
Abstract
There is a paucity of information to rely on when caring for transgender and gender diverse (TGD) individuals with epilepsy. Clinicians must be aware of the mechanisms of antiseizure medications, potential unique side effects, and medication interactions that require monitoring. This principle is central to the clinical care of the TGD population, specifically for those pursuing gender-affirming care via hormone treatment and/or surgical interventions. This resource aims to support the delivery of quality healthcare with a comprehensive approach for TGD individuals living with epilepsy. This article discusses diverse topics, including antiseizure medications, drug–drug interactions, surgical and neuromodulation techniques, as well as general considerations for managing complex cases of medication-resistant epilepsy in TGD individuals. It also aims to make neurologists familiar with the basics of medical and surgical care for the same population and highlight potential reciprocal effects between comprehensive gender-affirming and epilepsy care.
Keywords
Introduction
Transgender and gender diverse (TGD) is a term which describe people whose gender identity differs from the biological sex they were assigned at birth. 1 Recent research conservatively estimates that up to 5.1% of adults ages 18 to 29 are transgender or nonbinary, with 2.0% who are a transgender man or transgender woman and 3.0% who are nonbinary. 1 TGD individuals often encounter discrimination and stigma, even within healthcare settings, which may be fueled by implicit or explicit biases.2–5 Lack of knowledge about best practices in TGD healthcare can result in suboptimal care and avoidance of healthcare by TGD individuals, jeopardizing their health and wellbeing.3,4 To mitigate these issues, it is imperative to establish welcoming, safe, and non-judgmental healthcare environments. 2
Gender dysphoria, characterized by clinical distress from the incongruence between gender identity and sex assigned at birth, is a common experience for TGD individuals. 6 Gender-affirming treatments, like hormone therapy and surgical treatments can help reduce dysphoria for TGD individuals. These treatments have shown to be effective, improve quality of life, and emotional health2,6
Given these considerations, it is crucial for clinicians to ensure proficiency in caring for TGD individuals. This review serves as a guide for providers treating TGD individuals with epilepsy, offering insights into the bidirectional effects of treatments and essential considerations specific to TGD individuals. By acknowledging and addressing the unique needs and experiences of TGD patients, healthcare providers can deliver more inclusive and effective care.
The prevalence of TGD individuals with epilepsy is undefined due to poor documentation of gender identity in electronic health records and research registries, potentially stemming from clinicians’ failure to inquire or a patient's discomfort disclosing this information. Although the precise number of TGD individuals living with epilepsy is unknown, the prevalence of epilepsy among TGD people receiving Medicare is 10.5%, which exceeds that of cisgender individuals.7–9 With limited peer-reviewed literature studying the intersection of epilepsy and gender-affirming care (GAC), clinicians are ill prepared to serve a significant portion of the population, underscoring a knowledge gap in the field. To bridge this gap, this paper extrapolates from existing knowledge of antiseizure medications (ASMs) and endogenous/exogenous hormonal interactions, along with the known pharmacologic interactions between ASMs and hepatic cytochrome P450 enzymes. Additionally, this paper provides suggestions for perioperative care of TGD patients with medication-resistant epilepsy (MRE) who may undergo surgical and medical interventions for both their epilepsy and GAC.
Methods
This article is a narrative review of current best practices in treating transgender patients, including the application of current standards in epilepsy care. Literature reviewed was limited to published primary research, review articles, and textbooks written in English, inclusive of years 2000 to 2023 and indexed in PubMed. We excluded non–peer-reviewed articles and those in non-English languages. Relevant patient care guidelines and online publications were included when representing primary source material.
Gender-Affirming Care: Medical Management and Surgical Procedures
Gender-Affirming Hormone Therapy
TGD individuals seeking gender-affirming hormone therapy (GAHT) require a personalized approach to care, considering their transition goals, age, comorbidities, and treatment preferences. 6 Some TGD individuals seek GAHT for masculinization or feminization of the body to help relieve their gender dysphoria.
