
Abstract
Introduction:
Biosafety and biosecurity play increasingly important roles in global health security. Although many countries have established national policies to govern these practices, the existence of regulation does not guarantee its application or stronger biosecurity in practice.
Methods:
We analyzed survey data collected from biosafety and biosecurity practitioners in > 40 countries. An institutional-level biosecurity implementation index was developed and aligned with country-level Global Health Security (GHS) Index scores to construct a policy–practice gap (PPG) index. Descriptive analyses and multivariable regression models were used to assess variation in implementation and to identify factors associated with implementation scores.
Results:
High-income countries had policy development outpacing institutional implementation (PPG mean = 23.5). In contrast, low- and middle-income countries obtained higher implementation scores than their national policy frameworks (PPG mean = −35.7). The study also identified areas requiring greater attention to implementation, including psychological programs for personnel vetting, cross-border transfer, end-use transfer, and cybersecurity. Multivariable analyses showed that experience working in high-containment laboratories, engagement in international collaboration (β = 6.9, p < 0.05), access to high-quality training (β = 2.3, p < 0.05), and adequate institutional financial support (β = 3.51, p < 0.05) were positively associated with implementation index. The magnitude and significance of these associations varied between U.S.-based and non-U.S. respondents.
Conclusions:
These findings help to understand the differences between national biosecurity policies and implementation across many countries. It shows the limitations of policy-only approaches to strengthening global biosecurity and informs future efforts to address some specific biosecurity practices.
Introduction
Biosecurity is one of the fundamental elements of pandemic prevention and global health security. 1 The concept of biosecurity has evolved significantly since 1980, when it was primarily associated with agriculture and pest control. However, it has gradually expanded into public health, laboratory regulation, and national security. 2 Biosecurity now involves protecting against biological weapons, bioterrorism, and concerns about pathogen release, theft, and misuse.3–5 During the late 20th and early 21st centuries, events such as the 2001 anthrax attacks in the United States, the emergence of severe zoonoses such as severe acute respiratory syndrome, highly pathogenic avian influenza A, and Middle East respiratory syndrome and an increasing number of high-containment laboratories 6 accelerated recognition of biosecurity as not only an agricultural or animal health issue 7 but as a multidisciplinary global health challenge.
Biosafety and biosecurity are related but distinct concepts. 2 While biosafety focuses on the laboratory practices that prevent unintentional exposure to biological hazards,7,8 biosecurity emphasizes measures to prevent the unauthorized access, misuse, loss, theft, diversion, or intentional release of biological agents and toxins and related materials. 9 Despite having different definitions, they are complementary to each other. 7 Biosafety is therefore mentioned in this article to support the meaning of biosecurity in laboratory environments.
Research and governance in biosecurity are widely recognized as an area of interest, following recognition that mismanagement, misuse, or accidental release of biological materials could have global implications.10–14 Laboratory incidents, whether through human error, inadequate containment, insufficient oversight, or other causes, can escalate and have the potential to trigger infection outside the laboratory and potentially large-scale outbreaks. 10 For example, a 2014 modeling study using the Centers for Disease Control and Prevention (CDC) data on laboratory-acquired infections (LAIs) estimated that under the worst scenario of both lab escape probability and transmission, research with potential pandemic pathogens over a decade could carry up to 27% probability of seeding a global pandemic. 13 Other empirical evidence supports this concern: A comprehensive review of LAIs and accidental pathogen escapes (APELs) from 2000 to 2021 identified 309 documented LAIs and 16 APELs, several of which were associated with community-level transmission. 14 These findings illustrate that even rare laboratory failures have the potential to pose significant public health impacts. Some suggestions to improve biosafety and biosecurity include minimizing the number of high-containment laboratories, reducing the number of people handling dangerous pathogens, and implementing nonpunitive incident reporting for shared learning.15,16
The rapid advancement of biotechnology in the 21st century has also elevated the dual-use potential associated with life sciences. Emerging capabilities in gene editing and artificial intelligence-driven biodesign have increased concerns about the feasibility of creating or modifying pathogens outside traditional institutional settings.17,18 At the same time, the Global Biolabs 2023 report 6 identified 51 operational Biosafety Level 4 (BSL-4) laboratories and 18 additional facilities under planning or construction, including 12 established or proposed since the onset of COVID-19. The increase in high-containment labs raises concerns about possible accidents and releases from these facilities.
