
Abstract
Purpose:
Established tonic–clonic status epilepticus (SE) does not stop in one-third of patients when treated with an intravenous (IV) benzodiazepine bolus followed by a loading dose of a second antiseizure medication (ASM). These patients have refractory status epilepticus (RSE) and a high risk of morbidity and death. For patients with convulsive refractory status epilepticus (CRSE), we sought to determine the strength of evidence for 8 parenteral ASMs used as third-line treatment in stopping clinical CRSE.
Methods:
A structured literature search (MEDLINE, Embase, CENTRAL, CINAHL) was performed to identify original studies on the treatment of CRSE in children and adults using IV brivaracetam, ketamine, lacosamide, levetiracetam (LEV), midazolam (MDZ), pentobarbital (PTB; and thiopental), propofol (PRO), and valproic acid (VPA). Adrenocorticotropic hormone (ACTH), corticosteroids, intravenous immunoglobulin (IVIg), magnesium sulfate, and pyridoxine were added to determine the effectiveness in treating hard-to-control seizures in special circumstances. Studies were evaluated by predefined criteria and were classified by strength of evidence in stopping clinical CRSE (either as the last ASM added or compared to another ASM) according to the 2017 American Academy of Neurology process.
Results:
No studies exist on the use of ACTH, corticosteroids, or IVIg for the treatment of CRSE. Small series and case reports exist on the use of these agents in the treatment of RSE of suspected immune etiology, severe epileptic encephalopathies, and rare epilepsy syndromes. For adults with CRSE, insufficient evidence exists on the effectiveness of brivaracetam (level U; 4 class IV studies). For children and adults with CRSE, insufficient evidence exists on the effectiveness of ketamine (level U; 25 class IV studies). For children and adults with CRSE, it is possible that lacosamide is effective at stopping RSE (level C; 2 class III, 14 class IV studies). For children with CRSE, insufficient evidence exists that LEV and VPA are equally effective (level U, 1 class III study). For adults with CRSE, insufficient evidence exists to support the effectiveness of LEV (level U; 2 class IV studies). Magnesium sulfate may be effective in the treatment of eclampsia, but there are only case reports of its use for CRSE. For children with CRSE, insufficient evidence exists to support either that MDZ and diazepam infusions are equally effective (level U; 1 class III study) or that MDZ infusion and PTB are equally effective (level U; 1 class III study). For adults with CRSE, insufficient evidence exists to support either that MDZ infusion and PRO are equally effective (level U; 1 class III study) or that low-dose and high-dose MDZ infusions are equally effective (level U; 1 class III study). For children and adults with CRSE, insufficient evidence exists to support that MDZ is effective as the last drug added (level U; 29 class IV studies). For adults with CRSE, insufficient evidence exists to support that PTB and PRO are equally effective (level U; 1 class III study). For adults and children with CRSE, insufficient evidence exists to support that PTB is effective as the last ASM added (level U; 42 class IV studies). For CRSE, insufficient evidence exists to support that PRO is effective as the last ASM used (level U; 26 class IV studies). No pediatric-only studies exist on the use of PRO for CRSE, and many guidelines do not recommend its use in children aged <16 years. Pyridoxine-dependent and pyridoxine-responsive epilepsies should be considered in children presenting between birth and age 3 years with refractory seizures and no imaging lesion or other acquired cause of seizures. For children with CRSE, insufficient evidence exists that VPA and diazepam infusion are equally effective (level U, 1 class III study). No class I to III studies have been reported in adults treated with VPA for CRSE. In comparison, for children and adults with established convulsive SE (ie, not RSE), after an initial benzodiazepine, it is likely that loading doses of LEV 60 mg/kg, VPA 40 mg/kg, and fosphenytoin 20 mg PE/kg are equally effective at stopping SE (level B, 1 class I study).
Conclusions:
Mostly insufficient evidence exists on the efficacy of stopping clinical CRSE using brivaracetam, lacosamide, LEV, valproate, ketamine, MDZ, PTB, and PRO either as the last ASM or compared to others of these drugs. Adrenocorticotropic hormone, IVIg, corticosteroids, magnesium sulfate, and pyridoxine have been used in special situations but have not been studied for CRSE. For the treatment of established convulsive SE (ie, not RSE), LEV, VPA, and fosphenytoin are likely equally effective, but whether this is also true for CRSE is unknown. Triple-masked, randomized controlled trials are needed to compare the effectiveness of parenteral anesthetizing and nonanesthetizing ASMs in the treatment of CRSE.
Keywords
Introduction
Convulsive status epilepticus (CSE) is a medical emergency defined as a tonic–clonic convulsion lasting >5 minutes or repeated convulsions. 1 Older guidelines for the treatment of established CSE 2 have been replaced with evidence-based guidelines. 3 -5 Antiseizure medications (ASMs) recommended in the 2016 American Epilepsy Society (AES) guidelines 3 for the treatment of established CSE are first to give a bolus of intravenous (IV) lorazepam, diazepam, or phenobarbital, or intramuscular (IM) midazolam (MDZ; level A, effective), then second to give a loading dose (and then maintenance doses) of IV phenytoin (PHT) or fosphenytoin (level A, effective), valproic acid (VPA; level C, possibly effective), or levetiracetam (LEV; level U, data inadequate). In approximately one-third of patients, CSE continues despite the use of appropriate initial ASMs. Among adults with CSE, a US Veterans Administration trial showed that the first ASM worked in 55.5%, the second ASM worked in another 7.0%, and the third ASM worked in only 2.3% of patients. 6 In children, the second ASM appears less effective than the first, and there are no data about the third ASM. 3 Refractory status epilepticus (RSE) is an SE that continues despite treatment with both benzodiazepine (BDZ) and a second appropriately selected and dosed ASM. 7 Refractory status epilepticus develops in about 23% to 43% of SE patients, causes death in 17% to 39% of adults (a lower rate in children), and leads to a return to baseline neurological status in a minority and longer hospital stays and increased need for rehabilitation in many patients. 8 -12
To help avoid complications of convulsive refractory status epilepticus (CRSE), clinicians often use continuous infusions of anesthetizing ASMs such as MDZ, pentobarbital (PTB), or propofol (PRO) as third-line therapy, but concerns have been raised about their serious adverse effects (AEs). A class III study found that IV anesthetic ASM use was associated with a 3-fold relative increased risk of death and 4-fold increased incidence of infection, even when correcting for age and SE severity. 13 Another class III study of IV anesthetic ASMs found a 7-fold relative increased risk of new disability, a 9-fold increased risk of death, a 4-fold increased risk of infection, and 1 week longer hospital stays. 14 One must interpret the results of these retrospective studies cautiously because selection bias may have compromised the findings: Patients receiving anesthetizing ASMs may have been more ill and their CSE may have been more refractory. Furthermore, many treatment series do not control for ASM timing and dosing, which may potentially affect outcomes. A class III study found that the use of anesthetic ASMs (“therapeutic coma [TC]”) was much more common at 3 affiliated Boston hospitals than at a Swiss center. 15 In that large study, TC was associated with longer hospitalizations but not with increased mortality, and TC was more commonly used in patients with refractory SE, higher Status Epilepticus Scale Score (STESS), 16 and younger age. A recent retrospective observational study reported that shorter duration, yet deeper, TC was associated with fewer in-hospital complications and fewer poor outcomes. 17
Novy et al 12 reported that escalating treatment with a nonsedating ASM terminated RSE in more than half their patients. Similarly, a class III study of lorazepam followed by PHT, LEV, and VPA for CSE found that by the time all 3 were used sequentially, SE was controlled in 92% of patients and anesthetizing ASMs could be avoided. 10 This strategy may avoid the complications of a long intensive care unit (ICU) stay associated with anesthetizing ASMs. In the last several years, 4 nonsedating IV ASMs (brivaracetam [BRV], lacosamide [LCM], LEV, and VPA) have become available and have been used off-label in RSE. At this time there is no consensus on whether TC should be used after failure of a BDZ and a second ASM or whether a third nonanesthetizing ASM should be used prior to starting TC. 15
The goals of this review were firstly to identify, analyze, and grade all of the research literature on the efficacy of BRV, ketamine (KET), LCM, LEV, VPA, MDZ, PTB, and PRO at stopping CRSE and secondly to examine 5 other IV ASMs used in the treatment of special populations (eg, children, pregnant women) with hard-to-control seizures.
Methods
The AES Treatments Committee formed the Refractory Status Epilepticus Taskforce in 2012, which included a multidisciplinary team of adult neurologists, child neurologists, and neuropharmacologists. A methodologist (D.S.G.) was added in 2019 to review taskforce members’ level-of-evidence grading of included studies and to review the final manuscript. Conflict of interest was managed by ensuring that no more than one medication section author had a relationship with the manufacturer of any ASM. Selection of the topic for this systematic review was by the AES Treatments Committee, and the topics were approved by the AES Council on Clinical Activities, executives, and board of directors.
In 2016, the AES published the guideline for the initial treatment of (established) SE. 3 It focused solely on the treatment of CSE (nonconvulsive status epilepticus [NCSE] was excluded). The present review was designed to be a sequel to the AES guideline, 3 with the goal of identifying and analyzing the existing literature supporting the use of ASMs other than PHT and phenobarbital in the treatment of CRSE. It focuses on CSE because it is serious, has been the best studied, and is often clinically easier to recognize than NCSE or electrographic SE. Phenytoin and phenobarbital were excluded because they have a level A evidence rating for treating established CSE in the AES guideline. 3 The goal was to conduct a comprehensive review of the original studies on the treatment of CRSE using 4 nonanesthetizing parenteral ASMs and continuous infusions of 4 anesthetizing ASMs. Immunotherapies, pyridoxine, and magnesium sulfate (MgSO4) were added to review the evidence on the treatment of children, pregnant women, and patients with autoimmune epilepsies with refractory seizures (which do not typically result in RSE). The parenteral ASMs reviewed for this consensus statement are (in alphabetical order) adrenocorticotropic hormone (ACTH), BRV, corticosteroids, intravenous immunoglobulin (IVIg), KET, LCM, LEV, MgSO4, MDZ, PTB (and thiopental [THP]), PRO, pyridoxine, and VPA. After this review was completed, the class I Established Status Epilepticus Treatment Trial (ESETT) was published in November 2019. 18 The ESETT study involves the treatment of convulsive established SE. It is discussed in the Results section for context and for comparison with the studies on CRSE.
