
Abstract
The effects of obesity on asthma diagnosis, control, and exacerbation severity are increasingly recognized; however, the underlying pathophysiology of this association is poorly understood. Mainstream clinical practice has yet to adopt aggressive management of obesity as a modifiable risk factor in asthma care, as is the case with a risk factor like tobacco or allergen exposure. This review summarizes existing data that support the pathophysiologic mechanisms underlying the association between obesity and asthma, as well as the current and future state of treatment for the obese patient with asthma. Our review suggests that evidence of chronic inflammatory response linking obesity and asthma indicates a need to address obesity during asthma management, possibly using patient-centered approaches such as shared decision making. There is a need for research to better understand the mechanisms of asthma in the obese patient and to develop new therapies specifically targeted to this unique patient population.
Introduction
Asthma prevalence
Asthma is classically described as reversible inflammation of airways, characterized by recurrent attacks of shortness of breath, cough, and wheeze, affecting people of all ages. While airway obstruction and bronchial hyper-responsiveness are typically associated with asthma, these symptoms are pathologically related to other factors, such as atopy, obesity, reflux, stressors, and obstructive sleep apnea. 1 Asthma prevalence is increasing worldwide, affecting over 300 million people. 2 Over the period 1980–1996, asthma prevalence increased among all ages, genders, and racial groups, especially in more urbanized nations such as the US. 3 Currently, 24.6 million people living in the US have been diagnosed with asthma. 4
Disparities in asthma
Although asthma affects people of all ages, it disproportionately affects children.5–7 Currently, in the US, over 10 million children and adolescents have been diagnosed with asthma, making it the leading chronic childhood illness. 8 Since 1999, children 5–17 years of age have demonstrated the highest prevalence rates with 109.3 per 1000 diagnosed with asthma, compared with 76.8 per 1000 in those over 18 years of age. 9
Marked disparities in asthma outcomes exist for vulnerable populations such as low income, Hispanic, and African American populations. 10 Significant racial inequalities exist, especially in more industrialized countries with the highest numbers of asthma prevalence. For example, in the US, asthma prevalence is 43% higher for non-Hispanic blacks compared with non-Hispanic whites. 9
Even among children, these racial differences are evident.7–9 Results from the National Health Interview Survey 1997–2003 found that asthma prevalence was consistently greater among non-Hispanic black children (15.7%) compared with non-Hispanic white children (11.5%) across all levels of income. 11 In addition, non-Hispanic black children are 3.6 times more likely to use the emergency department (ED) for asthma-related issues than non-Hispanic white children. 12 Multiple asthma-related ED visits are considered risk factors for fatal asthma, which is reflected in the rates of asthma mortality seen among minority groups, especially African Americans. 13 In 2006, non-Hispanic blacks had a rate of asthma mortality over 200% higher than non-Hispanic whites. 14 Furthermore, from 2003 to 2005, the Centers for Disease Control and Prevention reported that African American children had a rate of asthma mortality 7 times higher than non-Hispanic white children. 15 Reasons for poor outcomes are considered multifactorial and include: lack of continuity care, poverty, lack of transportation, limited access to care and health insurance, and not having an asthma action plan.16–18
Asthma costs
Health care costs increase in patients with more severe asthma, but the effect of asthma exacerbations on costs among patients with more severe asthma is difficult to quantify. Comparison of direct health care costs between patients with moderate/severe persistent asthma with and without exacerbations showed patients with moderate/severe persistent asthma who had exacerbations had higher total and asthma-related health care costs than those without exacerbations. 19 Moreover, asthma controller medication use was higher in patients with exacerbations. Hospitalization and medications were found to be the most important cost driver of direct costs. Work and school loss accounted for the greatest percentage of indirect costs. The cost of asthma was correlated with co-morbidities, age, and disease severity. Despite the availability of effective preventive therapy, costs associated with asthma are increasing. Strategies including education of patients and physicians, and regular follow-up are required to reduce the economic burden of asthma. 19
In a study of Kaiser Permanente’s Southern California System, there was a $3499 difference in direct costs for those with uncontrolled versus controlled asthma – $3298 versus $6797, respectively. 20 A national study found a difference of $4212 21 . From these numbers we can assume asthma control saves >$4000 per patient. For a typical large healthcare system with 60,000 asthma patients, if we assume control could be improved for between 2 and 10% of patients, then cost savings vary between $4.8 and $24 million dollars. When lost productivity and premature death are considered, the resultant financial burden of asthma is even higher ($56 billion). 22 Because of the high burden of suffering and cost, the Institute of Medicine and Agency for Healthcare Research and Quality (AHRQ) identified asthma as a high priority condition requiring further research.23–25 Research is encouraged around patient-centered initiatives especially those targeting vulnerable, low-income and minority ethnicity patients.
