
Abstract
Background:
Cancer pain is a prevalent and persistent issue, and while there have been some observations of the possible benefits of acupuncture in managing cancer pain, there is still debate regarding its safety and effectiveness. This study aims to compare the efficacy and safety of different acupuncture modalities in the treatment of cancer pain through a network meta-analysis.
Methods:
Between the time each database was created and June 3, 2024, eight databases were queried: PubMed, Cochrane, Embase, Web of Science, CNKI, Wanfang, VIP, and China Biomedicine. Randomized controlled trials investigating the use of various acupuncture and moxibustion techniques in the treatment of cancer pain were identified. Publication bias and quality of randomized controlled trials were assessed using the Cochrane Risk of Bias tool and the Jadad scale, and network meta-analyses were performed using Stata 15 and R 4.3.2.
Results:
We incorporated 111 studies encompassing 9549 individuals diagnosed with cancer, examining 29 distinct therapies. Network meta-analysis showed that, compared to Usual Medicine, Acupuncture + Usual Medicine + Traditional Chinese medicine (MD = −1.83, 95% CI: −2.86 to −0.80) could reduce NRS scores, Acupuncture + Traditional Chinese medicine (OR = 30.86, 95% CI: 3.75-254.20) could improve cancer pain relief, Moxibustion + Usual Medicine (MD = 2.12, 95% CI: 0.43-3.80) could effectively improve KPS score, Acupuncture + Application of Chinese medicine (OR = 0.16, 95% CI: 0.04-0.66) is associated with a lower incidence of constipation, Electro-Acupuncture + Usual Medicine (OR = 0.11, 95% CI: 0.03-0.45) shows a lower incidence of nausea and vomiting, Acupuncture + Moxibustion + Usual Medicine (OR = 0.29, 95% CI: 0.09-0.90) is associated with a lower incidence of dizziness.
Conclusion:
Acupuncture + Traditional Chinese medicine is the best intervention for different acupuncture methods in the treatment of cancer pain, and Moxibustion + Usual Medicine is the best intervention to improve the quality of life of patients.
Introduction
Cancer is a prominent global cause of death, with multifaceted and intricate causes, encompassing hereditary, environmental, and lifestyle variables. With globalization and an ageing population, the global cancer burden is expected to reach 28.4 million cases by 2040, a 47% increase from 2020, posing a huge challenge to public health systems. 1 Cancer patients often have painful symptoms that can occur at all stages of various cancers. According to 2022 statistics, the overall prevalence of pain in cancer patients is 44.5%, of which 30.6% have experienced moderate to severe pain. 2 The pain caused by cancer has a serious impact on the survival rate and quality of life of patients. 3 In addition to the physical pain, cancer pain also causes significant psychological damage to patients, including severe psychological distress and depression. 4 Depression and pain are prevalent and disabling in a variety of cancer types and stages, often co-occurring, with additional adverse effects. 5
Recent studies have shown that acupuncture can stimulate the body’s natural pain-relieving mechanisms and promote healing by targeting tissues such as muscles, fascia, and nerves. 6 It has a favorable effect on the relief of various pains, and the efficacy is significant, the tolerance is good, and the adverse reactions are less, and it can be used as a complementary alternative therapy. 7 The use of acupuncture in the perioperative period as an adjunct or alternative to opioids has become increasingly common. 8 Acupuncture also shows unique advantages when it comes to treating cancer pain. A randomized clinical trial showed that acupuncture was not only effective in reducing pain scores and relieving pain, but also improved fatigue, insomnia, and quality of life. 9 Moxibustion is also effective in relieving cancer pain, and compared with sham moxibustion, the BPI pain score of cancer pain patients after moxibustion is significantly reduced, and the pain is relieved. 10 The study found that electroacupuncture treatment of patients with cancer pain significantly reduced VAS pain scores, which was also effective in relieving cancer pain. 11 In addition, the combination of acupuncture and medication can also reduce patients’ dependence on drugs and alleviate drug-induced adverse effects. 12
Multiple studies have demonstrated the effectiveness of acupuncture in reducing cancer pain scores and providing relief to patients suffering from cancer-related pain, but most of the current studies are limited to the efficacy of acupuncture and moxibustion compared with conventional drugs or sham acupuncture, and the efficacy and safety between different acupuncture methods need to be explored.
Method
We conducted this study according to the Preferred Reporting Program for Systematic Review and Meta-Analysis (PRISMA NMA), which is registered with the International Register of Prospective Systematic Reviews (PROSPERO), ID: CRD42024510773.
Search Strategy
From the period of inception until June 3, 2024, the following databases were utilized: PubMed, Cochrane, Embase, Web of Science, CNKI, Wanfang, VIP, and China Biomedical. The survey is not limited to any one region, although it only supports English and Chinese languages. Search terms: people (“cancer pain,” “Cancer Associated Pain,” “Neoplasm Related Pain,” “Oncological Pain,” “Tumor Related Pain”) and treatments (“Acupuncture,” “Moxibustion,” “Electric Acupuncture,” “Auricular Acupuncture”). See Supplemental Table 1 for the specific search strategy.
Inclusion and Exclusion Criteria
Inclusion criteria
P (population): The patients in our review were people with pathologically diagnosed cancer;
I (intervention methods): The intervention methods in this review used a variety of acupuncture methods, such as acupuncture, auricular acupuncture, electroacupuncture, and moxibustion;
C (control methods): The control group in this review used conventional medical treatment, sham acupuncture, etc.;
O (outcome measures): the primary outcomes of this review were NRS, KPS score, and cancer pain relief, with secondary outcomes being adverse events;
S (type of study): The types of studies included in this review were randomized controlled trials.
Exclusion criteria
S (study type): (1) non-RCT studies, (2) non-peer reviewed abstracts of public meetings, (3) duplicate publication of the same trial study, (4) no full text available, (5) animal and cell experiments, (6) non-Chinese and English literature, (7) notices, reports, guidelines, registries, books, etc.
Screening and Extraction of Data
All studies were imported into Endnote X9 and evaluated independently by two researchers to identify studies that matched the inclusion criteria.
Studies that meet the criteria were included for data extraction. The data extraction is as follows: (1) Basic information of the article: name of the first author, publication year, country, research type. (2) Basic characteristics of the research object: type of cancer, age, gender, number of interventions, number of controls, etc. (3) Intervention information: intervention and control measures, treatment time, follow-up time. (4) Outcome measures and (5) Assessment of risk of bias factors.
The literature screening and data extraction mentioned above were conducted autonomously by two researchers, and in the event of disagreement or uncertainty, a third researcher was consulted to resolve the issue.
Assessment of Risk of Bias and Quality of the Literature
The Cochrane Collaborative Risk of Risk of Bias (RCT) tool was used to assess the bias of the included studies. 13 The quality of the included literature was assessed using the Jadad scale. The evaluation was conducted independently by two researchers and arbitrated by discussion or by inviting a third researcher in case of disagreement or doubt.
Statistics and Methods
This network meta-analysis employed a Bayesian random-effects model to assess the comparative efficacy of different therapies. We calculated standard deviations (SMDs) for continuous outcomes and odds ratios (ORs) for dichotomous outcomes using a random-effects model, with corresponding 95% confidence intervals (CIs). All statistical analyses were performed using Stata 15 and R 4.3.2, and the bilateral P-value < .05 was considered statistically significant. The interventions were ranked according to SUCRA, and league tables were generated to compare the differences in effects between the interventions. Funnel plots were used to visually reflect the heterogeneity between studies.
Results Section
Literature Search
Eight databases were searched: PubMed, Cochrane, Embase, Web of science, CNKI, Wanfang, VIP, and China Biomedicine. From the establishment of the database to the publication of literature on June 3, 2024, 8340 studies were obtained, 3876 duplicate articles were excluded, and 4203 articles were excluded by reading the title and abstract (1417 reviews, 67 meta, 652 disease inconsistencies, 344 intervention inconsistencies, 369 unrelated, 227 experimental registries, 209 animal and cell experiments, 100 conference abstracts, 308 case reports, 206 non-journal and non-Chinese core journal articles, 72 non-Chinese and English studies, 34 non-RCT studies, 198 guidelines, letters, books, reports, experimental protocols, etc.), and 150 studies were excluded (26 could not obtain the full text, 30 could not extract data, 64 were surgical pain, 10 were chemotherapy pain, 10 were drug-induced pain, and 10 were inconsistent outcome indicators), and 111 studies were finally included.
The experimental screening process is shown in Figure 1.

