
Abstract
Drug-induced liver injury remains a major concern in the pharmacological management of epilepsy. Antiseizure medication (ASM)-related liver injury has multiple phenotypes, and in the majority of cases it is “idiosyncratic,” involving hypersensitivity reactions. Awareness of drug- and patient-related risk factors can help direct treatment selection, monitoring, and ASM discontinuation, when necessary. This article examines the typical patterns of ASM-induced liver injury, from mild elevations of hepatic enzymes to life-threatening conditions. We also discuss risk factors, means for preventing liver injury in people with epilepsy treated with ASMs, and emerging biomarkers.
Keywords
Introduction
Drug-induced liver injury (DILI) is the harm that medications, including prescription, over-the-counter, and herbal/dietary supplements, can cause to the liver.1–3 DILI is rare, with an estimated annual incidence ranging from 2.4 to 13.9 per 100 000 inhabitants.1,3 The injury can mimic almost any type of liver disease and can vary from mild liver test abnormalities to fatal liver failure. 3 Serious liver injury is a major cause of drug attrition during clinical trials and during post-marketing surveillance, which has limited the use of promising therapies.4,5 For example, the antiseizure medication (ASM) candidate phethenylate (Thiantoin) was withdrawn from the market due to hepatic necrosis, 6 and felbamate use was restricted following cases of aplastic anemia and serious hepatotoxicity.7–9 Over the last 2 decades, the frequency of ASM-associated DILI10,11 and liver transplantation due to acute liver failure 12 in the United States decreased, as older-generation ASM use declined. 10 However, ASMs remain on the top-10 lists of implicated agents in Latin America 13 and in India. 14
