareness of HIV/AIDS and prevention programs is high in Botswana, two factors in particular complicate the adoption of such programs among Tswana: the importance of fertility and the role of food.
Anti-retroviral therapies and their attendant weight gain are being blamed for allowing individuals to “pass” undetected in broader society as potential carriers of HIV, as ideal sexual and reproductive partners.
Food and the Idea of Fat
In the past, fatness and wealth went hand-in-hand. They were key factors in signalling socio-economic position, wealth and prestige. Lebogang, Gorata’s university friend, tells me, “today there is too much pressure to be thin, beautiful. The problem nowadays is not to be too thin.” In addition to possibly making others think you’re HIV positive, thinness, for Tswana, indicates a state of dryness. That is, in a desert, to be desicated is to be unhealthy, undesirable, and infertile, so “dryness” is a dangerous state. As Lebogang understands: “For women, it’s a struggle—you want to be traditional for your family, but if you want to attract a man or be successful, you want to be thin and wear nice clothes. If you are too fat, too thin, people will say you are witched, or sick. They will think you are sick either way.”
Stuck in the middle, Tswana women want to be both thin and “thick,” fashionable but also fecund. Because of ARVs, people with HIV who were once observably “sickly” are now almost indistinguishable from the greater community. One university student insists, “You can see real slimming disease, you can tell, you can point them out on campus, walking around, you can almost see right through them.” But ARVs cause individuals to gain weight and regain a healthier and heavier body, ironically stigmatizing them again as HIV positive and even potentially contrary to Western ideals of thinness.
According to recent World Health Organization statistics, the prevalence of obesity among women and men aged 30 years and above in 2005 in both rural and urban areas of Botswana was estimated at 7.7% and 19.5%, in 2010 at 9.7% and 23.2%, and in 2015 at 12.1% and 27.2%, respectively. As global trade and economic development increase (Botswana boasts an international export trade in diamonds and cattle), food insecurity is becoming less prevalent. Yet, in 2009, approximately 500,000 people in Botswana had inadequate access to food. Thus, while obesity rates are skyrocketing as symbols of a “modern lifestyle” and wealthy status, only those who can achieve and aspire to a particular middle-class lifestyle have the means to consume imported, often high fat and refined foods and to lead more sedentary lives. Coupled with other forms of stigma, such as the fear that fatness indicates less about socio-economic prestige and more about one’s HIV status (since ARVs “make you fat”), Tswana navigate a tricky terrain of health and beauty concerns. In an attempt to allay medical and media concern around ties between ARVs and weight gain, an assistant Minister of Health, stated in 2010 that ARVs do not cause obesity; rather, it is the return of appetite, good health, and potentially poor dietary choices that make people gain weight.
Unsurprisingly, the ability to bear children, to “fatten” up and show that your “fat eggs” can combat “weak worms” (bad male sperm as a result of the high STD and HIV rates) is also important among “modern” Tswana women. Given the context of HIV/AIDS and the advent of both ARVs and the growing national concern over obesity and obesity-related diseases such as diabetes and hypertension, fertility fears lie at the nexus of cultural beliefs about the necessity of childbearing and contemporary concerns over other visible markers of “health.”
The Stigma of Infertility
The stigma of infertility is central to Tswana ideas of “health” and maturity. To be a real adult—a successful and (re)productive person—one must bear children. Both men and women experience this cultural pressure, although ultimately women bear the greatest burden. Barren or infertile persons are often described as moopa, unable to provide fruit or sustain life. A moopa woman’s eggs are not considered to be “fat” enough. For both men and women, the need to “prove” one’s fertile status remains an important cultural norm and is sought throughout the life course. Deborah, a mother of three girls, says, “no matter if you are a big person [wealthy, with high socio-economic status] or small, it is important to have children. You don’t want to marry someone if they cannot have a child. People will say you are crazy.” Traditionally, Tswana women are taught that childbearing itself confers health: it cleanses the blood, it makes you stronger, fatter, and more fit. Today the messages communicated by a fat or a thin body are ever more complex.