Flow chart of literature screening.
Characteristics of the Study
From the beginning until June 3, 2024, we conducted searches in eight databases: Cochrane, Embase, PubMed, Web of Science, CNKI, Wanfang, VIP, and China Biomedicine. We ended up including 111 studies.9,10,14-122 The six studies are from the United States,9,16,19,21,27,30 99 from China,14,18,22,24,26,28,29,31-122 two from Korea,10,23 and one each from Brazil, 15 France, 17 the United Kingdom, 20 and Indonesia. 25 A total of 9549 patients were included, of whom 4417 were males, 4152 were females, and 980 for whom sex was not mentioned. There were 53 articles on lung cancer patients, 41 articles on breast cancer patients, 34 articles on gastric cancer patients, 43 articles on liver cancer patients, and 14 articles on pancreatic cancer patients. Interventions included: Acupuncture (A), inserting fine needles at specific points to regulate Qi (the essence of life) and alleviate pain; Auricular Acupuncture (AA), performing needle insertion at specific points on the ear to utilize the reflex relationship between the ear and the entire body for treatment; Electro-Acupuncture (EA), applying low-frequency electric current to acupuncture needles; Moxibustion (M), using burning mugwort (moxa) to heat specific acupuncture points, etc. Control measures include: Usual Medicine (U), commonly used analgesics; Sham Acupuncture/Auricular Acupuncture/Electro-Acupuncture/Moxibustion (Sham), procedures that do not stimulate the acupoints, do not apply electrical current, or do not involve moxibustion; Traditional Chinese medicine (ZN), utilizing phytotherapy to regulate the body and treat illnesses, typically in the form of decoctions or pills; Application of Chinese medicine (ZW), involving the preparation of herbal medicines as ointments or powders to be directly applied to the skin for the treatment of localized conditions; Point injection (PI), involving the direct injection of normal Saline into specific acupoints, etc. The number of people in each group ranges from 3 to 148, A736, AA395, EA596, M40, A + U1167, AA + U70, EA + U154, M + U363, A + AA209, EA + M30, A + M + U141, A + U + ZN239, A + U + ZW211, A + ZN76, A + ZW227, U7339, ZN23, ZW138, Sham 233 people. The specific characteristics of the included studies are shown in Supplemental Table 2.
Risk of Bias
We incorporated 111 studies.9,10,14-122 According to the Jadad scale, 0 to 3 was low quality and 4 to 7 was high quality, of which 89 were low-quality and 22 were high-quality. The included studies included 16 that were high-risk, and 95 with unclear risk. Risk of bias is shown in Figure 2. Detailed bias risk charts and Jadad scale scores are provided in the supplement materials.