Manifestations
Most cases of DILI are diagnosed 5 days to 6 months after starting a medication, 15 but longer latencies have been documented.10,16 Felbamate can cause severe hepatic dysfunction, often progressing to liver failure, within 3 weeks of treatment initiation, typically without prodromal symptoms. 17 Valproate-induced Reye-like syndrome usually develops within 30-90 days from treatment onset, but hyperammonemia and hepatocellular injury can manifest after more than 3 months.7,8,16,18 Most patients who develop phenytoin- or carbamazepine-hepatotoxicity do so during the first 6 months, 7 but severe injury has also been reported to occur after 12 months of carbamazepine therapy. 7 Hypersensitivity reactions usually occur during the first 3-6 months of treatment,19,20 but may develop within 24 to 72 h, especially upon repeated exposure to the drug.15,21
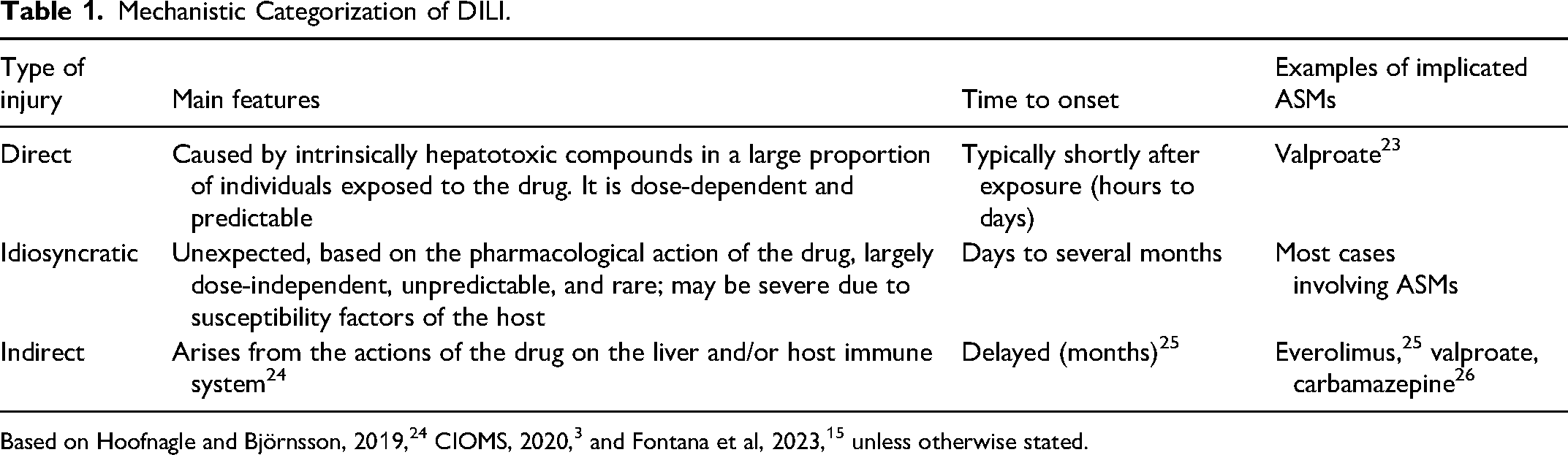
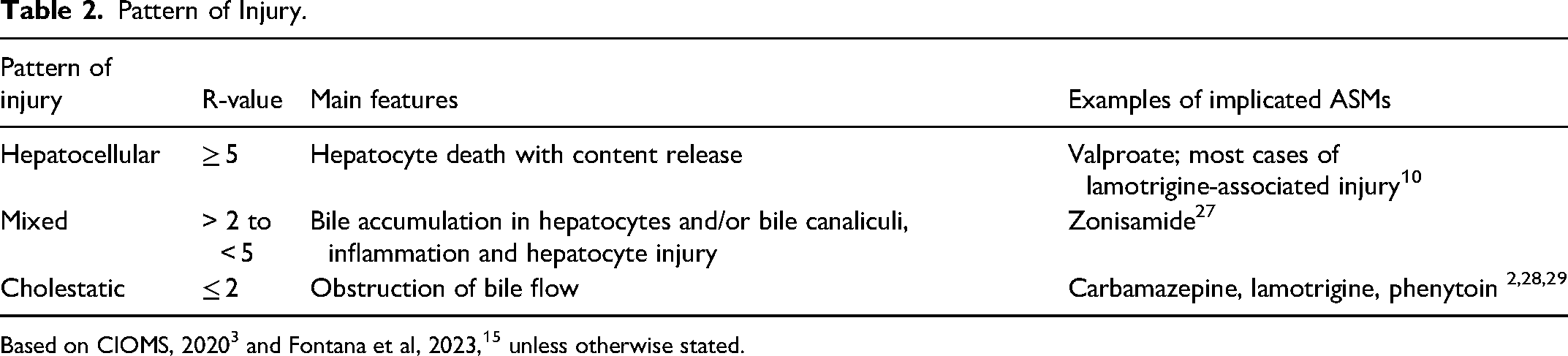
DILI is categorized into 3 classes: direct, indirect, and idiosyncratic (Table 1). Most cases of concern are idiosyncratic. The pattern of injury is generally classified based on the R-value, which is the ratio of serum alanine aminotransferase (ALT) to alkaline phosphatase (AP) (both expressed as multiples of the upper limit of the normal range, ULN; Table 2). 15 The R-value helps describe DILI as hepatocellular (R > 5), mixed (5 > R > 2) or cholestatic (R < 2). The R-value is most accurate for predicting severe liver injury when calculated upon recognition of DILI and these values may shift over time. 22
Mechanistic Categorization of DILI.
Pattern of Injury.
