
Abstract
Context
Due to therapeutic side effects and physical weakness, patients are not always able to carry out strenuous and lengthy exercises. Hence, this study investigated the effectiveness and feasibility of a short-term Whole-body electromyostimulation (WB-EMS) for oncological patients during and after anticancer treatment. The primary aim was to ensure the feasibility of WB-EMS training. Furthermore, the effects of WB-EMS training were investigated over a period of 2 weeks on parameters such as quality of life, body composition and physical performance.
Method
Thirteen cancer patients with different diagnosis, disease stages and treatment state were included. They participated in supervised WB-EMS sessions 4 times over a 2-week period. Physical functioning, body composition, depression, fatigue, and quality of life were measured before and after the intervention period. Moreover, a pre-post measurement of the patients’ perceived body constitution was conducted in every exercise session.
Results
All included patients (n = 13) were able to complete the 4 WB-EMS sessions. At the end of the 2 weeks, a significant increase of the muscle strength could be observed. Additionally, patients improved their cardiovascular fitness. The body composition analyses showed significant reductions in body lean mass and extracellular water. Muscle mass remained unchanged. Furthermore, patients reported an improved perceived body constitution reduced pain and discomfort following all 4 WB-EMS sessions.
Conclusion
This study suggests that WB-EMS is safe and feasible for cancer patients. Furthermore, it showed that even after 2 weeks, improvements concerning the physical performance and patient-reported outcomes can be achieved. This study indicates benefits of WB-EMS as short-term exercise methode in cancer patients, that could be utelised in fields such as cancer prehabilitation.
Trial Registration
This trial has been registered with the ISRCTN-Registry (ISRCTN68069634).
Keywords
Introduction
More than 18 million people worldwide were diagnosed with cancer in the year 2022. 1 Trends and projections predict a significant increase in the incidence of new cancer cases by 2040, with an estimated 29.5 million patients each year receiving a cancer diagnosis. 2 The rate of lethality in cancer cases continues to decrease. The reduced mortality rate can be attributed to modern diagnostics, various early detection programs, and improved and individualized forms of therapy. 3 However, cancer therapies can lead to several physical, psychological and cognitive impairments that can last throughout the medical treatment. These impairments are associated with a reduced quality of life and everyday functionality, but also may complicate the medical treatment. Fatigue and cancer cachexia (CC) are common cancer-related impairments. Patients with CC progressively lose skeletal muscle mass, leading to reduced muscle strength and, thus, decreased functional capacity. 4 Regular physical activity could be an efficient and cost-effective approach to stop muscle catabolism, reduce further side effects and to maintain or even increase the patients’ quality of life. Various studies show that exercise is feasible both before, during, and after completed therapy in different exercise intensities.5 -7 However, it is not always possible for patients to perform strenuous and time-consuming exercise programs due to physical discomfort, listlessness or fatigue. For that reason, whole-body electromyostimulation (WB-EMS) may be an interesting alternative form of exercise for cancer patients. WB-EMS applies simultaneous muscle contraction to all large muscle groups and is supported by easy-to-perform physical exercises such as a lunge. The efficacy of this method has been tested in athletes, elderly participants, and even patients with type 2 diabetes mellitus.8 -10 Until 2024, oncological diseases were considered absolute contraindications for the use of WB-EMS. 11 However, in recent years, various study protocols have demonstrated the feasibility and significance of WB-EMS for this patient cohort. Schink et al showed that applying WB-EMS to oncological patients is not only feasible but also associated with positive effects on the patients’ physical condition and performance, as well as a decreased burden of fatigue. In further subgroup analyses, the research group of Schwappacher et al12,13 confirmed the feasibility of WB-EMS for various types of cancer. Previous study protocols included an intervention period of 12 weeks. 14 We reason that WB-EMS could also be an interesting and promising exercise technology for shorter time periods such as the phase of prehabilitation. As an effective and beginner friendly exercise method, WB-EMS could be considered in patients whose operation is imminent. Therefore, the primary aim of this study was to examine whether 2 weeks of WB-EMS exercise are feasible and beneficial in cancer patients.
