
Abstract
Background:
The prevalence of brain metastases (BM) in lung cancer patients is notably high and is associated with poor prognoses. The efficacy of standard treatment regimens in improving intracranial progression-free survival (IPFS) for lung cancer BM is markedly limited. While traditional Chinese medicine (TCM) has been effective in enhancing the quality of life and prognosis of lung cancer patients, its efficacy in treating BM remains unreported.
Case presentation
Here, we present a case of a middle-aged female with lung cancer BM, whose condition was assessed as progressive post-standard treatment including two local surgeries (both involving resection of cerebellar space-occupying lesions), stereotactic radiotherapy, chemotherapy and EGFR-TKIs. Subsequently, she underwent treatment with the traditional Chinese herbal formula gubenxiaoyi (GBXY). The patient was treated with GBXY for a total duration of 55 months. After treatment, a significant reduction of about 50% in intracranial lesions was observed, accompanied by an extension of both Intracranial Progression-Free Survival (IPFS) and Cognitive Deterioration-Free Survival (CDFS) exceeding 50 months.
Conclusion
These results demonstrate that in patients with lung cancer brain metastases (BM) unresponsive to standard treatments, GBXY not only has the potential to effectively prolong IPFS and decelerate cognitive decline, but may also contribute to a reduction in intracranial tumor burden. This suggests that GBXY could be a promising therapeutic option that warrants further investigation.
Keywords
Introduction
Brain metastases (BMs) manifest with notable frequency in the patient population grappling with lung cancer. Comprehensive studies delineate that the primary culprits of brain metastasis encompass melanoma, accounting for 28.2%, followed by lung cancer at a rate of 20%-30%, and renal cancer contributing to 10% of such cases. 1 Among individuals afflicted with non-small cell lung cancer (NSCLC), about 10.4% will eventually develop BMs, with this proportion increasing to 25% in stage IV patients. 2 The dire prognosis associated with lung cancer is closely linked to the presence of BMs. Studies demonstrate that NSCLC patients with untreated BMs have a median survival of approximately 2.8 months 3 The European Association of Neuro-Oncology (EANO) and European Society for Medical Oncology (ESMO) guidelines endorse surgical resection and stereotactic radiosurgery (SRS) as treatments. 4 Research has shown that patients receiving standard SRS treatment have a median cognitive-deterioration-free survival of about 3.7 months and a median overall survival of approximately 12.2 months, 5 outcomes that are still deemed unsatisfactory.
In China, traditional Chinese medicine (TCM) is extensively employed in lung cancer treatment. Jiang et al 6 have discovered that maintenance treatment with TCM, compared to maintenance chemotherapy, improves patients’ quality of life and yields a higher 1-year survival rate. Meta-analyses also indicate that the objective response rate (ORR), disease control rate (DCR), and improvement or stability in Karnofsky performance status (KPS) are significantly enhanced in advanced NSCLC patients treated with a combination of TCM and epidermal growth factor receptor tyrosine kinase inhibitors (EGFR-TKIs). Additionally, this combination therapy results in higher one- and two-year survival rates compared to EGFR-TKI monotherapy.7 -9 All these findings substantiate the effectiveness and safety of TCM in lung cancer treatment. However, the impact of TCM on brain metastases originating from lung cancer is seldom reported. Professor Wang Xiaomin, who has extensively worked in TCM oncology for decades and possesses considerable clinical experience, has formulated the Gubenxiaoyi decoction for effectiveness in treating lung cancer BMs.
This is the first case report on the treatment of brain metastases from lung cancer with traditional Chinese medicine, written strictly in accordance with the CARE (Case Report) guidelines. This case report presents a middle-aged female patient with lung cancer BMs. After undergoing standard treatments including two local surgeries, stereotactic radiotherapy, chemotherapy, and EGFR-TKIs, her intracranial lesions proliferated. Subsequently, she turned to TCM decoction treatment, resulting in lesion reduction. Currently, the patient’s intracranial progression-free survival (IPFS) has extended beyond 50 months, with an overall survival of over 7 years.
