
Abstract
Epilepsy and psychiatric illness have been long studied and today are better accepted as co-occurring than as discrete illnesses that are independent even if associated. Common pathophysiology may not be easily explained, but clearly exists given the significant overrepresentation of psychiatric illness among individuals with epilepsy. Conditions like autism spectrum disorder, anxiety, depression, and attention deficit hyperactivity disorder are prevalent in pediatric epilepsy much more than expected, even in the context of chronic neurologic disease. The interplay between pediatric epilepsy and neuropsychiatric symptoms represents a complex clinical circumstance that is not well subtended by the chasm-like division of labor between psychiatrists and neurologists. The unfortunate result is that children and families often experience care that is fractured and at worst, counterproductive for their quality of life. A neuropsychiatric paradigm is essential to address epilepsy and its intrinsic psychiatric symptoms. Practical strategies will be discussed to address this challenge.
Introduction
As a field, we have known for a very long time that there is something different about epilepsy. Epilepsy is more complicated than other chronic medical illness when it comes to co-occurring psychiatric symptoms. For over 50 years, we have known that pediatric epilepsy has a particularly high prevalence of psychiatric comorbidity, the explanation of which cannot be accounted for solely by psychosocial stress of chronic disease or side effects of treatment. 1 Although such symptom etiologies are notable, they are not specific to epilepsy. Instead, with epilepsy overall and especially in pediatrics, we are called upon to think neuropsychiatrically, with a new paradigm that incorporates both neurologic and psychiatric heuristics.
Therein lies a daunting problem that neurologists and psychiatrists often don’t talk to each other. 2 In medical education of the past 100 years, doctors have been taught that behavior and seizures must be addressed differently. The neurologist will treat the seizures, and the psychiatrist will treat the behavior. However, this is a spurious dichotomy, unfortunately or unwittingly reinforced by the momentum of compartmentalization that allows even intellectually advantaged physicians to settle for partial solutions to problems. Although our treatment armamentarium has expanded, our understanding of pathophysiology has not kept pace. Individual clinicians who are well versed in both epilepsy and behavior to the point of determining comprehensive treatment plans are still uncommon.
However, there is room for optimism. Voices continue to be heard regarding the plight of children and families seeking to have a unifying treatment approach. Program content in 2023 conferences of the International League Against Epilepsy and the American Epilepsy Society has included prominent symposia addressing comorbidity. The concept of developmental and epileptic encephalopathies has propelled a comprehensive treatment approach, to the extent that a dedicated questionnaire tool in Tuberous Sclerosis Complex includes an “associated neuropsychiatric disorders” assessment and de facto acknowledgement. 3
For this review, we highlight evidence that reinforces a neuropsychiatric paradigm, one that suggests that blending treatment targets of seizure counts and behavior issues is not only intuitive but necessary to improve outcomes. Such an approach emphasizes the importance of integrated treatment strategies implemented by a coordinated clinical team.
The Neuropsychiatric Diaspora in Epilepsy
A significant proportion of children experience neuropsychiatric comorbidities, including attention deficit hyperactivity disorder (ADHD), autism spectrum disorder (ASD), anxiety, and depression which significantly impair quality of life (QOL) and complicate treatment strategies. The cognitive, behavioral, and social challenges associated with pediatric epilepsy must be addressed concurrently, considering a child’s vibrant neurodevelopment and the brain’s activity-dependent processes of growth and maturation.
Recent reports of bidirectionality lend additional credence to the notion that epilepsy is different from other chronic illness. Although it may be intuitive that the stress of having epilepsy may worsen mood and lead to the development of depression, the notion that psychiatric illness may also beget epilepsy has been reinforced by many recent studies. 4 -7 A higher-than-expected prevalence of psychiatric disorders among children with epilepsy compared to their peers has been well documented in literature. 4,8 -10 The classic Isle of Wight childhood epidemiology study highlighted that 29% of children with epilepsy exhibit psychiatric illnesses, as opposed to 16% in those with other chronic medical conditions. 11 Epilepsy co-occurs in up to 30% of children with ASD, 12,13 plus anxiety and depression are prevalent in 10% to 33% of people with epilepsy. 14 -16 Children with epilepsy exhibit a higher prevalence of ADHD, particularly the inattentive subtype 17 with around 22% also displaying hyperactivity or impulsivity. 17,18 It cannot be denied that epilepsy often includes psychiatric comorbidity but the co-occurring symptoms may involve intrinsic brain and behavior relationships that imply pathophysiologic overlap.