For TGD adolescents in early puberty, gonadotropin-releasing hormone (GnRH) analogs are often used to suppress gonadotropin levels and pause puberty.5,6 GnRH analogs, also known as puberty blockers, are reversible and allow for resumption of puberty if discontinued. 10 GnRH analogs are administered as injections every 1–6 months or as an implant that can be replaced yearly.6,10
In late or post puberty, treatment can be initiated directly with GAHT. 6 For transfeminine individuals, feminizing hormone therapy includes the use of 17-β-estradiol and an antiandrogen, like spironolactone or cyproterone acetate.6,11 Spironolactone is the most used antiandrogen in the United States and acts in peripheral tissues as an androgen antagonist. 12 Cyproterone acetate, a progesterone derivative, is commonly used as an antiandrogen in Europe. 11 GnRH analogs may be used as an antiandrogen because they also suppress gonadotropins; these are typically administered as injections or implants.5,6 Finasteride, a 5 α-reductase inhibitor, may also be used as an antiandrogen but it does not decrease testosterone levels and has potential adverse effects. 13 The feminizing effects of estradiol begin within a few months of treatment and continue to develop until they plateau at 3 to 5 years. 6 For full feminization, the estradiol target is 100 to 200 pg/mL and the goal for testosterone is <55 ng/dL. 6 Transfeminine individuals may use progesterone for breast development and mood benefit, but there is limited evidence for its use as a standard part of GAHT.5,14
For transmasculine people, testosterone is used for masculinization and can be prescribed as a subcutaneous or intramuscular injection (administered every 7–14 days) or in its gel form.6,15,16 Masculinization typically begins within the first few months of treatment and continues for several years.6,15 For those using testosterone for full masculinization, the goal testosterone level at the midpoint between injections is 400 to 700 ng/dL. 6
Laboratory testing may be used to monitor hormone levels and guide dose adjustments for TGD people with epilepsy to achieve individual transition goals. 6 Values, doses, and clinical goals may differ in nonbinary people pursuing an androgynous or ambiguous presentation. There are no absolute contraindications to GAHT, and though there are potential risks, most are rare and can be mitigated with close monitoring and dose adjustment.
Gender-Affirming Surgical Procedures
Many TGD individuals, but not all, may pursue various surgical procedures with transition, like chest reconstruction, breast augmentation, bilateral mastectomy, hysterectomy, phalloplasty, metoidioplasty, and vaginoplasty.5,17 Neurologists must be at least aware of these to provide compatible care.
Transmasculine individuals may seek chest reconstruction including bilateral mastectomy and the creation of a masculine-appearing chest. 18 Breast growth with transfeminine individuals on GAHT is variable and some may seek breast augmentation procedures.
Facial and neck procedures can be performed, including masculinization of the thyroid cartilage or thyroid cartilage minimization, rhinoplasty, facial feminization, and other procedures of the hairline and forehead.add reference.19–21
Impact of ASMs on Gender-Affirming Hormone Treatments
While ASMs have the potential to impact a variety of drug metabolic enzymes as well as transport proteins, most of the current literature to date utilizes data extrapolated from oral contraceptive and hormone replacement therapy studies. 22 Some pharmacokinetic interactions between hormone treatments and ASMs may be bidirectional. Clinicians must anticipate potential interactions between hormone therapies and commonly used ASMs. The following statements were derived from extensive literature search encompassing use of the Summary of Antiseizure Medications Available in the United States: 4th Edition, FDA-approved prescribing information to ensure all metabolism pathways are accounted for and listed, plus supplementation with data from Lexicomp whenever information was not available from the above. 23
ASMs that induce or inhibit various cytochrome P450 isozymes (CYP) and the UDP-glucuronyltransferase (UGT) isozyme systems can markedly alter the bioavailability and apparent oral clearance of commonly used non-epilepsy medications, including sex hormones, antiretrovirals, and various psychotropics.24,25 While enzyme induction or inhibition is predictable, the actual clinical impact of these pharmacokinetic interactions is sometimes not as straightforward. 26
As discussed above, the majority of TGD adults on GAHT will receive hormone therapy with either a 17-β-estradiol or testosterone formulation and may receive adjunctive treatment with androgen-suppressing drugs such as spironolactone or cyproterone.27,28 Both testosterone and estradiol are extensively metabolized via CYP isozymes, the bioactive fractions of both hormones are dependent on binding to both albumin and sex hormone binding globulin (SHBG). 28 CYP3A4 metabolizes about 80% of exogenously administered testosterone. CYPs 2C19, 2C9 and 2B6 also contribute. Estradiol is also primarily metabolized via CYP3A4, as well as CYP1A2, 2B6, 2C9, 2C19 and 2D6. UGT1A1 also contributes. Enzyme-inducing ASMs (EIASM) (Table 1) are expected to reduce plasma concentrations of both estradiol and testosterone. Agents like finasteride, which is also a substrate of CYP3A4/5, are expected to have reduced activity in patients receiving concomitant EIASMs. In addition to induction of metabolic enzyme activity, EIASMs can increase the plasma concentration of SHBG, and can decrease the bioactive fraction of both hormones. 29 Clinically, this may warrant monitoring of unbound testosterone concentrations in individuals receiving concomitant treatment with an EIASM. This should be a collaborative effort, led by the clinician leading GAC management.