Risk of bias graph.
Meta-Outcome Analysis
NRS score
Out of the 111 studies that were considered, 37 studies were selected for analysis of extractable data.14,23,26,28,31,36,37,49,50,61,64,65,70,73,74,78,84,85,88,91,93-96,98,99,101,106,108-110,112,114,115,119-121 The effect of 11 acupuncture modalities on NRS scores in patients with cancer pain were evaluated. The network diagram for comparison between interventions is shown in Figure 3, and it can be seen from the network diagram below that a total of 14 interventions were included, with the largest node of U, indicating the largest sample size, and the thickest line segments of A + U and U, indicating that the two were compared with the most studies.

NRS score network diagram.
Compared to U, A + U + ZN (MD = −1.83, 95% CI: −2.86 to −0.80), EA (MD = −1.42, 95% CI: −1.93 to −0.91), A + U (MD = −1.42, 95% CI: −2.21 to −0.64) can reduce NRS score. It has an improvement effect on the patient’s pain, as shown in Figure 4.

NRS score league chart.
According to the SUCRA table, the intervention A + U + ZN (SUCRA = 85.11%) appears to be the most effective in reducing the NRS score and alleviating cancer pain in patients with cancer pain, as indicated in Table 1.
NRS Score Ranking Table.

Abbreviations: A, acupuncture; AA, auricular acupuncture; EA, electro acupuncture; Sham, Sham acupuncture/auricular acupuncture/electro acupuncture/moxibustion; M, moxibustion; ZN, traditional Chinese medicine; ZW, application of Chinese medicine; U, usual medicine therapy.
Cancer pain relief effect
Out of the 111 papers that were considered, 79 studies were included for analysis of extractable data.24,26,33,35-37,39,40,42-55,57-59,61-68,73,75-80,82-97,99-113,115-122 The effect of 19 acupuncture modalities on cancer pain relief were evaluated, and compared with the network diagram between the interventions, see Figure 5. As can be seen from the network diagram below, a total of 24 interventions were included, with the largest U node, indicating the largest sample size, and the thickest A + U and U line segments, indicating the most comparative studies.

Cancer pain relief effect network diagram.
Compared with U, A + ZN (OR = 30.86, 95% CI: 3.75-254.20) and A + AA + U (OR = 15.38, 95% CI: 1.81-130.41) could improve the pain relief effect of cancer pain, as shown in Figure 6.

Cancer pain relief effect league chart.
Based on the SUCRA table, A + ZN (SUCRA = 94.63%) may be the best intervention to improve the efficacy of cancer pain relief, as shown in Table 2.
Cancer Pain Relief Effect Ranking Table.