Despite its importance, biosecurity remains one of the least empirically assessed dimensions within global preparedness frameworks. While it is included in the Prevention category of the Global Health Security (GHS) Index, 1 data on the actual implementation of biosecurity measures are scarce. Many low- and middle-income countries (LMIC) report minimal capacity in this domain, and in some countries, the concept is still developing in national health governance. 1 Biosecurity is often perceived as a concern of high-income countries (HICs) with advanced technology and research infrastructures, which may result in uneven global adoption and oversight.19,20 In an interconnected world shaped by globalization, scientific collaboration, and international trade, these disparities can create vulnerabilities as pathogens or materials originating in one place can easily affect others. In addition, the existence of policy frameworks does not guarantee implementation fidelity. The translation of biosecurity policy into institutional practice remains uncertain and leaves a gap in the understanding of how biosecurity is managed and implemented nationally and globally.
The GHS Index was designed to provide a standardized, transparent, and evidence-based assessment of countries’ capacities to prevent, detect, and respond to infectious disease threats. 1 It evaluates 195 countries across six core domains considered pillars of pandemic preparedness: prevention, detection and reporting, rapid response, health system, compliance with international norms, and risk environment. Within these domains, the Index aggregates 37 indicators and 96 sub-indicators, each normalized, weighted, and combined into an overall preparedness score (0–100 range).The GHS Index has been a popular metric used in comparative analyses of national pandemic preparedness and performance.21,22 Studies have examined its relationship with diverse health outcomes, including COVID-19 case fatality rates,23–25 vaccination coverage, 24 and response speed. 19 The GHS Index primarily captures the existence of official policies, plans, and regulations; however, it may not fully represent the effectiveness of implementation, institutional coordination, or public compliance. Thus, formal capacity is not always aligned with capability.1,23,24 The actual governance of biosecurity depends on how these policies are interpreted, enforced, and practiced within laboratories and research institutions. 26 In the U.S, for example, a series of policies 27 including the 2012 U.S. Government Policy for Oversight of Life Sciences Dual-Use Research of Concern (2012 Federal DURC Policy), 28 the 2014 United States Government Policy for Institutional Oversight of Life Sciences Dual-Use Research of Concern (2014 Institutional DURC Policy), 29 the 2017 HHS Framework for Guiding Funding Decisions About Proposed Research Involving Enhanced Potential Pandemic Pathogens (2017 HHS P3CO Framework), 30 and the recently rescinded 2024 OSTP Policy for the Oversight of Dual-Use Research of Concern and Pathogens with Enhanced Pandemic Potential (DURC/PEPP Policy), 31 establish mechanisms to mitigate the risks of research involving pathogens. Globally, the World Health Organization (WHO)’s Laboratory Biosecurity Guidance 32 and related international standards were widely adopted from countries without clear and standardized oversight systems. Despite these policies, little is known about how effectively and consistently biosecurity frameworks are implemented across institutions and countries.
To address this challenge, this study provides the first empirical cross-national assessment of biosecurity implementation at the working level. Using survey data collected from biosafety and biosecurity practitioners in >40 countries, the study examines the degree of awareness, oversight, and implementation of biosecurity practices. By aligning individual implementation data with their country’s GHS biosecurity score, we develop a policy–practice gap (PPG) score that quantifies discrepancies between policy capacity and implementation.
Although the dataset covers a limited number of countries, this analysis represents an important first step toward understanding how biosecurity frameworks are translated into practice. The findings contribute to both theory and policy by (1) empirically validating whether formal biosecurity capacity corresponds with implementation realities and (2) identifying specific factors that may influence the implementation. This study seeks to strengthen the evidence base for evaluating biosecurity implementation and to inform future efforts to align policy design with practical application in support of public health and pandemic prevention.
Methods
Study Design and Participants
This study draws on data collected through an online survey of biosafety and biosecurity professionals conducted in 2025. Participants included individuals with past interactions with the authors, biosafety practitioners affiliated with the American Biological Safety Association International (ABSA International), and individuals listed as Institutional Biosafety Committee contacts with the U.S. National Institutes of Health Office of Science Policy. To broaden the geographic reach of the survey, the study team also conducted targeted outreach to biosafety and biosecurity organizations and professional networks in multiple regions, including Latin America, Africa, and Asia. Representatives of these organizations were asked to distribute the survey link within their professional communities. Despite these efforts, responses were more represented among professionals in the United States or those connected to international biosafety networks. As a result, the sample likely reflects the perspectives of internationally engaged biosafety professionals rather than the full diversity of laboratory contexts worldwide.
This project was approved by the Institutional Review Boards at University of Nevada, Reno (IRB no. 2330367) and Arizona State University (IRB no. 00016457).
Eligible participants were 18 years of age or older and provided informed consent before participating. Respondents were permitted to skip questions or select “I don’t know” or “Prefer not to answer” for any questions; therefore, completion rates varied across survey questions.
A total of 395 responses were received from individuals in 57 countries. Among these, 298 respondents (75%) completed the full survey and were retained for analysis. To focus the analysis on those with relevant professional responsibilities, only participants who reported having biosecurity-related duties were included, resulting in a final sample of 222 participants from 44 countries (see Supplementary Figure S1 for exclusion flow diagram).