Case Presentation
Ethical Statement and Informed Consent
This study has been approved by the Ethics Committee of Beijing Hospital of Traditional Chinese Medicine affiliated with Capital Medical University (Approval Number: 2023BL02-122-02). The patient consented to the publication of all images, clinical data, and other data contained within the manuscript, and we have obtained written informed consent from the patient, ensuring that her name and family-related information will not be disclosed in the published article. Her personal privacy will be strictly protected.
Patient Information and Clinical Findings
A 40-year-old female patient presented at a local hospital in October 2016 with persistent headaches and was subsequently diagnosed with poorly differentiated adenocarcinoma (T2N0M1) of the right lung and left cerebellar metastasis. The general conditions of the patients are shown in Table 1.
Baseline Characteristics of Patient Before Treatment.

Abbreviation: ECOG PS, Eastern Cooperative Oncology Group performance status.
The histological conclusion is based on the pathological findings from the patient’s craniocerebral surgery.
For intracranial results, the modified response evaluation criteria for solid tumors version 1.1 guideline for evaluating brain metastases was used.
Cognitive function was assessed using the HVLT-R (Hopkins Verbal Learning Test—Revised).
From 2016 to 2017, the patient underwent two neurosurgical procedures for tumor resection. Postoperatively, gefitinib therapy was initiated following the first surgery. The treatment regimen after the second surgery included six cycles of chemotherapy (Pemetrexed:700 mg d 2 ; Carboplatin: 450 mg d 2 ) and 25 sessions of radiation therapy (Figure 1). Unfortunately, the final MRI during the last chemotherapy cycle revealed progressive disease (Figure 2). 10 The brain metastatic lesion increased in size from 2.2 × 1.5 cm before treatment to 3.3 × 4.1 cm after treatment. Consequently, the patient opted to use traditional Chinese medicine, seeking an alternative approach due to the lack of response to standard therapies.

Treatment process of the patient.

Comparison of MRI before and after standard treatment. (A) Long T1 and long T2 signals can be seen in the left cerebellar hemisphere, T2 flair is high signal, the size is about 2.2 × 1.5 cm, and enhancement can be seen in the solid part (10/2016). (B) Metastatic tumor recurrence, about 3.2 × 2.5 cm in size, with enhancement visible in the solid portion (1/2018). (C) The size of the tumor was 3.3 × 4.1 cm on review after standard treatment, with increased volume and solid components compared to the 1/2018 (6/2018).
At her initial consultation, the patient described experiencing cranial discomfort following radiotherapy, itching at the cranial surgery site, and nocturnal numbness in her left upper limb. Concurrently, she exhibited symptoms including general weakness, lethargy, frequent burping, bloating, and diarrhea. Her tongue was light red and dull, with a thin and white coating, and her pulse was small and deep. The patient, generally in good health, denies any history of smoking and reports no familial history of similar conditions. The patient’s initial MRI in October 2016 revealed that the left cerebellar hemisphere could be visualized with long T1 and long T2 signals, with a high T2 flair, measuring approximately 2.2 × 1.5 cm, and enhancement was seen in the solid portion (as shown in Figure 2A). After treatments, a follow-up MRI in 1/2018 revealed a recurrence of the tumor, which was approximately 3.2 × 2.5 cm in size (Figure 2B), and after receiving standard treatment, the MRI results revealed a tumor size of 3.3 × 4.1 cm (Figure 2C). It is worth noting that the patient first started using gefitinib in November 2016 and after 30 months, discontinued it due to inability to obtain higher therapeutic benefits (Figure 1). Her liver and kidney functions, blood count, and tumor markers were all within normal ranges.
Diagnostic Assessment and Therapeutic Intervention
We confirmed the patient’s condition through her MRI, CT scans, intraoperative pathology, and laboratory diagnostics. In addition to these methods, we employed traditional Chinese medicine (TCM) diagnostic techniques, which identified her condition as a combination of essence deficiency, coupled with blood stasis and toxin. Given the advanced stage of her disease, the TCM treatment principle was primarily focused on tonifying essence, detoxification and blood circulation.