Mild Elevations of Hepatic Enzymes in Serum
ALT or AP elevations without jaundice (total bilirubin <2.5 mg/dL) 22 can be caused even by drugs that have a low potential for causing severe hepatotoxicity, 24 and have been documented with nearly all ASMs. Mild transaminase and gamma-glutamyl transferase (GGT) elevations caused by phenytoin, phenobarbital, and carbamazepine can be secondary to hepatic enzyme induction without hepatic pathology.3,18,30 AP is elevated in 30% to 40% of patients treated chronically with enzyme-inducing ASMs. 31 No clinically severe DILI was reported in cannabidiol's clinical studies or during post-marketing surveillance. 32 However, in healthy volunteers, cannabidiol increased ALT levels by ≥5XULN 33 or caused liver enzyme elevations coupled with eosinophilia. 34 Several cases have required treatment withdrawal. Valproate can induce asymptomatic serum aminotransferase elevations or hyperammonemia without other evidence of liver injury. 10 The hyperammonemia in this context is not a sign of liver failure. Therefore, valproate treatment may sometimes be continued if liver tests are up to 3X the baseline levels and the patient is asymptomatic.7,35
Most enzyme elevations resolve even with continued drug exposure.4,36 In a 2011 phenotype standardization paper, the ALT elevation cutoff was raised for low-risk medications (e.g., cannabidiol and brivaracetam)17,35,37 to 5XULN to better represent clinically important liver injury as is used in the US National Institutes of Health-sponsored Drug-Induced Liver Injury Network (DILIN).1,12 Thresholds have also been set for AP elevations, combined bilirubin and ALT elevations, and international normalized ratio. 1 These thresholds do not apply to certain conditions such as hypersensitivity reactions and mitochondrial toxicity. For example, felbamate should be discontinued if liver enzymes rise to 2XULN, or with the appearance of clinical symptoms indicative of liver failure. 8 The threshold for valproate is 2 to 3X ULN. In August 2025, the Food and Drug Administration (FDA) issued a safety warning for cenobamate due to markedly elevated serum hepatic transaminases with elevated total bilirubin and cases of acute liver failure requiring transplantation. 17 A predictor for cenobamate severe liver injury is ≥3-fold elevation of hepatic transaminases with ≥2-fold elevated total bilirubin. 17 Failure to withdraw drugs that lead to test abnormalities can result in severe or persistent liver damage.18,23