Abbreviations: A, acupuncture; AA, auricular acupuncture; EA, electro acupuncture; Sham, Sham acupuncture/auricular acupuncture/electro acupuncture/moxibustion; M, moxibustion; PI, point injection; C, cognitive behavioral therapy; R, relaxation therapy; ZN, traditional Chinese medicine; ZW, application of Chinese medicine; U, usual medicine therapy.
KPS score
Out of the 111 papers that were considered, 18 studies were selected for examination of extractable data.36,39,56,58,64,67,88,93,95,97,101,102,109,110,113,115,118,121 The effect of seven acupuncture modalities on KPS scores in patients with cancer pain were evaluated, and compared with the network diagram between the interventions, see Figure 7, as can be seen from the network relationship diagram below. A total of eight interventions were included; the node of U is the largest, indicating that it has the largest sample size, and the A + U and U segments are the thickest, showing that most comparative studies were conducted.

KPS score network diagram.
Compared with U, M + U (MD = 2.12, 95% CI: 0.43-3.80) and EA + U (MD = 1.62, 95% CI: 0.42-2.82) could effectively improve KPS score. It has been shown to improve the quality of life of patients, as shown in Figure 8.

KPS score league chart.
Based on the SUCRA table, M + U (SUCRA = 86.67%) may be the best intervention to improve the KPS score and quality of life of patients with cancer pain, as shown in Table 3.
KPS Score Ranking Table.

Abbreviations: A, acupuncture; AA, auricular acupuncture; EA, electro acupuncture; M, moxibustion; ZN, traditional Chinese medicine; ZW, application of Chinese medicine; U, usual medicine therapy.
Adverse events
Out of the 111 studies included, 47 documented adverse events.9,16,19,23,30,33,40,43,46,52,56,58-61,64-69,74-75,77,78,80-82,85,86,91,94,96,98,101-103,106-108,111,114-116,119,121 The number of adverse events that occurred with 17 different interventions was counted, and three adverse events of constipation, nausea and vomiting, and dizziness were extracted and analyzed. By analyzing these adverse events, we aim to assess the relative safety of acupuncture in treating cancer pain compared to other interventions.
Constipation
Out of the 111 papers that were considered, 29 studies were selected for examination of extractable data.33,39,40,52,56,59,61,64-67,73-75,77,78,85,91,94,96,101,102,106,107,111,114,115,119,121 The effect of 10 acupuncture modalities on the occurrence of constipation in patients with cancer pain were evaluated, and a comparative network diagram between interventions was constructed, see Figure 9. As can be seen from the network diagram below, a total of 11 interventions were included, with the largest node of U, indicating the largest sample size, and the thickest A + U and U line segments, indicating the most comparative studies.

Constipation network diagram.
Compared with U, the incidence of constipation was lower in A + ZW (OR = 0.16, 95% CI: 0.04-0.66) and A (OR = 0.18, 95% CI: 0.07-0.45), indicating that these interventions were associated with fewer adverse events of constipation and higher safety, as shown in Figure 10.

Constipation league chart.
Based on the SUCRA table, U (SUCRA = 91.41%) was the most commonly used intervention for constipation in patients with cancer pain, A + ZW (SUCRA = 25.47%) had the least constipation reaction, as shown in Table 4.
Constipation Ranking Table.

Abbreviations: A, acupuncture; AA, auricular acupuncture; EA, electro acupuncture; M, moxibustion; PI, point injection; ZN, traditional Chinese medicine; ZW, application of Chinese medicine; U, usual medicine therapy.
Nausea and vomiting
Out of the 111 papers that were considered, 36 studies were selected for examination of extractable data.19,33,39,43,46,52,56,59-61,64-67,73-75,77,78,81,82,85,91,94,96,98,101,102,106,107,111,114-116,119,121 The effects of 14 acupuncture modalities on the occurrence of nausea and vomiting in patients with cancer pain were evaluated, and compared with the network diagram between the interventions, see Figure 11. As can be seen from the network diagram below, a total of 16 interventions were included, with the largest U node, indicating the largest sample size, and the thickest A + U and U line segments, indicating the most comparative studies.

Nausea and vomiting network diagram.
Compared with U, the incidence of nausea and vomiting was lower in EA + U (OR = 0.11, 95% CI: 0.03-0.45) and M + ZN (OR = 0.21, 95% CI: 0.09-0.50), indicating that these interventions were associated with a lower rate of nausea and vomiting adverse events and higher safety, as shown in Figure 12.