We prescribed a Gubenxiaoyi (GBXY)-based herbal medicine for the patient. The formula consists of: 60 g Shudihuang (prepared rehmannia root), 30 g Bajitian (medicinal morinda root), 20 g Tusizi (Chinese dodder seed), 30 g Longkui (black nightshade herb), 30 g Baiying (bittersweet herb), 60 g Baihuasheshecao (Hedyotis diffusa), 60 g Banzhilian (Scutellaria barbata), 15 g Cheqianzi (plantago), 5 g Quanxie (scorpion), 3 g Wugong (centipede), 10 g Tuyuan (ground beetle), 60 g Tengligen (rattan pear root), 20 g Mubiezi (Cochinchina momordica seed), 10 g Shichangpu (grass leaved sweetflag), 10 g Chaihu (Chinese thorowax root), 10 g Huangqin (baikal skullcap root), 10 g Dannanxing (arisaema with bile), and 10 g Yujin (Wenchow turmeric root tuber). The 20 doses of the herbal formula are to be administered over 20 days, with one dose taken daily in two divided portions—morning and evening—for five consecutive days, followed by a two-day break. We advised the patient to soak the herbs in purified water for 40 minutes, then decoct the mixture twice, combining and reducing the liquid to 200 mL. The recommended times for medication are between 9:00 to 11:00 in the morning and 2:00 to 4:00 in the afternoon. Alongside the herbal formula, we advised the patient to continue her gefitinib treatment.
Intracranial Progression-Free Survival (IPFS) is the primary efficacy endpoint following treatment, while Cognitive-Deterioration-Free Survival (CDFS) serves as a secondary evaluation index.
We prescribe a 2 months course of treatment for patients at each follow-up visit, adjusting the prescription based on their symptoms. During follow-up, we noted excellent patient compliance, with standardized and timely medication use. At the patient’s fourth visit, we were pleased to observe a significant reduction in the size of the space-occupying lesion in the left posterior cerebellar region compared to earlier MRI results (Figure 3A). Notably, the patient’s symptoms, including arm numbness and constipation, especially when lying down, were completely alleviated, prompting us to modify her treatment regimen accordingly (Table 2).

Changes in cranial MRI of the patient during traditional Chinese medicine treatment. (A) Tumor size after traditional Chinese medicine treatment was 2.9 × 2.4 cm, decreased from 6/2018 (4/2019). (B) After continuation of treatment with traditional Chinese medicine, only a long T1 and long T2 with T2-Flair low signal was seen on follow-up, and no significant enhancement of cystic signal was seen (8/2023).
Changes in the Prescription of Chinese Herbal Medicine for Patients During Treatment.

GBXY is composed of 60 g Shudihuang (prepared rehmannia root), 30 g Bajitian (medicinal morinda root), 20 g Tusizi (Chinese dodder seed), 30 g Longkui (black nightshade herb), 30 g Baiying (bittersweet herb), 60 g Baihuasheshecao (Hedyotis diffusa), 60 g Banzhilian (Scutellaria barbata), 15 g Cheqianzi (plantago), 5 g Quanxie (scorpion), 3 g Wugong (centipede), 10 g Tuyuan (ground beetle), 60 g Tengligen (rattan pear root), 20 g Mubiezi (Cochinchina momordica seed), and 10 g Shichangpu (grass leaved sweetflag).
Subsequent MRI results at her sixth and eighth visits indicated a gradual reduction in the lesion size (from 2.62 × 3 cm to 2.41 × 3 cm). During the sixth visit, she reported experiencing sleep disturbances, dizziness, and cervical spine discomfort. Accordingly, we modified the herbal prescription to address these symptoms (Table 2).