The previous ILAE definition of SE was, “a single epileptic seizure of >30 minutes duration or a series of epileptic seizures during which function is not regained between ictal events in a >30-minute period.” 19(593) Modern research studies often use a much shorter duration of seizures to define CSE. For this report, we use the studies’ own definitions as long as they included overt convulsions lasting >5 minutes or 2+ back-to-back tonic–clonic seizures without full return of consciousness between them. This is consistent with the modern ILAE definition. 1 The 4 stages of SE are as follows: developing: seizures leading up to SE, established: >5 minutes’ duration and therapy is initiated, refractory: failure of 2 adequately dosed ASMs in different drug classes (eg, BDZ and PHT), and super-refractory status epilepticus (SRSE): SE persisting despite >24 hours of anesthesia. 7
For each medication section, 2 to 4 authors searched bibliographic databases, identified research studies meeting the inclusion/exclusion criteria (below), and abstracted and reached consensus on the data in each study. To minimize bias, the Cochrane Handbook of Systematic Reviews of Interventions 20 guided this review. Medication section authors searched MEDLINE, Embase, CINAHL, and the Cochrane Central Register of Controlled Trials with the assistance of their own institution’s librarian. In addition, the reference lists contained in each study identified from the database searches were hand-reviewed by section authors to ensure that no pertinent studies were missed. Review articles were also searched to identify additional studies. In the database searches, both free-text words and subject terms were used. These words and terms were linked by the Boolean operators “OR” or “AND,” but the operator “NOT” was not used. Examples of free-text word searches are “lacosamide AND status epilepticus,” and “pentobarbital AND status epilepticus AND human.” A wide range of free-text terms were used including synonyms (eg, “antiepileptic drug’ OR “anticonvulsant’”), related terms (eg, “brain” OR “head”), and spelling variations (eg, “tumor” OR “tumour”). Another example of synonyms is “lacosamide” OR “harkoseride.” Depending on the database service provider, operators such as “*” or “?” were used for truncation or wildcards. In addition to free-text terms, each database was searched using a variety of subject terms selected from the databases’ controlled vocabulary (eg, MeSH for MEDLINE, and EMTREE for Embase). Databases were searched chronologically as far back in time as permitted by each database.
Included studies were original clinical trials and case series on ASM treatment of CRSE in humans. Excluded studies were those published only in abstract form, those on the treatment of only refractory NCSE (absence, focal impaired awareness, or electrographic) or anoxic–ischemic RSE, or those that used non-parenteral medications, devices, or surgery. If a study reported a mix of generalized CRSE, focal SE, and NCSE patients, we attempted to extract treatment outcomes for the CRSE patients. The language was not restricted to English, but an English or German abstract had to be available. Each study was abstracted for specific predefined data which were placed in a computer spreadsheet for detailed analysis. This spreadsheet contained the same categories as was used for the AES guideline on established CSE. 3 The question we sought to answer was whether each ASM was either as effective when it was the last drug added or as a comparator(s) at stopping clinical CRSE. It was assumed that clinical cessation of seizures is an objective measure. The efficacy of a loading dose followed by maintenance dosing of each ASM was noted.
Articles were classified as class I (triple masked, prospective, randomized controlled trials), class II (prospective matched group cohort study), class III (all other controlled trials), or class IV (evidence from uncontrolled studies, case series or reports, or expert opinions) according to the American Academy of Neurology Clinical Practice Guideline Process Manual. 21 That manual’s recommended terminology was used for this review’s evidence-based conclusions for the various ASMs.
Results
Database searches identified no class I, no class II, 9 class III, and multiple class IV studies on the use of the 13 ASMs in the treatment of CRSE.
Adrenocorticotropic Hormone, Corticosteroids, and IVIg
Immunomodulatory therapies include IM ACTH, IV corticosteroids, and IVIg. The mechanisms and roles that inflammation and the immune system play in epilepsy and SE are currently a topic of active investigation. Conditions associated with SE that may respond to immunomodulatory therapies include Rasmussen encephalitis, Hashimoto encephalitis, antibody-mediated encephalitis (eg, N-methyl
Investigations on the use of ACTH, corticosteroids (methylprednisolone, prednisone, and prednisolone), and IVIg often involve patients with epileptic spasms, severe epileptic encephalopathies, and rare epilepsy syndromes. These are predominantly disorders with onset in infancy and early childhood defined in the 2017 ILAE Classification of the Epilepsies, 28 including Ohtahara syndrome, epilepsy of infancy with migrating focal seizures, epileptic encephalopathy with continuous spike-and-wave during sleep, and Lennox-Gastaut syndrome. Seizures in these patients are resistant to conventional ASMs and often have NCSE (but not CRSE). On occasion these patients present with focal SE that evolves to CSE or CSE which becomes RSE, but due to the heterogeneity and rarity of these disorders and variability of the presentations in the patients treated with ACTH, corticosteroids, and IVIg, there are no publications of cohorts with RSE. In addition, there are no studies on the efficacy of ACTH, corticosteroids, or IVIg in CSE or RSE. The dosing of ACTH, corticosteroids, and IVIg is based on the treatment of acute and chronic seizures, epilepsy syndromes, and other neuroimmunological disorders (Table 1). 30 New-onset refractory status epilepticus (and its subset, FIRES) often starts as focal SE, evolves into CSE, usually results in SRSE, is mostly unresponsive to conventional ASMs, is temporarily responsive to IV anesthetic drugs, and (despite a lack of evidence from controlled trials) is often treated empirically with steroids, IVIg, ketogenic diet, and other immunomodulatory or anti-inflammatory therapies, including novel antibody therapies such as rituximab. 25
Parenteral Drugs for Refractory Status Epilepticus.
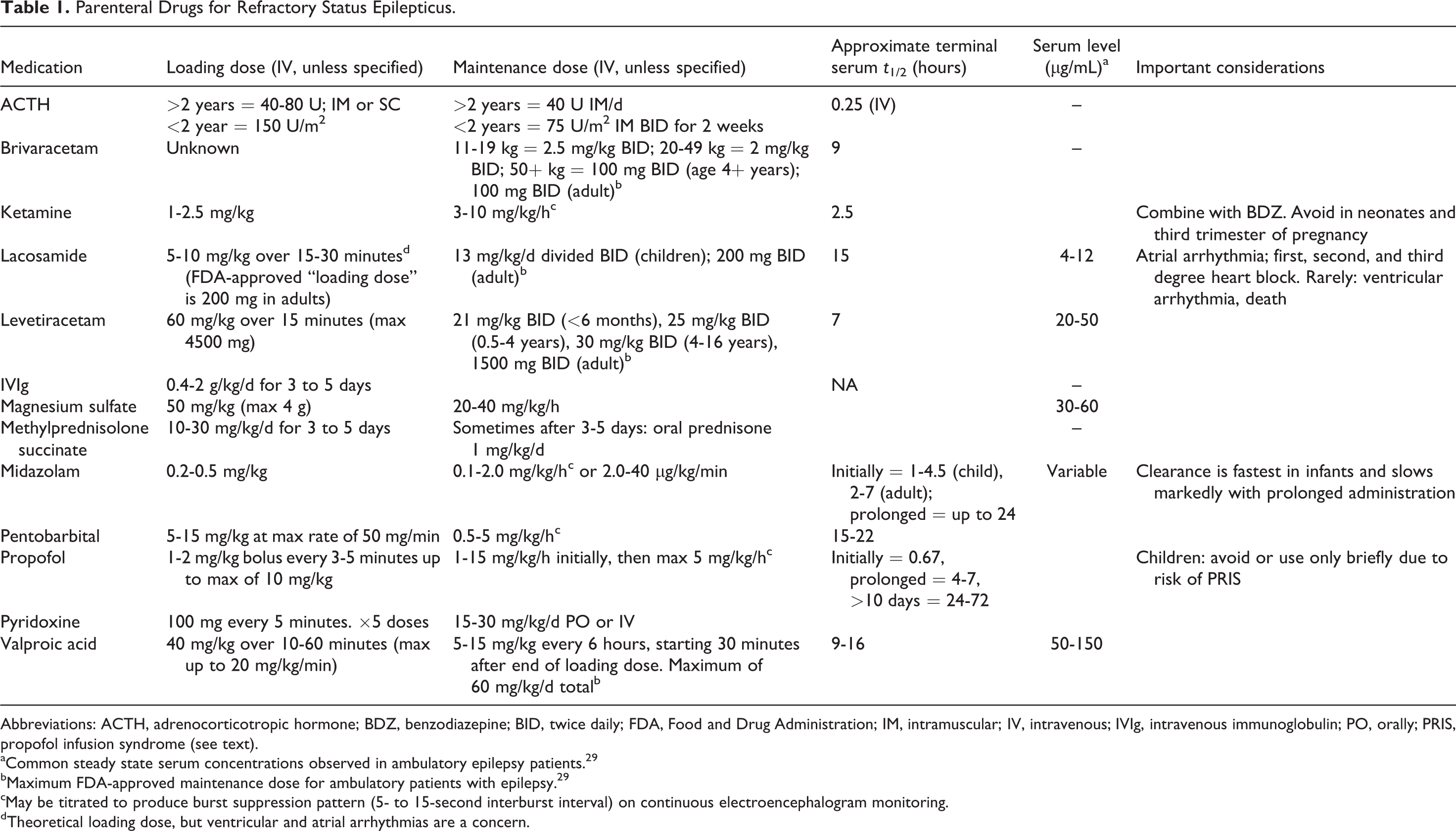
Abbreviations: ACTH, adrenocorticotropic hormone; BDZ, benzodiazepine; BID, twice daily; FDA, Food and Drug Administration; IM, intramuscular; IV, intravenous; IVIg, intravenous immunoglobulin; PO, orally; PRIS, propofol infusion syndrome (see text).
aCommon steady state serum concentrations observed in ambulatory epilepsy patients. 29
bMaximum FDA-approved maintenance dose for ambulatory patients with epilepsy. 29
cMay be titrated to produce burst suppression pattern (5- to 15-second interburst interval) on continuous electroencephalogram monitoring.
d Theoretical loading dose, but ventricular and atrial arrhythmias are a concern.