Obesity and asthma
The prevalence of obesity in the US is increasing at an alarming rate. Body mass index (BMI), defined as the weight in kilograms divided by the square of the height in meters, is commonly used to classify overweight and obesity. 26 In adults, a BMI between 25 and 29.9 is defined as overweight and a BMI of 30 or higher is considered obese. For children, overweight is defined as a BMI between the 85th and 94th percentile for age and gender, and obese is defined at a BMI at or above the 95th percentile for age and gender. 26 The increased prevalence of obesity in adults has been accompanied by a similar increase in the prevalence of obesity in children. 27 Similar to asthma, racial and ethnic disparities exist with obesity prevalence. In the US, non-Hispanic blacks have a 51% higher rate of obesity, and Hispanics have a 21% higher rate of obesity compared with non-Hispanic whites. 28 Similar to adults, the combined prevalence of obesity and overweight is also higher in non-Hispanic black children (35.4%) compared with non-Hispanic white children (28.2%). 29 Hispanic boys ages 6–11 have the highest combined obesity and overweight prevalence (43.9%).
The parallel increase in asthma and obesity prevalence has led to several studies examining the possible relationship between these two conditions. A study examining the trends in obesity among adults, using data from the NHANES I (1971–1975), II (1976–1980), and III (1988–1994), found that BMI increased universally among adults with asthma and those without; however, the prevalence of obesity rose more in the asthma group (21.3–32.8%) compared with the non-asthma group (14.6–22.8%). 30 A retrospective study of 143 adults found a similar association between obesity prevalence and asthma severity. 31 Obese asthmatics show disparities in response to therapy and have a nearly fivefold risk of hospitalizations due to exacerbations. 32 Identifying new mechanisms that improve the delivery of asthma care is an important step toward advancing patient outcomes, avoiding preventable ED visits and hospitalizations, while simultaneously reducing overall healthcare costs.33,34
This relationship between asthma and obesity has also been replicated in the pediatric population. A cross-sectional study using data from the Third National Health and Nutrition Examination Survey 1988–1994 showed that one of the highest risk groups for developing asthma were children over the age of 10 with a BMI greater than or equal to the 85th percentile. 35 A European study found that obesity among children 4–11 years of age was associated with asthma regardless of ethnicity, especially among girls. 36 Findings from the National Longitudinal Survey of Youth, which followed more than 4000 asthma-free children for 14 years, discovered a BMI at or greater than the 85th percentile at age 2–3 years was a risk factor for subsequent asthma development in boys. 37