DILI “Signatures” and Hypersensitivity Reactions
Aromatic ASMs, including carbamazepine, lamotrigine, and zonisamide, have signature clinical and laboratory DILI phenotypes (Table 3). Other notable phenotypes include drug reaction with eosinophilia and systemic symptoms (DRESS), also known as anticonvulsant hypersensitivity syndrome 38 and Stevens-Johnson syndrome and toxic epidermal necrolysis (SJS/TEN).3,23
Examples of DILI Phenotypes.
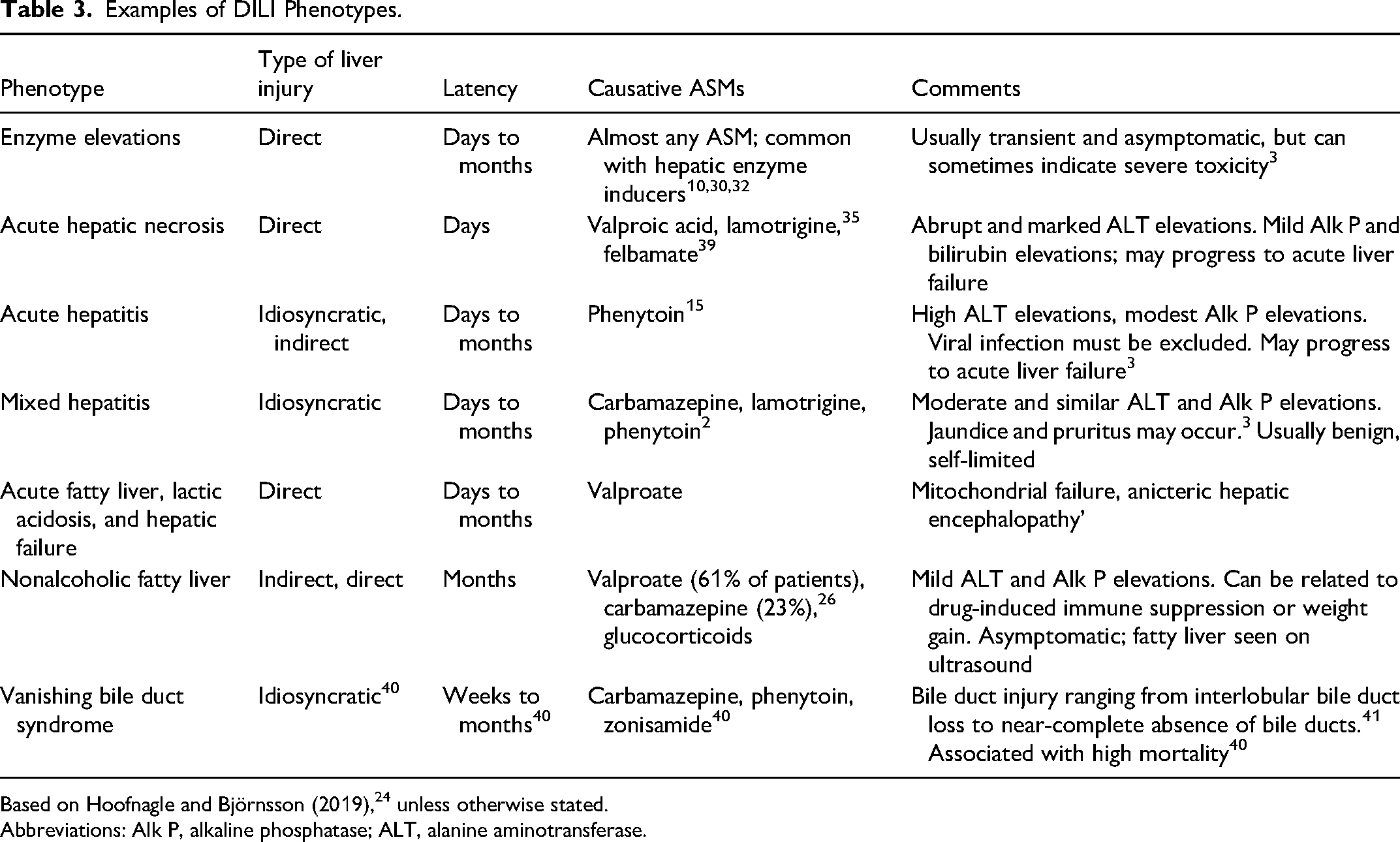
Based on Hoofnagle and Björnsson (2019), 24 unless otherwise stated.
Abbreviations: Alk P, alkaline phosphatase; ALT, alanine aminotransferase.
DRESS affects the liver in 60% to 100% of cases, 23 and DRESS-like features are commonly seen in liver injury related to lamotrigine, phenytoin, and carbamazepine, but are rarely observed with valproate and gabapentin. 10 DRESS cases have also been reported with eslicarbazepine, levetiracetam, and clobazam,17,42 as well as with rapid titration of cenobamate. 35 As of October 2025, no cases were reported under the FDA-approved slow cenobamate titration schedule.35,43
SJS/TEN represent a spectrum of severe adverse cutaneous reactions associated with high mortality that increases in the presence of DILI (36% to 46%). 3 SJS/TEN has been primarily attributed to the aromatic ASMs carbamazepine, phenytoin, and lamotrigine, and, less frequently, oxcarbazepine 19 and eslicarbazepine. 17
Injury Mechanisms
The 3 most common mechanisms of direct hepatotoxicity are mitochondrial dysfunction, oxidative stress, and inhibition of bile acid efflux transporters.1–3 Mitochondrial dysfunction often has a delayed presentation over several months, 44 and has been implicated in almost all forms of valproate7,8 and phenobarbital hepatotoxicity. 7 Oxidative stress can occur when the pool of hepatic glutathione or the free radical scavenger carnitine is depleted.8,44 Inhibition of canalicular efflux transporters is not typically implicated in ASM-induced DILI.