Brivaracetam
Brivaracetam, like LEV and piracetam, is in the racetam class. It presynaptically binds the synaptic vesicle 2A protein (SV2A) with high affinity and has faster blood–brain barrier penetration than LEV (apparent permeability coefficients at 2 hours were 25.5 × 10−6 cm/s for BRV and 9.6 × 10−6 cm/s for LEV). Brivaracetam and LEV bind SV2A at closely related sites, but in different ways, and affect vesicles which are actively releasing neurotransmitters. 31 Following a 2-minute IV bolus, Tmax is <5 minutes. Brivaracetam is only 20% protein-bound and t 1/2 is 9 hours. It is not recommended for use in patients with end-stage kidney disease.
Four uncontrolled studies examined the cessation of clinical CSE when BRV was the last ASM administered (no comparison group). Strzelczyk et al 32 treated 8 adults with RSE (6 were switched from LEV to BRV) and 3 with SRSE using 100 mg of BRV and found a 27% SE cessation. Kalss et al 33 reported 1 adult with “early-stage” CSE who responded to BRV. Aicua-Rapun 34 found that 200 mg of BRV had 50% effectiveness in 14 adults with RSE, but only 4 patients had CRSE. A Spanish registry of 43 adults with SE treated with BRV included 7 patients with CSE. 35 Of these 43 patients, 9 had established SE and 34 had RSE, but outcomes for (and the number of) patients with CRSE are not stated.
Drug–drug interactions exist: Brivaracetam can increase the serum concentrations of PHT and carbamazepine epoxide. Serious AEs include bronchospasm and angioedema. The IV formulation is not US Food and Drug Administration (FDA) approved for patients younger than age 16 years and is not approved for the treatment of SE. For adults with CRSE, insufficient evidence exists to support the effectiveness of BRV (level U, 4 class IV studies).
Ketamine
Ketamine is a synthetic drug and works mainly as a noncompetitive NMDA glutamate receptor antagonist.
36
Synaptic NMDA receptor numbers increase during SE, so KET may be a particularly effective treatment for RSE.
37
Fujikawa recommended that KET be started early in the sequence of treatments for RSE because it acts as a neuroprotectant against glutamate-induced widespread neuronal necrosis (despite ongoing ictal discharges) in animal models of SE.
38
It also interacts with opioid, monoaminergic, muscarinic, and nicotinic receptor ion channels (
Ketamine has a rapid onset of action (<1 minute IV) and a rapid distribution in the brain. Owing to its high lipid solubility, small size, and low protein binding (10%-30%), it has a large volume of distribution (Vd) at 3.1 L/kg, quickly crosses the blood–brain barrier, and has rapid systemic clearance at 19 mL/min/kg. 40,42 It is rapidly distributed to peripheral sites with an initial t 1/2 of 2 to 4 minutes and terminal elimination t 1/2 of 2.5 hours. 42 Ketamine undergoes metabolism (demethylation mainly by CYP3A4, secondarily by CYP2B6 and CYP2C9). The major metabolite is norketamine, a pharmacologically active metabolite, which undergoes further metabolism to inactive compounds. 42 Excretion of metabolites is principally renal (95% urine, 3% feces). 40 The effects of KET can be potentiated by selected cytochrome P450 inhibitors, other anesthetics or central nervous system (CNS) depressants, and sympathomimetics.
Animal models of SE show that KET is effective in the treatment of RSE and SRSE. Most human studies on KET for the treatment of CRSE are small retrospective series or isolated cases focused on the late use of this drug when multiple ASMs have failed, making it difficult to formulate recommendations, but ongoing clinical trials may provide further information. 43 We identified no class I to III and 25 class IV references, including 14 case reports and 11 case series containing from 2 to less than 15 cases of CRSE in infants, children, and adults, with age ranging from a preterm neonate age 1 day of life to an 88-year-old patient. Variability in studies encompasses not only age but also SE etiology, timing of KET treatment, ranging from days to weeks after onset, number of continuous infusions tried prior to KET, and the number of concomitant ASMs. While some case reports did not find a response, 44 -47 and while some larger series are not sufficiently granular to determine specific KET treatment outcome in RSE, 48 others report a response in most of the episodes, 49 -51 or partial response in their series. 52 -55 In a large multicenter class IV study of 58 children and adults (which included NCSE cases), KET was started after a median of 9 days, yet it controlled RSE “likely” in 12% and “possibly” in additional 20%. 54 Studies usually suggest a loading dose of 1 mg/kg (loading dose, repeatable), followed by 1 to 7 mg/kg/h (continuous infusion). In an ongoing RCT in adults (NCT03115489), an IV loading dose of 2.5 mg/kg of KET is given followed by a continuous infusion at 3 mg/kg/h until a burst suppression pattern is seen or up to a maximum dose of 10 mg/kg/h.
Adverse effects are transient dissociative psychosis (mitigated by concomitant BDZ use) and potential excessive sympathetic stimulation.37 Older studies suggest possible increased intracranial pressure, but recent literature does not support this side effect. Of note, some animal and clinical studies suggest neuroprotection in the setting of a major insult but also tentative neurotoxicity (particularly in immature brains without an insult and after repeated application). 56,57 Ketamine may produce less hypotension than other anesthetics, presumably due to promotion of sympathetic and respiratory stimulation. Fujikawa notes that KET should be avoided in neonates and in women during the third trimester owing to evidence that it increases neuronal apoptosis in rats during these stages of infant development. 38
For children and adults with CRS,E insufficient evidence exists to support the effectiveness of KET (level U; 25 class IV studies). Nevertheless, the lack of substantial hypotension and its inhibition of NMDA receptors make KET attractive for RSE treatment. Ongoing clinical trials (NCT02431663 for children and NCT03115489 for adults) comparing KET, MDZ, and PRO in the treatment of RSE are expected to provide higher strength evidence on comparative efficacy and safety.
Lacosamide
Lacosamide (formerly, harkoseride) is a functionalized amino acid available in the United States as an IV solution. Its proposed mechanism of action is enhancement of Na+ channel slow inactivation. It has linear PK, is demethylated by CYP3A4, 2C9, and 2C19, and is then 95% renally excreted. The t 1/2 is 15 hours, and there are no significant drug–drug interactions.
Literature searches yielded 124 references. Review articles and reports which did not study SE were excluded. Between 2009 and 2019, 32 clinical trials were reported using IV LCM as treatment for SE: 3 class III and 29 class IV. They used different definitions of RSE, and some included a large proportion of focal SE or electrographic NCSE cases. Two studies involved patients who had only received a BDZ prior to LCM (established SE). 58,59 Most commonly, efficacy was defined as cessation of clinical or electrographic ictal activity when LCM was the last drug added.
Sixteen studies on adults or on both children and adults examined the efficacy of LCM in the treatment of CRSE (2 class III and 14 class IV studies). 60 -75 Most of these 16 CRSE studies were flawed. They often included a mix of tonic–clonic SE, focal SE, and NCSE. In only a few studies, the results in CRSE patients were presented separately. Some studies had a mix of established SE and RSE patients, and a few do not make it clear if patients had one, the other, or both. 61 Rarely was it possible to identify the results in patients with only CRSE. 63 In one class III study, 45 adults with RSE (9 had CRSE) who received LCM 200 mg twice a day (no loading dose) had a significantly lower odds of death and a non-significant greater odds of SE control than did a historical control group. 76 In a second class III study of 31 adults with RSE (4 had CRSE), 68% had seizure control with LCM 400 mg load followed by 200 mg twice a day, which was not different from comparison groups which received LEV or VPA. 68 In 14 class IV studies, 0% to 100% (mean = ∼50%) of patients with CRSE or mixed RSE reportedly responded to LCM. The median loading dose was 300 mg, and maintenance dose was 200 mg twice a day. Perrenoud et al. found no correlation between response to LCM and the loading doses they investigated. 61 Adverse effects possibly related to LCM were bradycardia, hypotension, PR interval prolongation, high-degree heart block, rash (n = 3), and angioedema (n = 2).
Six class IV studies on children studied the use of LCM in the treatment of RSE. Three studies included 26 children with an average age of 5 years, but the exact ratios of those with CRSE versus focal RSE were not stated. 77 -79 Among these children, RSE responded to LCM in 15 of 20 cases, the median loading dose was 8.7 mg/kg, daily maintenance dose was 13 to 14 mg/kg/d, and 1 child had an adverse event (bradycardia). Three studies reported on 5 children: one with NCSE and congenital heart disease had an arrhythmia after LCM, and 1 with SRSE and 3 with tonic RSE all had SE stopped after receiving LCM. 80 -82
For comparison, a class III study of second-line treatment of established CSE (ie, not RSE), 66 adults received a single dose of LCM 400 mg or VPA 30 mg/kg after a BDZ. 58 Cessation of CSE at 1 hour was 63.3% for LCM and 69.7% for VPA, and 24-hour seizure freedom was 45.5% and 60.6% respectively (P = nonsignificant [NS] for both). In the LCM group, 1 had bradycardia, 1 had hypotension, and 2 had sedation. In the VPA group, 6 had hepatic dysfunction.
The FDA has approved an adult LCM “loading dose” of 200 mg given either IV (over 15-60 minutes) or orally. 83 A true loading dose is defined by the formula: DL = Vd × Css (DL = loading dose in mg/kg, Vd = volume of distribution, Css = steady state serum concentration). The Vd of LCM is ∼0.6 L/kg; so to produce a suggested target Css of 15 μg/mL, a loading dose of 9 mg/kg would be required. In an observational study, 84 it was found that patients receiving a loading dose of 10 mg/kg often had a serum level of 15 to 20 μg/mL. Perrenoud et al confirmed in patients with SE that high LCM loading doses (>9 mg/kg) were associated with a serum level in the 10 to 20 μg/mL range. 61 Based upon these considerations, a loading dose of 10 mg/kg is theoretically reasonable.