Implementation Index
Nine different biosecurity practices, which were assessed in the WHO Guidelines for Biosafety and Biosecurity, 32 were used to contribute to one composite implementation index, which provides a summary measure of overall institutional implementation. These practices were chosen to mirror the key biosecurity policy domains measured by the GHS Index.
Respondents were asked about the implementation of these biosecurity practices at their workplace. Responses were converted into binary variables for index construction (“Yes” = 1, “No”/“I don’t know”/NA = 0). This approach provides more conservative results for the implementation index. When evidence of implementation is uncertain, the capacity is recorded as being absent. Coding “I don’t know” and NA responses as 0 ensures that the implementation index reflects only confirmed presence of biosecurity practices and avoids inflating scores due to uncertainty or lack of awareness. Although this method likely underestimates true implementation, it provides a cautious approach for cross-country comparison. The biosecurity practices included in the implementation index and their weights for calculating the final score are presented in Supplementary Table S1. The implementation index was calculated for each respondent by averaging the binary-coded items across all biosecurity indicators and scaling the result to a 0–100 range.
To assess the index’s internal coherence, we examined the correlation across the individual practices. The results show generally positive associations between these practices (see Supplementary Table S2), which means the institutions reporting the presence of one practice tend to report the presence of another practice. Correlation ranged from 0.1 to 0.46; therefore, the practices are weakly to moderately correlated, but still represent distinct dimensions of biosecurity implementation.
Gap Index
The policy–implementation gap is calculated on an individual level using the GHS Biosecurity Index (see Supplementary Table S3 for its categories) and the newly constructed implementation index.

A positive gap indicates that national biosecurity policy capacity exceeds implementation at the institutional level. On the contrary, while a negative gap suggests that implementation is stronger than formal policy recognition, there are several ways to interpret this gap. It may indicate that institutions have adopted biosecurity practices that go beyond the requirements established by national policy, a commitment to implementation in countries having policy framework in place. However, in countries where national biosecurity governance is limited, the negative gap shows that national policy frameworks have not yet caught up with practices already implemented at the laboratory level. The higher implementation score could also be driven by international collaborations, funder’s requirements, or participation. Therefore, the negative gap was not only shaped by domestic policy environments but also by external standards via collaboration and cross-border learning. In addition to the direction of the gap, the magnitude of the gap reflects the degree of divergence between policy and practice.
Determinants of Implementation Index
In an effort to understand the factors having an impact on implementation, there are three levels of factors that were examined in this study. They are national factors, institutional-level factors, and individual-level factors. Detailed variables and their coding schemes are summarized in Figure 1, with additional questionnaire details for individual-level factors provided in Supplementary Table S4.

Three levels of factors of implementation index and their coding schemes. BSL, Biosafety Level; GHS, Global Health Security; HICs, high-income countries; LMICs, low- and middle-income countries.
Statistical Analysis
Independent Student’s t-test or analysis of variance (ANOVA) was conducted to assess the difference of implementation index and gap index among multiple factors including the country income level, the existence of the BSL-3/4 at national and institutional levels, and the institution categories. Prior to these tests, the data were examined for normality and equality of variances to ensure the validity of the analysis. Normality checks were performed to confirm that the distributions were approximately normal, even in cases of large differences among groups or small sample sizes.
A multivariable analysis was then performed to identify determinants of the implementation index. The dependent variable was the implementation index, while the independent variables included national-, institutional-, and individual-level factors (Figure 1). Because a large proportion of respondents were from the United States, which could skew the results toward HICs and U.S.-specific trends, three linear regression models were conducted: one including all respondents, one limited to U.S. respondents, and one excluding them. For the models including all and non-U.S. respondents, an analysis of covariance framework, ANCOVA, was run to test for differences in country income while controlling for remaining factors. Multicollinearity among predictors was also assessed, using the variance inflation factor (VIF). Other predictors had VIF <5, showing the low correlation. The GHS index score has VIF of around 5, indicating the moderate correlation since it may be correlated with the country’s income level. Because these predictors represent distinct dimensions of national capacity and VIF was below the threshold used for severe multicollinearity,33,34 we decided to keep them in the model. The detailed VIFs were presented in Supplementary Table S5. All analyses were conducted in SAS, with the significance level set at 0.05.
Results
Of 222 respondents of the survey, 137 (61%) were based in the United States, followed by a smaller number of people from other countries in North America and Europe. In contrast, representation from Asian and African regions was limited, with only 13 people from South and East Asian countries and 18 from sub-Saharan African countries.
