
Abstract
In an age of ongoing military conflict, more and more veterans survive battle wounds only to find they return home to face psychological wounds. Why aren’t they seeking the mental health services offered by the Veterans’ Association and other groups?
Keywords
A marine waits with a pile of bloodwork. The test he is getting may one day predict the risk of PTSD.
The Associated Press/Jae C. Hong

The U.S. Military offers veterans and active personnel a variety of mental health support services. Yet many of those who would most benefit from help choose to suffer in silence.
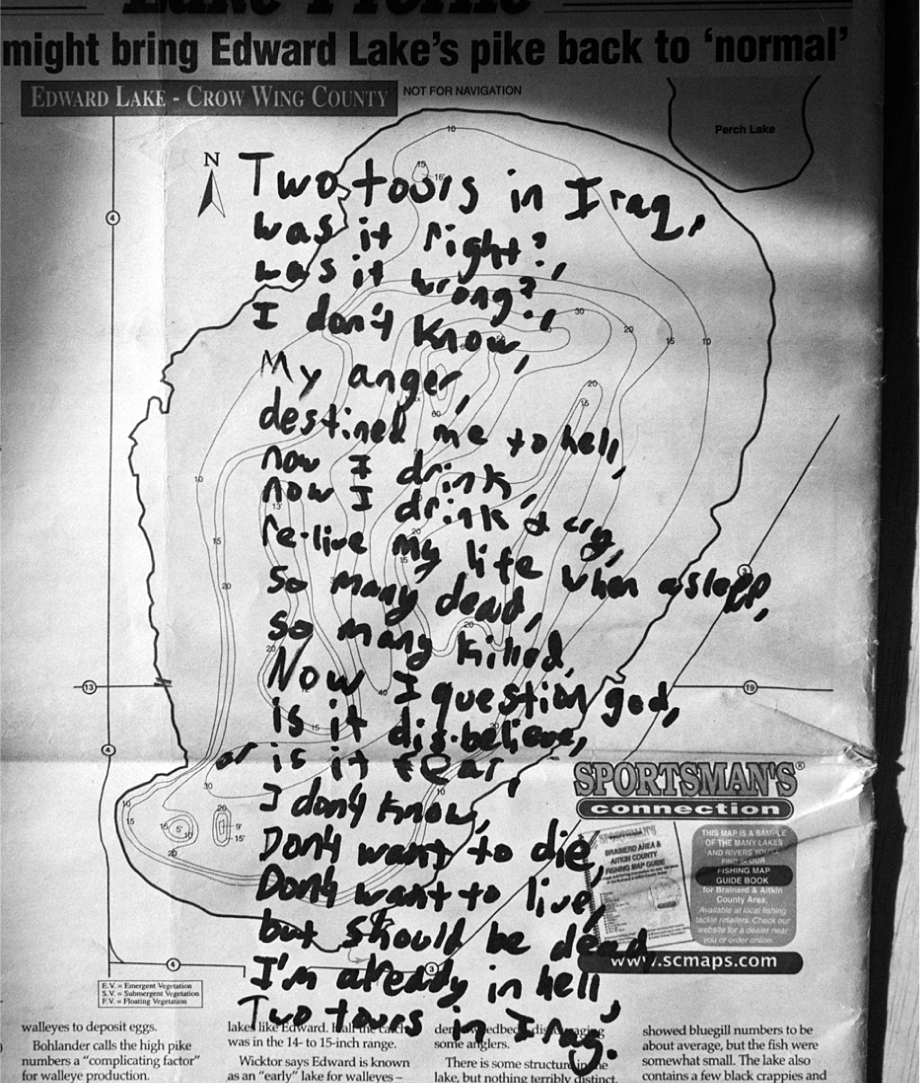
This poem, titled “Two Tours in Iraq,” was written shortly before a soldier with severe PTSD killed himself.
Ashley Gilbertson/VII/Corbis
Andre and Kenny hit it off the night they met. They swapped stories for hours, shared dinner together, and even learned they had attended neighboring high schools. Andre wasn’t on the patrol the next day when Kenny was killed—but he watched as Kenny’s tank was towed back to base with the tarp-covered body inside.
