
Abstract
This review compiles scientific data about the real dangers faced by people with epilepsy (PWE) who drive. Those include risks of motor vehicle accidents (MVA) in PWE as compared with controls (individuals without epilepsy) and as compared with persons with other medical conditions that impact fitness to drive. Data regarding Accident rates as related to seizure free intervals (SFI), single vs. multiple seizure events, and/or antiseizure drug (ASD) taper and reintroduction are discussed. Variation in state, national, and international laws and guidance for non-commercial and commercial drivers is highlighted, along with some related reasons for driving restrictions. The review concludes by emphasizing the importance of physicians educating patients about local driving laws and about risks of ASD non-adherence. The need for a broader, multi-stakeholder re-examination of driving regulations for PWE is noted.
Keywords
Epilepsy and Driving: Background
According to the World Health Organization, approximately 50 million people worldwide have epilepsy. 1 Seventy-three percent of people with epilepsy (PWE) have a driver’s license compared to 94% of the general adult population. 2 The ability to drive is a key measure in 2 of the Quality of Life in Epilepsy Inventories (QOLIE-89 and QOLIE-31). Despite the importance to individuals, granting or suspending driving privileges is the sole legal prerogative of the state, not clinicians. 3 Rules regarding driving in PWE vary among the US states. 4,5 Although fitness to drive might be threatened by many medical conditions, patients with neurological disorders feature prominently in such reports, and it is assumed that PWE are less fit to drive than those afflicted with some other medical conditions. 6 In general, rules aim to restrict driving by PWE who have greatest risk of having seizures while driving.
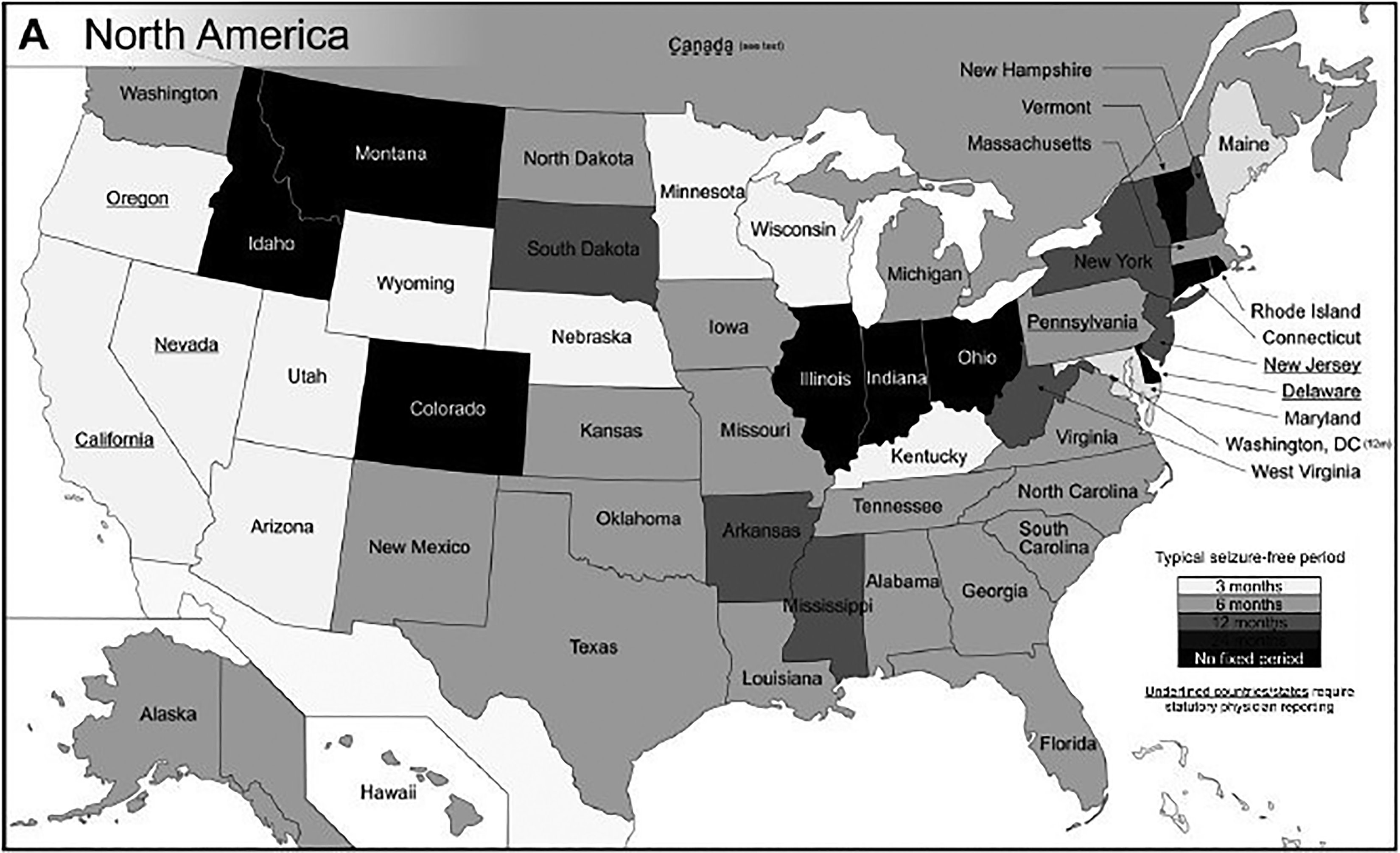
The last joint consensus statement regarding driving in epilepsy was published in 1994 by the American Academy of Neurology (AAN) and American Epilepsy Society and Epilepsy Foundation of America. This consensus statement recommends that in order to be able to drive PWE should have a SFI of at least 3 months, but PWE with focal aware seizures, consistent and prolonged auras, or nocturnal seizures may still drive on a case-by-case basis. 7 The Epilepsy Foundation’s state driving laws website tool can be used to inform individuals about the laws of each state. In addition, the Epilepsy Foundation provides a wall poster which provides an overview of each state’s seizure-free period requirement for the ability to drive, physician reporting requirements, and periodic medical update requirements. 5 The National Highway Traffic Safety Administration provides guidance to assist licensing agencies in making decisions about an individual’s fitness for driving. 8 Due to unique state laws and variable physician awareness regarding these, patients may receive the wrong advice regarding driving. 9,10 This could possibly result in patient noncompliance with recommendations. 11 Polychronopoulos et al 12 found that to maintain employment many patients are noncompliant with such restrictions.
In 2010, the AAN included driving and safety education as 1 of the 8 final quality improvement measures approved by the Physician Consortium for Performance Improvement. 13 It is therefore very important to review current, existing, evidence-based literature about driving and epilepsy.