Adverse effects of LCM include dizziness, ataxia, diplopia, headache, nausea, prolonged PR interval, atrial arrhythmias, and syncope (especially with diabetes). Warnings are bradycardia, AV block, and ventricular tachyarrhythmia, which have rarely resulted in asystole, cardiac arrest, and death. Most cases had occurred in patients with underlying proarrhythmic conditions or in those taking concomitant medications that affect cardiac conduction or prolong the PR interval. These events have occurred with both oral and IV routes and at prescribed doses as well as in the setting of overdose. Therefore, LCM should be used with caution in patients with underlying proarrhythmic conditions such as known cardiac conduction problems (eg, marked 1° AV block, 2° or higher AV block, and sick sinus syndrome without pacemaker), severe cardiac disease (eg, myocardial ischemia or heart failure, or structural heart disease), and cardiac sodium channelopathies (eg, Brugada syndrome), and in patients on concomitant medications that affect cardiac conduction, including sodium channel blockers, β-blockers, calcium channel blockers, potassium channel blockers, and medications that prolong the PR interval. 83
For children and adults with CRSE, it is possible that LCM is effective at stopping RSE (level C; 2 class III, 14 class IV studies). For adults with established CSE (after first-line treatment with a BDZ, that is, not RSE), insufficient evidence exists to support that LCM and VPA are equally effective as second-line treatment (level U, 1 class III study). An LCM loading dose of 10 mg/kg can be calculated using a standard pharmacokinetic formula, but recent warnings on atrial and ventricular arrhythmias are a concern.
Levetiracetam
The putative mechanisms of action of LEV are to bind SV2A proteins and amino-3-hydroxyl-5-methylisoxazole-4-propionic acid (AMPA) receptors and to inhibit high voltage-activated Ca2+ channels. Oral absorption is rapid, but food can negatively affect the concentration and time-to-effect. Levetiracetam has a Vd of 0.5 to 0.7 L/kg, has a t 1/2 of 7 hours, and is <10% protein bound. It undergoes enzymatic hydrolysis (noncytochrome P450) to an inactive metabolite and is ∼66% eliminated unchanged in the urine; so in renal insufficiency, the dose must be reduced proportionate to creatinine clearance. Hemodialysis eliminates 40% in 4 hours (up to 73% in critically ill patients). It has few drug–drug interactions.
Levetiracetam for the treatment of CRSE
Isguder et al reported a class III review of 78 children (median age: 31 months) with RSE who received 20 mg/kg IV loading doses of LEV or VPA. Both drugs were equally effective, but LEV was safer (12.5% of VPA patients had hepatic dysfunction). 85 In a class IV study, Moddel et al reported that among 36 RSE adults (50% had CRSE) treated with a median of 3000 mg/d of LEV, 69% of patients had RSE stopped. No cardiovascular AEs were seen. 86 In a class IV report, Rantsch et al studied 118 adults to determine the efficacy of various ASMs in terminating RSE. 87 Only 10 patients treated with LEV had CRSE. Levetiracetam was more effective in terminating CRSE than other ASMs, but the difference was not significant given the small numbers.
Levetiracetam for the treatment of established CSE
The majority of studies published on LEV are for the treatment of established CSE (first line or second line after a BDZ), not for CRSE. Navarro et al conducted the class II SAMUKeppra study of 203 adults with CSE treated in the prehospital setting concurrently with IV clonazepam 1 to 2 mg plus either 2500 mg of LEV or placebo. 88 There was no difference between LEV and placebo in CSE control after 15 minutes (relative risk = 0.88, 95% CI: 0.74-1.05, P = .14). Nene et al conducted a class II study of 118 patients older than age 60 years with CSE not controlled with first-line LZP. 89 Patients received 20 to 25 mg/kg of either LEV or VPA. Control of CSE was not different between the groups, but higher STESS was associated with poorer therapeutic response (P < .05).
Gujjar et al reported a class III study of 52 adults who received first-line treatment with a BDZ followed by a loading dose of LEV 30 mg/kg or PHT 20 mg/kg. There was no difference in efficacy or side effects, but 4 patients developed RSE despite receiving both LEV and PHT sequentially. 90 Chakravarthi et al reported a class III study in which 44 adults first treated with LZP were then given either LEV or PHT, both at 20 mg/kg. 91 There was no difference: 28 of 44 had initial CSE controlled, but 16 required further treatment. Phenytoin was associated with hypotension in 2 patients. Mundlamuri et al reported a class III study of LEV in 150 adults with established CSE, 29% of whom progressed to RSE. 10 After first receiving 4 to 6 mg of LZP, patients were randomized 1:1:1 to receive a loading dose of LEV 25 mg/kg, PHT 20 mg/kg, or VPA 30 mg/kg. Of those receiving LEV, 22% progressed to RSE and were given PHT. Of those who received PHT or VPA, 32% went on to RSE and were crossed over to the other drug, and then if RSE persisted, LEV was given. Overall, no efficacy difference was found between the 3 drugs. Three PHT patients died: 1 from arrhythmia and 2 from hypotension and respiratory failure. In a class III study of established SE in 167 adults with adjustment for severity by STESS score, VPA was slightly superior to LEV, but PHT was equal to LEV or VPA—all at 20 mg/kg loading doses. 92 In a class IV study of 9 elderly patients with established SE, Fattouch et al 93 reported that first-line therapy with a 1500 mg loading dose of LEV was effective with no significant adverse events. Finally, a class III study in children and adults with CSE compared first-line treatment with LEV at 20 mg/kg to LZP. Both were equally effective, but LZP was associated with more respiratory compromise and hypotension. 94 Fifteen retrospective class IV studies were found on LEV as second-line treatment for established CSE in children and adults.
With regard to LEV dosing, the 2016 AES guideline for treatment of established CSE is to give a BDZ, followed by an IV loading dose of LEV of 60 mg/kg (maximum 4500 mg). 3 Older studies reported an adult loading dose of LEV 20 to 30 mg/kg infused at 5 mg/kg/min followed by a maintenance dose. 91 Rossetti et al reported that LEV may be useful in SE, but escalating the dose above 3000 mg/d was unlikely to provide further benefit. 95 Gallentine et al investigated LEV in children aged 0 to 8 years with RSE and reported a mean loading dose of 30 mg/kg IV with daily titration for persistent seizures. 96 Another group found a mean loading dose of 37.5 mg/kg in responders in children aged 0 to 16 years. 97
In 3 major randomized trials published in 2019, larger loading doses of LEV were studied for established CSE. In the class I ESETT study, 384 patients aged 1 to 95 years with BDZ-resistant established CSE (not RSE) were randomized using a Bayesian adaptive design to receive fosphenytoin 20 mg PE/kg, LEV 60 mg/kg, or VPA 40 mg/kg. 18 Cessation of CSE was seen in equal proportions with LEV (47%), PHT (45%), and VPA (46%; P = NS). No differences were seen in improved level of consciousness or major safety events, but numerically more episodes of hypotension and intubation occurred with PHT and more deaths occurred with LEV. In the class III EcLiPSE open-label randomized controlled trial in the United Kingdom, second-line treatment with loading doses of IV LEV at 40 mg/kg and IV PHT at 20 mg/kg were compared in 286 children with CSE following first line with a BDZ. 98 Convulsive status epilepticus was terminated slightly more often and faster with LEV than with PHT (P = .20), and serious AEs occurred with PHT (life-threatening hypotension, worsened focal seizures, and decreased level of consciousness). The class III ConSEPT open-label randomized controlled trial in Australia and New Zealand also compared second-line treatment with loading doses of IV LEV at 40 mg/kg and IV PHT at 20 mg/kg in 352 children with CSE following first-line treatment with a BDZ. 99 Clinical cessation of seizures 5 minutes after the completion of the loading dose occurred in 60% of children in the PHT group and 50% in the LEV group (P = .16), and there were no serious AEs.
In summary, for children with CRSE, insufficient evidence exists that LEV and VPA are equally effective (level U, 1 class III study). For adults with CRSE, insufficient evidence exists to support the effectiveness of LEV (level U; 2 class IV studies). By comparison, for children and adults with established CSE (ie, not RSE), after only an initial BDZ, it is likely that loading doses of LEV 60 mg/kg, VPA 40 mg/kg, and PHT 20 mg PE/kg are equally effective at stopping CSE (level B, 1 class I study). For children with established CSE, it is possible that LEV 40 mg/kg and fosphenytoin (PHT) at 20 mg PE/kg are equally effective (level C; 2 class III studies). For adults with established CSE, it is possible that LEV 20 to 30 mg/kg, VPA 20 to 30 mg/kg, and PHT 20 mg PE/kg are equally effective (level C; 1 class II and 4 class III studies). For adults with established CSE, it is possible that LEV at 2.5 g is as effective as placebo (level C; 1 class II study).
Magnesium Sulfate
Magnesium sulfate has been used for decades to treat preeclampsia. In a randomized trial of 2138 pregnant women with hypertension admitted for delivery, MgSO4 was superior to PHT in the prevention of eclampsia. 100 Although not fully understood, it may have 3 mechanisms of action. Firstly, it is believed to inhibit the NMDA-glutamate receptor, which is upregulated during seizures. Secondly, it is known to act as a cerebral vasodilator which is helpful as cerebral blood flow tends to be impaired during seizures. Thirdly, it appears to act as a calcium channel blocker. It is appealing as an ASM due to its lack of major adverse events. 101 Magnesium sulfate is 30% to 40% protein bound (primarily albumin) and is renally eliminated. The exact t 1/2 is unknown, but 90% of the drug is believed to be eliminated within 24 hours. Magnesium sulfate follows a 2-compartment model with rapid distribution α phase and a slow β phase of elimination. The therapeutic range of MgSO4 in practice has varied owing to a lack of controlled trials. We are aware of only case reports, among which a therapeutic range of 3 to 6 mg/100 mL was reported. 102 Magnesium sulfate is believed to have relatively few drug interactions, likely due to both a lack of study and incomplete knowledge of its metabolism.