Drug Interactions Between ASMs and GAHTs.
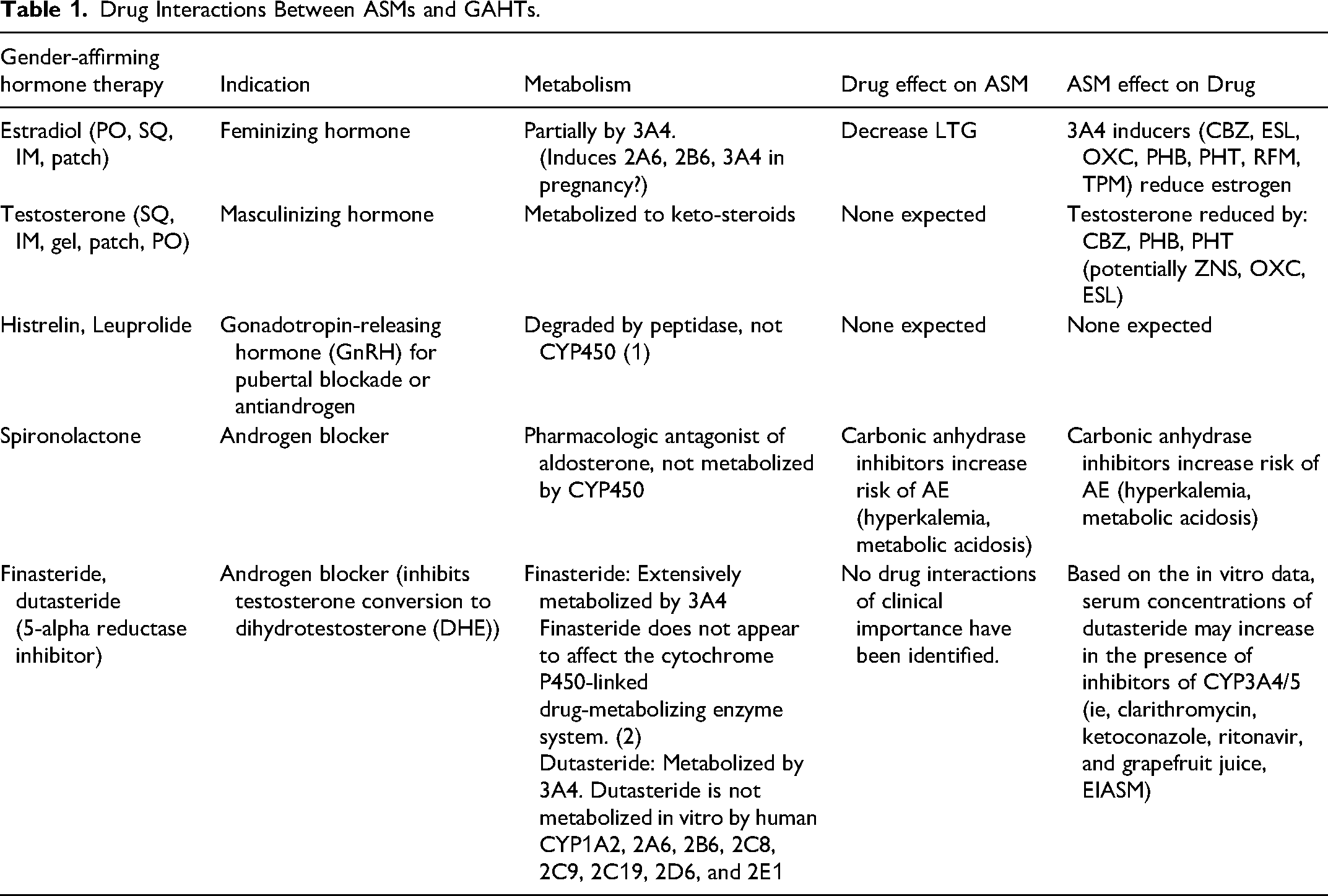
Valproic acid (VPA) has been reported to increase androgen concentrations in patients with epilepsy. 30 The mechanism for this apparent interaction may involve VPA interference with hormonal feedback mechanisms (LH, FSH secretion) as well as potentially hormonal metabolism. While CYP3A4 appears to be most important in testosterone metabolism, UGT isozymes UGT2B7, UGT2B15 and UGT2B17 also participate. 31
Spironolactone undergoes hepatic metabolism to several active metabolites, however, this bioactivation does not appear to be dependent upon the CYP isozyme system, so interactions with current ASMs would not be predicted.