Results and Follow-Up
After the patient’s last visit in 2019, she discontinued her medication in mid-February 2020 due to the impact of COVID-19. During this period, her CT results remained similar to the previous ones. There was noticeable alleviation in the discomfort and fatigue in the surgical area, with only occasional expectoration and episodes of nausea and vomiting. 267 days after stopping all treatment, the patient underwent a follow-up MRI, which showed that her condition had remained essentially stable.
Due to the incomplete regression of the patient’s original tumor and metastatic lesions, the patient continued to visit the clinic. The latest visit was on November 15, 2023. At this visit, the treatment outcome was assessed as partial remission (PR) 10 (Figure 3B). Since starting the therapeutic regimen, there has been a steady reduction in the size of the primary pulmonary lesion, which is now almost completely resolved (Figure 4). The patient achieved a CDFS and IPFS of up to 60 months. Figure 4 also includes the patient’s CT results for comparison. Notably, her quality of life has significantly improved compared to the period of previous treatment (Table 3) with no serious adverse reactions reported (Table 4). The patient continues her herbal decoction treatment and remains under our observation. The latest visit was on September 15, 2024. The patient’s condition remains stable, with no significant discomfort reported.
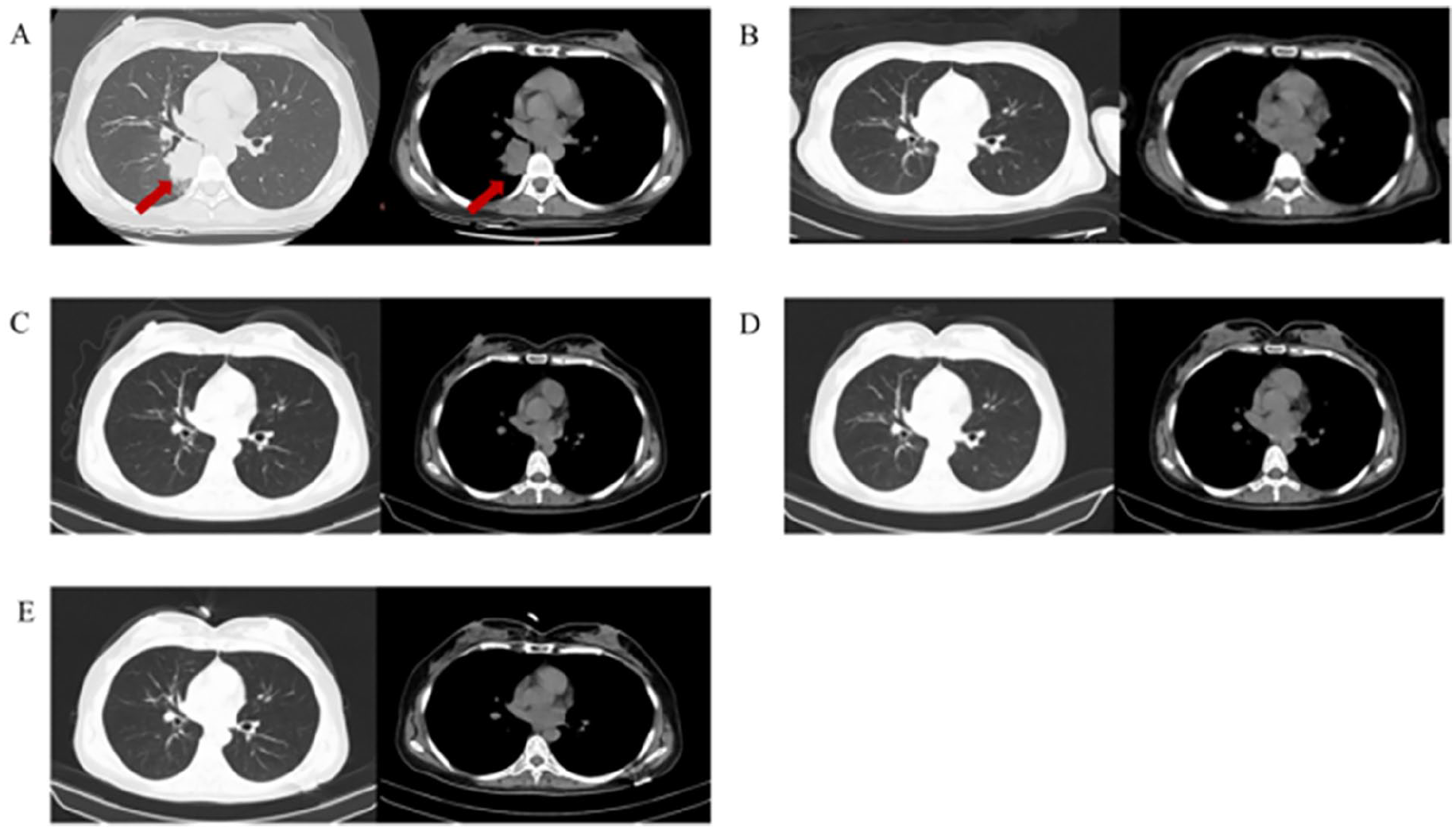
Changes in the patient’s chest CT since the initiation of treatment. (A) Solid mass shadow in the lower lobe of the right lung, about 4.0 × 3.9 cm in size (10/2016). (B-E) Image shows no solid mass (11/2017, 10/2018, 4/2019, 8/2023).
Comprehensive Evaluation of Treatment Outcomes in Patients Before and After Administration of the GBXY Formula.

Cognitive function was assessed using the HVLT-R (Hopkins Verbal Learning Test—Revised). A decline of one standard deviation in scores compared to the baseline is defined as cognitive function deterioration.
Abbreviations: TCM, traditional Chinese medicine; IPFS, intracranial progression-free survival.
The size of the tumor was assessed using Magnetic Resonance Imaging (MRI).
The modified response evaluation criteria for solid tumors version 1.1 guideline for evaluating brain metastases was used.
CDFS, Cognitive-Deterioration-Free Survival.
ECOG PS, Eastern Cooperative Oncology Group performance status.