There have been no randomized controlled trials evaluating the efficacy of MgSO4 in patients with CRSE, but several case reports have been published. Lansberg et al reported the use of MgSO4 in a 23-year old pregnant woman with epilepsy. 103 As mentioned above, MgSO4 has been used as an effective prophylactic and therapeutic agent for preeclampsia and eclampsia due to its lack of fetal toxicity concerns. Additionally, Pandey et al 104 reported an 18-year-old patient with NORSE treated successfully with MgSO4 after MDZ, PHT, phenobarbital, lamotrigine, and clonazepam had been ineffective. Zaatreh 105 reported the addition of MgSO4 to LEV to treat a patient who had SE and acute intermittent porphyria. Finally, Hatch et al 106 reported immediate reduction in seizures with MgSO4 in a 31-year old patient who developed RSE after inadvertent intrathecal injection of tranexamic acid.
Due to the off-label use and the lack of randomized controlled trials, the doses of MgSO4 reported for CRSE are highly variable. Tan et al 107 reported successfully treating seizures using a loading dose of 50 mg/kg (max 4 g/dose) and a maintenance dose of 20 to 40 mg/kg/h. Case reports have reported MgSO4 at a therapeutic range of 30 to 60 μg/ mL. 102 Magnesium sulfate is well tolerated. Adverse events (believed to be related to magnesium toxicity include cardiac arrhythmias or torsades de pointes, vasodilation, flushing, hypotension, and constipation. 101,108 While MgSO4 is affordable and widely available, there are only case reports evaluating its use in CRSE. More studies are needed to establish its role in CRSE.
Midazolam
Midazolam is a 1,4 BDZ which binds synaptic GABAA receptors with γ subunits to enhance opening of the chloride ionophore. Midazolam may be given by continuous infusion because it is water-soluble at lower pH and therefore does not require propylene glycol as a vehicle. By contrast, other BDZs (eg, lorazepam) cannot be used by infusion because propylene glycol may cause lactic acidosis. 109 At physiologic pH, MDZ is lipophilic, resulting in rapid CNS penetration. 110 Midazolam is highly (94%-97%) protein-bound and is metabolized by hepatic and intestinal CYP3A4 to its main active metabolite, 1′-hydroxymidazolam. Its metabolites are subsequently glucuronidated, then renally excreted. Elimination of MDZ is biphasic, consisting of an initial rapid phase (likely into adipose tissue) and a slower terminal phase with a t 1/2 which is shortest in infancy, 1 to 4.5 hours in children and 1.8 to 6.8 hours in adults. 111 -113 In single-dose studies, the t 1/2 of 1′-hydroxymidazolam is similar to the parent compound MDZ. 114 Hepatic metabolism is induced with prolonged use, so clearance increases 5- to 10-fold. Despite hepatic induction, its t 1/2 is prolonged up to as long as 24 hours with high-dose, long-term use. 112,113,115 -117 Enzyme-inducing ASMs such as carbamazepine, phenobarbital, and PHT reduce MDZ serum levels. Renal insufficiency and inhibitors of CYP3A4 prolong MDZ clearance and may result in prolonged sedation. 118 Moderate CYP3A4 inhibitors are erythromycin, diltiazem, and verapamil, and strong inhibitors are ketoconazole, itraconazole, and carithromycin. 114
Reports on the use of MDZ for RSE emerged in the late 1980s and early 1990s because of the incidence of hypotension and problems caused by the long t 1/2 of PTB. 119 -121 Literature searches identified 479 articles, of which 33 studies reported using continuous IV MDZ infusions for the treatment of RSE. Reports on the use of IM, intranasal, buccal, or bolus IV MDZ as the first treatment for SE were excluded. Of these 33 original studies, 0 were class I or II, 4 were class III, and 29 were class IV.
One class III study prospectively compared 12 adults who received MDZ infusion at 0.1 to 0.4 mg/kg/h to 11 adults who received PRO infusion reaching doses of 0.5 to 2.5 μg/mL. 122 Refractory status epilepticus was controlled in 25% of MDZ and 45% of PRO recipients (P = NS); 65% failed these anesthetics (SRSE) and went on to receive THP. Convulsive RSE was seen in a slightly greater percentage of the PRO patients. The mean STESS score was 3. A second class III study compared 100 adults who received high-dose MDZ infusion (median maximum: 0.4 mg/kg/h) to 29 who received low-dose MDZ (median maximum: 0.2 mg/kg/h). 123 The high-dose group started MDZ 1 day earlier, had fewer withdrawal seizures in the first 48 hours, and had lower mortality at discharge, but no difference in ultimate failure of MDZ (needing other ASMs) or hospital complications.
One class III prospective study compared 21 children who received MDZ infusion at 2 to 10 μg/kg/min to 19 who received diazepam infusion at 0.01 to 0.1 mg/kg/min. 124 Refractory status epilepticus was controlled in 86% and 89% of MDZ and DZP patients, respectively (P = NS). A second class III prospective observational cohort study compared 42 children who received MDZ as the first anesthetizing ASM to 13 children who received PTB as the first (n = 2), second (n = 9), and third (n = 2) anesthetizing ASM. 125 Refractory status epilepticus was controlled by MDZ in 71% and by PTB in 85%, but a direct comparison is not possible because most children received PTB after first receiving MDZ.
Twenty-nine class IV retrospective studies or case reports were published between 1992 and June 2019. The oldest study included 7 children and adults, 119 1 was a study of 55 neonates <1 week of age, 126 15 studies included 760 children, and 12 studies involved 457 adults treated with MDZ infusion for RSE. The number of patients per study ranged from as small as one to as large as 358 children 127 and 339 adults. 128 Efficacy (as determined by cessation of clinical or electrographic RSE when MDZ was the last ASM added) was 56% in neonates. 126 Efficacy was 46.7% to 100% (median = 89%, regardless of sample size) across the studies in children. In the largest study, 64.5% of children had RSE controlled with MDZ. 127 In the adult studies, efficacy was 10% to 100% (median = 86%). In 5 of these 29 studies, efficacy of MDZ compared favorably to PRO, but the number of patients was small. In 12 of the 29 class IV studies, MDZ efficacy was similar to PTB/THP or high-dose PB.
The median MDZ dose rate was 0.25 mg/kg/h in the neonatal study. 126 In the 17 studies of children with specified doses, the total loading dose ranged from 0.1 to 0.2 mg/kg and the continuous infusion rates ranged from 0.06 to 1.5 mg/kg/h. The most common pediatric loading dose was 0.2 to 0.3 mg/kg and maximum infusion rate was 0.25 to 1.4 mg/kg/h. In the 11 studies of adults specifying doses, the total loading dose ranged from 0.03 to 0.5 mg/kg and the continuous infusion rates ranged from 0.02 to 2.9 mg/kg/h. The most common adult total loading dose was 0.15 mg/kg and maximum infusion rates were about 0.4 to 1.2 mg/kg/h. Infusions were typically reported to begin at low rates with subsequent titration at increments of 0.1 mg/kg/h at unreported intervals up to a maximum rate.
Adverse effects of MDZ in RSE patients were respiratory depression, hypotension, seizure recurrence upon MDZ withdrawal, development of drug resistance, nonanion gap hyperchloremic metabolic acidosis, 129,130 infection, and death (mostly attributed to the underlying etiology of the RSE). Inotropic support was needed less often with MDZ than with PTB in 3 of the class IV studies and 2 of the class III studies. 122,125 Longer hospital stays and more frequent infections were reported with PTB/THP than with MDZ. In 1 study, 0 of 16 patients receiving MDZ and 5 of 9 receiving PRO developed propofol infusion syndrome (PRIS). 131 Mortality was 17% with MDZ and 57% with PRO (P = NS) in 1 study. 132 In April 2017, the FDA updated a warning that all anesthetic drugs used for >3 hours in pregnant women and in children <3 years of age may cause neuronal loss in the child. 133 In general, the concomitant use of MDZ and opioids, barbiturates, or alcohol may result in hypotension, respiratory depression, airway obstruction, desaturation, apnea, coma, and death. 114
For children with CRSE, insufficient evidence exists to support either that MDZ and diazepam infusions are equally effective (level U; 1 class III study) or that MDZ infusion and PTB are equally effective (level U; 1 class III study). For adults with CRSE, insufficient evidence exists to support either that MDZ infusion and PRO are equally effective (level U; 1 class III study) or that low-dose and high-dose MDZ infusions are equally effective (level U; 1 class III study). For children and adults with CRSE, insufficient evidence exists to support that MDZ is effective as the last drug added (level U; 29 class IV studies).
Pentobarbital and Thiopental
The barbiturates PTB and THP bind GABAA receptors nonspecifically, thereby affecting both synaptic (phasic) and extrasynaptic (tonic) receptors to enhance neuronal chloride channel opening and inhibition of cortical function. This differs from BDZs which bind only GABAA receptors containing a γ subunit. They also appear to inhibit AMPA receptors resulting in suppression of glutamatergic neurotransmission. Pentobarbital is used in the United States, and THP is more commonly used in Europe. Thiopental is 25% metabolized to PTB, so literature devoted exclusively to use of THP in RSE is included in this review. Compared to other barbiturates, these agents are moderately lipophilic and readily cross the blood–brain barrier. Onset of action is rapid: ∼1 minute after IV administration. Elimination of PTB is biphasic: about 4 hours in first phase and up to 50 hours (dose dependent) in the second phase. The change in duration is largely due to sequestration in fat and muscle. Once redistributed, the free fraction undergoes metabolism in the liver, with potent induction of the hepatic microsomal enzymes (especially CYP2A6).