Obesity is a risk factor for asthma in multiple demographic groups.7,38 Female gender is significantly associated with asthma and obesity. 39 In addition, obese asthmatics have a decreased quality of life and increased utilization of resources compared to their non-obese counterparts. 40 Factors that could contribute to the pathogenesis of asthma in the obese include both mechanical factors and altered inflammation and immune responses related to the obese state.
Obese asthma phenotypes
Pathophysiology of asthma has been described in detail. 41 The disease is considered an inflammatory disease in the airway, leading to airway hyper-responsiveness, obstruction, mucus hyper-production, and airway wall remodeling. Studies in immunology and molecular biology have resulted in an extensive evaluation of inflammatory cells and mediators involved in the pathophysiology of asthma. It is recognized that airway remodeling, characterized by thickening of the airway wall, can contribute to the chronic progression of the disease. Epithelial to mesenchymal cell transitions cause persistence of the inflammatory infiltration and induce histological changes in the airway wall, increasing thickness of the basement membrane, collagen deposition, and smooth muscle hypertrophy and hyperplasia. Resulting airway inflammation and remodeling leads to the airway wall thickening and induces increased airway smooth muscle mass, which generates asthmatic symptoms. Asthma has been considered a classic T helper 2 (TH2) cell-associated inflammatory disease, with TH2-type cytokines, such as interleukin-4 (IL-4), IL-5, and IL-13, driving the disease pathology in patients. Although atopic asthma has a substantial TH2 cell component, the disease is notoriously heterogeneous, and recent evidence has suggested that other T cells also contribute to the development of asthma. 42
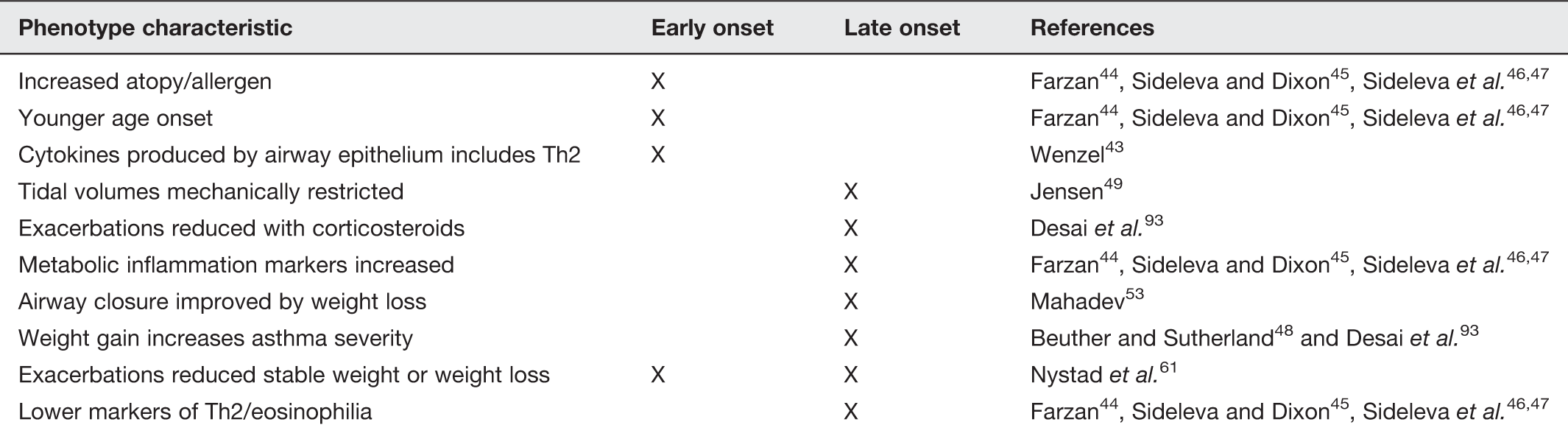
Recent studies suggest that there are at least two distinct phenotypes of asthma in obesity (Figure 1, Table 1).43,44 The obese state alters both early onset allergic asthma and also leads to the development of a novel form of late onset asthma, in part due to obesity.45–47 Patients with the atopic phenotype are likely to have pathophysiology consistent with early onset allergic asthma that is complicated by the development of obesity. Early onset allergic asthma is characterized by TH2 driven lymphocytic inflammation with increases in cytokines such as IL-4 and IL-5 that promote airway eosinophilia and IL-13 leading to mucus hypersecretion.42,43 Atopic asthma is an inflammatory disorder characterized by accumulation of eosinophils, mast cells, and CD4+ T lymphocytes, and with remodeling of the airway.
Image of asthma phenotypes for early and late onset obesity-associated asthma (A color version of this figure is available in the online journal) Asthma–obesity phenotypes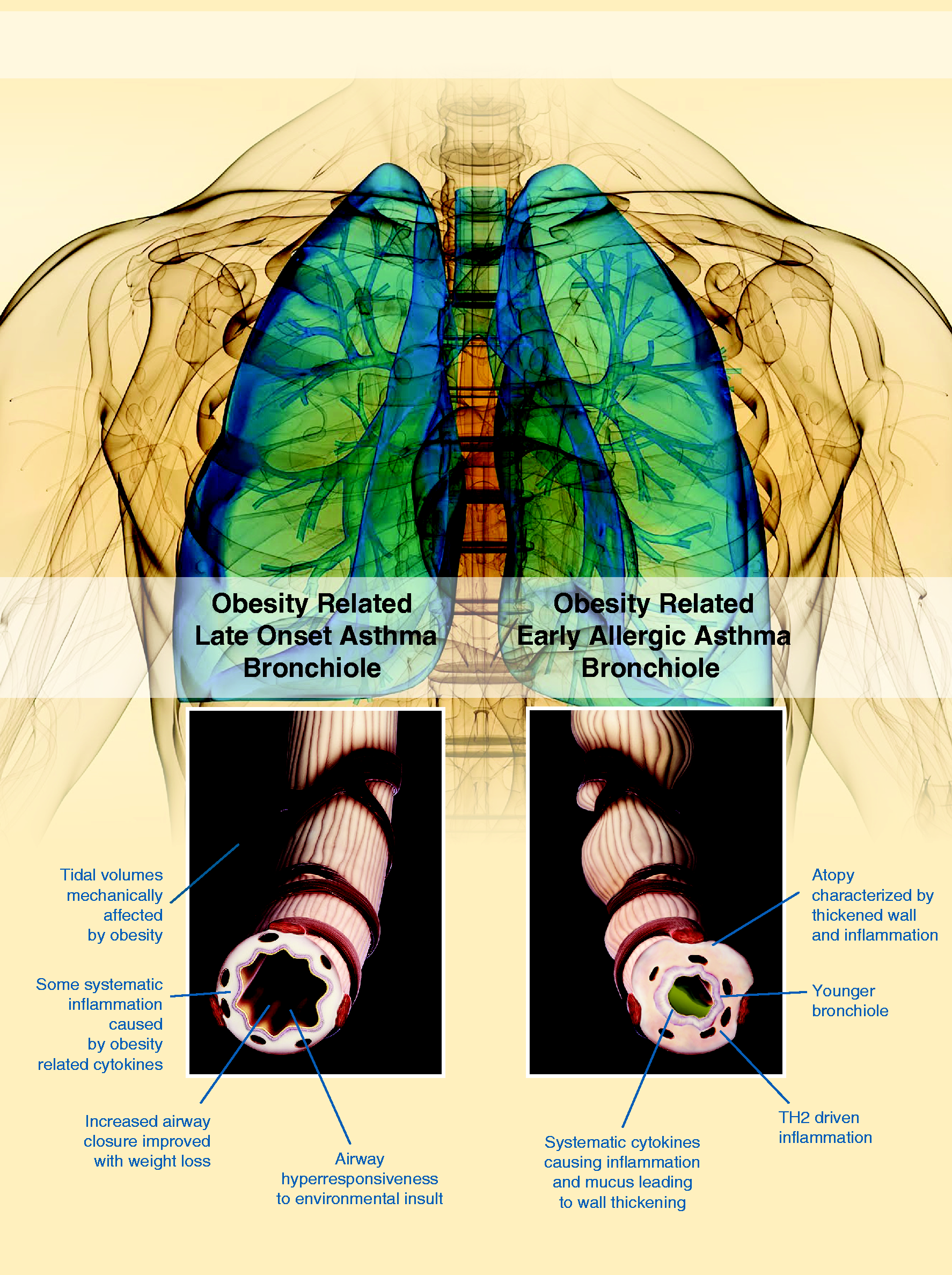