Driving and Epilepsy: Are PWE More Likely to be Involved in Crashes? Facts Supported by Existing Literature
PWE are between 1.13 and 2.16 times more likely to experience a serious (one that requires an emergency visit to a health facility/causes death) MVA than controls. 14,15 PWE also have a 2.2-fold increased risk of pedestrian accidents, and 1.7-fold risk of bicycle accidents. 15 However, 8% to 18% of MVAs in PWE are related to a first seizure. 16 The causative risk factors for MVA in epilepsy are unclear. In PWE, the proportion of accidents due to an actual seizure versus a driver error is difficult to determine owing to the mixed instances of how these crashes are reported. Most studies to date indicate that the majority of MVAs are not due to a seizure. 15 A 1999 study by Krauss et al suggested that the strongest predictor of seizure-related crashes is the SFI. 17 An evidence-based review by Classen et al identified that in self-reported or proxy-reported crashes, epilepsy surgery (level B), SFI (6-12 months: level B), few prior seizure-related crashes (level B), and regular ASD adjustment (level B) are factors associated with a reduced risk of crashes. 18 For officially reported crashes, however, this same review concluded from 4 class II studies that PWE do not have increased crash risk compared to healthy controls but do have an increased risk when compared with other medical groups. According to the authors, this discrepancy is possibly related to potential underestimation bias because crash databases underestimate crashes as compared to insurance databases. The authors go on to remind readers that for their primary aim—assessing factors associated with officially reported crash and casualty—the 4 class II studies assessed were very heterogeneous with respect to age ranges, sample sizes, settings (in one study, the unit of analysis was a crash, while in another, the unit of analysis was PWE)—making generalizations to PWE difficult. In the discussion section, the authors caution readers to “continue with current recommendations for reporting and license restrictions as required by state guidelines” until studies that are more rigorous are published.
How Do MVA in PWE Compare to Other Medical Conditions Where Data Are Available, and Driving Might Be Restricted?
The published data in medical conditions such as diabetes, stroke/TIA, and dementia that might affect fitness to drive are riddled with the same concerns about self-reporting of data, nonuniform comparisons, and so on as noted in PWE and MVA. Overall, the risk of an MVA in diabetes is 30% higher than in nondiabetics. 19
In a 2019, systematic review of the risk of an MVA after stroke or TIA, only 1 of 3 case–control studies found an association between stroke and MVA (odds ratio: 1.9; 95% confidence interval [CI]: 1.0-3.9), while 2 of 4 cross-sectional studies using computerized driving simulators found a 2-fold increase in MVA risk in patients with stroke. 20 This review concluded that mixed evidence did not support robust increase in MVAs in stroke. 20 One study quoted a self-reported association between MVAs and Parkinson disease in 15% to 30% patients. 21 For patients with dementia, the risk of MVAs is felt to be 2 to 5 times controls. 22
Driving restrictions differ by medical conditions listed above and can be found by accessing local and national medical fitness guidelines for the condition in question. 8
What Is the Nature of MVA in PWE? How Does the ASD Choice Influence the Nature of MVA?