Nausea and vomiting league chart.
According to the SUCRA table, U had the highest likelihood (SUCRA = 87.44%) of being used as an intervention for nausea and vomiting in patients with cancer pain. On the other hand, EA + U had the lowest incidence (SUCRA = 13.24%) of nausea and vomiting reactions (see Table 5).
Nausea and Vomiting Ranking Table.
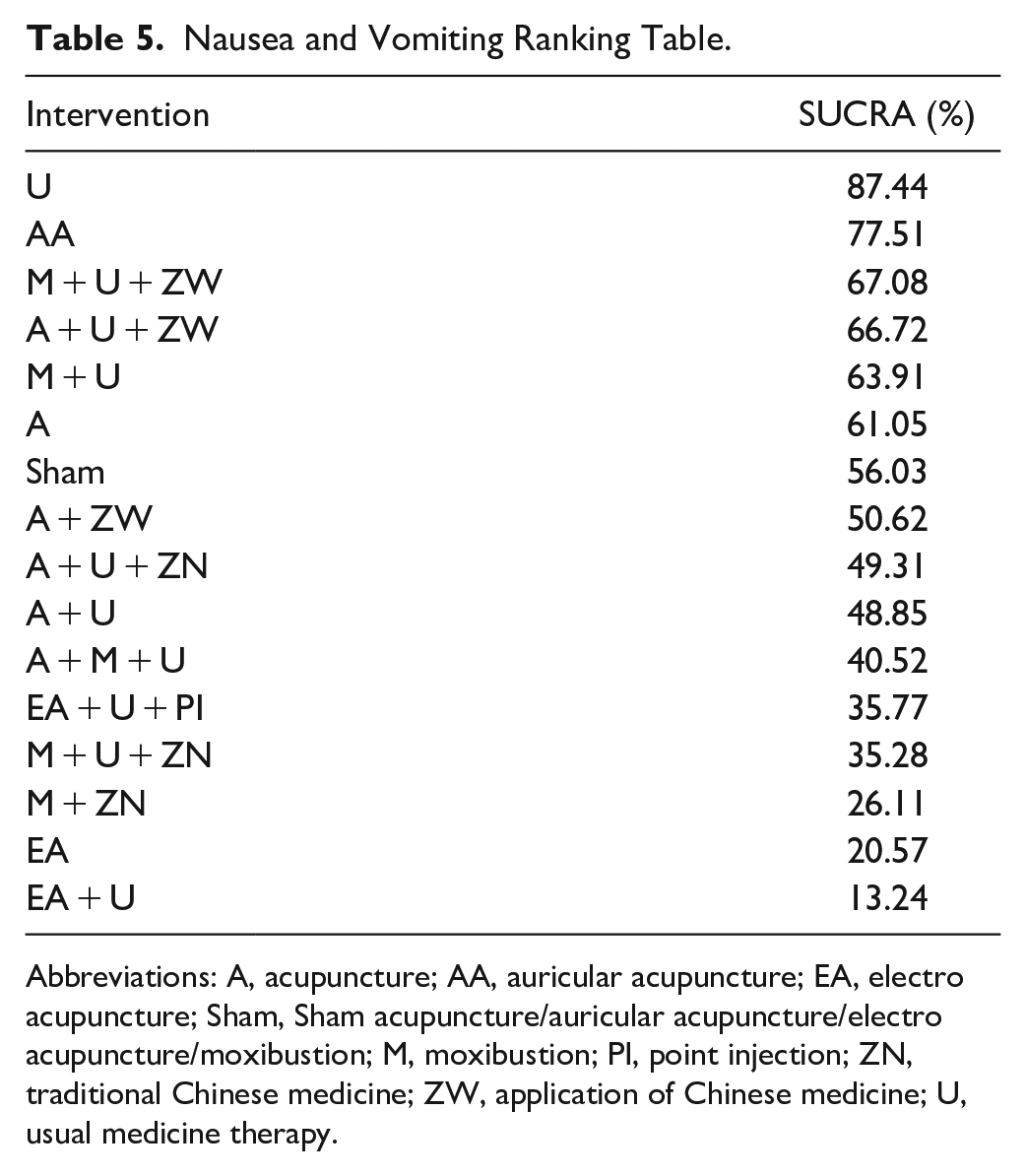
Abbreviations: A, acupuncture; AA, auricular acupuncture; EA, electro acupuncture; Sham, Sham acupuncture/auricular acupuncture/electro acupuncture/moxibustion; M, moxibustion; PI, point injection; ZN, traditional Chinese medicine; ZW, application of Chinese medicine; U, usual medicine therapy.
Dizziness
Out of the 111 studies considered, 18 were selected for the analysis of extractable data.19,33,39,40,46,59,61,64,66,75,77,98,101,106,107,111,115,121 The effect of nine acupuncture modalities on the occurrence of dizziness in patients with cancer pain were evaluated, and a comparative network diagram between interventions was constructed, see Figure 13. As can be seen from the network diagram below, a total of 11 interventions were included, with U having the largest node, indicating the largest sample size, and A + U and U line segments being the thickest, indicating that the most studies were compared.