Adipose tissue produces a number of cytokines and adipokines which may have a synergistic adverse effect on the airways. Cytokines produced by adipose tissue include plasminogen activator inhibitor-1, monocyte chemotactic factor-1, interleukins 6 and which may affect the airway such as plasminogen activator inhibitor-1, monocyte chemotactic factor-1, IL-6 and 8, and adipokines such as leptin and adiponectin. The precise role of many of these mediators in the pathogenesis of allergic airway disease is not well known; however, a number of studies have shown the potential role of adiponectin (which is decreased in obesity) and leptin (which increases in obesity) in allergic asthma.45–47
The second phenotype relates to obese patients with later onset of asthma and a much lower prevalence of allergic disease. These individuals have late onset asthma, in which obesity plays a role. Meta-analyses demonstrate a direct correlation between obesity and increased risk of the developing non-atopic asthma characterized by this phenotype. 48 This type of asthma is currently poorly understood but appears to be characterized by lower markers of airway eosinophilia and TH2 inflammation than are typical of early onset allergic asthma. Additionally, late-onset, non-atopic form of asthma is more common in women than men. A number of factors, both molecular and mechanical, could contribute to innate increases in airway reactivity and lung function with obesity. In addition to the airway hyper-responsiveness caused by the biochemical effects of adipose related cytokines and adipokines described earlier, mechanical changes in lung function and airways likely play an important role. This mechanical linkage between obesity and asthma is thought to be related to restrictive physiology. 49 In obese patients, tidal volumes are decreased due to a reduction in chest expansion that is caused both by the weight on the chest itself and the effect of abdominal obesity on flattening the diaphragms. Patients with asthma have an intrinsic impairment of the ability for inspiration to stretch airway smooth muscle. Breathing at the low lung volumes seen with a restrictive lung pattern leads to increased airway hyper-responsiveness. 50 It has been hypothesized that breathing at low lung volumes may lead to increased actin–myosin cross-linking in airway smooth muscle, effectively making the muscle stiffer. 51 This stretch of smooth muscle is a critical determinant of airway reactivity in vivo; furthermore, in vitro studies have demonstrated that smooth muscle stretch modulates the expression of proteins in airway smooth muscle. Supporting this theory, others have shown that continuous positive airway pressure leads to decreased airway reactivity in both animal models and in humans with asthma. 52 Thus, one plausible explanation for the obese asthma phenotype is the effect that breathing at low lung volumes has on smooth muscle remodeling and resultant smooth muscle function and hyper-reactivity.