He recalled: “The tank completely blew to pieces. When it hit the landmine… all of the ammunition stuff started going off inside, and a couple of the guys got caught inside the tank… the seat had embedded into [the driver’s] spinal cord, and they tried to pull him out. He was screaming; they couldn’t pull him out. He was… he burnt on fire.”
Today, Andre is haunted by the image of his friend’s burned corpse, which he glimpsed as the wind lifted the tarp. Before the war, he was jovial, known to clown around and deescalate neighborhood conflicts. But his wartime experiences transformed him. His ex-wife—they divorced after his deployment—noticed he’d changed too.
When he returned home, Andre attended a mental health-screening program designed to identify Post-Traumatic Stress Disorder (PTSD) among combat veterans. During the screening, he recalled, “the flood-gates just opened up. I didn’t know it was bothering me that much until, you know, they had me really talking about it. And I just started crying and I couldn’t stop.”
A new set of troubles began. Once diagnosed with PTSD, Andre was forced to leave the military. But his civilian job, working in aviation for the federal government, required him to be a standing member of the National Guard, so he lost the job.
In the aftermath of the Vietnam War, activist anti-war veterans and psychologists developed PTSD as a formal diagnosis, eventually forcing the military and the Veterans’ Administration (VA) to adopt policies to deal with psychological problems. Today, however, screening programs for the disorder can serve as a sorting mechanism, removing those deemed “damaged.”
Andre experienced traumas that most of us cannot fathom. His story and those of other veterans show that policies designed to ease reintegration often hurt. Popular, well-meaning programs, such as mental health screenings, mark soldiers as trouble-makers unfit for service in a process I call “punitive empathy.” While publicly, the military points to these programs as evidence that mental health issues are being taken seriously, service members who report problems have a different version of events.
Over the past year and a half, I interviewed 50 veterans about their wartime experiences and reintegration into post-military life. The ravages of combat are written on their bodies, in slumped shoulders, broken speech, and tears. In searching for meaning in their experiences, their anguish makes it clear why many veterans are reticent to talk. Some have learned that discussing war comes with a social price tag. Family and friends often don’t understand, and may condemn them. Punitive empathy in the military reinforces this culture of silence.
I had expected veterans to tell me about the mental health problems associated with their service. But I was surprised that many hid their issues from the military. If the military and the general public acknowledge that combat can have life-long psychological effects, though, why do some veterans avoid getting care?
In 2007, the Washington Post reported that Walter Reed, the nation’s premier Veterans Affairs hospital, was systematically failing. The articles chronicled a labyrinthine bureaucracy that failed to heal the physical and psychological scars of combat. Since then, a steady stream of stories has depicted a VA bogged down by the growing volume of mental health cases. Recently, the Department of Veterans Affairs’ Inspector General reported that the average wait for preliminary screenings is nearly three months—at a time when the number of suicides among veterans and active duty troops now exceeds combat deaths in Afghanistan.
Explanations that focus on the VA system’s inadequate facilities or capacities fail to tell the whole story. Nor can explanations that focus on the masculine culture of military and the tendency to shame those who seek out help. My interviews suggest that it’s the organizational culture of the military that systematically inhibits veterans from seeking out mental health treatment.
Force Readiness?
Throughout the 20th century, the military has been under pressure to provide therapeutic help for its members who suffer from mental health problems. But having deployable soldiers fit for combat regardless of trauma—“force readiness,” in military jargon—is a paramount internal goal.
Soldiers are marked as trouble-makers, unfit to serve if they seek out mental health services.
Historically, then, the United States military has veered between ensuring the internal goal of force readiness and helping its personnel navigate psychological trauma. According to sociologist Wilbur Scott, what was known as “shell shock” during WWI was thought to afflict only “weaklings.” So, when the U.S. military joined the war effort, psychiatrists were to ensure soldiers returned to combat as quickly as possible following trauma exposure. Short-term force readiness was a more immediate concern than soldiers’ long-term mental health, and those complaining of severe distress risked labels like coward or malingerer.