Dizziness network diagram.
Compared with U, the incidence of dizziness was lower in A + M + U (OR = 0.29, 95% CI: 0.09-0.90) and A + U (OR = 0.44, 95% CI: 0.27-0.71), indicating that these interventions were associated with fewer adverse events of dizziness and higher safety, as shown in Figure 14.

Dizziness league chart.
Based on the SUCRA table, AA (SUCRA = 89.86%) was the most common intervention for dizziness in patients with cancer pain, and EA + U + PI (SUCRA = 25.59%) had the lowest incidence of dizziness, as shown in Table 6.
Dizziness Ranking Table.

Abbreviations: A, acupuncture; AA, auricular acupuncture; EA, electro acupuncture; Sham, Sham acupuncture/auricular acupuncture/electro acupuncture/moxibustion; M, moxibustion; PI, point injection; ZW, application of Chinese medicine; U, usual medicine therapy.
Publication bias
Comparative funnel plots were utilized to assess the publication bias of the six outcomes: NRS score, cancer pain relief, KPS score, constipation, nausea and vomiting, and dizziness, as depicted in Figures 15 to 20. The findings revealed a general presence of publication bias in the studies included, suggesting publication bias or a small sample effect in the randomized controlled studies incorporated.

NRS funnel chart.

Cancer pain relief funnel chart.

KPS funnel chart.