Expiratory flow limitations can be caused by both a reduction in operating lung volume, as occurs in obesity, and bronchoconstriction, as occurs in asthma. Obese individuals breathe close to the closing volume of the airways, which may promote reduction in operating lung volume. Bronchoconstriction, as occurs in asthma, can also increase expiratory flow limitation during tidal breathing. 53 This premature airway closure seen in obesity may have direct effects on airway caliber and airway function in the setting of obesity. Mediators produced by adipose tissue may be important in the pathogenesis of late onset asthma in obesity. Markers of adipose tissue metabolic inflammation are increased particularly in visceral fat of patients with this form of asthma. 46 This was not related to enhanced airway inflammation, suggesting that these metabolic mediators could be having a direct effect on the airway.
Many studies have reported elevated serum leptin to be associated with asthma in obesity.45,54 Leptin was significantly increased in visceral adipose tissue of obese asthmatics, and this was related to airway reactivity. Leptin may have multiple effects on lung development; leptin deficient mice show decreased lung volume and alveolar surface area 55 and decreased proliferation of tracheal epithelium. 56 Further study should be performed to elucidate the role of leptin in the pathogenesis of asthma using conditional leptin knockout mice.
The exact mechanism creating the dose effect seen between obesity and asthma is not fully known. Proposed theories for obesity causing asthma include mechanical, dietary, genetic, and hormonal factors. 57 One main theory that has generated the most discussion is the role pro-inflammatory cytokines such as leptin play in the process because adipose tissue is known as a primary source of these systemic immunomodulating agents and could be contributing to the chronic inflammation seen in asthma, creating more symptoms of the disease. 57 One theory proposed, which supports the less common view that asthma causes obesity, is that individuals with asthma restrict their levels of activity for fear of inducing an asthma exacerbation, which then leads to a more sedentary lifestyle and an increased risk of obesity. 58
Asthma severity – dose response
Obesity is not only a risk factor for the development of asthma in adults and children, but is also associated with worse asthma-related health outcomes as indicated by Manion, 7 Guerra et al., 59 and Hjellvik et al. 60 A large Norwegian study of more than 135,000 men and women found a 10% increase in asthma prevalence per unit of increase in BMI in men and a 7% increase in prevalence per unit increase in BMI in women. 60 In men, the risk of asthma increased by 10% with each unit of increased BMI between 25 and 30. The similar value for women was 7%. Overweight or obese persons reported asthma more often than did normal BMI persons after adjustment for smoking, education, and physical activity. 61
Diagnosis
Initially, asthma is diagnosed by physical exam and symptomatology. Signs of respiratory distress, rhinitis, nasal irritation and swelling, prolonged expiratory phases, and triggers of symptoms assist in the diagnosis. Laboratory evaluation is minimal, occasionally involving assessment for eosinophilia or an elevated IgE. Objective diagnosis is obtained by spirometry or pulmonary function tests. A reduced Forced Expiratory Volume1/Forced Vital Capacity (FEV1/FVC) ratio, with reversibility after using bronchodilators, verifies the diagnosis of asthma. Limits occur within this objective testing, primarily in obtaining reproducible flow/volume curves in young children. 62 Relatively few data in this age group exist, and performing spirometry in young children requires specific expertise. Spirometry is often not feasible outside the research arena or more specialized clinical settings. Challenge testing, with methacholine, histamine, or exercise has increased specificity for diagnosing asthma, but also is rarely used in clinical settings due to expertise required to administer tests, access to testing, and other factors. 63
International guidelines advise that asthma diagnosis should be based on both the presence of symptoms and objective measurements of variable airflow obstruction or bronchial hyper-responsiveness when challenged with bronchodilators. 61 However, physicians frequently diagnose asthma based on symptoms without confirmation by pulmonary function tests or spirometry. 63
Confirmation of asthma may be more difficult in patients who are taking regular asthma-controlling medications. Patients on inhaled corticosteroids (ICS), even for <3 months, can experience not only an improvement in symptoms but also a decrease in demonstrable airway responsiveness, even returning to the normal range on bronchial challenge testing. Objective testing, which may include negative bronchial challenge testing results or absence of change in postbronchodilator forced expiratory volume in 1 s (FEV1) can indicate either a well-controlled asthmatic or a non-asthmatic. Even among subjects not started on ICSs, confirming a physician diagnosis of asthma can be difficult if there are minimal symptoms, and hence probably minimal airway inflammation, at the time of testing. 63 Because of the overlap in respiratory symptoms and compromised function, obesity creates a unique challenge in the use of symptoms for the diagnosis of asthma and places particular importance on the use of lung function test/spirometry. Indeed, obese individuals presenting for evaluation of acute respiratory symptoms are also more likely to receive a misdiagnosis of asthma.62,64 Overdiagnosis of asthma can lead to inappropriate treatment, with increased risk of side effects and increased costs.60,65–67 Multiple studies report that asthma could be excluded after extensive testing in a third of physician-diagnosed asthma.63,67,68 Underdiagnosis is also an important issue. 69 Impaired dyspnea perception and poor perception of airflow obstruction may lead to undertreatment of asthma in the obese. In addition to confirming previous reports on overdiagnosis of asthma, a substantial proportion of morbidly obese asthma patients were underdiagnosed. There were few differences between the underdiagnosed and the overdiagnosed subjects.
