
Abstract
This review provides a practical, evidence-informed approach to initiating pharmacologic treatment for children and adolescents with epilepsy who present with comorbid neuropsychiatric symptoms including depression, behavioral dyscontrol, and attention-deficit/hyperactivity disorder. The paper addresses how to determine when medication is warranted, outlines considerations for medication selection, and offers general principles for medication initiation and monitoring. Although the discourse is aimed at a pediatric population, the concepts are applicable to other ages as well. The goal is to provide clinicians with a decision-making framework to optimize both neurological and psychiatric outcomes in this complex population.
Keywords
Introduction
Persons with epilepsy are at increased risk for neuropsychiatric comorbidities, including anxiety, mood disorders, behavioral dysregulation, and attention-deficit/hyperactivity disorder (ADHD). In pediatrics, epidemiological studies suggest that 30%–50% meet diagnostic criteria for at least 1 psychiatric disorder. 1 These comorbidities often contribute to greater functional impairment than the seizures themselves. However, managing these symptoms pharmacologically is complicated by concerns about seizure threshold, medication side effects, and diagnostic uncertainty. This review provides an evidence-informed practical guide to using common psychiatric medications in pediatric epilepsy.
When to Consider Psychiatric Medication
Because psychiatric illness is so commonly associated with epilepsy, neurologists often face the prospect of considering psychiatric medicines. The availability of specialty pediatric neuropsychiatrists is low, and even then, most general psychiatrists have little experience with developmental disabilities or epilepsy. However, most neurologists can initiate a basic treatment plan that can effectively bridge the gap until a specialist is available. 2 It should be noted that behavioral treatments or psychotherapy are often preferred as initial steps, though in many cases, such efforts have already been attempted without success.
The first step is an assessment of the level of impairment. If day-to-day function or typical development is significantly and persistently altered, then aggressive treatment should be considered. Certain clinical features can be considered as red flags that more often necessitate pharmacologic intervention. These include persistent and significant irritability, social withdrawal, apathy, academic decline, episodes of explosive aggression or marked impulsivity, and neurovegetative symptoms such as impaired energy, sleep, appetite, or nonspecific somatic complaints such as gastrointestinal discomfort or headaches. 3
The next step is to rule out seizure-related causes of behavioral symptoms, including ictal or peri-ictal phenomena. It is equally important to assess for iatrogenic causes of psychiatric symptoms. Mood disruption (or improvement) may result from any antiseizure medicine (ASM) though often occurs with levetiracetam or phenobarbital.4,5 Cognitive disturbances or sedation may result from the use of benzodiazepines. Still, it is prudent to adjust ASMs as a first step, as opposed to prescribing additional psychiatric medications.
From Behavior to Diagnosis: A Dimensional Framework
Neurologists may feel pressured to convincingly establish a diagnosis prior to considering psychiatric treatment. However, ambiguity is inherent in psychiatric diagnoses, despite longstanding efforts to aggregate categorical criteria into diagnostic entities. Behavioral symptoms in epilepsy may be even more difficult to isolate, but may be better understood through a dimensional lens rather than with rigid diagnostic categories. Symptoms such as impulsivity or aggressive outbursts overlap diagnostic categories and may be reasonable to consider as specific medication targets. Validated questionnaires may be useful, but usually only as an adjunct to clinical impressions.
Understanding the temporal association of symptoms with seizure activity, medication changes, and environmental stressors is also helpful in decision-making. Although psychiatric medication may be necessary regardless of the temporal relationship of target symptoms to seizure events, closely related symptoms may imply ASM adjustments as initial steps. Another key distinction to be assessed is whether a behavior is spontaneous, reflecting intrinsic biological instability, versus reactive—contextually triggered or situation-specific. Spontaneous outbursts of aggression or severe outbursts even if contextually related, both imply paroxysmal neuronal activity. Such behaviors may then be good targets for ASMs, which are ideally suited to address the rapid propagation of disruptive neuronal activity.