Idiosyncratic DILI is believed to be multifactorial, involving individual, genetic, and environmental factors. It has been attributed to the stimulation of the immune system by immunogenic haptens, usually in association with reactive metabolites. 2 Everolimus can exert indirect hepatotoxicity with potentially fatal reactivation of hepatitis B virus due to its immunosuppressive effects as well as direct liver injury. 25 Another example of indirect hepatotoxicity is the weight gain associated with valproate treatment that can lead to the development of fatty liver. 26
Risk Determinants
A patient's risk of developing idiosyncratic DILI is determined by interactions among the drug properties, host factors, and the environment. 21
Host Factors
Coexistent liver disease is associated with poor outcomes with a DILI episode but not necessarily with a higher DILI risk.15,45 The relationships between ASM-DILI susceptibility and the individual's characteristics are not well-established. Standardized DILI risk increases with age, likely in association with polypharmacy, 23 whereas children younger than 10 years old have a higher risk of developing valproate-associated DILI than adults, and those less than 2 have the highest risk of a fatal outcome. 23 The higher risk of younger children has been attributed to inborn impairment of mitochondrial function 16 and to an increased formation of the reactive metabolite 4-ene-valproate by CYP2C9. 46
African Americans were over-represented among individuals who developed liver injury due to phenytoin,10,24 lamotrigine, and carbamazepine. 10 In line with this phenomenon, the human lymphocyte antigen (HLA)-B∗53:01 was identified in 8 of 9 phenytoin DILI cases involving African Americans (odds ratio 9.2, 95% confidence interval [CI]: 3.61-23.28), and was also a risk factor for other ASMs. 47
Carriers of HLA-B*15:02 of south-Asian ancestries are at an increased risk of carbamazepine, oxcarbazepine, or lamotrigine-induced SJS/TEN, with a carbamazepine-oxcarbazepine cross-sensitivity (likely encompassing also eslicarbazepine).17,19 The predictive value of other HLA associations for ASM-induced liver injury is currently low. 15
Valproate is contraindicated in patients with mitochondrial disorders caused by polymerase γ gene (POLG) mutations. 17 Patients with inborn errors of metabolism or reduced hepatic mitochondrial activity may also be at an increased risk for topiramate hyperammonemia with or without encephalopathy. 17 Polymorphism (rs2476601) in PTPN22, encoding a protein that down-regulates T-cell receptor signaling, is a risk factor for all-cause DILI, 15 with an odds ratio for valproate of 2.43 (95% CI 0.99-5.95). 48
Drug Properties
Attempts to predict DILI risk have commonly implied the drug's dose, lipophilicity, and the formation of reactive metabolites.21,44,49 The daily dose of ASMs implicated in DILI is >50-100 mg.2,15,44 Idiosyncratic DILI may also be associated with dose elevations. For instance, escalation of the daily lamotrigine doses preceded 10 of 18 liver injury cases. 15 Higher lipophilicity is associated with increased off-target binding 23 and facilitated drug uptake into hepatocytes with subsequent hepatic metabolism. Because reactive metabolites can bind covalently to cellular proteins and modify their properties, such that they become haptens or activate cellular pathways, they are considered an important DILI risk factor.23,44 Presumed hepatotoxic metabolites include the arene oxides (epoxides) of phenytoin, carbamazepine, and lamotrigine,18,20 and valproate's 4-ene metabolite. 18 Reactive metabolites may also play a role in the hepatotoxicity of felbamate and phenobarbital.8,20
LiverTox (www. https://www.ncbi.nlm.nih.gov/books/NBK547852/) 35 provides likelihood scales that consider the number of related hepatotoxicity reports per drug. Five ASMs and corticosteroids are included in category A (well-known hepatotoxins). Felbamate is a category B drug because it is not in common use. When the DILI score was applied to a series of 24 FDA-approved ASMs, it was well correlated with their likelihood of liver injury based on their aforementioned characteristics (Figure 1). It also predicted low hepatotoxic propensity of fenfluramine and moderate risk for ganaxolone, both of which are not included in LiverTox as of October 2025.