What Is Comorbidity?
It is a sad and true statement that the word, “comorbidity” does not do justice to a disease like epilepsy. Comorbidity defined means that multiple disparate conditions co-occur in the same person. A person with seizures localized to the mesial temporal lobe may commonly have symptoms of anxiety or depression. That much we know, and studies in pediatrics have affirmed this supposition. 19,20 But what if there is a nuance to thinking about “temporal lobe epilepsy” in that symptoms of the disease include not only focal unaware seizures but also acute anxiety phenomena as well as chronic depression.
Thinking separately about psychiatry and neurology means that we have to make arbitrary definitions of seizure time periods and then declare symptoms as either peri-ictal or inter-ictal. Depending upon the attribution given to chemical and electrical instability prior to or following the seizure event, definitions of peri-ictal periods may vary anywhere from a few minutes to a few days. Further confusing our understanding is that ictal phenomena may include psychiatric symptoms. In the case of mesial temporal lobe seizure foci, anxiety or fear may be present as part of the ictus. In the case of frontal or generalized seizures, inattention or disrupted consciousness may be constituent components of the event.
While the effort to consider psychiatric comorbidity in relationships to seizure events was groundbreaking decades ago, separating out such symptoms has recently proven to be reductionistic to the point of hindering treatment. Examples abound of either a neurologist or a psychiatrist, even when adhering to standard of care approaches in their workspace, nevertheless neglect associated symptoms that compromise function. For example, an adolescent may have focal unaware seizures localized to the temporal lobe that occur weekly. Such a patient may not reveal to the neurologist that they also have mild depression and irritability. The neurologist, seeking a high yield treatment to address seizures, may prescribe levetiracetam. The seizures may become markedly less frequent, but the mood and irritability may worsen, as has been shown to occur with levetiracetam. 21,22 The neurologist will consider that the mission has been accomplished. However, the patient is not actually better, and indeed the patient’s QOL has worsened, even though the seizure control has apparently improved.
Quality of Life
Quality of life is a universal human goal. Regardless of targeted arbitrary medical metrics, improving how someone lives is the ultimate reason for seeking health care. In epilepsy, we already know that treating behavioral comorbidities is an efficient pathway to improving QOL. Reasonable studies have been done showing that treating comorbid psychiatric symptoms will improve QOL even more than improving seizure control. 23 While this may seem intuitive, in practice such treatment approaches are not instinctive given our siloed and divergent approach to health care and mental health care. In pediatrics, several measures of QOL have been well established. An adolescent self-report scale has been developed (QOLIE-AD) 24 as well as a parent scale (QOLCE). 25 These have been well used in research circles, though less so for clinical purposes. Ultimately, treatment that is geared to improving QOL will necessitate treatment of associated psychiatric illness.
Depression in Epilepsy
Treating depression may be the surest way to improve QOL for persons with epilepsy. 26 Depression is common in pediatrics, although in younger aged children, somatic symptoms such as persistent headaches or gastrointestinal issues may overshadow the emotional components of the disorder. Children commonly have irritability rather than overt dysphoria and may present with disruptive behavior. Increased appetite and hypersomnia are more common in children and adolescents than in adults, though similar to adults, substance abuse may occur as a self-medicating response. Apathy, social withdrawal, and anhedonia are also notable symptoms that may reflect the presence of depression.