Adverse Events Possibly Related to the Treatment Regimen.

Abbreviation: CTCAE, Common Terminology Criteria for Adverse Events.
Adverse effects were evaluated according to the National Cancer Institute Common Terminology Criteria.
Discussion
In this case report, we report a patient with lung cancer brain metastasis who experienced a reduction of approximately 50% in intracranial lesions after receiving Chinese herbal medicine after standard modern medical treatment failed. After receiving traditional Chinese herbal medicine treatment, the patient’s Intracranial Progression-Free Survival (IPFS) and Cognitive-Deterioration-Free Survival (CDFS) have both about 60 months, and the lung lesions have remained stable to date.
IPFS is widely used to evaluate the efficacy of intracranial metastatic tumors. Studies have shown that the median progression-free survival of lung cancer brain metastases treated with nivolumab and ipilimumab is 8.6 months (95% CI: 5.7-19.5), 11 while the median survival of patients receiving standard SRS treatment without cognitive deterioration is approximately 3.7 months, and the median OS is approximately 12.2 months. In this case, the patient’s IPFS extended to 60 months, significantly surpassing the outcomes of standard treatment regimens.
Traditional Chinese medicine has been shown to effectively enhance the quality of life for lung cancer patients and extend their survival period.8,9 Additionally, it exhibits notable efficacy in improving cognitive functions. 12 According to traditional Chinese medical theory, kidney deficiency and brain dysfunction are pivotal in the pathogenesis of cognitive dysfunction. Research indicates that Liuwei Dihuang Pill, following the principle of kidney tonification and essence replenishment, can decelerate the aging process in mice, mitigate cognitive impairments, and balance the neuroendocrine immune regulatory system 13 Morinda officinalis oligosaccharides have been observed to enhance memory, reduce brain tissue swelling and neuronal apoptosis in mice, and downregulate Aβ1-42. 14 Furthermore, Acorus calamus, known for its mind-stimulating properties, contains α- and β-asarone in its rhizomes, which play a neuroprotective role. These compounds alleviate oxidative stress, abnormal protein accumulation, neuroinflammation, and neurotrophic factor deficiency, thereby promoting nerve cell survival and activating various neuroprotective signaling pathways, 15 thus improving brain cognitive functions.