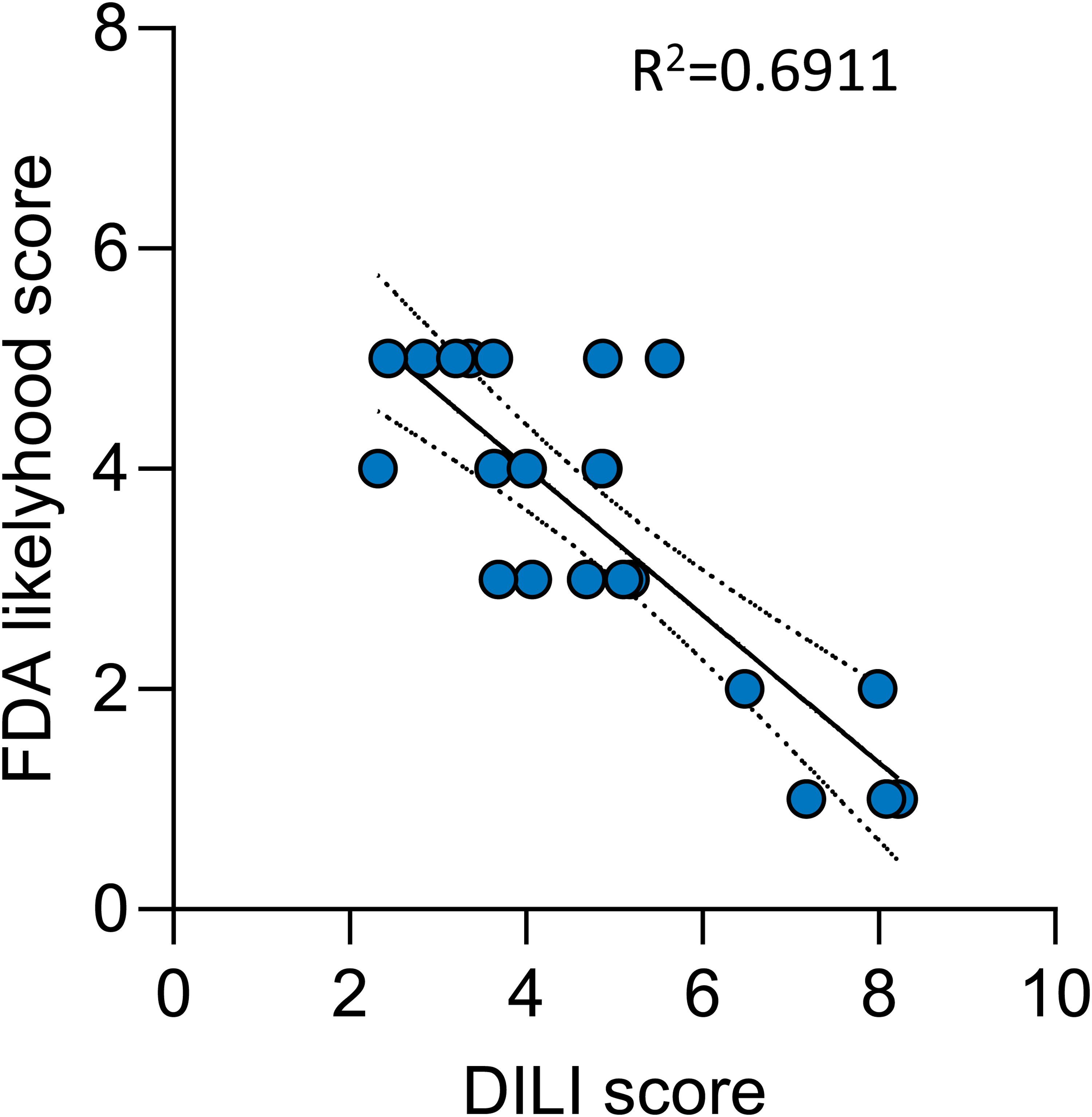
Correlation between DILI scores and LiverTox likelihood scales for 24 ASMs at their maximal daily recommended doses. The likelihood scales A-E were substituted with numerical values (5 = high likelihood). ASMs categorized as E* were excluded due to low reliability. The interpolated likelihood scores for fenfluramine and ganaxolone (for which no likelihood was assigned in LiverTox) were E (Low) and C (moderate), respectively. The maximal daily dose of fenfluramine is <50 mg, its LogP (a lipophilicity indicator) is 3.5, and it has an active but not reactive metabolite. The maximal daily dose of ganaxolone is 1800 mg, its LogP is 4 (more lipophilic than fenfluramine), and it does not generate a reactive metabolite.