Impact of Hormone Treatment on ASM Pharmacokinetics
With respect to drug metabolism, it must be recognized that specific CYP/UGT studies in patients receiving GAC are lacking. Although GAHT may impact body composition (fat/lean muscle mass), it is unclear whether this results in meaningful changes in drug pharmacokinetics. 32
The effect of testosterone on CYP1A2, 2C9, 2C19 or 2D6 has not been directly evaluated. Exogenous estrogen does not appear to influence the activity of CYP2C9 or 2D6. 33 Conversely, there are data to suggest that CYP2B6 activity may be induced by high-dose estrogen treatment. 28 Similarly, induction of several UGT isozymes by estrogen (UGT1A1,1A4) have been noted. This is likely the explanation for the decrease in lamotrigine plasma concentration seen with oral contraceptives. 34
Although estrogen given as hormone replacement treatment does not appear to alter CYP3A4— mediated clearance of the substrate midazolam in in vitro experiments attempting to understand the mechanism of pregnancy-associated increases in CYP3A4 activity do suggest a role for estrogen as an inducer.35,36
In addition to the documented effect of exogenous ethinyl estradiol on lamotrigine clearance, data from pregnant patients demonstrate that the serum levels of both total and unbound lamotrigine are also reduced with increasing estrogen concentrations during pregnancy (both E2 and E3). This further supports the notion that estrogen can impact lamotrigine pharmacokinetics. In a retrospective analysis of claims, around 25% of cisgender women who took exogenous estrogen through estrogen-containing oral contraceptives or hormone replacement therapy had an increase in their lamotrigine dosage within the first year of starting exogenous estrogen. 37 While transfeminine individuals were excluded from that study, monitoring lamotrigine levels before and after initiating exogenous estrogen as part of GAC may help inform necessary dose adjustments.
Finally, many ASMs are eliminated, at least in part, via glomerular filtration. Based upon the limited data available, it does not appear that exogenous hormones should be anticipated to result in direct, independent changes in filtration. It is recognized that pregnancy can result in increases in the activities of transport proteins OAT1, OAT2 and p-glycoprotein, as well as GFR. 38 Therefore, while changes are unlikely in TGD adults, it is still uncertain and worthy of further investigation (Table 2).
ASM Metabolism.