Constipation funnel chart.
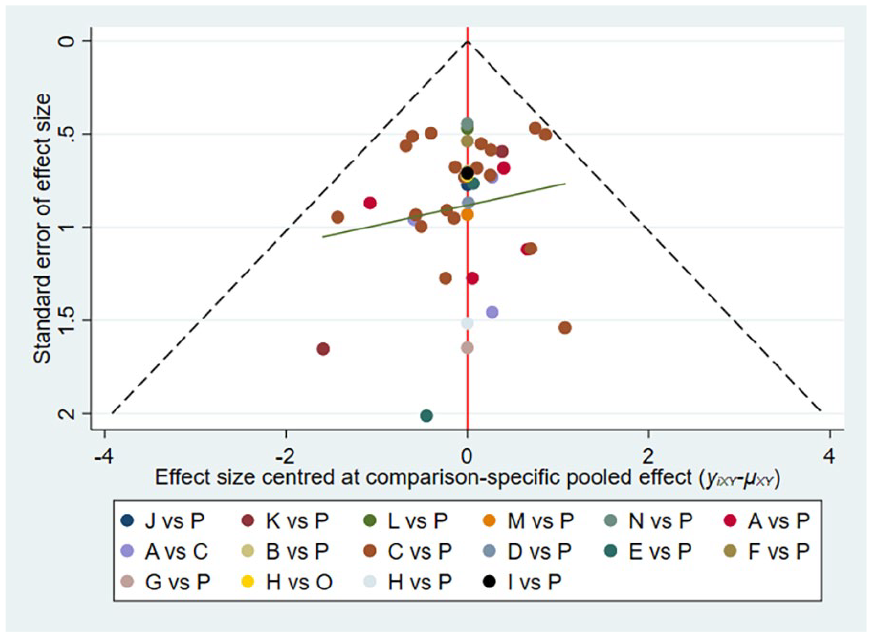
Nausea and vomiting funnel chart.
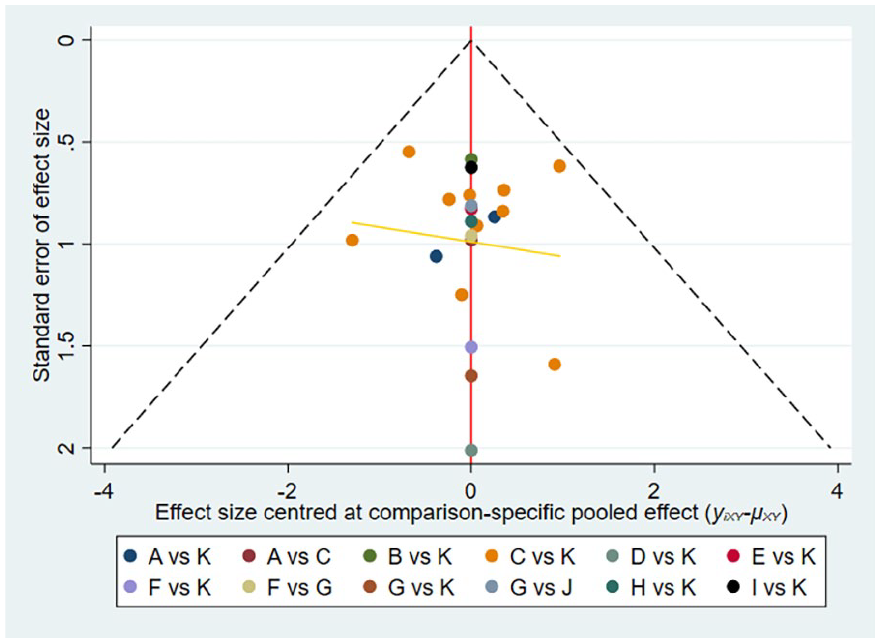
Dizziness funnel chart.
Discussion
Comparison of Results Interpretation with Previous Studies
This study aimed to assess and compare the effectiveness and safety of several acupuncture techniques in managing cancer-related pain. Our findings identified the most optimal intervention for alleviating cancer pain from the multiple acupuncture modalities examined. Due to limitations in the literature included for the outcomes of multiple intervention studies, we were unable to compare all interventions in each outcome. The results of the study are as follows:
For the alleviation of cancer pain in patients, we analyzed the NRS score and cancer pain relief effect of each intervention, and the top three interventions with significant effects were: A + ZN, A + AA + U, and EA + ZW. Acupuncture combined with traditional Chinese medicine or Western medicine has a favorable effect in the treatment of cancer pain. There may be some variation as the drugs used in each study vary, but the combination of needle and drug regimens has shown good efficacy.
For improving patients’ quality of life, we analyzed the KPS score through each intervention, and the top three interventions with significant improvement effect were: M + U, EA + U, and A + U + ZN. Moxibustion combined with conventional Western medicine treatment is effective in improving the quality of life of patients, and a large part of it may come from the warm and tonic effect of moxibustion on the human body.
For adverse events, the interventions with the least occurrence of constipation, nausea and vomiting, and dizziness were: A + ZW, EA + U, and EA + U + PI, respectively. Our study revealed that the use of conventional Western medicine resulted in a higher occurrence of adverse events compared to the combination of acupuncture and conventional Western medicine. Therefore, we suggest incorporating acupuncture and moxibustion into conventional Western medicine treatment could decrease adverse events in patients.
In the field of traditional Chinese medicine, the occurrence of pain syndrome can be summarized into two contents: “pain arises when there is no free flow” and “pain arises when there is a lack of nourishment,” and the treatment principles of traditional Chinese medicine for pain syndrome are mainly as follows: invigorating blood and removing stasis to relieve pain, and nourishing Qi (the essence of life) and blood to alleviate pain. Acupuncture therapy can not only treat the pain caused by Qi and blood stagnation and meridian blockage, but also strengthen the foundation, nourish Qi, and blood, and treat the pain caused by Qi and blood deficiency and deprivation of nourishment in the meridians.
In current pain management strategies, pharmacological treatment is usually the first choice, with opioids, nonsteroidal anti-inflammatory drugs (NSAIDs), and acetaminophen being the most commonly used medications. Due to the limited efficacy of NSAIDs and acetaminophen, most patients, especially those with cancer-related pain, often rely on opioids in the later stages of their condition. As a result, opioids have become the most commonly used treatment in cancer pain management. Although opioids are effective in alleviating pain, their long-term use is associated with significant side effects, such as tolerance, addiction, constipation, and gastrointestinal discomfort, all of which severely impact patients’ quality of life.123,124 The side effects of opioids have become a challenging issue in current pain management. Acupuncture, an important component of traditional Chinese medicine, is gaining increasing attention due to its simplicity, rapid effect, and remarkable therapeutic outcomes. With the advancement of modern acupuncture research, numerous studies have shown that acupuncture not only provides significant and rapid pain relief for cancer-related pain, but also has fewer side effects, higher safety, and the potential to reduce drug dependence, making it a promising alternative therapy. Therefore, acupuncture has become an important alternative therapy in pain management. 125 Studies have found that acupuncture combined with medication is more effective in improving pain relief in cancer pain treatment than using conventional cancer pain management medications alone and it can also reduce the adverse effects caused by opioids, offering higher safety.126,127 At the same time, acupuncture can effectively reduce the drug usage in patients who are dependent on opioids, thereby lowering the incidence of opioid addiction. 128 However, different acupuncture modalities have various levels, pathways and targets, and their efficacy and safety are also different. Another study showed no difference in the effectiveness of auricular acupuncture versus pharmacotherapy in pain relief, but auricular acupuncture combined with pharmacotherapy was more effective than pharmacotherapy alone in terms of pain relief and adverse effects. 129 A systematic review and meta-analysis of moxibustion found that moxibustion combined with drug treatment for cancer pain could improve the pain relief rate of patients, lower pain scores, shorten onset of analgesia, prolong the duration of analgesia, improve quality of life and reduce adverse drug reactions. 130 The efficacy of acupuncture for cancer pain has been proven, but there are many ways of acupuncture, and which method has the best effect on cancer pain needs to be studied, so the innovation of this study is to find the best intervention in acupuncture to relieve cancer pain.