For further details on ASM-DILI, the reader is referred to the AES website (https://aesnet.org/docs/default-source/pdfs-clinical/antiseizure-medications-and-liver-health-a-summary-of-drug-induced-liver-injury-(3).pdf?sfvrsn=ae981ca1_1).
Drug-Drug and Drug-Diet Interactions
Enzyme-inducing ASMs can increase the formation of reactive metabolites, such as those of valproate 23 and acetaminophen, 15 necessitating higher doses of the affected drug with further metabolite exposure. This adds to the hepatotoxic potential of inducers like phenytoin and carbamazepine. Combinations with enzyme inducers have been reported to increase the incidence of valproate-related hepatotoxicity, hyperammonemia, and encephalopathy. 20 Similarly, long-term ASM use heightens acetaminophen 50 and isoniazid51,52 hepatotoxicity. Strong inducers are contraindicated with the tyrosine kinase inhibitor lorlatinib. 17 The pharmacokinetic interaction between lamotrigine and valproate involves enzyme inhibition, shifting lamotrigine metabolism from glucuronidation to oxidation with enhanced formation of lamotrigine's arene oxide. 20 This combination raises the risk of DRESS and SJS/TEN, often with hepatotoxicity. 1
Coadministration of topiramate and valproate has been associated with hyperammonemia, with or without encephalopathy, even in patients who tolerate each drug alone.7,17 In clinical trials of cannabidiol, transaminase elevations above 3XULN were more common in patients already on valproate. Risk was even greater when cannabidiol is combined with clobazam and valproic acid. 17 Severe hepatotoxicity has also been reported with the ketogenic diet-valproate combination. 53 Carnitine levels should be monitored in children receiving this cotherapy. 54
Management and Outcomes
Discontinuing suspect drugs is central to managing idiosyncratic DILI but can be challenging. For example, tapering felbamate over approximately 2 weeks and adjusting concomitant ASMs resulted in a significant increase in seizure frequency, 9 with at least one report of status epilepticus during tapering. 55
The decision to add another ASM during DILI management depends on seizure severity and concurrent medications. Benzodiazepines can be used for status epilepticus and as bridging therapy, but caution is needed in acute liver injury. Lorazepam may be considered as its metabolism is minimally affected by liver disease, 7 although midazolam could be favored due to shorter half-life or for continuous infusion. Levetiracetam, brivaracetam, and lacosamide can be intravenously loaded for rapid coverage during medication transition with low encephalopathy risk. Gabapentin and perampanel are oral options with low risk for hepatotoxicity or hypersensitivity reactions.7,56
Beyond drug withdrawal and supportive care, N-acetylcysteine therapy may be considered for treatment of DILI in adults, especially severe DILI with acute liver failure, with recent reviews suggesting value, but it is not currently routine practice.57–61 Steroids may help in hypersensitivity reactions, 7 but their overall value in DILI is unclear. 62 In valproate-associated liver injury, carnitine supplementation is recommended. 7
Early consultation with a hepatologist and referral to a liver transplant center, before encephalopathy, is critical. Recent case reports estimate DILI-related mortality is 13%. 63
Prevention
Even when based on limited exposure, early safety signals may be present during the pre-approval process, although they are sometimes overlooked. The FDA and European Medicines Agency (EMA) provide clear guidance on evaluating such signals in the context of premarketing clinical development, and for preclinical evaluation.5,64
The value of routine monitoring of liver enzyme levels in serum in asymptomatic patients has not been established. 8 However, the likelihood of recovery from DILI can be enhanced by frequent blood tests and patient reporting on early signs of toxicity with immediate withdrawal of the suspect drug. 17 Therefore, liver enzyme tests should be monitored before treatment and periodically in patients treated with high-risk ASMs, including cannabidiol, carbamazepine, cenobamate, ethosuximide, felbamate, and valproate. 17 Monitoring has also been recommended by the EMA for stiripentol. 56 For the other ASMs, monitoring is recommended before ASM initiation or addition, in symptomatic patients, high-risk populations, and non-verbal patients. 20 Liver enzyme monitoring may be particularly useful in the pediatric population. 65 It is also advisable to screen for the presence of hepatitis B before starting everolimus therapy. 35
The American College of Gastroenterology strongly recommends against re-exposure to a drug that likely led to hepatotoxicity, except in life-threatening conditions when no alternative is available. 16 Oxcarbazepine (and eslicarbazepine acetate) should not be prescribed for patients who have had hypersensitivity reactions to carbamazepine, unless the potential benefit justifies the potential risk, 19 and avoiding other aromatic ASMs should be considered. 17 Aromatic ASMs are suggested to be avoided in African American patients, or if used, patients should be followed closely and advised to stop the drug promptly at the first signs of skin reactions or liver damage. 10
Patients should be educated about the risks of hepatotoxic ASMs, identification of hepatotoxicity symptoms, and the importance of prompt reporting of any new or untoward symptoms to their provider.15,37 Symptoms potentially related to hepatotoxicity include abdominal pain, nausea, vomiting, itching, dark urine, and rash.