Understandably, any messages that promote the limitation of fertility as well as those that promote the limitation of fat, fit, fertile selves are met with resistance in this context. Abstinence and the use of condoms, which inhibit fertility, are understood among many Tswana as causing infertility and sickness. The idea for many middle-class, successful women that they would need to limit their caloric, sugar, or fat intake and ascribe to a different model and vision of “health” conflicts with traditional cultural values that remain important, despite development and modernization. This vision challenges the latent yet argually still omnipresent fears over stigma related to HIV status and the role of ARVs in everyday life.
A leaflet about the 2011 “Miss HIV Stigma Free Pageant.”
CEYGHO
The 2008 “Miss HIV Stigma Free” pageant contestants.
CEYGHO, Facebook

Tshebestso Thobolo, “Miss HIV Stigma Free Queen” 2008.
CEYGHO, Facebook
Even as the ties between fat eggs and fertility remain salient, Botswana is seeing a new emphasis on the dangers of “diseases of development” such as obesity and diabetes. A 28-year-old woman explains, “Traditionally, you want people to know that you have fat eggs, that you are able to conceive a child, that your womb is not slippery, the eggs are not dry, that you will have no problem keeping a child and you will receive the male’s blood [sperm].” But she continues, outlining the paradox: “Today, most people still think that, and they like women who look fit—not too fat, but not too skinny. But there are also problems if you are too fat—health problems like with sugar in the blood or you are on pills for HIV. Either way, people will talk.”
In both rural and urban settings, Tswana women worry that without “fat eggs” they will be unable to conceive, and so they reject the Ministry of Health’s warnings about obesity.
Public health personnel increasingly warn that Tswana are at risk for diabetes, heart attacks, and high blood pressure, all associated with greater body mass indices. Tswana people are aware of these diseases of development and even that obesity can be linked to infertility and miscarriage. The intersections of medical knowledge and cultural norms seem to bind many. One young woman at the pageant makes it clear that not only do food and fertility motivate particular behaviors, the can also affect the efficacy of ARV programs and HIV/AIDS prevention: “The problem with ARVs… they make those people get fat, so you are attracted to them. They look healthy, and, if you did not know them before, you would think they were fine. But those people, they go on ARVs and then they trick you. They say they are fine and you get bitten [infected with HIV], your blood gets weak and they get fatter. Before you worried that, if you were slim, they would think you had the disease. Now you have to be careful that you are not too fat because they will avoid you, but for the same reasons. It is not just about beauty.”
Mixed Messages and the Fat Trap
Being “traditionally built” and able to consume fattening foods remains important for modern Tswana even as obesity fears (particularly those around reduced fertility) begin to permeate local discourse. Neo, a 25-year-old mother of two, tells me, “If you are not taking your pills [ARVs], then you will get slimmer, but you will be sick. …[I]f you do take the pills, then you will be healthy, but you will get too fat. …[T]he doctors told me that, either way, I cannot fall pregnant.” It’s a no-win situation, a double-bind for women who know that if they become too thin, they will be seen as sick, infertile, and of lower socio-economic status, but if they are too fat, they may be seen as being on ARVs, admonished that obesity is a health and fertility risk, and, ironically, again taken to be of lower socio-economic status. Neo laments, “It is like being in a trap. You cannot turn around, because any choice you make will hurt you. The doctors will tell you now that you should not have too much fat, it is bad for your heart, and if you are trying to have a child, the fat will block the sperms, it will make the blood too thick, too slippery. But when we were young, we heard about people who were too thin, those were witches and you had to be careful. They were wasted and too small, their bodies could not hold a child or carry it.”
A physician in a rural village tells me that this push and pull between traditional norms and contemporary, more Western, urbanized norms is overwhelming: “I see women here in the villages who are trying to stay fat, who are happy to have ARVs because they gain weight again and they look healthy. But then they hear these messages, from family or friends, those in the cities who say that being too fat now is the latest problem, what are they supposed to do?” For many women, the central tension between these two messages is not beauty, but fertility. In both rural and urban settings, they worry that without “fat eggs” they will be unable to conceive, and so they reject the Ministry of Health’s warnings about obesity. Women in both settings emphasize too the fears that ARVs will ironically make them “look fatter” than they intended and will give away HIV status, making them less desirable sexual and reproductive partners.