It Is OK to Use an Antidepressant for Depression
Neurologists may be reticent to prescribe antidepressants, especially in pediatrics, but this hesitation may be unfounded. Studies have consistently demonstrated the safety and effective management of anxiety and depression in primary care settings. 27,28 Neurologists tend to spend nearly as much time in office visits as many psychiatrists, and typically build very strong rapport with patients. Studies in adults have shown that patients want their neurologists to be involved in treating depression, if not actually prescribing the antidepressants. 28
In children with depression but without epilepsy, the best evidence is for fluoxetine and sertraline. Open-label trials of fluoxetine and sertraline showed improvement without adverse effects on seizures. 29 In the STAR*D study, citalopram was used in treating patients with depression in both primary and psychiatric care and showed similar success rates. 30 The United States Food and Drug Administration pediatric indications are in place for fluoxetine (major depression), sertraline and fluvoxamine (obsessive compulsive disorder), and escitalopram (major depression in adolescents). Note that fluoxetine and sertraline are typically more activating or energizing medicines, and citalopram and escitalopram tend to be more sedating. Starting with low dosages is necessary as side effects like nausea or restlessness may appear first and mood benefits may require 2 to 4 weeks to be apparent. Stepwise approaches are reasonable and well outlined in recent publications. 31
Anti-Seizure Medicines Are Powerful Tools
Even if neurologists are uncomfortable prescribing antidepressants, they may be reassured that the familiar territory of anti-seizure medications (ASMs) have wide ranging efficacy for psychiatric conditions. Although side effects may limit utility, most of the time, even adjunctive use of ASMs may be very beneficial for neuropsychiatric comorbidity. Selecting ASMs with neuropsychiatric targets in mind, in addition to seizure targets, is rapidly becoming the standard of care. Certain ASMs have been identified for their dual therapeutic roles. Carbamazepine, divalproex sodium, lamotrigine, and oxcarbazepine have shown promise in managing bipolar spectrum disorders in pediatric epilepsy cases. 32 Other examples of “dual role” medicines may include clobazam, 33 lacosamide, 34 and cannabidiol. 35,36 Temporal lobe seizure foci are often associated with depression. 20,37 Thus, using an ASM that may also have benefits for treating depression, such as lamotrigine, may be an intuitive choice for treatment in those patients. 38,39
Stimulants May Have a Favorable Risk Benefit Profile
Stimulant medications are increasingly being recognized for their potential benefits in managing ADHD symptoms in children with epilepsy. The concurrent presentation of epilepsy and ADHD complicates clinical management, yet stimulants, particularly methylphenidate, have been shown to offer a favorable risk–benefit profile and are generally considered safe for use in most pediatric epilepsy cases. A growing consensus is that methylphenidate usage in persons with a seizure frequency of less than once a month confers no additional seizure risk. 40 -42 The evidence base is robust for methylphenidate, where response rates range between 65% and 83%. 43 -46
Ecosystem of Care
The comprehensive management of childhood epilepsy includes nonpharmacological strategies to address associated neuropsychiatric symptoms. Psychotherapy, particularly cognitive behavioral therapy, plays a critical role in supporting psychological well-being, providing a confidential space for emotional and behavioral adjustment. 47,48 Emotional regulation is fostered by developing a nuanced emotional lexicon, which may be crucial for children to express their emotional states. A strong therapeutic alliance, built on trust and understanding, is essential for treatment success. Family-centered care is central to any therapeutic approach in pediatrics. Offering education and emotional support to caregivers and reinforcing their role in helping to manage their child’s epilepsy enhances the therapeutic process and promotes effective communication between the clinical team and the family. Structured living environments, routine schedules, nutritional guidance, and sleep hygiene are also key strategies for stress reduction and stability.
A commitment to a comprehensive evaluation should be the first step in developing an integrated treatment plan that may effectively blend clinical, neurophysiological, and psychological assessments. Service delivery models for specialized epilepsy centers should prioritize integrated care that facilitates collaboration among neurologists, psychiatrists, psychologists, and other professionals that are involved in the child’s daily living. 49 A network of care is essential to support patients and families who are trying to improve their wellness. That network includes not only clinicians but support from other patients and families and advocacy organizations like the Epilepsy Foundation (www.epilepsy.com). An algorithmic approach is outlined in Figure 1.