Unmet Needs and Knowledge Gaps
The likelihood of idiosyncratic DILI related to newly introduced ASMs and several less commonly used older ASMs has not yet been established. Signals can be detected by pharmacovigilance systems such as the Adverse Event Reporting System (FAERS) database, as has been recently reported for clobazam, 42 oxcarbazepine, and levetiracetam. 28 Knowledge gaps are also related to an incomplete understanding of genetic risk and limited guidance for re-challenge in patients who have experienced ASM-DILI. Another unmet need is the identification of more sensitive and specific diagnostic and prognostic DILI biomarkers. Emerging candidates include miRNA-122 (miR-122) and raised serum glutamate dehydrogenase (GLDH),3,15,16 but these and other emerging biomarkers have not been validated for any ASM. 16
Conclusions
ASM-related liver injury is often manifested as “idiosyncratic” reactions yet may be preventable. Important precautions include the consideration of the individual's risk factors; baseline and periodic monitoring of hepatic function for high-risk drugs and at-risk individuals; slow titration, particularly for lamotrigine and cenobamate; avoiding combinations of hepatotoxic compounds with enzyme inducers when possible; immediate discontinuation under medical supervision of causative ASMs when hepatotoxicity or hypersensitivity reactions are suspected; and patient education. Given the multitude of DILI phenotypes and the potential for severe consequences, it is recommended that a hepatologist is consulted early in the course of DILI.
Highlights
The antiseizure medications (ASMs) associated with the highest liver injury risk are carbamazepine, felbamate, lamotrigine, phenytoin, valproate, and corticosteroids.
Additional newer-generations ASMs, including oxcarbazepine and cenobamate, have also been associated with liver injury.
Combinations of hepatotoxic ASMs, particularly hepatic enzyme inducers, with other liver-damaging compounds should be avoided when possible.
The hepatotoxicity risk of some ASMs is higher among African Americans, the elderly, and children.
Routine hepatic enzyme monitoring is recommended particularly for at-risk patients or those treated with high-risk ASMs.
Footnotes
Acknowledgments
The authors undertook this effort as representatives of the Treatments Committee of the American Epilepsy Society. This publication underscores the commitment of the American Epilepsy Society, the Council on Clinical Activities, and its committees to advancing patient care, promoting education, and fostering innovation within the epilepsy community. The authors thank Lauren Orciuoli for facilitating meetings, overseeing progress, and helpful comments on the manuscript.
Author Contributions
All authors contributed to the conception of the review. The first draft of the manuscript was written by SE in collaboration with MB. All authors critically reviewed and commented on the manuscript and approved the final manuscript for submission.
Declaration of Conflicting Interests
Nicole Woodrich is on the advisory board for SK Life. Sara Eyal has served as a consultant for Dexcel, Israel. The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Eyal's research is funded by the Israel Science Foundation and the Israeli Ministry of Science and Technology.