Several researchers have tried to elaborate on the nature of MVA in PWE. Neal et al 23 cross-checked 20 000 unique PWE in an Australian database for MVA as corroborated with medical records and police records and identified 62 patients involved in 71 crashes out of 288 PWE. These were compared to 137 126 nonseizure-related crashes in 220 975 drivers during the same time frame. Seizure-related crashes were noted in 52% (37/71), involved single vehicles (57% vs 29%), had a sole occupant (57% vs 16%), and were mostly with a fixed object (54% vs 17%).
In the study by Sundelin et al, 29 220 PWE were compared to 267 637 matched Swedish controls to study the association between epilepsy, ASDs, and serious MVA. 15 Serious MVA was defined as one associated with an emergency visit at a hospital or death. The use of newer versus older ASD (carbamazepine or oxcarbazepine monotherapy was compared to lamotrigine or levetiracetam monotherapy) did not influence the risk of serious MVA in population-level comparisons or within individual (PWE) comparisons. 15 Therefore, while counseling PWE concerning driving, one might emphasize the importance of taking ASDs regularly over the specific choice of ASD to limit seizures and risk of serious car crashes.
What Proportion of Fatal MVAs in PWE Are Seizure Related?
Of all fatal MVAs, only 0.1% to 0.2% are seizure related compared to 30% that are alcohol related. 24
What Are the Data Regarding SFI, Risk of Recurrent Seizures, and Fitness to Drive?
Seizure-free interval in the context of driving is that time period of seizure freedom after which the risk of seizure recurrence is low enough to make driving safe. 25 In the United States, this time period varies from 3 to 12 months depending on individual state laws. 4 State restrictions do not distinguish between PWE with a single seizure versus repeated seizures. This is important in the context of the new International League Against Epilepsy definition of epilepsy which includes a single seizure with a 60% risk of recurrence in the ensuing 10 years. 26 Seizure-free interval is the most important measure in determining fitness to drive. 27
Risk of Recurrent Seizures After a Single Event
In the European Union, PWE are allowed to drive after a single seizure, if seizure-free for 6 months after the event and if their risk of seizure recurrence within the next 12 months is less than 20%. The rate of seizure recurrence after a single unprovoked seizure in an adult is highest in the first 1 to 2 years with greatest risk (32%) in the first year as compared to 46% at 5 years according to the recent evidence-based guideline about management of a first unprovoked seizure in an adult. 29 In a study by Bonnett et al, among patients with first seizure who started an ASD, after an initial 6 month of seizure freedom, the risk of subsequent seizure recurrence is 14% after 12 months (95% CI: 10%-18%), and 7% after 24 months of seizure freedom (95% CI: 3%-10%). 30,31 These same studies also identify risk factors for recurrent seizures after an initial 6 month of seizure freedom. Risk factors for unmedicated patients with a “non-remote” symptomatic etiology for seizures are an abnormal magnetic resonance imaging and electroencephalogram (EEG; epileptiform discharges) and for patients with remote symptomatic etiology: an abnormal EEG.
Reprinted with permission 28
Risk of Crashes After Multiple Seizures
Between 20% and 30% of PWE with poorly controlled seizures continue to drive. 32,33 In Krauss’ case–control study of PWE with crashes and PWE not involved in crashes, having a good driving record with low accident rate, optimizing therapy with ASDs, and consistent and reliable auras before a seizure could reduce but not completely eliminate the excess risk of crashes. 17 Overall, this same study found that in PWE, the risk of accident was reduced by 85% in patients with >6 months of seizure freedom, and by 93% in patients with >12 months. 17 A recent Australian study found that although 20% of individuals with epilepsy had a crash prior to a diagnosis of epilepsy, 19% of seizure-induced crashes were due to noncompliance once ASDs were prescribed. 23 Nonadherence to ASDs does have a higher incidence of MVA injuries (incidence rate ratio = 2.08, 95% CI = 1.81-2.39) than periods of adherence. 34
Risk of Seizures After ASD Taper
Currently, there are no laws regarding driving restriction during or after ASD taper, but 80% of epilepsy specialists in the United States would advise PWE to not drive for 3 months after a drug taper. 35 In the United Kingdom, PWE are advised to not drive during drug withdrawal and for 6 months after a taper. The only research done in the setting of driving was the Medical Research Council ASD withdrawal study involving 1021 PWE. 36 Results indicate a risk of 30% for seizure recurrence over 12 months immediately after drug withdrawal. This and other studies that only look at seizure recurrence in PWE after drug withdrawal 37 ; indicate decreasing risks with longer SFI: from 7% to 19% at 3 months, to 6% to 16% after 6 months, and to 4% to 12% after 12 months. 38 In the case of seizure recurrence—with reinstitution of ASDs, the risks of seizure recurrence with SFI at 3, 6, and 12 months are 26%, 18%, and 17%, respectively. 36
International Experience
Although an exhaustive review of the driving regulations among foreign countries is beyond the scope of this article, some are reviewed here. For example, the Australian National Transportation Commission provides guidance stating that individuals with epilepsy may drive if they are responsible individuals with well-managed seizures. 39 Well-managed epilepsy is defined as an appropriate seizure-free period and medication and/or treatment compliance.