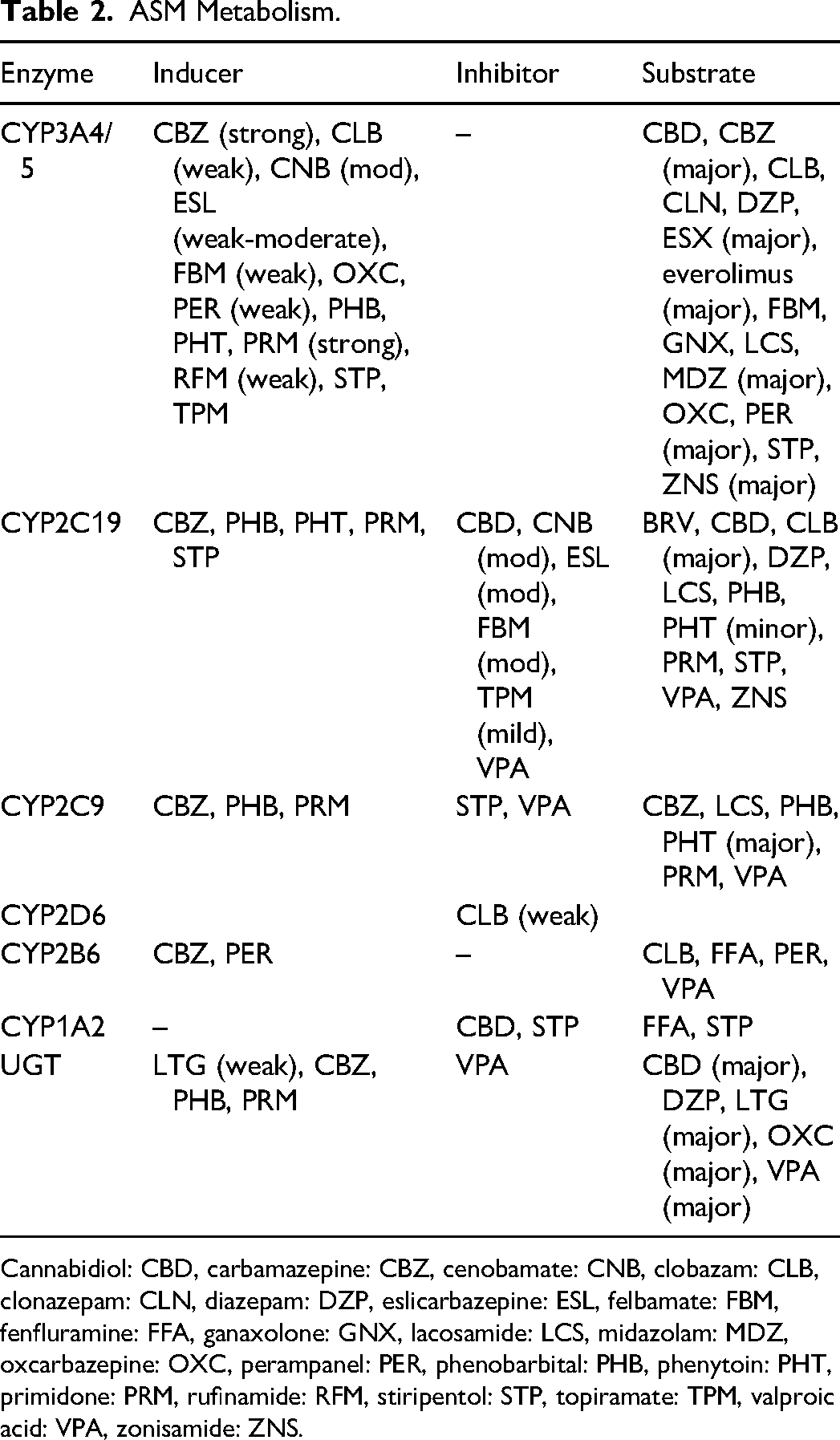
Cannabidiol: CBD, carbamazepine: CBZ, cenobamate: CNB, clobazam: CLB, clonazepam: CLN, diazepam: DZP, eslicarbazepine: ESL, felbamate: FBM, fenfluramine: FFA, ganaxolone: GNX, lacosamide: LCS, midazolam: MDZ, oxcarbazepine: OXC, perampanel: PER, phenobarbital: PHB, phenytoin: PHT, primidone: PRM, rufinamide: RFM, stiripentol: STP, topiramate: TPM, valproic acid: VPA, zonisamide: ZNS.
Bidirectional Medication Interactions Between ASMs and GAHTs
Epilepsy Surgery and Other Surgical Concerns for TGD Individuals
Epilepsy surgery should always be considered for TGD individuals with MRE. This entails balancing GAHT, gender-affirming surgeries, and epilepsy surgery. Due to current limited information, data from presumed cisgender patients undergoing hormone treatments and TGD individuals without epilepsy has been used to guide the subsequent clinical considerations. This section includes discussion of hormone therapy interactions with surgery and epilepsy surgery considerations specific to TGD patients.
