
Abstract
How can we explain the exponential increase of the cesarean section in the U.S. in recent decades? Drawing from 130 in-depth interviews with women, obstetricians, midwives, and labor and delivery nurses, sociologist Theresa Morris explains the epidemic that affects the lives, health, and families of every woman in America.
The performance of cesarean section births has reached an epidemic level in the United States. In 2012, 32.8 percent of women who gave birth in the United States had c-sections. The World Health Organization warns that countries with a c-section rate over 15 percent put women’s lives at risk, and a recent study finds that annual U.S. healthcare costs could be reduced by more than $5 billion if the C-section rate were reduced to 15 percent. In an attempt to understand the C-section trend, I interviewed 50 maternity clinicians—obstetricians, family physicians, certified nurse-midwives, and labor and delivery nurses—and 83 women who had given birth the day before. These sociological data illustrate the context of medical routines and practices that shape the decisions of pregnant women and their physicians and lead to a high rate of C-sections.
Economic pressures on hospitals and fear of lawsuits are the main drivers of an epidemic C-section rate.
My research demonstrates that increased economic pressures on hospitals, as well as hospital administrators’ and maternity clinicians’ fear of lawsuits, are the main drivers of the C-section rate. Malpractice insurance cycles are a known phenomenon, and clinicians define malpractice crises in hard cycles, which are characterized by a shortage of malpractice insurance policies and high malpractice insurance premiums. Hard cycles have occurred in the American malpractice industry in 1975-1978, 1984-1987, and 2001-2004. Each of these periods coincides with a precipitous increase in the C-section rate, and the rate becomes institutionalized, continuing after the crisis subsides (see chart on p. 71). The C-section rate has increased by 34 percent since 2001, the beginning of the last defined crisis. Additionally, changes in Medicaid compensation mandated by Congress in 1982 spurred corporatization of hospitals and medical practices. As a result, physician autonomy has steadily declined, and hospitals face increased economic pressures. These structural changes, along with more intense attention to the economic threat of malpractice lawsuits, have led hospital administrators and maternity clinicians to search for an expedient mode of birth that will also protect them from lawsuits. The answer: C-sections.
The Specter of Malpractice Suits
Many negative birth outcomes, like cerebral palsy, are unpredictable and, for the most part, unpreventable. Nevertheless, maternity clinicians are often held accountable, regardless of whether the care they provided caused the outcome. Obstetrics is a high-risk specialty in terms of malpractice allegations. Obstetricians have the third-highest lawsuit rate among physician specialties, third only to neurologists and neurosurgeons, and almost every obstetrician will be sued before age 65. Moreover, malpractice insurance premiums and average malpractice awards have been increasing. All of this heightens attention to liability in the obstetrics field; a concern that was prevalent among the maternity clinicians I interviewed.
Harris & Ewing Collection, Library of Congress

Two types of C-sections are reflected in the epidemic rate—the increase in primary or first C-sections and the increase in repeat C-sections. In terms of primary C-sections, physicians are often intolerant of irregularities in fetal heart beat measurements and perform C-sections during the course of labor as a result. Yet, as a good example of Peter Berger’s sociological insight that things are not always what they seem, there is no evidence that the increase in C-sections is due to better identification of problems with the baby during labor or that there has been any resultant improvement in outcomes.
Almost all hospital births in the United States include continuous monitoring of the fetal heartbeat. This is an increase from 44.6 percent in 1980. One might be surprised, then, to learn that these monitors incorrectly identify fetal distress 99.8 percent of the time, which means that 99.8 percent of babies identified to have “non-reassuring” heart rate patterns by continuous electronic monitoring will not be compromised at birth. Despite this lack of predictability, electronic fetal monitors are widely used continuously, and maternity clinicians intervene quickly when babies have “non-reassuring” fetal heart rate patterns, even though almost always the fetus is not compromised. Studies show that intermittently monitoring the fetal heart rate produces outcomes that are just as good as continuous monitoring, but with a much lower c-section rate (see Alfirevic, Devane, and Gyte’s 2013 review “Continuous cardiotocography (CTG) as a form of electronic fetal monitoring (EFM) for fetal assessment during labour” in the Cochrane Database of Systematic Reviews). Women’s labors are monitored continuously not because fetal outcomes are improved, but because the strip of paper (or electronic record) produced from the monitor documents the fetal heart rate throughout the labor and can be used as evidence in court cases if there is a negative outcome.
Other practices, such as inducing women rather than allowing them to go into labor naturally, contribute to more C-sections, especially among first time mothers. Women whose labors are induced are twice as likely to have a C-section as women who go into labor spontaneously. Women are sometimes induced so that clinicians can avoid being sued if a bad outcome occurs in women who deliver past their due dates. Physicians also often induce or schedule C-sections for suspected “big” babies (defined as an estimated weight over 9 pounds 15 ounces), even though there is no scientific evidence of improved outcome over a vaginal delivery and professional guidelines discourage this practice. Further, women with twin pregnancies and women with babies in a breech position (bottom down) are routinely scheduled for C-sections. Maternity clinicians I interviewed reported that these C-sections are done to prevent blame for bad outcomes in vaginal deliveries, even though evidence suggests that vaginal birth leads to equally good outcomes as C-section in these situations.