After prolonged administration, t 1/2 of THP is 14 to 36 hours and t 1/2 of PTB is 15 to 22 hours, 134 but Rashkin et al reports the t 1/2 of PTB is 15 to 60 hours. 135 Van Ness et al state that PTB has somewhat shorter t 1/2, less immunosuppression, more linear kinetics at higher doses, and fewer cardiovascular effects than THP. 136 Barbiturates reportedly decrease cerebral metabolism and blood flow and reduce intracranial pressure as a result. 137 Pentobarbital crosses the placenta, has significant teratogenicity, and is contraindicated in pregnancy. Pentobarbital has high potential for drug interactions due to enzyme induction and protein binding. The IV solution has a pH of 9.5 and (similar to PHT and phenobarbital) is solubilized in propylene glycol, thus making it incompatible with many other IV medications and infusions.
A literature search resulted in 231 references, most of which were discussions, reviews, or animal studies. Forty-four original studies published between 1967 and 2019 reported the use of PTB or THP for RSE: 2 were class III and the other 42 were class IV. However, these studies varied in inclusion of CSE or NCSE, and some did not characterize SE. Ten studies addressed pediatric SE exclusively, and one was restricted to neonates. 138 Efficacy was usually defined as no recurrence of electrographic seizures after weaning off PTB.
A class III study compared 42 children who received MDZ as the first anesthetizing ASM to 13 children who received PTB as the first (n = 2), second (n = 9), and third (n = 2) anesthetizing ASM. 125 Refractory status epilepticus was controlled by MDZ in 71% and by PTB in 85%, but a direct comparison is not possible because most children received PTB after first receiving MDZ. The other class III single-blind randomized multicenter study compared THP and PTB to PRO in RSE in 24 adults but was halted due to slow recruitment. 134 Control of RSE occurred in 6 of 14 (43%) PRO and 2 of 9 (22%) THP patients (P = NS; RR: 1.50; 95% CI: 0.4-5.61). There were no significant differences in mortality, infection, or hypotension, but there was a longer period of mechanical ventilation required for the THP group (median: 17 days) than the PRO group (median: 4 days). A class IV study found PTB stopped RSE in 90% of patients, but with recurrence in 48%. By adding phenobarbital, weaning success increased to 80%. 139 A class IV study by Parvianinen et al found THP at a loading dose of 5 mg/kg followed by infusion of 5 mg/kg/h controlled clinical and electrographic RSE in 10 of 10 adults. 140 Recovery from anesthesia was prolonged. The remaining class IV studies on adults, children, and both age groups suggest that PTB/THP can successfully stop RSE.
Most reviewed studies used initial PTB bolus dose of 5 mg/kg, with increase to 20 mg/kg, titrated to achieve burst suppression on electroencephalogram (EEG). For THP, the dose was initiated to achieve burst suppression at 2 to 5 mg/kg/h. The duration of infusion before weaning was not clearly specified, with ranges of 4 to 65 hours reported before weaning. The FDA recommendation for PTB use in SE is to administer 5 to 15 mg/kg IV load at a rate of no greater than 50 mg/min. An additional loading dose of 5 to 10 mg/kg may be given, followed by a continuous infusion of 0.5 to 5 mg/kg/h. The infusion should be titrated by 0.5 to 1 mg/kg/h to induce coma state characterized by absent brain stem reflexes and suppression of the EEG. Although intermittent IV infusion of PTB is FDA approved for the treatment of SE, specific dosing and weaning recommendations are not available.
The most common AE of PTB reported in all studies was hypotension. Tasker et al 125 reported that significantly more patients treated for SE required vasopressors with PTB (7/11 or 64%) than with MDZ (12/42 or 29%). Other complications reported included longer mechanical ventilation times, pneumonia, and acidosis. Two case reports have noted severe lactic acidosis after prolonged PTB infusion attributed to the 40% propylene glycol content of the vehicle. 141,142 The availability of PTB has been variable; current shortages can be found on the FDA website. 143
In summary, for children with CRSE, insufficient evidence exists to support that MDZ infusion and PTB are equally effective (level U; 1 class III study). For adults with CRSE, insufficient evidence exists to support that PTB and PRO are equally effective (level U; 1 class III study). For adults and children with CRSE, insufficient evidence exists to support that PTB is effective as the last ASM added (level U; 42 class IV studies).
Propofol
Propofol is an IV agent with sedative–hypnotic properties. It inhibits NMDA receptors (via channel gating modulation). It also is a GABAA receptor agonist by activating the β-1 subunit of the chloride channel in the receptor, but it is unclear if it binds the receptor directly or mediates it through second messengers. Both PRO and BDZs affect GABAA deactivation (with a similar rate to decay following drug termination), but they affect drug desensitization differently. In submaximal concentrations of GABA, both drugs slow the rate and extent of receptor desensitization, but in saturated GABA states, only PRO decreases the rate and extent of receptor saturation. In hypercarbia, PRO results in increased cerebrovascular tone; thus, it can decrease cerebral blood flow.
Propofol contains the active ingredient 2, 6-diisopropylphenol. It is highly lipophilic and rapidly distributed, so it equilibrates quickly between plasma and brain. It crosses the placenta, enters breast milk, and is >95% protein bound. Propofol is a major substrate of hepatic isozyme CYP2B6, but its metabolism is primarily through glucuronidation to inactive metabolites which are then renally excreted. Onset of action is rapid: within 30 to 60 seconds to achieve sedation and EEG anesthetic changes. Elimination t 1/2 varies based upon the duration of its use (Table 1). The t 1/2 is context-sensitive, varying from 10 minutes with a 3-hour infusion to 30 minutes with infusions lasting up to 8 hours. 42 With longer infusions, the t 1/2 is 3 to 12 hours due to slow release from fat, with about 70% of a single initial dose excreted in 1 day and 90% in 5 days. Terminal t 1/2 after a 10-day infusion varies and may extend up to 3 days, but after longer administration, the t 1/2 of PRO has been found to be only 140 minutes, allowing for rapid titration and withdrawal. 134
Literature searches between 1988 and 2019 yielded 256 articles. Most were reviews or were irrelevant to use of PRO for the treatment of RSE. Forty-three articles exclusively addressed complications of PRO, including PRIS, withdrawal, and induced seizures, and 23 case reports of use of PRO in seizures, of which 8 were specific to SE. Only 28 articles directly addressed use of PRO in the treatment of RSE.
One prospective class III study randomized 23 adults with RSE to either PRO or MDZ. 122 Status epilepticus control was higher in the PRO group (45% compared to 25% P = .4), but mortality was higher in the PRO group (72.7% vs 58.3%, P = .67). Complications, including progression to SRSE, were not different between the 2 groups. A second class III study of 24 adults comparing PRO to PTB showed no difference in seizure control, mortality, or complications. 134 Several class IV studies have indicated successful use of PRO in RSE. One study documented 31 episodes, all treated with PRO in combination with other agents, with successful control in 67%. 144 Sabharwal et al retrospectively analyzed 67 patients with SRSE treated simultaneously with combination of KET and PRO, with 79% requiring vasopressors and 39% overall mortality. 145 The overall RSE resolution rate was 91%, with 5 of 13 patients with anoxic injury. 145 A recent retrospective observational study in which 162 (89%) of 182 of adults received PRO found that shorter duration, higher dose TC was associated with fewer in-hospital complications and poor outcomes. 17
A common IV bolus dose in adults is 1 to 2 mg/kg repeated every 3 to 5 minutes up to a maximum of 10 mg/kg. This is followed by a continuous infusion at 1 to 10 mg/kg/h to maintain a seizure-free state. Infusion rates over 10 to mg/kg/h may be required but should not be maintained for more than 48 hours because of the risk of the PRIS. The pathophysiology of PRIS is either direct mitochondrial respiratory chain inhibition or impaired mitochondrial fatty acid metabolism mediated by PRO. Geriatric patients usually should receive 50% lower induction and maintenance doses. Propofol infusion syndrome, characterized by metabolic acidosis, cardiac failure, bradycardia (typically right bundle branch block), hypertriglyceridemia, hepatotoxicity, rhabdomyolysis, renal failure, and death, 146 has been associated with use of higher dose (>4 mg/kg/h) and longer duration (>48 hours) therapy. 147,148 The use of concomitant ASMs may allow one to lower the dose of PRO. 144 Other predisposing factors for PRIS are young age, catecholamine or glucocorticoid administration, low carbohydrate intake, and subclinical mitochondrial disease. Many guidelines do not recommend the use of PRO for RSE treatment in children younger than age 16 years. 149 Drug–drug interactions with VPA elevate PRO blood concentrations. Propofol should be used with caution in patients with dehydration or cardiac, cerebrovascular, or pulmonary disease. During weaning, when the patient has reached light anesthesia, maintenance of some sedation is needed to reduce the risk of PRO withdrawal, which can be associated with seizures, agitation, tachycardia, anxiety, tremulousness, and resistance to mechanical ventilation. 150 A rare reported benign effect of PRO in some individuals is green discoloration of the urine. 151
In summary, for adults with CRSE, insufficient evidence exists to support either that MDZ infusion and PRO are equally effective (level U; 1 class III study) or that PTB and PRO are equally effective (level U; 1 class III study). For CRSE, insufficient evidence exists to support that PRO is effective as the last ASM used (level U; 26 class IV studies). No pediatric-only studies exist on the use of PRO for CRSE, and many guidelines do not recommend its use in children aged <16 years.
Pyridoxine
Patients with epilepsy caused by inherited metabolic disorders may be resistant to ASMs and progress to RSE. 152 These disorders are especially important to recognize early due to the availability of treatments other than conventional ASMs. Pyridoxine (vitamin B6) is an important cofactor for many enzymes and specific amino acid and metabolic pathways in the brain which involve GABA and glutamate. 153 Pyridoxine-responsive and pyridoxine-dependent epilepsies are the canonical examples of inherited metabolic epilepsy and should be considered in neonates, infants, and children up to age 3 years presenting with refractory epilepsy without any identifiable lesion on imaging and other acquired cause of seizures. The typical presentation is a neonate in whom acquired causes of seizures have been excluded and who does not respond to ASMs. Atypical presentations include patients in whom seizures are initially controlled with ASMs but have frequent breakthrough seizures and episodes of SE as infants or toddlers. 154,155
In the past, the diagnosis was confirmed empirically using a trial of pyridoxine followed by its discontinuation and observation of seizure recurrence. The discovery of the molecular basis of this disorder and specific biochemical biomarkers makes definitive diagnosis more readily available. 156 The diagnosis leads to the proper treatment with 100 mg of IV pyridoxine while monitoring EEG, oxygen saturation, and vital signs. The dose of pyridoxine may be repeated at 5- to 10-minute intervals up to a dose of 500 mg. Clinical seizures often respond immediately (or within minutes) and the epileptiform discharges in the EEG often subside. The improvement in EEG background activity may be delayed for several hours.