Epilepsy Surgery
Considerations for TGD individuals who are epilepsy surgical candidates include potential effects of medications commonly used for GAC on surgical interventions and modifications depending on epilepsy surgical procedure planned. Surgical interventions and modifications for all patients include any variation of intracranial electrode placement for presurgical video-EEG monitoring (stereo-encephalography, subdural evaluation with grids and strips (SDE), or depth electrodes), laser interstitial thermal therapy (LITT), standard cortical resections, lesionectomies, disconnection procedures, neuromodulator placement, or any combination of the above. Considerations for implantation of neuromodulation devices vary between those implanted intracranially/cranially versus those implanted in the chest.
Potential Effects of Medications Commonly Used for GAC on Epilepsy Surgical Interventions
Transfeminine individuals on estradiol undergoing anesthesia face a theoretical increased risk of thrombosis.39,40 While ethinyl estradiol carriers a higher risk of venous thromboembolism (VTE), this is not typically used for TGD individuals. 40 Previously, holding estradiol before surgery was recommended but is no longer advised due to potential negative impacts on mental health and quality of life. 41 Longer durations of estradiol interruption, especially for sequential procedures, can exacerbate gender dysphoria and mood issues. The risks of undergoing surgery while continuing estradiol are low if there are no other added risks (e.g., smoking, hypertension, hypercholesterolemia, clotting disorders). In an individual with non-reversible risk factors for clotting, holding of estrogen for a longer procedure and period of immobilization may be warranted, although this has not been studied in clinical trials. Additionally, appropriate VTE prophylaxis is essential for all surgeries involving extended immobility, like intracranial implantation and subsequent epilepsy monitoring unit (EMU) admission.
The use of GnRH agonists should be considered when planning epilepsy surgery. Leuprolide has rarely been associated with acute mania and psychiatric symptoms.42–44 Individuals on GnRH agonists should be monitored for this possibility until there is more data. Additionally, limited studies have shown that deep brain stimulators (DBS) targeting the anterior nucleus of the thalamus (ANT) can worsen depression or contribute to psychosis. 45 Considering the limited data available, precaution for DBS placement is recommended in cases of severe mood issues, mirroring the recommendation for cisgender individuals. Caution should be taken with any combination of DBS, GnRH, or ASMs which may additively exacerbate mental health problems. No significant effects relating to surgery exist for spironolactone.
For transmasculine individuals, testosterone usage is a crucial consideration. Its use has been linked to polycythemia, particularly within the first year of use, which heightens the risk of blood clots due to increased hemoglobin and hematocrit (H/H) levels. 46 If H/H levels are not significantly elevated, the risk is comparable to that of cisgender individuals not on testosterone. While delaying procedures until after the first year of testosterone initiation may mitigate risk, it may not be feasible depending on epilepsy severity. The association between testosterone and VTE risk remains unclear, with conflicting data from studies that predominantly involve cisgender men. As of this publication, testosterone use should not be presumed to increase the risk of VTE.47,48
LITT carries low risks. 41 This minimally invasive procedure is short, involves minimal bleeding, and does not require prolonged immobility, compared to more extensive open surgeries. For extended EMU monitoring, early mobility should be prioritized, supported by physical therapy, and complemented using sequential compression devices and compression/anti-embolism stockings. This proactive approach to mobility and circulatory support is advised for any of the surgeries discussed herein.
Neuromodulation Restricted to Skull-Implanted Devices (Responsive Neurostimulation [RNS] System)
RNS is typically not affected by hormone treatments. If gender-affirming surgeries have been completed, there are no additional concerns. However, if RNS is already implanted and gender-affirming surgery is later pursued, standard precautions for any surgery below the head should be followed. While the RNS device does not need to be turned off during surgery, it is recommended as a precaution that it be turned off for surgery and back on after, with parameters checked at that time. 49
Neuromodulation Including Chest-Implanted Devices (Vagus Nerve Stimulator [VNS] and Intracranial/Chest Portion Deep Brain Stimulators [DBS])
If gender-affirming surgeries have been completed, there is no concern. If chest modification or breast augmentation surgery has not been completed (but may be considered in the future), placement of the VNS or DBS chest portion in the back may be considered.