The increase in repeat C-sections also contributes to the epidemic rates. For women who have had a C-section and become pregnant again, VBAC (vaginal birth after cesarean section) is an option in theory, if not always available in practice. Presently, 91 percent of women who give birth following a C-section have a repeat C-section, even though survey evidence suggests that nearly half would like to attempt a VBAC. VBACs are just as safe as first vaginal births and catastrophic outcomes are exceedingly rare, but because of the small risk of the uterine scar rupturing during labor, many hospitals and physicians do not offer this option. Physicians know the risk of a catastrophic uterine rupture is slight, but fear they will be successfully sued if a uterine rupture occurs and the baby is injured or dies.
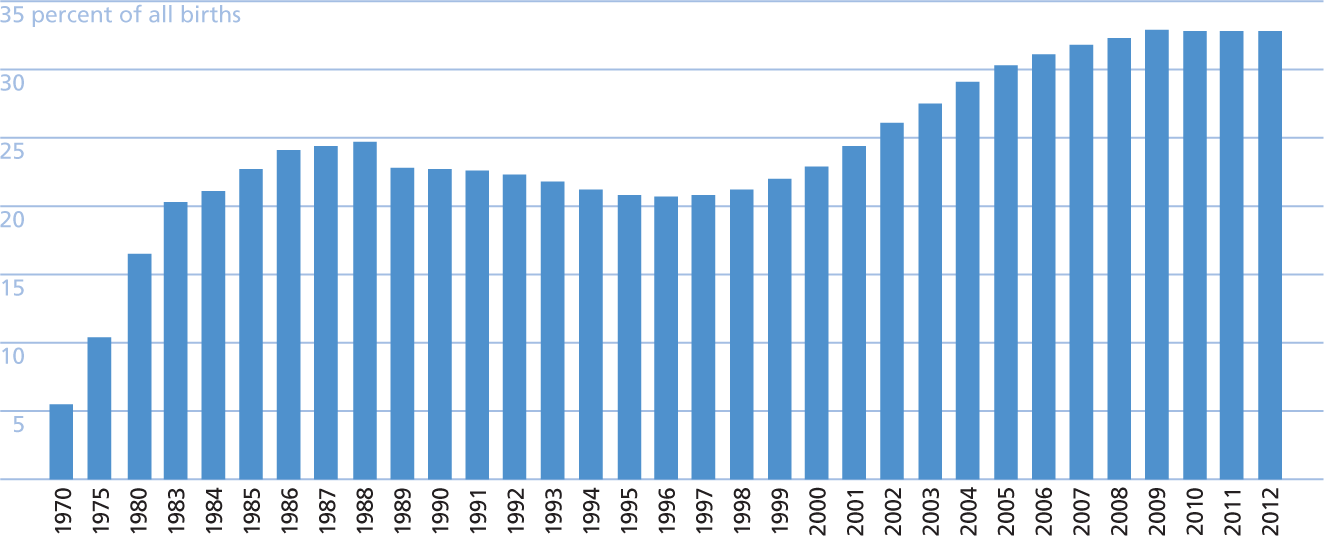
U.S. Cesarean Section Rates 1970-2012
Source: Compiled from CDC; Taffel, Placek, & Liss (1987).
(MIS)Leading Organizational Influence
Organizational influence over individual decisions is particularly evident in the hesitation of physicians around VBACs. The professional organization of obstetricians in the United States, the American College of Obstetricians and Gynecologists (ACOG), officially recommends that obstetricians, anesthesiology staff, and operating rooms be immediately available in hospitals that offer women VBAC opportunities, even though there is no empirical evidence that such requirements improve outcomes and there are no similar recommendations that apply to other, more common, obstetric emergencies, such as hemorrhage.
Many hospitals face challenges in meeting these recommendations due to limited facilities and/or staff. The only significant decrease in the past forty years in the c-section rate was between 1988 and 1998, when ACOG issued practice guidelines that encouraged VBACs and changed the language from its first VBAC practice guideline (issued in 1982) suggesting staff and resources be “immediately available” to a more flexible “readily available” requirement. The VBAC rate reached an all time high of 28.3 percent in 1996, and the C-section rate dropped to 20.7 percent. However, this ended in 1999 when ACOG issued a new VBAC practice guideline reverting back to the “immediately available” staff and resources guideline, which was reaffirmed in the most recent practice guideline issued in 2010. This ACOG stance stands out as one of its guidelines least tied to empirical evidence.
ACOG is not the only organization to bear responsibility for the low VBAC rate. Malpractice insurers may define VBACs as non-covered events, meaning that if an obstetrician oversees a VBAC attempt, the malpractice insurance company will not cover a malpractice suit resulting from that birth. In addition, reinsurance companies, which insure malpractice insurance companies against large claims, also may deny coverage for VBACs. In both cases medical care (including surgery) is not linked to medical science but, instead, is influenced by organizational recommendations or requirements outside the control of physicians and hospital administrators.
Solutions to the C-Section Epidemic
Because maternity clinicians’ fear of liability underlies much of the C-section epidemic, any effective solution must address this problem directly. For example, currently in most states, malpractice must be alleged for a family to seek compensation for an injured baby. The federal government should change the system of addressing malpractice to a no-fault system. In such a system, families of babies born with injuries would be compensated regardless of whether the injury was caused by medical negligence. Further, federal policy should prohibit malpractice and reinsurance companies from excluding established medical procedures, such as VBACs and vaginal twin and breech deliveries, from their range of coverage, and hospitals and obstetrical guidelines should refrain from banning these deliveries. In addition, the indiscriminate use of continuous electronic fetal monitoring on low-risk women should be abandoned. Finally, we all need to learn more about how economic and organizational pressures and guidelines may shape labor and birth practices in ways that contribute to patterns such as epidemic C-section rates.