Valproic Acid
Valproic acid is a short-chain fatty acid approved in Europe in the 1960s and in the United States in 1978 for oral administration. It is effective against absence, myoclonic, focal impaired awareness, and generalized-onset tonic–clonic seizures. Multiple mechanisms of action are reported, including attenuation of voltage-gated sodium channels and indirect effects on GABA economy (though it is not a direct GABA agonist). A commonly used IV loading dose is 20 mg/kg infused over 1 hour, but the ESETT study used a loading dose of 40 mg/kg administered over 10 minutes. 18 Initial serum levels drop as VPA distributes into body fat, so maintenance dosing should be started 30 minutes to 2 hours after the IV load. A typical maintenance dose for IV use is 1 mg/kg/h, or 5 mg/kg every 6 hours, to maintain a steady state trough serum concentration of 50 to 100 μg/mL. The terminal elimination t 1/2 of 6 to 15 hours may be shortened by induction of hepatic metabolism by other drugs, notably PHT and barbiturates. Valproic acid is extensively metabolized by the liver, primarily via glucuronidation and less so by the fatty acid oxidation system and CYP2C9. Valproic acid can act as a hepatic enzyme inhibitor, thereby raising serum levels of several ASMs. The apparent Vd is small at 0.22 L/kg because of extensive protein binding. Valproic acid competes with PHT and BDZs for serum protein binding sites, which can cause increased CNS action of the displaced free drugs.
The treatment of SE with VPA began in the early 1990s, soon after the IV formulation became available. 157 A literature search using the terms “valproate” and “status epilepticus” yielded 615 references. Other sources did not reveal other relevant reports. However, most references proved to be general reviews or case reports, and most studies have small numbers of patients.
Valproic acid for the treatment of CRSE
In 1 class III study, 40 children with RSE were randomized to receive VPA 30 to 40 mg/kg or diazepam 10 to 100 μg/kg/min infusion. Refractory status epilepticus was controlled after 30 minutes in 80% of VPA and 85% of diazepam infusion patients (P = NS). 158 In another class III study of 78 children with RSE who failed BDZ and PHT and then received either 20 mg/kg of VPA or LEV, efficacy was no different. 85
Valproic acid for the treatment of established SE
In the recent class I ESETT study, 384 patients aged 1 to 95 years with BDZ-resistant established CSE (ie, not RSE) were randomized to receive fosphenytoin 20 mg PE/kg, LEV 60 mg/kg, or VPA 40 mg/kg. 18 Cessation of CSE was seen in equal proportions in both children and adults treated with LEV (47%), PHT (45%), and VPA (46%). No significant differences were seen in improved level of consciousness or major safety events, although numerically more episodes of hypotension and intubation occurred with PHT and more deaths occurred with LEV. In a class II study of 80 children aged 6 months to 10 years with established CSE treated with VPA or PB at 20 mg/kg each, PB was significantly more effective. 159 Nene et al conducted a class II study of 118 patients older than age 60 years with established CSE who received 20 to 25 mg/kg of either LEV or VPA, and there was no difference in efficacy. 44 In a class II study of 73 adults, PB 20 mg/kg was superior to VPA 30 mg/kg in initial efficacy as well as in a lower recurrence rate of seizures within 24 hours (P <.05). 160
In a class III study of 30 children and adults (aged 14-73 years) randomized to VPA or PHT both at 20 mg/kg, established CSE cessation was 73.3% and 60%, respectively (P = NS). 161 In a class III study, 37 patients aged > 15 years with CSE were randomized to loading doses of VPA 20 mg/kg or PHT 13 mg/kg, with no difference in efficacy observed. 162 In a class III study of established CSE, 66 adults received a single dose of LCM 400 mg or VPA 30 mg/kg. 58 Convulsive status epilepticus cessation at 1 hour was 63.3% for LCM and 69.7% for VPA, and 24-hour seizure freedom was 45.5% and 60.6%, respectively (P = NS for both). In a class III study of 110 adults with established SE, control was 78% for VPA 30 mg/kg versus 71% for PHT 20 mg/kg (P = NS). 163 Mundlamuri et al reported a class III study of 150 adults with established CSE, 29% of whom progressed to RSE. 10 After first receiving 4 to 6 mg of LZP, patients were randomized 1:1:1 to receive a loading dose of LEV 25 mg/kg, PHT 20 mg/kg, or VPA 30 mg/kg. Of those receiving LEV, 22% progressed to RSE and were given PHT. Of those who received PHT or VPA, 32% went on to RSE and were crossed over to the other drug, and then if RSE persisted, LEV was given. Overall, no efficacy difference was found between the 3 ASMs. In a class III study of established SE in 167 adults with adjustment for severity using STESS, VPA was superior to LEV (odds ratio [OR] = 2.69, 95% CI: 1.19-6.08), but PHT was equal to LEV or VPA—all at 20 mg/kg loading doses. 92
Intravenous VPA is well tolerated. The most common side effects are nausea and dizziness. Fewer than 5% of patients experience somnolence, an advantage over sedating agents. There are some reports of acutely elevated serum transaminases. Eleven of 28 patients treated for SE with VPA in one series 164 had ammonia levels of >50 μmol/L, but there are other causes for elevated ammonia in ICU patients, including nutritional factors and cancers, so a causal relationship to encephalopathy is often unclear. Valproic acid is contraindicated in children and adults with known or suspected mitochondrial disorders or disorders of fatty acid metabolism and in women with X-linked hyperammonemia. Valproic acid is a teratogen and should not be given to pregnant women with SE. Most other side effects of VPA, such as tremor, weight gain, and thrombocytopenia, are not considerations with short-term IV use.
Valproic acid infusion may be stored at room temperature, may be given in any aqueous solution, and is not excessively expensive. The manufacturer recommends infusion over 60 minutes, not faster than 20 mg/min. However, to give 40 mg/kg at this rate would take over 2 hours. Much faster administration, such as 3 mg/kg/min, or the entire dose over 10 minutes, appears to be safe and is more likely appropriate for SE. 165 It is often given diluted 1:1 in aqueous medium but can be given undiluted. Valproic acid may follow PHT in a treatment sequence for CSE, so free PHT levels, not total levels, would need to be monitored when using that combination because of the protein binding interaction between these drugs. After IV infusion, a VPA serum level should not be checked for at least 2 hours because it takes time for the drug to distribute into all compartments. Hyperammonemia may occur but is infrequently implicated in encephalopathy in this patient population. Advantages are that it is relatively nonsedating and the IV form is well tolerated.
In summary, for children with CRSE, insufficient evidence exists to support either that VPA and LEV are equally effective (level U, 1 class III study) or that VPA and diazepam infusion are equally effective (level U, 1 class III study). No class I to III studies have been reported in adults treated with VPA for CRSE. By contrast, for children and adults with established CSE (ie, not RSE), after receiving an initial BDZ bolus, it is likely that loading doses of VPA 40 mg/kg, LEV 60 mg/kg, and PHT 20 mg PE/kg are equally effective (level B, 1 class I study). For infants and young children with established CSE, it is possible that phenobarbital is more effective than a 20 mg/kg loading dose of VPA (level C, 1 class II study). For children and adults with established CSE, it is possible that loading doses of VPA 20 to 30 mg/kg and PHT 13 to 20 mg/kg are equally effective (level C; 2 class III studies). For adults with established CSE, it is possible that VPA and LEV at 20 to 25 mg/kg each are equally effective (level C, 1 class II study), it is possible that phenobarbital 20 mg/kg is slightly more effective than VPA 30 mg/kg (level C; 1 class II study), insufficient evidence exists to support that VPA is as effective as LCM (level U; 1 class III study), and it is possible that VPA 20 to 30 mg/kg, LEV 20 to 25 mg/kg, and PHT 20 mg PE/kg are about equally effective (level C; 3 class III studies).
Discussion
Refractory status epilepticus is a medical emergency, with a high degree of morbidity and mortality. Unlike the treatment of convulsive established (initial) SE, no guidelines exist for the treatment of CRSE. The selection of ASM treatment of RSE has been at the discretion of clinicians based upon their training, personal experience, expert opinion, and published cases or mostly small uncontrolled studies. Some studies have reported the use of a tiered therapeutic approach in which nonsedating ASMs are added in succession until SE is controlled. 10,12 Many clinicians favor an approach which moves to IV anesthetizing ASMs after failure to treat established CSE with an initial BDZ and one nonsedating ASM (PHT, VPA, LEV, PB), but recent studies have raised concerns about the use of anesthetizing ASMs. Sutter et al 13 found greater complications in CSE patients receiving anesthetizing ASMs than those receiving only nonsedating ASMs. Others also reported greater complications with anesthetizing ASMs. 14,15,17 Kowalski et al 166 found that poor outcome and death were associated with the use of IV anesthetizing ASMs. As these were retrospective studies, selection bias likely affected the results. Our review found no strong evidence to support either a treatment approach which uses a series of nonsedating ASMs or the early use of an anesthetizing ASM for CRSE. Therefore, we focused our review solely on the evidence to support whether each individual ASM we examined was effective in terminating CRSE.