Antiseizure Medications as Neuropsychiatric Agents
The positive psychotropic properties of ASMs are becoming increasingly recognized. Valproate, lamotrigine, and carbamazepine have established mood-stabilizing properties in children with epilepsy and comorbid affective dysregulation.6,7 Any ASM with such dual action may be especially advantageous for psychiatric comorbidity. 8 Anxiety control may improve with clobazam, pregabalin, or cannabidiol.9–12 Ultimately, the strategic use of ASMs to stabilize mood or impulsivity along with epilepsy may be a powerful intervention. 13
Monitoring of ASM serum levels may be nuanced for psychiatric management. As an example, for valproate, seizure control may be obtained at lower serum levels than that necessary for mood stability. Mood symptoms have been reported to require higher blood levels, above 94 mcg/mL, which is above the level typically required for seizure control. 14 A first step for clinicians may be to increase doses of existing ASMs to synergistically address behavioral concerns.
Medication Side Effects Mimicking Neuropsychiatric Symptoms
Sometimes ASMs can induce or exacerbate psychiatric symptoms. 15 Phenobarbital and topiramate are associated with elevated risk for depressive and cognitive side effects, including slowed processing and affect flattening.16,17 Levetiracetam, perampanel, and clobazam have been associated with increased irritability, aggression, and mood lability. Cognitive side effects may also arise from clobazam, topiramate, and abrupt withdrawal of benzodiazepines.16,18,19 A high index of suspicion and a clear understanding of ASM side effect profiles are essential to distinguish iatrogenic effects from independent psychopathology. Details of the potential positive and negative psychiatric effects of ASMs are given in Table 1.
Possible Positive and Negative Psychiatric Effects of Antiseizure Medications.

Case Examples
Attention-Deficit/Hyperactivity Disorder (ADHD)
A 7-year-old male with bilateral motor seizures had been seizure-free for over a year with levetiracetam. His development was age-appropriate; however, over the past year, he had worsening distractibility and impulse control. He frequently interrupted others, left his seat without permission, and blurted out answers before being called on. He appeared easily distracted by sounds in the hallway or by other students. Homework had become a nightly battle, taking hours to complete even a 15-min assignment, and his grades slipped. During the office visit, he was friendly but had difficulty staying seated and often interrupted to talk about his favorite video game. His neurologist observed no signs of anhedonia, dysphoria, irritability, or anxiety. Given the stable mood, the neurologist did not consider changing the levetiracetam. The neurologist asked the parents and the teacher to complete a standardized questionnaire, the Vanderbilt Parent and Teacher Rating Scale, which was obtained and showed elevated scores in both inattention and hyperactivity/impulsivity domains. Given his age, neurological history, and broad impact on daily life, the neurologist diagnosed ADHD, Combined Type, and determined that intervention was necessary.
The neurologist explained that ADHD is more common in children with epilepsy and can emerge even in the context of well-controlled seizures. They discussed nonpharmacological interventions including classroom accommodations and behavioral therapy. However, given the level of impairment and failure of nonmedical interventions, sustained release methylphenidate (50/50 biphasic release) 10 mg QAM was recommended.
The family was cautioned about the potential exacerbation of seizures, but also noted that since the epilepsy was stable, at a rate of <1 seizure per month, the risk was very low. The family was told to watch for any potential side effects, mood disruption particularly. The family was also instructed to be disciplined about having breakfast, as appetite for lunch may be decreased. The patient rapidly improved sustained attention and impulse control, though, after 2 weeks, he appeared to have residual symptoms. The dose was increased to 20 mg in the morning, and by the following week, most symptoms of ADHD had resolved.
Depression
A 17-year-old female with focal unaware seizures had good seizure control with brivaracetam. However, in the past 6 months, she began refusing to do schoolwork and her grades worsened from A's to C's. She was argumentative with her family and stopped socializing with friends. She complained of being tired, even though she slept 9 hours every night. Her appetite decreased, though she had not lost weight. When asked why she was resisting schoolwork, she snapped and said, “what is the point?” When asked if she was depressed, she shrugged and said, “I don’t know.” The neurologist boldly asked about self-harm, and the patient denied suicidality but did acknowledge that she did not think her life mattered. The neurologist was confident that the diagnosis was Major Depression, because of the presence of vegetative symptoms such as altered sleep and appetite, and other symptoms such as anhedonia, irritability, worsened academic function, negative outlook, and a distinct change from usual activities.