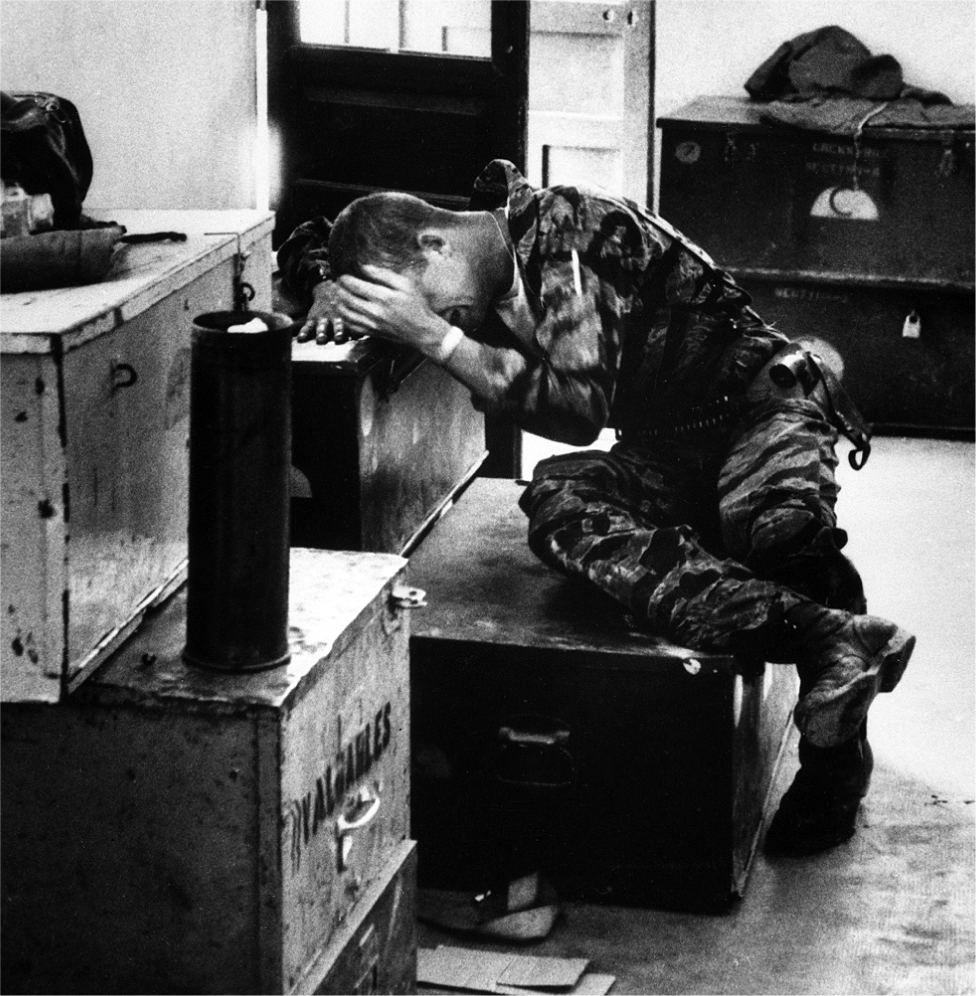
A young marine breaks down after a mission in Vietnam, 1965.
Getty
Institutions like the U.S. military derive their legitimacy, in part, from presenting “fronts” that conform to public expectations of care for their personnel. But while Department of Defense mental health programs demonstrate the military’s commitment to helping veterans, those who seek out help are often punished for doing so. Bosses, managers, or commanders frequently retaliate against those who come forward, strengthening the very institutional inequalities such programs were designed to alleviate.
Outside the media’s eye, in “back stage” interactions with commanders, fellow soldiers, and the military bureaucracy, service members are vulnerable to retribution, hazing, or worse. The military’s entrenched hierarchies mean that those with power have the discretion to apply policies that reinforce traditional hierarchies of race, gender, and mental health status.