If a VNS has already been placed and surgery within the upper body and near the device (breast/chest surgery on left) will be performed, the VNS should be turned off prior to surgery and turned back on and checked after the surgery is completed. If the surgery is lower in the body (away from the VNS implant) it does not need to be turned off but should be interrogated after the surgery to ensure proper functioning. Use of a magnet in the vicinity of the VNS, if off, is not problematic (breast tissue expanders with a magnetic injection port are not anticipated to be problematic). 50 Electrosurgery should be done as far from the generator and lead system as possible as it may damage the generator; the VNS should be checked after surgery to ensure normal functioning. 51
If undergoing gender-affirming surgery after DBS implantation, DBS should be turned off prior to surgery and back on afterwards. This can be done by the patient using their programmer and verified by the care team. 51 Bipolar electrosurgery is preferred, but if needed, monopolar cautery can be used on the lowest power setting possible, with the grounding pad as far away as possible (usually the opposite leg to the device). If there is any seizure worsening post-procedure the DBS should be interrogated to ensure proper functioning. Temporarily disabling any of these FDA-approved neuromodulation devices for surgery should not be detrimental for individual seizure control as these devices work by modulating brain networks over months to years. 52
While modern chest-implanted neuromodulation devices are considered MRI compatible for MR imaging of the brain, there are regions of the body that will be unable to have MRI imaging after VNS or DBS placement. Even when the device is off, MR pulses directly over the battery and programmer portion of the devices, also called the “can,” are contraindicated. This can preclude MR imaging of the chest directly. Therefore, if MR imaging is anticipated for evaluation of peri-surgical complications or long-term care of a TGD individual, then VNS or DBS may not be an ideal choice.
Neuropsychiatry of Epilepsy in TGD Individuals
Psychiatric comorbidity is more prevalent in those with MRE.53–55 Irrespective of epilepsy type, TGD individuals are more than twice as likely to receive a psychiatric diagnosis than cisgender individuals. 56 The odds of depression, anxiety, and psychotic disorders are higher in TGD patients admitted to the hospital, with self-injurious behaviors and completed suicide rates 13 times that of cisgender patients.56,57 Trauma and stress-related disorders, eating disorders, and substance use disorders are also elevated.57–63 These rates of psychiatric disorders are believed to be in part a consequence of the multifactorial interaction between social stigma, discrimination, trauma, and the collective weight of pervasive stress in TGD people. 64 GAC, including surgery, has been associated with long-term reduction in these mental health comorbidities. 5
More data on the intersection of TGD individuals’ mental health and epilepsy could help shed light on predisposing vulnerabilities, mechanisms, and potential interventions to improve symptom management, quality of life, and other significant psychosocial outcome measures. To underscore the imperative need for further research, both the general population living with epilepsy and the TGD population without epilepsy are independently at heightened risk for suicide. In people living with epilepsy, completed suicide may account for as much as 12% of all deaths, with over 23% experiencing suicidal ideation.65,66 At least one study suggests patients with temporal lobe epilepsy are at markedly increased risk for suicide compared to those with extratemporal epilepsy and the general population. 67 How the interaction between TGD identity and epilepsy may contribute to the cumulative risk for psychiatric conditions, including suicidal behaviors, has yet to be fully understood. The theoretical compounding effects of marginalization and stigma associated with TGD identity and that of epilepsy remain a significant factor. 68
As part of a comprehensive care approach, individuals with epilepsy should be routinely screened for psychiatric comorbidities and receive appropriate referrals to mental health services. This is especially important in vulnerable populations such as the TGD community. Ideally, mental health clinicians would be integrated into epilepsy teams to readily provide consultation to colleagues, evaluate patients, and assist in triaging patients to appropriate psychiatric care. Certain ASMs may have a higher propensity for mood complications, like levetiracetam, while others prove to be more beneficial for mood or anxiety, in particular VPA, lamotrigine, carbamazepine, oxcarbazepine, eslicarbazepine, and clobazam.69,70 When treatments reach beyond first- and second-line measures, psychiatrists are essential in considering more complex evidence-based psychopharmacology or nonpharmacologic interventions (e.g., electroconvulsive therapy). The clinician should give thought to side effect profiles of certain psychotropics (e.g., hyperprolactinemia and resultant gynecomastia or serotonergic agents and sexual side effects), as these may exacerbate depression and anxiety. 71 At the heart of any psychiatric assessment is a biopsychosocial formulation – a framework helping the clinician best approximate the patient's experience through not only a biological lens, but through the perspectives of their psychology and sociocultural narrative.72 Additionally, a comprehensive assessment of potential drug–drug interactions (DDI) between GAHT, ASMs, and antidepressants/antipsychotic agents should be performed. When possible, TGD people with seizures should be referred to gender-affirming psychotherapy providers. Local gender-affirming psychotherapists and other healthcare providers can be found on the provider directory housed by the World Professional Association for Transgender Health 73 and GLMA: Health Professionals Advancing LGBTQ Equality. 74