The neurologist discussed the diagnosis with the patient and family and added that epilepsy with a seizure focus in the temporal lobe is often associated with depression. The neurologist was very uncomfortable waiting for a psychiatry referral, given the neurovegetative symptoms (sleep and appetite), irritability, passive death ideas, and a notable decrease in functionality. The neurologist considered changing the ASM, but given the good seizure control, did not want to risk destabilization. Instead, sertraline was started at 25 mg in the morning, with instructions to carefully monitor for any worsening of mood, hyperactivity or activation, suicidality, as well as gastrointestinal (GI) symptoms such as nausea. The neurologist requested a follow-up appointment in 4 weeks and said that the office nurse would be contacting them by phone, weekly for a check-in.
After 2 weeks, there was no change in mood or function, and the nurse informed the neurologist who increased the dose to 50 mg. After 4 weeks, the parent reported that the patient's energy and sleep improved, and she became less argumentative and irritable. She still did not participate in activities but was turning in more schoolwork. The neurologist decided to keep the dose of the medicine the same but again wanted a follow-up appointment in 1 month, and that the nurse would check in again, in 2 weeks.
Aggressive Outbursts
A 13-year-old male with Lennox-Gastaut Syndrome and intellectual disability was referred due to escalating aggressive behavior. He had multiple seizure types—tonic, atypical absence, and occasional generalized tonic–clonic seizures, partially controlled on clobazam and valproate. He was ambulatory but had limited expressive language and required support for all daily activities. Over the past 6 months, caregivers and school staff reported frequent episodes of aggression, including hitting, biting, scratching, and throwing objects. These episodes occurred several times per week and appeared to be both spontaneous and reactive. Reactive aggression was typically triggered by transitions, demands placed on him, or sensory overload. Behavior logs showed no temporal relationship between aggression and seizure activity. Pain, illness, and medication side effects were ruled out. Given the significant aggression, risperidone was started at 0.25 mg in the morning. The rationale included its evidence base in managing irritability in children with neurodevelopmental disorders and favorable tolerability at low doses. 6 Concurrently, a school behavior plan was developed with visual supports, structured routines, and calming strategies. At a 4-week follow-up, he had fewer spontaneous outbursts and less intensity of reactive outbursts. No adverse effects were observed, and the weight was unchanged. The dose was increased to 0.5 mg daily and then twice a day, with improvement in the intensity of the outbursts.
Initiating and Monitoring Psychiatric Medication
The adage of “start low, go slow,” still holds true for titration; starting with the lowest possible dose and only gradually increasing will mitigate the risk of side effects. Therapeutic goals should be clearly defined, not only on symptom reduction, but also on measurable improvement in school performance, social interactions, and frequency of aggressive outbursts. Key clinical domains, including mood, behavior, sleep patterns, and seizure frequency should be evaluated at regular intervals—typically every 2 to 4 weeks during the early stages of treatment. Weekly monitoring during initiation phases may help avoid activation-related intolerance of antidepressants, or mood worsening with stimulants.
Monitoring is key for children and adolescents taking antipsychotics. Weight gain is a common risk, and is usually associated with appetite increase. Sometimes the medication needs to be discontinued in those circumstances. Serum monitoring of lipids, fasting glucose, and hemoglobin A1c (HbA1c) should be done. In any patient who has notable weight gain, consideration of an antihyperglycemic agent such as metformin should be strongly considered. Details for selected usage of selected psychiatric medications are given in Table 2.