The geographic imbalance likely reflects the global distribution of biosafety and biosecurity professional networks used in this survey. Biosecurity development has been concentrated in North America and Europe, where formal governance frameworks, research institutions, and professional societies (e.g., ABSA International, European Biosafety Association) have long been established. Existing surveys of biosafety and biosecurity professionals have also reported a high proportion of U.S. respondents. 35 It is also consistent with the concentration of high-containment laboratories and research institutions in the world.6,36
Demographic characteristics were diverse: Participants were approximately gender balanced. The majority were between 40 and 59 years of age and reported >15 years of professional experience. For a more detailed summary of the demographics of respondents, see Table 1.
Descriptive summary of survey participants

Implementation Index Result
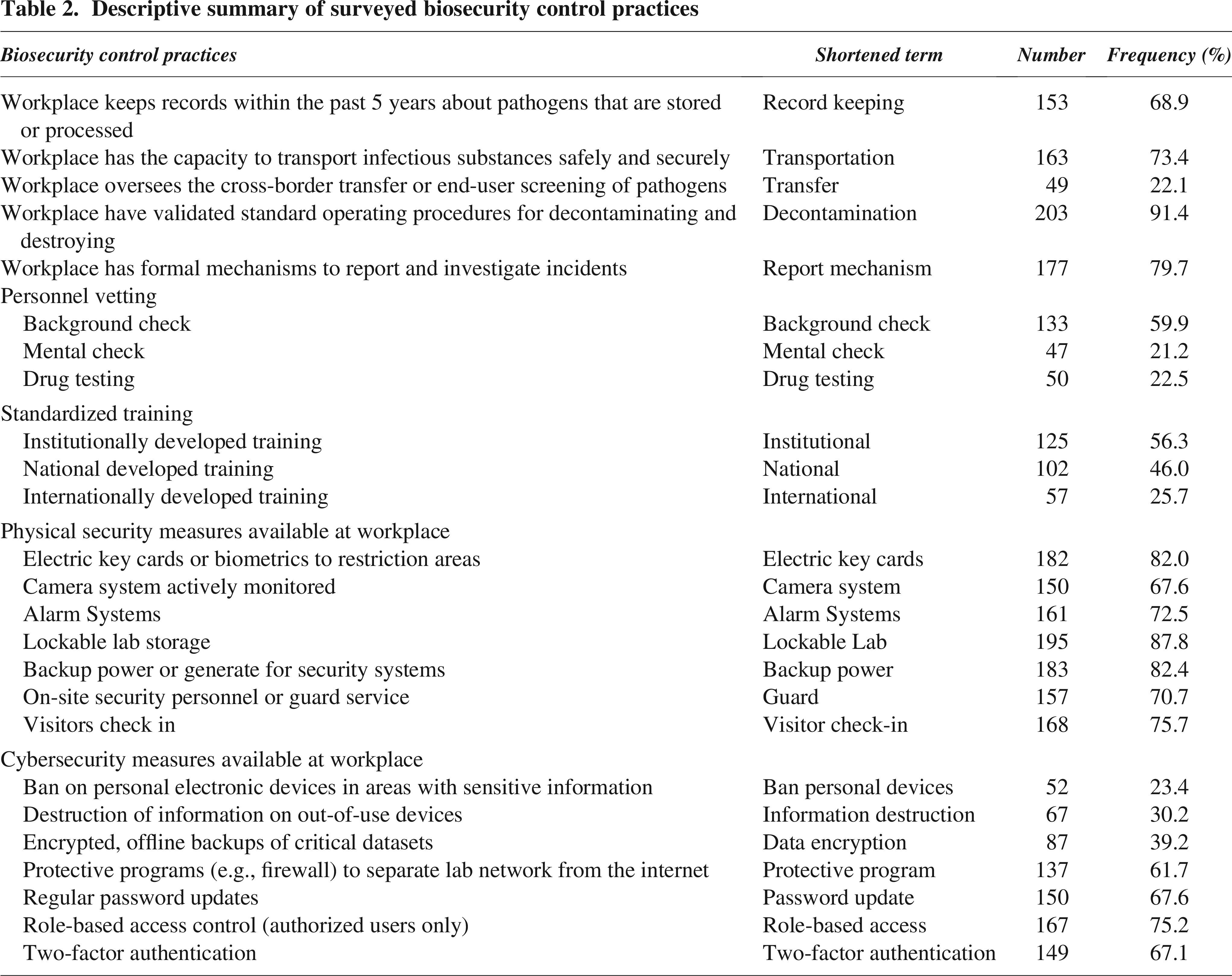
Nine biosecurity practices were examined, and respondents reported relatively high adoption of several core control measures. Most workplaces had validated procedures for the decontamination and destruction of pathogens (91.4%) and established formal mechanisms for incident reporting (79.7%). A high proportion also maintained secure transportation capacity for infectious substances (73.4%) and pathogen record-keeping within the past 5 years (68.9%). However, only 22.1% reported having oversight mechanisms for cross-border transfer and end-user screening, indicating limited engagement in international transfer control. Institutions from both HICs and LMICs showed similar levels of implementation of these biosecurity practices, although the percentages were generally higher among HICs (see Figure 2).