The study identified A + ZN as the most effective intervention for alleviating cancer pain through acupuncture. Additionally, M + U was found to be the most beneficial intervention for enhancing patients’ quality of life. This may be related to the analgesic effects of acupuncture. Acupuncture can promote the release of adenosine triphosphate from fibroblasts, in order to bind to purinergic receptors. When ATP is rapidly degraded to adenosine, it binds to the adenosine A1 receptor, thus mediating analgesia. 131 At the same time, acupuncture can regulate neurotransmission in the central nervous system, including opioids, serotonin, norepinephrine, orexin, and endocannabinoids to induce analgesia. In addition, acupuncture can also reduce peripheral levels of cyclooxygenase-2 and prostaglandin E2 levels by acting on the hypothalamic-pituitary-adrenal axis, which strengthens the sympathetic nervous system and promotes the release of opioids to the periphery to achieve analgesic effects.132,133 Therefore, the efficacy of acupuncture combined with drug therapy may be more significant than that of acupuncture or drug treatment alone, and acupuncture combined with drug therapy can reduce drug-induced adverse reactions.
Strengths and Limitations of This Study
We conducted a thorough survey and statistical analysis on the effectiveness and safety of 24 different acupuncture methods in treating cancer-related pain. NRS score, cancer pain relief effect, KPS score and adverse events were used as outcome indicators, and the efficacy and safety of different acupuncture methods on cancer pain were compared and ranked, which provided treatment ideas and evidence-based support for clinical practice. There were also some limitations in this study. We included Chinese studies and did not conduct subgroup analyses by region or country. We included all tumor types but did not perform subgroup analysis by tumor type. Due to limited data, we did not analyze acupuncture point selection.
Summary
In this comprehensive meta-study, we analyzed the effectiveness of 24 acupuncture modalities in treating cancer pain. Through the data analysis and probability ranking analysis of NRS score and cancer pain relief effect, it was found that A + ZN may be the best intervention for cancer pain relief, M + U is the best solution to improve the quality of life of patients, and it is safer than drug treatment alone. However, due to some limitations in this study, high-quality, multicenter, large-sample randomized controlled trials are needed to verify the effects of different acupuncture on cancer pain.
Supplemental Material
sj-docx-1-ict-10.1177_15347354251314500 – Supplemental material for Efficacy and Safety of Different Acupuncture Treatments for Cancer-Related Pain: A Systematic Review and Network Meta-Analysis
Supplemental material, sj-docx-1-ict-10.1177_15347354251314500 for Efficacy and Safety of Different Acupuncture Treatments for Cancer-Related Pain: A Systematic Review and Network Meta-Analysis by Tianle Xie, Can Liu, Yudi Wu, Xiuxiu Li, Qianyun Yang and Jing Tan in Integrative Cancer Therapies
Footnotes
Acknowledgements
The authors thank the financial support of the Natural Science Foundation of China Youth Project [No. 82205296], Natural Science Foundation of Hunan Province Youth Project [No. 2022JJ1531], Hunan Provincial Department of Education Scientific Research Outstanding Youth Project [No. 21B0380], Innovation and Entrepreneurship Training Program for College Students in Hunan Province [No. S202310541034, No. 2020XJJJ008].
Authors’ Contributions
Tianle Xie and Yudi Wu designed the study and developed the retrieve strategy. Tianle Xie and Can Liu executed the systematic evaluation as the first and second reviewers, searching and screening the summaries and titles, assessing the inclusion and exclusion criteria, generating data collection forms and extracting data, and evaluating the quality of the study. Tianle Xie and Xiuxiu Li performed meta-analysis. Tianle Xie drafted the article, which was reviewed and revised by Qianyun Yang and Jing Tan.
Availability of Data and Materials
The data of this study can be obtained from the corresponding author according to reasonable requirements.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research of our article was funded by the Natural Science Foundation of China Youth Project [No. 82205296], Natural Science Foundation of Hunan Province Youth Project [No. 2022JJ1531], Hunan Provincial Department of Education Scientific Research Outstanding Youth Project [No. 21B0380], Innovation and Entrepreneurship Training Program for College Students in Hunan Province [No. S202310541034, No. 2020XJJJ008].
Ethics Approval and Consent to Participate
This is a systematic review and meta-analysis, ethics approval and consent to participate are not applicable.
Consent for Publication
Not applicable. The manuscript does not include the participant’s identification image or other personal or clinical details.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.