Healthcare Avoidance and Non-Affirming Environments
Adherence to ASMs and epilepsy surgery for suitable candidates can improve clinical outcomes and quality of life.75,76 Studies indicate there is healthcare avoidance in TGD individuals due to perceived and anticipated discrimination. 77 Given the rates of general medical non-adherence and the importance of patient–provider interactions in epilepsy surgery workups and treatment, research is needed to better understand factors which may contribute to a better therapeutic alliance beyond baseline safe, welcoming healthcare environments for TGD individuals. Without safe and affirming healthcare, avoidance persists, leading to poor treatment adherence. By fostering open communication and collaboration, health care providers can ensure the patient's overall health and safety, including providing effective epilepsy management. There are numerous online resources to ensure clinicians and staff are well-versed in fomenting inclusive healthcare spaces, one being The Fenway Institute—The National LGBT Health Education Center. 78 Additionally, involvement of pharmacists beyond roles in management of pharmacokinetic interactions, with increased input in the individualization of complex medication regimens and supporting patient-focused medication education may help with overall medical adherence. 79
Conclusion
This work represents a compilation of information on the care of TGD individuals with epilepsy, specifically delving into the complex medical care of MRE and comorbidities in this heterogeneous population. It can serve as a valuable starting point for the development of new knowledge in this field and as an initial reference for practitioners who may not be fully acquainted with the intricacies involved in caring for TGD individuals. It is important to acknowledge the scarcity of information within the medical community, such as pregnancy in TGD persons, and real-world data of the natural history of epilepsy in those with MRE undergoing GAC. Suggestions have been derived from currently available information on related clinical management issues. There is a pressing need for more research in this field to address gaps in knowledge. There should also be increased education to ensure that providers are adequately equipped with the knowledge to deliver quality care to all segments of the epilepsy population. Given the dearth of information about TGD patients with epilepsy, additional research is warranted and comprehensive, multidisciplinary teams including professionals well-versed in GAC are needed to provide patients with the highest level of care.
Footnotes
Acknowledgments
The authors undertook this effort as representatives of the Treatments Committee of the American Epilepsy Society. This publication underscores the commitment of the American Epilepsy Society, the Council on Clinical Activities, and its committees to advancing patient care, promoting education, and fostering innovation within the epilepsy community. The authors thank Dr Lara Marcuse for participating in the initial concept drafting meeting and Lauren Orciuoli for facilitating meetings, overseeing progress, and assisting with references. Finally, the authors acknowledge TGD individuals living with epilepsy, many of whom have left an indelible impact on our lives and humanity (AI).
Author Contributions
Dr Alick-Lindstrom formulated the concept for this manuscript, functioned as primary writer for initial draft and all edits, created the multidisciplinary group of authors, and provided epilepsy expertise. Dr Kerr participated in editing. Dr Weingarten and Dr Gidal provided specialty information on the pharmacology aspects and DDI. Dr Falco-Walter assisted with writing and editing and provided epilepsy expertise. Dr Lane provided neuropsychiatry expertise. Dr L’Erario assisted in writing about FND, editing, verifying content accuracy, neurology expertise, and knowledge as a LMSW. Dr Abramowitz provided expertise on GAC as an endocrinologist and assisted in writing and editing. Dr Zeigler provided neurology expertise, and assisted in writing, editing, and verifying content accuracy.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Dr Alick-Lindstrom has performed consultancy work in magnetoencephalography and magnetic source imaging in epilepsy for MEGIN. Dr Kerr is a paid consultant for SK Life Sciences, Biohaven, Jazz Pharmaceuticals, and has collaborative or data use agreements with Eisai, Janssen, Radius Health, UCB, GlaxoSmithKline, Neureka, and Praxis. Dr Weingarten is employed by SK Life Science.Dr Gidal has received honoraria from SK Lifescience, Jazz, and Neurelis. Dr Falco-Walter, Dr Abramowitz, Dr Lane, Dr Zeigler, and Dr L’Erario have no relevant disclosures.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.