Percentage of survey participants adopting biosecurity practices at their institution by country income level.
Personnel reliability measures showed substantial variation. While background checks were conducted in 59.9% of workplaces, only about one-fifth performed mental health evaluations (21.2%) or drug testing (22.5%). Training programs were more commonly developed at the institutional (56.3%) or national (46.0%) level, whereas only 25.7% of respondents participated in internationally developed training. This pattern highlights a reliance on internal or country-specific training rather than globally standardized approaches. Notably, when disaggregated by country income, LMIC respondents reported a much higher rate of international training participation (58.6%) compared with 13.5% among HIC respondents. Conversely, a greater proportion of respondents from HICs reported receiving institutionally standardized and nationally developed training (Figure 2).
Physical security measures were widely implemented across workplaces, with most maintaining controlled access, monitored systems, and secure storage for sensitive materials: adopted by >60% of respondents. In contrast, cybersecurity measures were only moderately adopted, emphasizing access control (75.2%) and password protection (67.6%) but showing weaker implementation of data encryption (39.2%), information destruction (30.2%), and device restrictions (23.4%). Detailed frequencies for each measure are presented in Table 2. Although the overall difference in implementation between physical security measures was generally small (within 25%) across income groups, cybersecurity measures displayed a clearer disparity (up to 47%), with higher adoption rates among HICs than LMICs, particularly for two-factor authentication, information destruction, and protective programs.
Descriptive summary of surveyed biosecurity control practices
The biosecurity implementation index that was constructed from these measures ranged from 6.2 to 97.5, with a mean of 60.3. The resulting gap index averaged 6.3, with a wide range from −97.5 to +81.9, highlighting substantial variability in the alignment between biosecurity policy and implementation.
Differences in Indices
Analysis of the implementation index revealed no significant difference when comparing respondents by country income group and workplace category. However, when focusing on the presence of high-containment facilities (BSL-3/4) at a national and institutional level, a significant difference emerged. Respondents who worked in countries or institutions having BSL-3/4 reported substantially higher implementation scores (see Table 3). This indicates that research infrastructure and operational risk level are important factors of biosecurity implementation, more than national income status or general institutional categories. Interestingly, the presence of BSL-3/4 laboratories at the country level (F = −2.3, p < 0.05) corresponded with less significant differences in implementation scores, compared with the presence of these laboratories at the institution level (F = −6.9, p < 0.001).
Differences of implementation index and gap index by multiple categories

Represents one-way analysis of variance test.
*p < 0.05, **p < 0.0001.
BSL, Biosafety Level; LMIC, low- and middle-income country.
In contrast, the PPG index showed significant differences across multiple national and institutional factors. HIC had a positive gap (M = 21.5), while LMIC had a negative gap (M = −36.2), indicating a difference across income levels (F = 12.5, p < 0.0001). HIC experienced positive gap indices, suggesting that policy development has outpaced institutional implementation, while countries in other income groups displayed negative gap indices, meaning that institutional implementation levels exceeded national policy frameworks. Countries with BSL-3/4 exhibited higher gap scores (M = 10.2) compared with those without (M = −37.9; p < 0.0001). Similarly, significant variation was observed across workplace categories (F = 8.6, p < 0.0001), with public and private academic institutions showing higher gap scores (M ≈ 17) compared with government-related institutions (M = –11.7). Respondents working in BSL-3/4 facilities also reported a smaller gap (M = 1.1) than those not working in such facilities (M = 12.51; p < 0.05).
Biosecurity Implementation Index Prediction Model Result
Multiple linear regressions were conducted using the full sample, including nine variables across different levels, to identify factors associated with the biosecurity implementation index. The overall model was significant, explaining 40% of the variance in the outcome. National-level variables were not significantly associated with the implementation score. In contrast, institutional-level factors, including the presence of high-containment laboratories and international collaboration, were positively associated with the implementation index. Institutions with high-containment laboratories scored ∼11.4 points higher on the implementation index than those without, and institutions engaged in international collaborations scored ∼6.9 points higher than those without such collaborations.
At the individual level, respondents who reported more frequent training updates and greater financial support also demonstrated higher implementation scores, indicating that continued training and sufficient resources contribute to stronger biosecurity practices. When the sample was stratified into U.S. and non-U.S. respondents to account for the large representation from the United States, the impact of the national-level variable remains the same. The presence of high-containment laboratories continued to be a significant predictor in both groups. Financial support remained significantly associated with implementation among non-U.S. institutions but not among U.S. institutions, whereas international collaboration was a significant predictor only within the U.S. group (see Table 4). ANCOVA test controlling for country’s income category found no significant difference in the implementation index between these groups, and key predictors are still associated with implementation, showing the observed association is not solely driven by income differences or a large proportion of U.S. respondents.