Guide for Selected Psychotropic Medication: Dosing, Indications, and Monitoring. 48
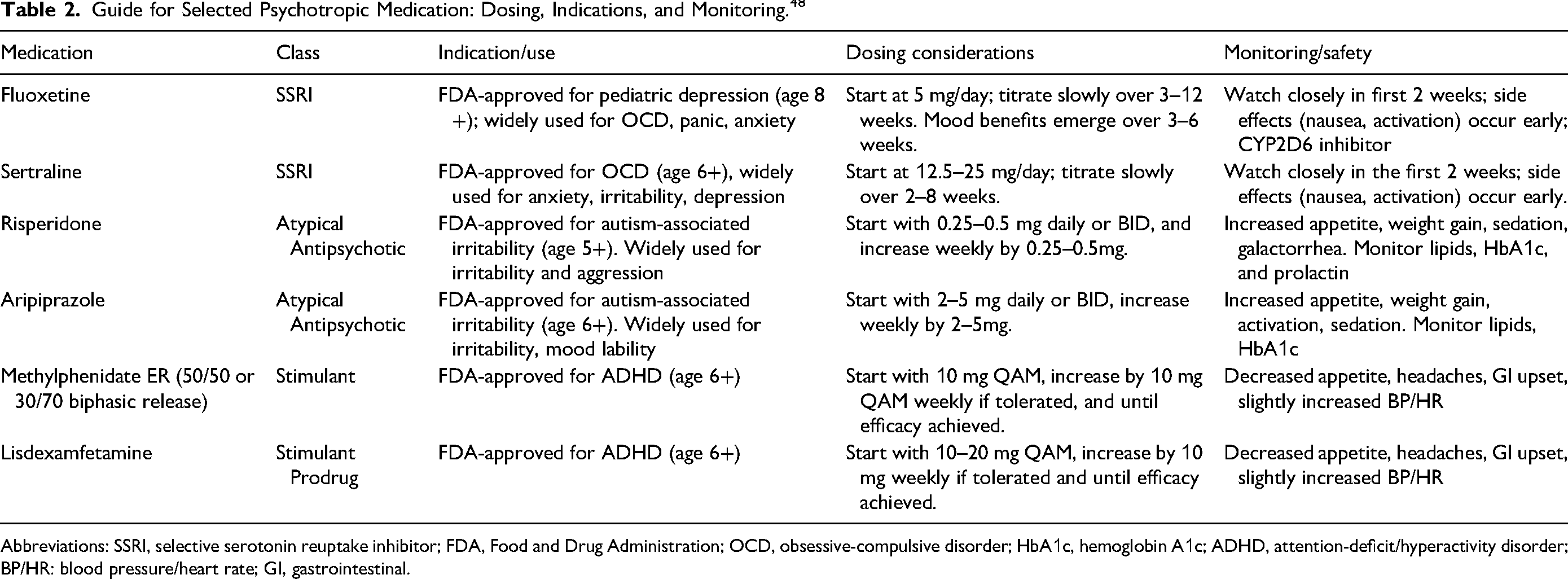
Abbreviations: SSRI, selective serotonin reuptake inhibitor; FDA, Food and Drug Administration; OCD, obsessive-compulsive disorder; HbA1c, hemoglobin A1c; ADHD, attention-deficit/hyperactivity disorder; BP/HR: blood pressure/heart rate; GI, gastrointestinal.
Additional Considerations
The intersection of epilepsy and psychiatric comorbidity may lead to complex pharmacologic regimens. Clinicians should resist pressure to engage in multiple simultaneous medication trials or to make frequent changes without clear justification. Priority should be given to using ASMs with dual efficacy and recognizing that psychiatric medicines may require a long time to work. It should also be noted that children with an intellectual disability or autism spectrum disorder may have paradoxical responses to treatment. Treatment in this population requires individualized goal setting and flexible monitoring that accommodates communication difficulties, atypical symptom presentations, and baseline behavioral variability.
Algorithm for Medication Initiation
Confirm psychiatric symptoms are not seizure-related or iatrogenic.
Confirm that functional impact is significant.
Review the ASM profile and avail agents with a possible “dual role.”
Choose psychiatric medication targeted to the most concerning symptoms.
Monitor often during the titration phase
Adjust the dose or discontinue medication based on symptom response and tolerability.
Conclusion
The field of neuropsychiatry provides a paradigm to consider brain-based diseases as inseparable from behavioral and mood concerns. Epilepsy fits well with this heuristic. Integrating psychopharmacology into epilepsy care requires the recognition that ASMs are not only antiseizure agents but also neuropsychiatric modulators. The selection of additional psychopharmacologic agents can be guided by the level of dysfunction, target symptoms, developmental context, and drug interaction profiles. Clinicians should be reassured that treating psychiatric symptoms can yield meaningful benefits in mood, behavior, and overall quality of life.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.