Treatment of asthma in the obese patient
Asthma treatment involves environmental trigger avoidance, treatment of co-morbid conditions, and use of pharmacotherapy with a goal of reducing both impairment and risk for exacerbations. The National Heart, Lung, and Blood Institute (NHLBI) Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma provides clinicians with comprehensive treatment recommendations. 64 The pharmacotherapy recommendations within this guideline follow a stepwise approach that is tailored to a patient’s level of impairment and risk. The treatments are directed at the underlying physiologic mechanisms of asthma and include short-acting beta agonists for symptom relief with a combination of ICSs, long-acting beta agonists (LABA), and leukotriene receptor antagonists to achieve long-term control. Currently, the NHLBI guidelines do not differentiate pharmacotherapy medication choices or dosing for asthma patients with co-morbid obesity. However, preliminary evidence suggests that the obese asthma phenotype may adversely affect standard treatment regimens, and a one-size fits all approach may not be best. 65 A recent review summarizes the growing number of studies that demonstrate obese asthmatics have less response as measured by spirometry and/or symptoms to ICS with comparable decreases seen in efficacy for treatment with combined ICS/LABA.32,63,66,67 Overweight and obese children have been shown to require increased amounts of B-agonists and higher oral steroid use. 69 Similarly, inhaled budesonide was less effective at improving measures of lung function and reducing ED visits/hospitalization for overweight/obese children when compared to their normal weight counterparts. 70 It is perhaps in part due to these differences in therapeutic effects that lead to an increase in disease severity and exacerbations for obese patients with a nearly fivefold risk of asthma-related hospitalizations. 32 Further research is needed to explore if pharmacotherapy can be more specifically tailored to the different physiologic mechanisms of disease activation in the obese asthma phenotypes.
In terms of obesity management in asthmatic patients, the NHLBI guidelines encourage clinicians to evaluate and treat co-morbid obesity, suggesting that despite limited evidence, such treatment may lead to better asthma control. In a 2012 Cochrane review, only four acceptable randomized controlled trials looked at the effect of weight loss strategies on asthma outcomes. 71 The trials had methodological limitations, but one trial did show a benefit of weight reduction on asthma control. Another systematic review of asthma and weight loss found reversibility of at least one asthma outcome irrespective of whether weight loss was a result of surgical or medical intervention. 72 Potential positive effects of weight loss have been demonstrated albeit at the extremes of both BMI and actual weight lost. In a cohort of 12 severely obese asthmatics, bariatric surgery and the resultant BMI decrease from 51.2 to 34.4 led to improved lung function, improved performance on methacholine challenge, and a decrease in self-reported asthma symptoms. 73 Also in a study of 500 morbidly obese patients who underwent laparoscopic adjustable gastric banding surgery, greater than 80% of the patients who had asthma symptoms before surgery reported resolution or improvement in their symptoms. 74 While existing studies do not provide definitive guidance on how to integrate weight loss into asthma treatment strategies, the constellation of evidence seems to suggest that weight loss would lead to improved asthma symptoms and decreased exacerbations.
Changing the paradigm of asthma treatment to include weight management and perhaps different pharmacotherapeutic regimens will require special attention to the unique barriers that underserved populations face in the treatment of asthma. These barriers include limited access to care and medications, cultural differences in understanding and accepting treatment options, and decreased health literacy.16,64,75–78 To address these complexities, innovative approaches to treatment are needed.
One example of a novel approach in asthma management is shared decision making (SDM) (Figure 2). SDM is a promising modality that it incorporates cultural beliefs, change theory, and health literacy by partnering with patients in understanding their asthma and developing management plans.