So while mental health screening programs serve a public relations function, those who use the programs run the risk of stigma. Fearful of losing their jobs, veterans often hide their mental health problems or seek help outside the military. The conflict between force readiness and mental health needs is key to understanding the issues facing today’s veterans.
Men who experience combat are more likely to be unemployed and disabled for the rest of their lives. In 2010, sociologist Alair Maclean showed that Vietnam combat veterans were nearly twice as likely to be unemployed in 1999 as non-combat veterans and non-veterans. Yet we know little about the organizational mechanisms shaping post-service life and work for Iraq and Afghanistan veterans.
The 2.3 million veterans who were deployed to Iraq and Afghanistan experienced a historically unprecedented cycle of service. These wars’ long duration, coupled with military procedures called “stop-loss policies” that keep service members enlisted long beyond their contractual end-dates, have profoundly stressed veterans, their families, and the healthcare system. When they return, veterans must contend with limited job opportunities in a recessionary civilian labor market. Together, these factors create a situation where service members frequently return to war when they might otherwise have left the military.
Multiple deployments increase the risk of trauma exposure. Nearly 20 percent of returning vets have been diagnosed with PTSD, and rates of traumatic brain injury (TBI), depression, and military sexual trauma (MST)—harassment or assaults often perpetrated by fellow soldiers or superiors—are also high. Insurgents’ asymmetrical warfare has erased traditional notions of the “front lines,” as Improvised Explosive Devices (IEDs) indiscriminately strike both “support” and combat service members. And despite the formal ban on women in combat (lifted only very recently), women have been serving on the “front lines.” These female service members experience higher rates of PTSD and MST than their male counterparts.
Rather than seek out treatment within the military healthcare system, many veterans and active-duty service members suffer in silence. They live with the threat of repercussions in the form of sabotaged careers, hazing through extra duty—such as when commanders force enlisted soldiers to do menial, degrading, or dangerous work—or expulsion. Military estimates of mental health disorders are therefore undercounts of the true psychological costs of conflict. Qualitative evidence of the complications of homecoming is vitally important for sociologists and policymakers to fully understand and address how the vicissitudes of combat shape veterans’ lives.