Traditional Chinese medicine posits that the fundamental pathogenesis of lung cancer’s brain metastasis involves a combination of blood stasis and toxin, coupled with essence and blood deficiency. As the core formulation of Professor Wang Xiaomin for treating this condition, Gubenxiaoyi comprises black nightshade herb, bittersweet herb, Hedyotis diffusa, Scutellaria barbata, Plantago, scorpion, centipede, Eupolyphaga, rattan pear root, Momordica cochinchinensis, prepared Rehmannia root, grass-leaved sweetflag, medicinal Indian mulberry root, and Chinese dodder seed. This formulation is designed to remove toxins, transform stasis, and nourish essence and blood. Research indicates that the aqueous extract of Solanum nigrum (AESN) significantly hinders MCF-7 breast cancer cells’ activity, activating caspase-3 and producing reactive oxygen species. By elevating E-cadherin levels and downregulating ZEB1, N-cadherin, and vimentin, AESN inhibits the EMT of MCF-7 breast cancer cells, thereby improving chemotherapy resistance 16 Ursolic acid, derived from Oldenlandia diffusa, can reduce vascular endothelial growth factor and transforming growth factor-β1 in cancer cells, inhibiting the expression of intercellular adhesion molecule-1 and matrix metalloproteinases, thereby decreasing lung cancer cell invasion and migration. 17 Scorpion, known for its detoxifying and nodular resolving properties, contains Margatoxin, which inhibits human lung cancer cell A549 proliferation and reduces tumor volume in nude mice. 18 Moreover, scorpion toxin exhibits broad-spectrum anti-tumor effects. 19 The methanol extract of Chaetomium globosum TW1-1, isolated from the ground beetle, contains novel cyclosporine alkaloids with inhibitory effects on various tumor cell lines, including liver, breast, and colorectal cancers. 20 SGR ethyl acetate (SGR-EA) exerts anti-tumor effects by inhibiting the HIF-1 signaling pathway and reprogramming tumor-associated macrophages to the M1 phenotype. 21 Rehmannia glutinosa polysaccharide (RGP) enhances NK cell activation and inhibits tumor growth in vivo in mice. 22
This case demonstrates that in lung cancer patients with brain metastases unresponsive to standard treatments, the traditional Chinese medicine (TCM) GBXY decoction can effectively halt the progression of intracranial lesions, prolong progression-free survival, and decelerate cognitive decline.
Of course, our research has certain limitations. In the realm of basic research, the active components, target sites, and mechanisms of action of GBXY remain to be elucidated. From a clinical research perspective, this study is based on a single case report. Consequently, there is a need for more comprehensive, rigorously designed randomized controlled trials to further verify the efficacy and safety of GBXY.
Conclusion
These results demonstrate that in patients with lung cancer brain metastases (BM) unresponsive to standard treatments, GBXY not only has the potential to effectively prolong IPFS and decelerate cognitive decline, but may also contribute to a reduction in intracranial tumor burden. This suggests that GBXY could be a promising therapeutic option that warrants further investigation.
Footnotes
Acknowledgements
We express our gratitude to the patient for her contributions to the advancement of medical science.
Author Contributions
Zhengzheng Yang conceptualized and designed the study. Zhengzheng Yang and Haiming Li co-authored the manuscript. Lei Chen was responsible for organizing and analyzing the patient’s radiological data. Shujiao Li participated in the case compilation. Taicheng Lu, Tongjing Ding, Dong Chen and Ruiyang Han engaged in the literature review. Xiaomin Wang served as the primary physician for the patient. Peiyu Cheng and Xiaomin Wang were in charge of the manuscript’s professional and scientific review. All authors have made substantive contributions to the manuscript and have read and agreed to the final version submitted for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.