Schematic representation of the elements of shared decision making (A color version of this figure is available in the online journal)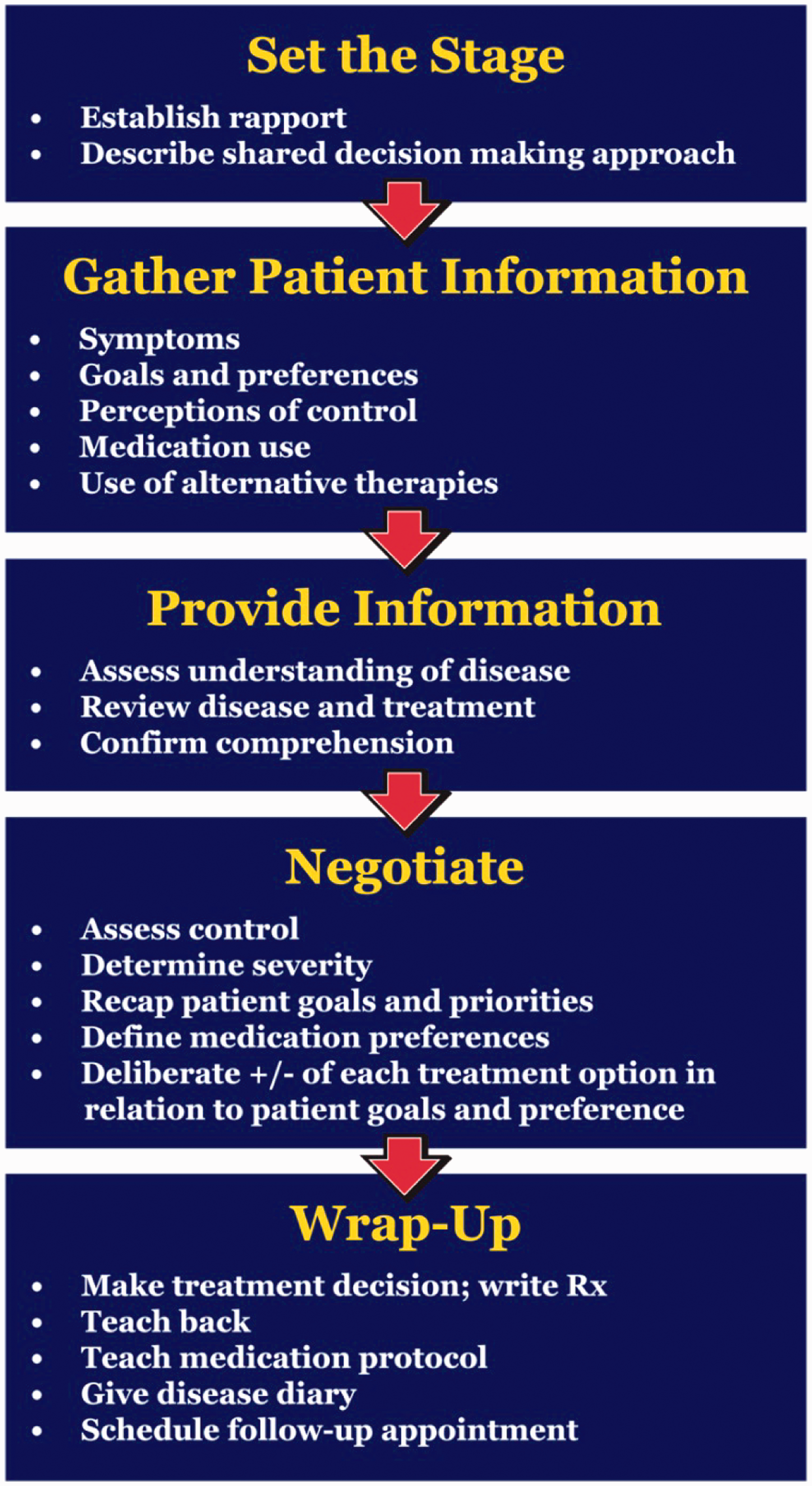
Patient-centered management of asthma in primary care – can SDM improve outcomes for obese patients with asthma?