The Canadian Council of Motor Transport Administrators (CCMTA) Medical Standards for Drivers and the Canadian Medical Association (CMA) both provide excellent guidance for assessing driving privileges. 40,41 The CMA and CCMTA guidelines state that a noncommercial driver with newly diagnosed epilepsy with 6 months of no seizures can generally be allowed to drive a car. The United Kingdom requires a 6- to 12-month SFI before an individual may resume driving. 42
The International Bureau for Epilepsy’s Driving Regulations Task Force provides a list of European countries that do and do not have driving regulations with respect to epilepsy and driving. 43
Commercial Driving
In the United States, restrictions for individuals with seizures or epilepsy are stricter for commercial drivers than for drivers of personal vehicles. Regulations may be different for interstate versus intrastate commercial driving, depending upon the state. For interstate trucking, federal law supersedes state laws [49 CFR 391.41(b)(8)]. The US Federal Motor Carrier Safety Administration (FMCSA) provides a guideline for obtaining and maintaining a commercial driver license (CDL) for those with epilepsy:
A history of epilepsy precludes an individual from obtaining unconditional certification to drive a commercial motor vehicle (CMV) for the purposes of interstate commerce.
A history of epilepsy, however, should not unconditionally exclude all individuals from driving a CMV; conditional certification may be possible in some instances.
An individual with a history of epilepsy may obtain conditional certification (or maintaining certification under conditional status) to drive a CMV if that individual meets the following criteria: Individual must have been seizure-free for a minimum of 8 years on or off ASDs; AND If all ASDs have been stopped, the individual must have been seizure-free for a minimum of 8 years from the time of medication cessation; OR If still using ASD, the individual must have been on a stable medication regimen for a minimum of 2 years. Recertification for drivers with epilepsy should be performed every year.
The US Department of Transportation, FMCSA does provide a CDL interstate driving Seizure Exemption Application form for those who have been seizure-free for 8 years or have had a one-time seizure event. The FMCSA medical programs division can be reached at 1-202-366-4001 or
In 2017, the FMCSA received applications from 6 individuals requesting exemption regarding the regulations regarding PWE to drive in interstate commerce (Docket No. FMCSA-2017-0254). This exemption was granted in 2018 and allows for such individuals who are taking ASD to operate CMVs in interstate commerce. 44,45
Conclusion
Driving restrictions may be inevitable for some PWE. A 10-year follow-up of individuals with childhood-onset epilepsy shows that those with uncomplicated epilepsy have lower rates of obtaining a driver’s license than a healthy cohort despite the legal eligibility to drive. 46 Although Drazkowski et al 47 found that reducing the driving restrictions from 12 to 3 months in Arizona did not change the incidence of MVA, it is of great importance that physicians educate patients on the local driving laws and risks of ASD nonadherence. It may be time to reexamine driving regulations, but clearly this is a much larger project that involves multiple stakeholders.
Footnotes
Acknowledgment
The authors are very grateful to Heidi Tibollo BSN, MLS who helped with the literature search and references quoted in this manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The following authors disclosed financial or non-financial relationships with a commercial or non-commercial entity: C. Joshi: Advisory board meeting for Zogenix; PI with institutional contract research support from GW Pharmaceuticals; clinical practice includes 14 weeks per year of reads routine and video EEGs.
M. Spanaki: Advisory Board for SK Life Science; A. Towne: Research: 1) Investigator, Chronic Effects of Neurotrauma Consortium (CENC) Award. Study 1: Observational study on late neurologic effects of mTBI in OEF-OIF Veterans, Department of Defense. 2014-present; 2) Principal Investigator, Detecting PNES with single-Channel sEMG, Brain Sentinel, Inc. 2017-present; and 3) Epidemiology of Epilepsy and Traumatic Brain Injury: Severity, Mechanism, and Outcomes, CDRMP (Foundation for Advancing Veterans’ Health Research). 2017-present.
D. Vossler: Consulting for SK Life Science; Speaker bureau/honoraria for UCB Pharmaceuticals and Sunovion; institutional contract research support from Pfizer, SK Life Science, Biogen, Eisai, and UCB Pharma.
J. Drazkowski reported no financial or non-financial relationships with a commercial or non-commercial entity.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.