To our knowledge, no evidence-based comprehensive review has been published on these 8 treatments for CRSE, and no guideline exists on the optimal approach to treatment of this serious condition. Therefore, beginning in 2012, we examined the world’s literature regarding the treatment of CRSE. At the outset, we suspected that the strength of evidence for the ASMs chosen would be low, and the number of randomized controlled trials would be few. This proved to be correct, even as years passed after the start of this project. No class I or II randomized controlled trials have been performed on the treatment of CRSE. Nine class III and numerous class IV studies and case series have been reported. We found that for 7 ASMs (except LCM), insufficient or no evidence exists to support the use of these agents in the treatment of CRSE. We report those results herein. In addition, we reviewed reports on the use of ACTH, corticosteroids, IVIg, MgSO4, and pyridoxine as treatments for patients with highly refractory seizures and for special situations.
One prospective, single-blind, multicenter class III study sought to recruit 75 patients treated with PRO and 75 patients with PTB/THP. 134 Due to difficulties with low recruitment (even at the largest site), low frequency of eligible cases, and absence of funding in the United States, only 23 patients were treated in 3 years, so the study was halted prematurely. The difficulties with recruitment raise the concern that if an RCT on the treatment of CRSE is contemplated, the engagement of multiple centers and careful development of study methodology will be required. One pediatric and one adult RCT are currently underway for the treatment of CRSE with KET.
Several class I to III studies have now been performed on established CSE for the use of LEV, PHT, and VPA for SE persisting after first-line administration of a BDZ. Together, these studies show no consistent difference between these 3 ASMs as the second-line agent in established CSE, but they provide no direct evidence to guide health care providers regarding the most effective and safe third, fourth, or later ASM to be used for CRSE.
The methodology used for this comprehensive review has limitations. We did not have a single librarian conduct the literature search. Instead, a small number of taskforce members was assigned to each of the 13 medications, and these small groups conducted independent searches for each medication. As a result, it is possible that each small group did not conduct identical search strategies. In addition, some groups did not track the exact number of articles identified nor catalog the reasons for excluding them beyond relying on the inclusion and exclusion criteria listed in the Methods section. Finally, neither the Institute of Medicine Standards for Systematic Reviews, published in 2011, 167 nor the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement 168 were explicitly used when our methodology was developed in 2012. Our methodology and reporting meet most of the Institute of Medicine and PRISMA standards, but given these limitations, we consider this a comprehensive review rather than a systematic review.
The reference list below includes all articles cited in this review, but interested readers may wish to refer the online complete bibliography in which additional relevant articles are listed (Supplemental Appendix 1).
In conclusion, mostly insufficient evidence exists on the efficacy of stopping clinical CRSE using BRV, LCM, LEV, valproate, KET, MDZ, PTB, and PRO either as the last ASM or compared to others of these drugs. Adrenocorticotropic hormone, IVIg, corticosteroids, MgSO4, and pyridoxine have been used in special situations but have not been studied for CRSE. For the treatment of established CSE (ie, not RSE), LEV, VPA, and fosphenytoin are likely equally effective, but whether this is also true for CRSE is unknown. Triple-masked, randomized controlled trials are needed to compare the effectiveness of parenteral anesthetizing and nonanesthetizing ASMs in the treatment of CRSE.
Supplemental Material
Supplemental Material, COI-RSE-Submitted_w_Manuscript - Treatment of Refractory Convulsive Status Epilepticus: A Comprehensive Review by the American Epilepsy Society Treatments Committee
Supplemental Material, COI-RSE-Submitted_w_Manuscript for Treatment of Refractory Convulsive Status Epilepticus: A Comprehensive Review by the American Epilepsy Society Treatments Committee by David G. Vossler, Jacquelyn L. Bainbridge, Jane G. Boggs, Edward J. Novotny, Tobias Loddenkemper, Edward Faught, Marta Amengual-Gual, Sarah N. Fischer, David S. Gloss, Donald M. Olson, Alan R. Towne, Dean Naritoku and Timothy E. Welty in Epilepsy Currents
Supplemental Material
Supplementary_Appendix - Treatment of Refractory Convulsive Status Epilepticus: A Comprehensive Review by the American Epilepsy Society Treatments Committee
Supplementary_Appendix for Treatment of Refractory Convulsive Status Epilepticus: A Comprehensive Review by the American Epilepsy Society Treatments Committee by David G. Vossler, Jacquelyn L. Bainbridge, Jane G. Boggs, Edward J. Novotny, Tobias Loddenkemper, Edward Faught, Marta Amengual-Gual, Sarah N. Fischer, David S. Gloss, Donald M. Olson, Alan R. Towne, Dean Naritoku and Timothy E. Welty in Epilepsy Currents
Footnotes
Acknowledgments
The authors appreciate the assistance of Heidi Tibollo, RN, in the initial organization of the manuscript reference list.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Bainbridge: Advisor to Sunovion; research support from Supernus; research academic relationship with GW Pharma (July 2016-July 2018). Dr. Boggs: Research support from LivaNova, NeuroPace, Medtronic, UCB Pharma, Upsher-Smith, Marinus, Lundbeck, and Eisai; advisory panel for SK Life Science. Dr. Faught: Stock in Pfizer; consultant for Biogen, Eisai, UCB Pharma (2015-2020); Data/Safety Monitoring Boards for SK Life Science, SAGE (2015-2020); expert testimony for Alabama Board of Medical Examiners (2018-2019); research support as site PI for Brain Sentinel, UCB Pharma, Xenon Pharmaceuticals (2015-2020); consultant for University of Alabama Birmingham and Emory University; Chair, Treatments Committee, American Epilepsy Society (2015-2018); Chair, ILAE Task Force on Epilepsy in the Elderly (2017-2021); Pharmacy Core Committee, Epilepsy Consortium (2014-2020). Dr. Fischer: Research grant from Supernus. Dr. Gloss: Employed as the chair of Neurology at Charleston Area Medical Center; approximately 5% of practice is caring for patients who are in status epileptics; Paid evidence-based medicine methodologist for AAN for part of study period. Dr. Gual: Partial research fellow salary support from private Spanish Foundation, Fundación Alfonso Martín Escudero (2018-2019). Dr. Loddenkemper: Self: Physician performing EEG procedures and other electrophysiological studies and evaluating pediatric neurology patients for Boston Children’s Hospital and affiliated hospitals; Speaker honorarium from AES, American Academy of Neurology, and Grand Rounds at various academic centers; Speaker honorarium/travel support from 7th London-Innsbruck Colloquium on Status Epilepticus and Acute Seizures, American Epilepsy Society, University of Paderborn, American Clinical Neurophysiology Society, and various international centers or meetings; travel support from Lehman Foundation; device loans from Embrace, Smartwatch, Neuroelectrics, Sam-E, and Epitel; pending patent applications for seizure detection/prediction/epilepsy management; founder and consortium PI for Pediatric Status Epilepticus Research Group; investigator-initiated research grants from Eisai, Lundbeck, Mallinckrodt, and Upsher-Smith; research support from Acorda Therapeutics, American Epilepsy Society, Boston Children’s Hospital, CIMIT/DoD, CURE, Danny Did Foundation, Empatica, Epilepsy Foundation of America, Epilepsy Research Fund, Epilepsy Therapy Project, HHV 6 Foundation, NIH, PCORI, Pediatric Epilepsy Research Foundation, Pfizer, Sage, and Sunovion; other support (consulting, speaker, advisory board, travel, epilepsy research, patient online consultation, or other) from Advance Medical, Amzell, ANA, Danny Did Foundation, Dreifuss Penry Award, Eisai, Elsevier, Engage, Grand Rounds, Integritas, Lundbeck, Market Research, SEK, Stratis, Sunovion, Trivox, UCB, Upsher-Smith, and Zogenix; Associate Editor for Seizure; Associate Editor for Wyllie’s Treatment of Epilepsy, 6th ed and 7th ed; Board Member for AMBRET, American Board of Clinical Neurophysiology, and NORSE Institute; Council Member, Vice President, and President for American Clinical Neurophysiology Society. Spouse: Physician performing EEG procedures and other electrophysiological studies and evaluating pediatric neurology patients for Northshore Medical Center/UMass Medical Center/Boston Children’s Hospital. Dr. Naritoku: Speakers bureau for Sunovion, Eisai, and SK Life Science; advisory board for SK Life Science; site PI in clinical trial for Xenon (XPF-008-201). Dr. Novotny: Self: Honorarium and travel for UCB (2016); honorarium for Upsher-Smith Lab (2015); scientific advisory board with travel expenses for Zogenix (July 2019); investigator on pSERG (Pediatric Status Epilepticus Research Group) supported by PERF (Pediatric Epilepsy Research Foundation) (2017-present); investigator for Clinical Trials for Eisai (E2007-G000-236) (2019-2020); investigator with research support from Seattle Children's Research Institute (Molecular diagnostic of focal cortical dysplasias) (11/2018 - 12/2020); investigator for Brotman-Baty Institute of Precision Medicine at University of Washington (Collaborative proposal to accelerate gene discovery in pediatric and adult epilepsy surgery) (7/2019 - 6/2020); site PI for The Epilepsy Phenome/Genome Project (EPGP) (NINDS 5U01NS053998-04. Lowenstein, D) (5/1/2007-4/30/2012). Spouse: Salary support as investigator for The NIH Undiagnosed Diseases Network (9/2019 - 10/2024); salary support as Fellowship Program Director for NIH Medical Genetics Postdoctoral Fellowship (5 T32 GM007454 43); Institutional Review Board (IRB) member with paid travel for NIH All of Us Research Program. Dr. Olson: No relevant disclosures. Dr. Vossler: Research support to institution as PI on clinical trials for UCB Pharma, Sunovion, GlaxoSmithKline, Vertex, Accorda, Pfizer, Eisai, SK Life Science, and Biogen; consultant to or speaker’s bureau for UCB Pharma, Lundbeck, Eisai, Otsuka, Omeros, and Greenwich Pharmaceuticals. Dr. Towne: Supported by the U.S. Department of Defense and the Department of Veterans Affairs; grants from UCB Pharma, Congressionally Directed Medical Research Programs, and Brain Sentinel Inc.; research grant and speakers bureau for Allergan (for headache, not epilepsy). Dr. Welty: No relevant financial relationships.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The American Epilepsy Society provided administrative staff support and librarian assistance for preparation of this review.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.