Multivariable analysis of implementation index

*p < 0.05.
SE, standard error.
Discussion
This research examined which biosecurity practices are implemented at different institutions around the globe. It also identified measures that could contribute to increased biosecurity implementation. Several biosecurity practices were well adopted in both HICs and LMICs; however, some variations were observed across practices and income-level contexts. Biosecurity on cross-border transfer and end-user screening is adopted at a low rate, raising concerns about accountability for the movement and use of biological materials globally. The limited implementation of end-user screening may also leave institutions and nationals vulnerable to malicious actors who might obtain and misuse biological materials without identity and intention verification.
Among the personnel vetting practices, background checks were reported by more than half of workplaces, while drug testing and mental health checks are implemented less frequently. Only 28% of respondents working in BSL-3/4 reported psychological or mental fitness screening. Some historical incidents 10 have shown how the stress of individuals working in the high-containment labs can contribute to serious security breaches. 37 This raises the question of whether there should be increased investment in personnel vetting, mental health assessments, and employee wellness programs in high-risk working environments. At the same time, the absence of such measures should not automatically be interpreted as weak biosecurity practices. The implementation of some personnel vetting practices can often be shaped by cultural norms, legal constraints, or ethical controversy and therefore varies across countries and institutions.
LMICs tended to rely on internationally standardized training for their biosecurity practices. This training adoption could result from past global efforts in training development for low-resource countries, motivating more targeted support for these countries. The physical security measures were generally well established across settings because many biosecurity frameworks have focused primarily on physical containment and material control. However, the rapid expansion of digital laboratory systems, genomic sequencing, and synthetic biology has increased the importance of protecting sensitive biological data.38–42 As a result, cybersecurity is becoming a central component of biosecurity risk governance. In this study, compared with physical security, cybersecurity was less implemented across institutions in all income settings. This pattern may point to broader systemic vulnerability as biosecurity governance was attempting to adapt to digitalized research environments and the rapid change of technology. Cybersecurity risk and biological risk are often governed by different agencies 43 and therefore may create ambiguity in how and what data should be shared across institutions and nations.43,44 The growing international collaboration may amplify these cybersecurity concerns. Consistent with these observations, respondents reported moderate concern regarding cybersecurity risks, misuse, or loss of control of shared biological data (mean ≈ 3.6 on a 5-point Likert scale with 5 as most concerned).
This analysis also provides empirical evidence to quantify the discrepancy between respondents’ implementation and their own policy. The results show that the gap index varies across multiple dimensions, including national income level, the existence of high-containment laboratories in the nation, institutional categories, and whether the respondents’ workplaces operate BSL-3/4.
HICs exhibited positive gap scores, suggesting stronger policy frameworks relative to implementation, whereas LMICs showed negative gaps, implying that institutional practices may, in some cases, outpace national-level governance. The gap index for LMICs is particularly noteworthy. Institutions in these settings appear to be adopting biosecurity measures more rapidly than their national governance structures (see Figure 3 for the distribution of respondents’ implementation score across policy index by income group). Among the nine respondents from low-income countries, eight reported working in institutions with BSL-3/4. Among 60 responses from LMIC, 78% of responses indicated collaboration with international partners, most often with institutions in the United States, Europe, or regional entities in Africa, Southeast Asia, or the Middle East and North Africa, where biosecurity standards could be higher, and policies are more mature. This result may indicate the influence of international funding mechanisms, cross-border collaborations, and commitment to global frameworks, such as the WHO’s biosafety and biosecurity guidance. This collaboration may require recipient institutions to comply with donor or partner-country standards, therefore facilitating the adoption of biosecurity practices in places with a lack of domestic regulatory systems.

Distribution of individual respondents across country level GHS Index scores and their implementation scores, stratified by income group. The figure displays the composite implementation index for each respondent alongside the GHS Index score of their respective country. Respondents are categorized by national income level as either HICs or LMICs. The plot is divided into four quadrants representing combinations of national policy strength and institutional implementation: High Policy–High Implementation, Low Policy–High Implementation, Low Policy–Low Implementation, and High Policy–Low Implementation.