Identifying new mechanisms that improve the delivery of asthma care is an important step toward advancing patient outcomes, avoiding preventable ED visits and hospitalizations, while simultaneously reducing overall healthcare costs. 33
Unfortunately, many patients with asthma lack adequate control of their symptoms, thus negatively impacting their overall quality of life. Indeed, almost 50% of adults with asthma have symptoms more than once weekly and 17% have daily symptoms.79,80 Consequently, over 30% of adults with asthma go to the ED for their asthma at least once per year, resulting in one or more days of missed work.79,80
The current approach to asthma management involves monitoring symptoms and lung function, encouraging use of controller meds and trigger avoidance, patient education, and collaborative patient–provider relationships that include written asthma action plans. 81 Adhering to NHLBI guidelines has been shown to be efficacious in a variety of pediatric populations, including high-risk populations such as inner city, poor, and/or African American populations.82–84 However, when patients see their primary care provider for preventative care, the majority are unlikely to be adequately evaluated and treated based on current guidelines.85,86 Clinical practice guidelines have had limited effect on changing provider behavior. Little is known about the process and factors involved in changing physician behaviors to improve guideline adherence.87,33 However, SDM may offer a solution to improve adherence to guidelines and improve patient-oriented outcomes. Only one study, by Dr Sandra Wilson and colleagues, has been published in this area. 88
Building off the work of Wilson, our group led the Asthma Comparative Effectiveness (ACE) Study funded by the AHRQ to create a toolkit to assist providers with implementation of a SDM approach to asthma care that would be effective in everyday practice.89,90 Initial results show that use of the asthma SDM toolkit is associated with improved quality of life, medication adherence, reduction in utilization of acute care services, and hence cost savings. SDM interventions may not be as effective in obese patients. Using data from a randomized controlled trial of 612 adults with poorly controlled asthma, 91 Ayala et al. hypothesized that obese patients would have benefitted less from the SDM intervention than did overweight or normal weight patients. Standard BMI categories were defined. Overweight SDM patients negotiated a higher daily controller dose than normal weight control. BMI negatively modified the SDM intervention effect on controller fill/refill adherence. Obese SDM patients also received a smaller intervention benefit (but still significantly better than usual care) than SDM patients in other weight groups.
The observed beneficial effects of SDM in our study and others did not change in relation to BMI for any of the clinical outcomes. Like normal weight and overweight SDM patients, obese SDM patients demonstrated significantly better clinical outcomes compared with obese patients in usual care for asthma-related health care utilization, use of rescue medication, the FEV1 and FEV1/FEV6 ratio, and the odds of reporting no asthma control problems. These results demonstrate that a SDM approach to treatment choice can clinically benefit adult patients with poorly controlled asthma, regardless of BMI. 91 We performed a retrospective review of data from our ACE study. In this unpublished analysis, we hypothesized that obese asthmatics undergoing SDM have a higher baseline asthma severity and greater reduction in exacerbations following SDM. BMI was used as a determinant of obesity for adults and children. Asthma severity/control was determined by the number of asthma-related ED visits, asthma-related inpatient events, prednisone orders as a marker of exacerbations, and quality of life surveys. Baseline evaluation before the SDM intervention showed obese adults with asthma have approximately twice the rate of prednisone orders, 3× the ED visit rate, and almost double the hospitalization rate compared with non-obese patients. By gender both obese men and women had more ED visits and hospitalizations than non-obese asthmatics, while obese women had more prednisone orders than non-obese women, a trend not seen in men.
For both children and adults in the obese and non-obese, there was a trend of decreased asthma severity for the 12 months following the SDM toolkit intervention compared to the 12 months before. Obese children saw a 67% decrease in asthma severity after the SDM compared to 38% for non-obese children, though the result was not statistically significant. Findings confirmed that obesity was associated with more severe asthma symptoms at baseline in adults, particularly in women. Additionally, SDM was associated with a drop in severity for all groups. SDM appears to be effective in improving asthma severity in obese patients and may be a mechanism for explicitly incorporating weight loss strategies. Possible SDM solutions include: incorporating education about the effects of obesity on asthma control, asking patients about goals around weight loss, and providing them with education and strategies for weight loss.
Increasingly, evidence suggests that obesity and asthma are physiologically linked through a chronic inflammatory response. Increased cost through more frequent hospitalizations and reduced quality of life lead to a need to address obesity during asthma management. This would make including weight loss strategies in primary care a compelling component of asthma management. Future care involving patient-centered approaches such as SDM may offer new strategies for management of the obese asthmatic patient.
Author Contributions
This work was conceived by SM, AW, MD, and HT. Literature search was conducted by SM, HT, and AW. SM, HT, and AW contributed to the writing of the manuscript and production of the figures.
Footnotes
Acknowledgments
We would like to gratefully acknowledge Jake Emmerson, Peter Salathe, Catherine Courtland, and Dr Alisahah Cole for their contributions to this manuscript. This work was supported by the Agency for Healthcare Research and Quality (AHRQ) Grant Number R18HS19946-G1. The authors declare that there is no conflict of interest.