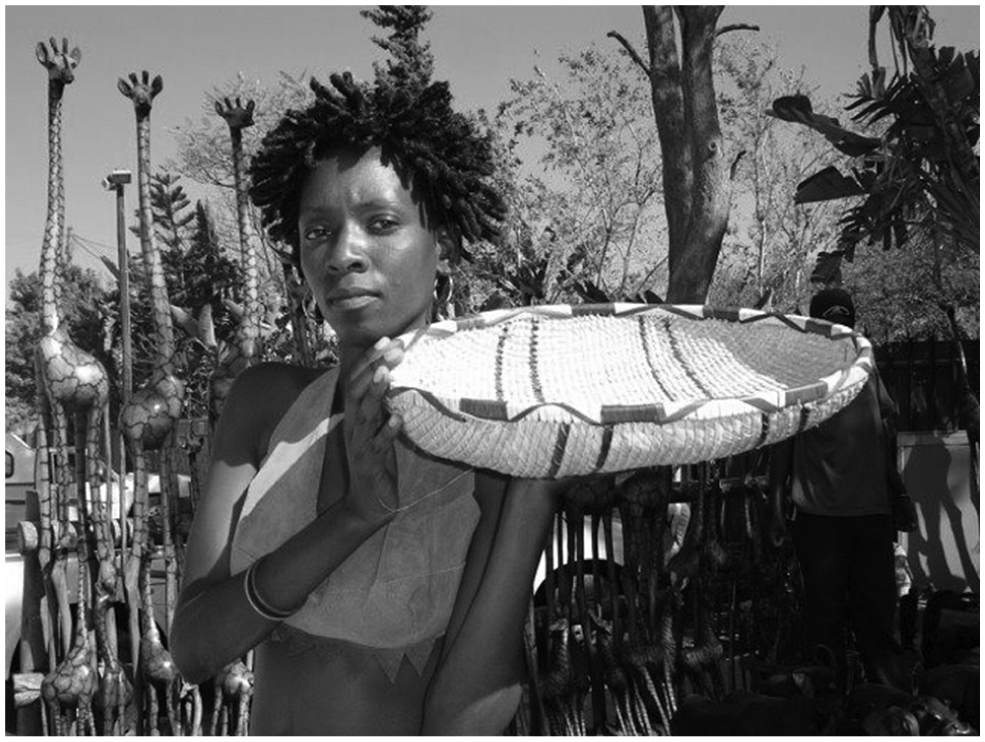
Western beauty ideals and “diseases of development” that have arrived with globalization further complicate how Tswana women’s bodies are perceived to reflect health, fertility, and beauty.
Pete Dominguez, Flickr CC

Unfortunately, HIV prevention programs (and, now, projects geared toward curbing obesity) in Botswana have rarely focused on cultural factors such as the meaning of fertility and embedded gender roles as they relate to health and well-being. Health is often understood as having access to medical care, food, and a modern lifestyle. Yet obesity rates are rising and posing challenges to efficacious HIV/AIDS prevention programs that would be better served by a focus on gender and fertility and how the two are inextricably intertwined with ideas of body, food, health and wealth in cultural context.
There are many lessons here for policy-makers. Among them is the fact that ARVs and their attendant weight gain are being blamed for allowing individuals to “pass” undetected in broader society as potential carriers of HIV. Since “fatness” remains an important cultural signifier of fertility, this means that HIV-positive people are also suspected of “passing” as potential and ideal reproductive partners. Simultaneously, ARVs and the HIV/AIDS epidemic complicate how health and fatness are understood, as Tswana increasingly experience diseases of development such as obesity. Socio-cultural conflations between being “fat” and wealthy and having “fat eggs” and being fertile are confounded by a growing belief that too much “fat” can signal poor health, even HIV positive status. Women like Gorata, Lebogang, and Deborah and her daughters are left navigating a space that is at once too thick and too thin.