On the contrary, HICs demonstrated strong governance, funding resources, and well-established oversight frameworks, which have led to more comprehensive policy systems. In the United States, more attention has been paid to biosecurity and bioterrorism. This has led the path to the creation of many oversight mechanisms. Future frameworks on gain-of-function research are also under development, following the 2025 Executive Order for Improving the Safety and Security of Biological Research. 45 Despite this continuous policy evolution and national commitment, consistent implementation remains a challenge. Institutions not directly engaged in dual-use or high-containment research often apply fewer biosecurity measures, contributing to a larger positive gap between policy and practice. Many biosafety and biosecurity practitioners in the United States reported tension between regulatory compliance and operational constraints, noting that federal guidance can sometimes lack clarity or consistency over time.11,26 These practical limitations demonstrate that no single oversight model fits all institutional settings. Effective biosecurity governance requires a balance between national-level policy coherence and institutional capacity and flexibility, so that both high-containment research facilities and routine laboratories are able to maintain appropriate levels of biosecurity implementation.
The sample is skewed toward U.S.-based and internationally connected respondents, with limited representation from LMICs. This imbalance may have influenced the observed differences between HICs and LMICs. In particular, LMIC respondents in this study may disproportionately reflect institutions engaged in international collaboration or external partnerships, which, in our sample, were common among LMIC participants. Such institutions may have greater access to resources, training, and externally driven standards and therefore may not be representative of the broader institutional landscape within their countries. This sampling structure may contribute to higher reported implementation levels among LMIC respondents and should be considered when interpreting the observed negative PPGs. At the same time, the high proportion of U.S. respondents may limit the extent to which findings reflect the diversity of HIC settings.
The implementation index is based on self-reported data and a conservative binary coding approach in which “I don’t know” responses are treated as the absence of implementation. This decision was intended to ensure that only confirmed practices contribute to the index and to avoid inflating implementation estimates due to uncertainty. However, this approach may underestimate true implementation, particularly in settings where respondents have limited visibility into institutional processes. As a result, differences in implementation scores across countries may reflect not only variation in actual practices but also differences in respondent awareness or access to information. This limitation is especially relevant in cross-country comparisons, where institutional structures and reporting norms may vary.
The interpretation of negative PPGs in LMICs should therefore be approached with caution. The findings may be influenced by selection bias toward internationally connected institutions, as well as limitations of the GHS Index, which primarily captures the presence of national-level policies rather than their implementation or enforcement. In addition, international collaborations and funding requirements may influence institutional practices in ways that are not captured by country level indicators.
In addition, the comparison of institutional-level survey responses with country level GHS Index scores introduces a cross-level mismatch. The GHS Index reflects national policy capacity, whereas the implementation index captures practices within specific institutions. The resulting PPG, therefore, reflects both differences between national frameworks and institutional practices and variation across institutions within the same country. Accordingly, this measure should not be interpreted as a direct estimate of country level policy–implementation alignment, but rather as an approximation based on the institutional settings represented in the sample.
The pattern observed across containment levels further highlights the critical role of understanding institutional diversity in shaping biosecurity implementation. Personnel working in BSL-3/4 laboratories consistently reported smaller or more balanced policy–implementation gaps and also predicted the higher implementation index. These facilities maintain strong compliance and oversight mechanisms aligned with national policies. While the association exists, the causal reference cannot be established. BSL-3/4 laboratories require a stronger governance culture and better resources that may support more biosecurity oversight practices. However, these findings also highlight a governance/implementation challenge: Biosecurity policies are often designed primarily for high-risk research settings, whereas lower-containment laboratories (BSL-1/2), where the majority of daily research occurs, tend to exhibit larger positive gaps and a lower implementation index.
Evidence from previous studies supports this concern. Reports on laboratory incidents involving potential exposures or releases of pathogens have shown that many incidents occur in BSL-2 laboratories,16,46 not in high-containment facilities.47–49 This may be due to stricter regulatory requirements and a more established safety culture found at higher biosafety levels. While oversight for high-containment laboratories is well defined, biosecurity implementation at lower levels (BSL-1/2) requires more attention. Although such high-containment laboratories may function as potential “norm diffusion hubs”, where training programs and governance structures can influence other laboratories through professional networks and collaboration, achieving increased biosecurity will require clearer, risk-based guidance, sustained financial support, and regular, high-quality training tailored to the operational realities of BSL-1/2 laboratories.
Multivariable analysis also revealed that some institutional and individual factors such as international collaboration, perception of training, and financial support helped predict the implementation index. The United States seems to have a higher implementation score if they are engaged in international activities, potentially due to the oversight policies31,40 before collaborating internationally. Basic life science research and risk assessment or mitigation are the top two collaborative activities of U.S. and non-U.S respondents; however, the percentage of U.S. respondents in basic life research science surpassed that of non-U.S. respondents (see Figure 4). On the contrary, financial support from respondents’ workplace is a good predictor for the implementation index in non-U.S. countries. While using the same predictors in the regression model for both U.S. and non-U.S. groups to compare their associations with implementation outcomes, the interpretation of these impacts could be influenced by differences in regulatory requirements, institutional structures, or cultural norms.