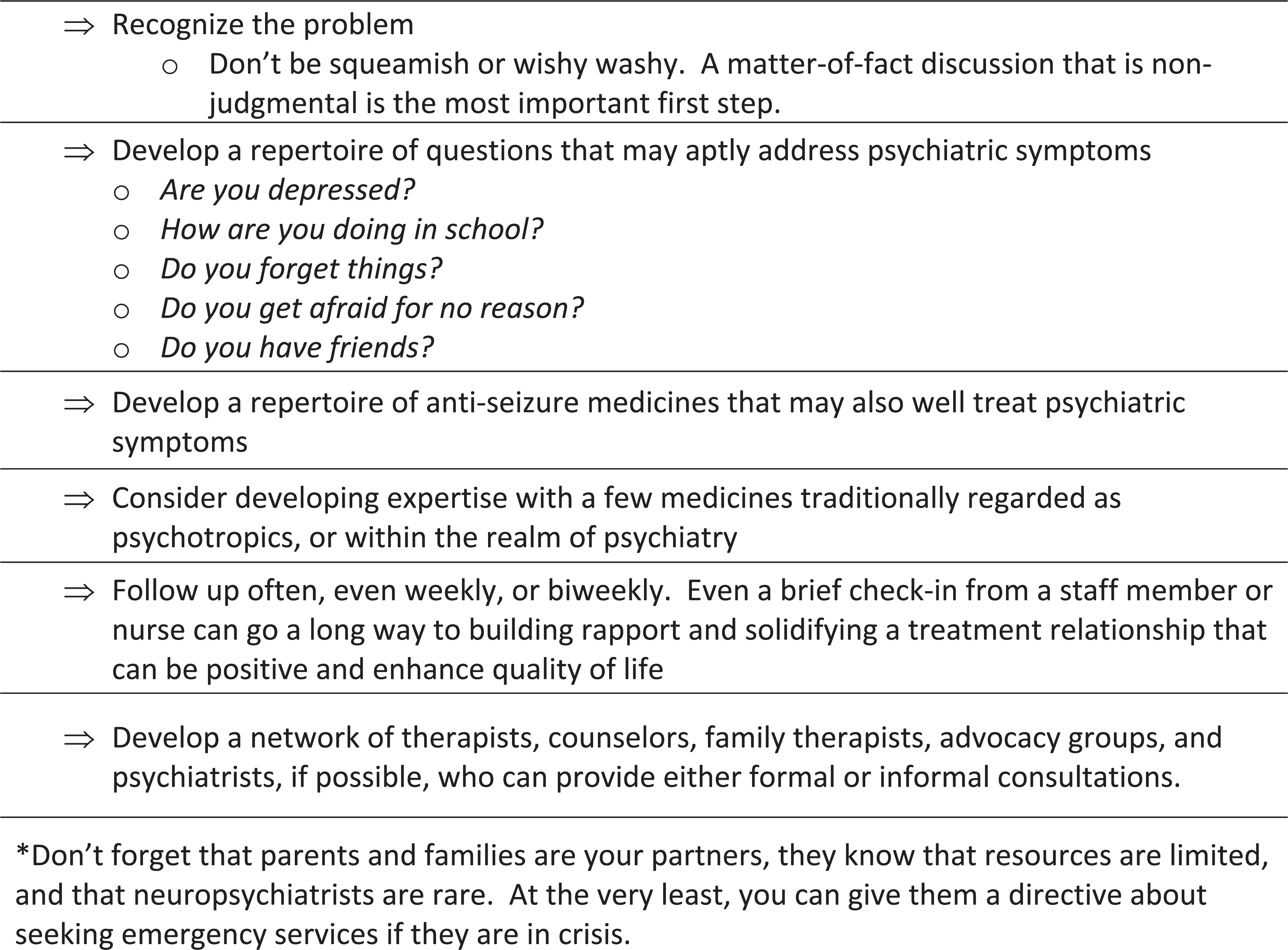
How to provide comprehensive care.
Conclusion
Pediatric epilepsy and its commonly associated neuropsychiatric symptoms demand a nuanced understanding that bridges neurology and psychiatry. A comprehensive framework is necessary to address the complex clinical needs of these patients. By adopting an integrated treatment approach that considers neurodevelopmental trajectories and the intersecting paths of neurodevelopmental disorders and epilepsy, clinicians can offer more effective and holistic care.
Footnotes
Author Contributions
JAS was involved in conceptualization, writing, editing, and review of the final draft. DDE was involved in writing, editing, and review of the final draft.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.