The organizational culture of the military systematically inhibits veterans from seeking out treatment.
The military has multiple programs in place to help with mental health issues affecting soldiers, including mandatory post-deployment mental health screenings. Psych-techs are available in the field and on base, and soldiers are often encouraged to seek care. The “front stage” of these apparently empathetic programs recognizes service members’ potential problems and tries to offer solutions—bolstering the combat mission and reputation on the home front.
But the veterans I interviewed still feared retribution.
Whether we call it “soldier’s heart,” “shell shock,” “battle fatigue,” or PTSD, the experience of war changes combatants’ lives.
Aubrey / ob1left

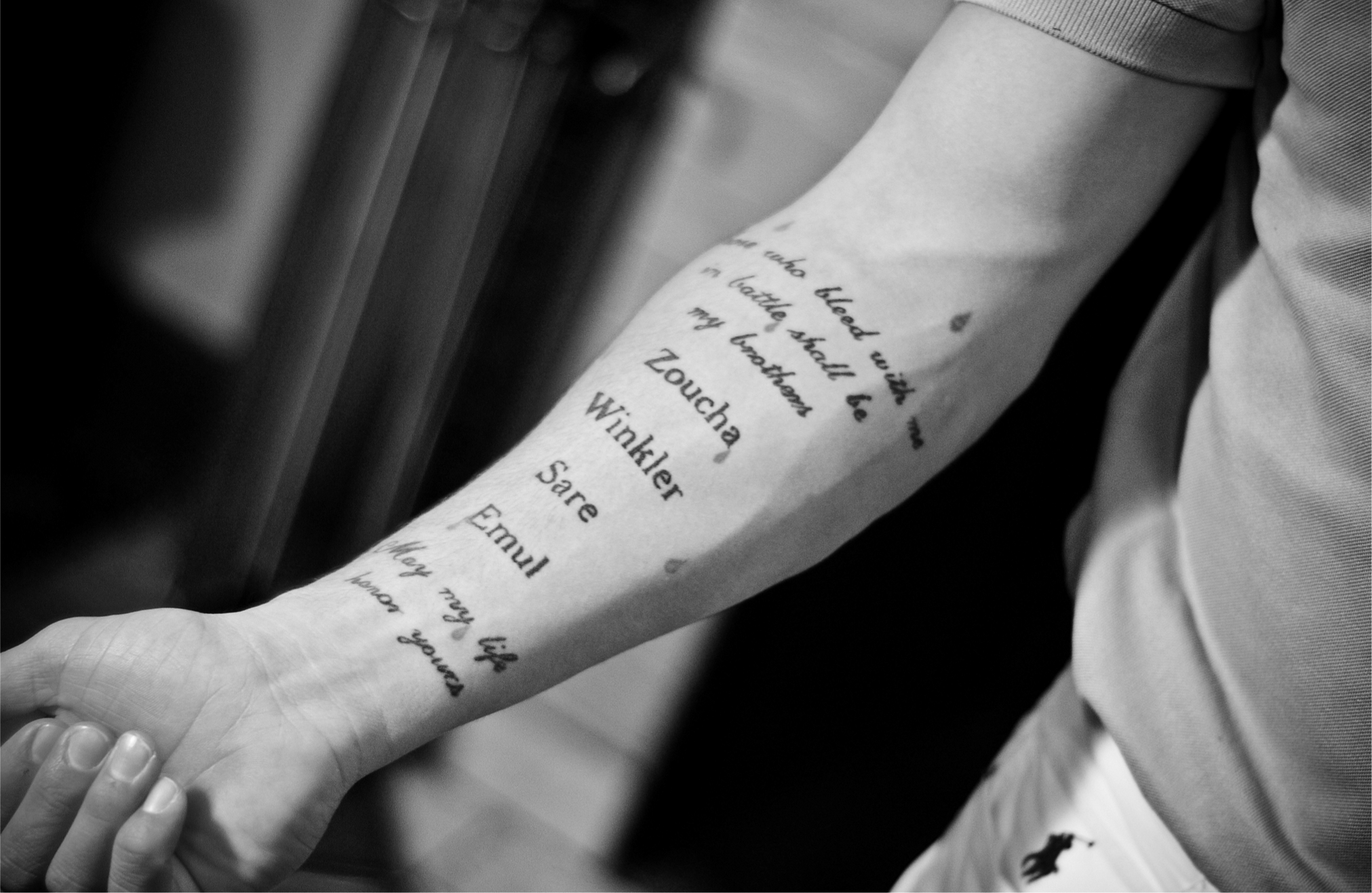
An Iraq veteran reveals his tattoo, which reads “All who bleed with me in battle shall be my brothers.”
KT King
“You’re Finished. You’re Done”
Like many soldiers, Joe joined the military for college tuition. A black single father of two in his mid-forties, he deployed to Afghanistan and experienced anxiety disorder and severe depression after combat. Joe was aware of the military’s media outreach encouraging soldiers to get mental healthcare, recalling, “they’ll come on TV and talk about, ‘Oh, generals go see the doctor and they talk, you know, they get help.’”
Joe’s voice was tinged with disgust as he implied that this outreach was disingenuous at best. “I don’t give a flying flip what they say… If that comes up in your file, you’re done. That next rank, you’re finished. You’re finished. You are done! If you are an enlisted guy… and it goes in your file that you went to the Gulf and you came back and you went to see somebody for major depressive disorder… You won’t reenlist. They won’t let you. You’re done.” Further, Joe had little faith that his relatively high-ranking status would help him. “If you’re an officer, you’re especially done,” he said. “I was a senior officer. So I knew that I had to protect myself.” Joe’s self-protection took the form of seeking care through an outside psychiatrist. For 18 months he received therapy twice a week, hiding his condition from the military to avoid repercussions.
Women were discharged after they reported sexual assaults.