International collaboration area by U.S. versus non-U.S. respondents (in %). The figure shows the percentage of respondents reporting different areas of international collaboration, stratified by U.S. and non-U.S. respondents. Among the survey participants, 119 individuals reported engaging in international collaboration activities, and only these respondents are included in this figure.
While some institutional factors were predictors for the implementation index, the national factors were not. This suggests that national policies or country capacity alone are insufficient predictors of practical performance; rather, effective biosecurity depends on how policies are implemented at the institutional level. However, it may suggest that the effects of national governance were mediated through institutional implementation: national policies establish broader guidance and expectations, and their practical impact may depend on how institutions interpret, resource requirements, and implement them. The institution’s environment is important but varies in risk tolerance, approaches to high-risk research, and the availability of internal guidance. These factors are often influenced by leadership expertise and risk perception.26,50 In addition, international collaboration plays an important role in strengthening biosecurity standards globally. Partnerships between countries with advanced biosecurity systems and those with developing frameworks can facilitate knowledge exchange, financial investment, and capacity building to help bridge the PPG in lower-capacity nations. Overall, biosecurity can be seen as an institutional and relational practice rather than a purely regulatory one.
Several limitations should be acknowledged when interpreting these findings. First, the sample size for several groups was uneven, with a disproportionate number of participants from the U.S. and limited representation from other regions. Responses from Asia and Sub-Saharan Africa were particularly sparse, and there were no respondents from key emerging countries with substantial high-risk research activity, such as China. This underrepresentation constrains the generalizability of the results and may not fully reflect the diversity of global biosecurity practices. The gap index shouldn’t be interpreted as the country’s policy–implementation gap, but as the individual gap in the country they are working in. Second, the GHS Index data used for national policy comparisons were drawn from the 2021 dataset. The current policy developments or governance changes at the national level may not be captured in this analysis. However, national biosecurity policies often evolve gradually, and there may be a time lag between the introduction of policy change and their observable effects on actual implementation. Alternate biosecurity benchmarks such as the 2024 Biosecurity Framework, lack standardized quantitative scores across countries for analysis. While being introduced in 2021, the GHS index is still relevant to illustrate the picture of biosecurity governance in the world. In addition, the biosecurity score was based only on nine subcategories and did not cover other important practices in biosecurity. Third, the implementation scores were based on a self-reported survey, reflecting the perceptions and awareness of participating individuals rather than verified institutional audits or performance metrics. The individual perception may be different from actual institutional practices. Respondents may overreport implementation due to social desirability bias or institutional loyalty, particularly when reporting on sensitive areas such as personnel reliability measures or material transfer oversight. Respondents from different countries and cultures may interpret survey questions differently and may introduce cross-cultural variation in interpretation. While self-reported data exists with certain biases, they provide valuable insight into how biosecurity policies are interpreted and implemented by practitioners. More data on respondents’ proficiency should also be collected in future surveys for adjusting the weighting of responses. Finally, potential selection bias exists among respondents from LMICs. Participants from these regions likely represent a small, internationally connected subset of biosecurity professionals, often affiliated with externally funded institutions. Their responses may overestimate national-level implementation capacity and not accurately represent the broader institutional landscape within their countries.
Conclusion
The study is the first empirical cross-national assessment of biosecurity implementation at the professional level and attempts to quantify the gap between national policy and implementation. The findings show that the policy–implementation gap varied across countries. HICs have policy development outpacing institutional implementation. In contrast, LMICs obtained higher implementation scores than their national policy frameworks. This suggests the need for targeted investment in biosecurity policy development and governance systems in countries where research activities are expanding but regulatory oversight remains limited or not well developed. The negative gap index may also reflect the international influence on institutions’ implementation via collaboration and training in these countries. For high GHS index countries, clearer and more standardized biosecurity policies would help to reduce confusion and inconsistency for implementers.
The study also identified some areas requiring greater attention in implementation, including psychological screening and wellness programs, personnel vetting, cross-border transfer, end-use transfer, and cybersecurity. Strengthening these practices through international standards, continuous financial support, and collaborations can help close the implementation gap and enhance global pandemic prevention capability.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. Restrictions may apply to data availability due to privacy or ethical considerations.
Authors’ Contributions
A.T.: Conceptualization, data curation, formal analysis, methodology, investigation, resources, writing—original draft, writing—review and editing, and validation. D.R.G. and K.M.V.: data curation, investigation, resources, writing—review and editing, and validation.
Footnotes
Acknowledgments
A.T. would like to thank Jennifer Fletcher at Accountability, Assessment and Research, Chandler Unified School District, Chandler, AZ, USA, for providing guidance and comments on an early version of this article.
Author Disclosure Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
The 2025 data collection was supported by the National Institute of General Medical Sciences of the National Institutes of Health under award number 1R01GM155913-01.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.