Despite the military’s front stage proclamations of support, Joe simply feared getting mental health care through the military. He describes a back stage where acknowledging a psychological disorder would harm a soldier’s career. According to Joe, if commanders think a soldier’s mental illness would impede the military’s internal organizational goals, the mission comes first. Soldiers’ concerns about reporting mental health issues are pervasive: several of the lower-ranking soldiers I interviewed explained that they feared the consequences of telling the truth about their mental health needs.
Punitive empathy also influences veterans’ willingness to report sexual assault, which female service members experience at twice the rate of civilian women. Women who experience sexual assaults may avoid reporting attacks for many reasons, including worry about the military’s response. The veterans I interviewed know women who were discharged after they reported such attacks.
Cherrie, for example, joined the military to escape a rough childhood and a string of bad relationships. Cherrie had tremendous family responsibilities, including helping to care for her HIV-positive mother. Despite these barriers, Cherrie had a remarkable career, earning two masters’ degrees during her service. A calm and pensive Latina, she credited the military for offering her opportunities absent in civilian life. Cherrie was on leave when she went to a party at a lifelong friend’s house. While there, she was drugged and sexually assaulted.
A young soldier suffering from PTSD, along with physical injuries, holds his daughter.
Getty Images

“I wanted to go to the police but I was ready to deploy. And I thought, I am not going to go to the cops because if they open up a case, I’m not going to deploy,” she said. “Plus, it’s going to affect my career because they are going to ask what drugs, let’s do a drug test, and you can get discharged.” Although a civilian had committed the assault, Cherrie believed that dealing with the military was too risky; she thought she’d be doubly victimized, forced out of her job. So instead of reporting her assault, Cherrie decided, in her words, to “push this away, and go on deployment and do what I have to do and deal with it later.” This decision placed her at greater risk for mental health problems, as another deployment exposed her to further trauma: she experienced several mortar attacks while she was at work providing mental health services to active duty troops. Ironically, Cherrie is a psych-tech, screening returning vets for the very problems she is afraid to reveal to her commanders.
Since she returned from her second deployment, Cherie continues to seek mental healthcare outside the military. Among other difficulties, she blames her mental health issues for the loss of some of her G.I. Bill benefits after she withdrew from a prestigious advanced degree program.
The Military—and Beyond
The term “punitive empathy” explains the gap between word and deed in organizations, and it has broad implications for understanding the reproduction of institutional inequality. Organizations require conformity to operate, and those who don’t fit organizational molds—because of racial, gender, or other differences—may be targeted for harassment. However, organizations do not exist in a vacuum; social pressures compel them to conform to prevailing notions of equal opportunity and compassion. For instance, the civil and women’s rights movements forced organizations to adopt policies to alleviate endemic racial and gender discrimination. Despite these on-paper reforms, racial and gender inequalities persist.
As sociologist Vincent Roscigno has shown, women reporting workplace sexual harassment “are often exposed and punished” through the very anti-discrimination programs designed to remedy the harassment. Roscigno claims that, in many cases, “workplace responses to harassment are as much a part of the problem as the harassment itself,” compounding problems for women workers. And diversity programs can harm people of color, according to sociologist Adia Harvey Wingfield. The backstage implementation of programs, in other words, is often odds with the front stage goal of addressing inequality, reinforcing traditional workplace hierarchies.
In the coming years, the strain on the Veterans Affairs health care system will only grow. The number of those diagnosed with PTSD, depression, and anxiety will also increase. And, although the military has implemented hundreds of new programs designed to address these issues, a recent comprehensive report from the Institute of Medicine at the National Academy of Science acknowledges that the effectiveness of these programs is unknown.
As I write, we are approaching the thirteenth year of war in Afghanistan, and combat troops are scheduled to remain in that country until at least 2014. Troops have only recently returned home from Iraq to begin changed lives. Despite the military’s front stage endorsement of its mental health programs, veterans like Joe and Cherrie still fear reprisals for seeking mental health care, so they avoid the programs designed to help them.