Methods
Study Design and Patients
This study was carried out as a single-arm trial in the University of Cologne, Germany. The study was approved by the Institutional Review Board of the Medical Faculty of the University of Cologne (reference number 17-165) and is registered in the ISRCTN Registry (ISRCTN68069634). From June to July 2019, Patient were recruited throughout the University Hospital Cologne and in-house exercise facilities. The majority of participants were already physically active and used to exercise before the intervention. Patients were eligible if they (1) are diagnosed with a solid tumor, (2) receive concurrent medical therapy, including chemotherapy, radiation, immunotherapy or were cancer survivors, receiving endocrine therapy (4) are over 18 years of age, (5) gave informed consent and (6) received medical clearance to exercise by a physician. In addition, participants were not allowed to be enrolled in any concomitant physical activity or nutritional therapy studies. Patients with acute severe cardiovascular or neurological diseases, were excluded from the study. Furthermore, patients with electrical implants (s.a. pacemaker or defibrillation), Osteosynthesis-related metal in the body or ongoing pregnancy were excluded. Based on the guidelines and contraindications from 2016 patient with acute venous thrombosis or major surgeries in stimulation areas (eg, Heart Surgery, Abdominal or Pelvic Surgeries, Orthopedic Surgeries, Neurosurgical Procedures) within the last 3 months were excluded. 15 Before and after the WB-EMS exercise period of 2 weeks, patients were assessed regarding physical performance, body composition and patient-reported outcomes. Additionally, before and immediately after every WB-EMS session the patient’s perceived physical condition was measured. The study was carried out in July to September 2019.
EMS Application
The patients performed 4 WB-EMS exercises sessions in 2 weeks. The training duration was 11 minutes in the first week, increasing to 20 minutes in the second week. The training was performed with an EMS device from Miha-Bodytech (Augsburg, Germany). Using 8 paired-electrodes, which were integrated into electrode vest and electrode belts for arms, legs and glutes, the major muscle groups of the core, lower and upper body were electrically stimulated. Patients wore special training cloth, which consisted of 47% Lyocell, 44% polyamides, and 9% elastane. Following the training recommendations of Filipovic et al and Kemmler et al, the following WB-EMS protocol was used: The type of impulse was set as biphasic at a frequency of 85 Hz and a pulse width of 350 μs. This led to a 4-second muscle stimulation followed by a 4-second resting period.16,17 During the electrical impulse stimulation, patients performed active body-weight movements such as Squats (Exemplary Protocol with exercises in the appendix). The intensity of each training session was controlled based on the participant’s subjective perception of effort using the RPE (Rate of Perceived Exertion; 0 = no exertion, 10 = maximum exertion) scale. Patients were instructed to aim for a WB-EMS intensity of a RPE of 4 to 5 in the first week and RPE 5 to 6 in the second week. The body weight exercise ratio of the lower and upper body and body core were balanced. The recovery time between 2 sessions was at least 48 hours.
Measures
Body composition was examined with a Bioelectrical Impedance Analysis (BIA), using the NutriPlus© software by Data Input GmbH. Endurance capacity was assessed as maximum reached load (W) in a modified step test according to the World Health Organization (WHO) protocol. The test was completed on a bike ergometer, starting with a resistance of 30 W and was increased by 15 W every minute until exhaustion (Borg scale > 18). Maximum hand strength was measured using the handgrip method (JAMAR 5030J1 hand dynamometer). Each hand was assessed 3 times and the best value documented. In addition, the muscle strength of the anterior thigh muscle (quadriceps femoris muscle) was measured using the hypothetical one-repetition maximum on a knee-extension machine from Milon GmbH (h1RM). Patients performed 3 to 8 repetitions till exhaustion and the one-repetition maximum was calculated with the Brzycki method.18,19 Due to an orthopedic injury in the area of the knee joint, the h1RM-assessment was changed to the chest press exercise in 1 patient.
Patient-Reported Outcomes (PROs)
Several patient-reported outcomes were measured before and after the 2-week intervention period. The Quality-of-Life Questionnaire (EORTC-QLQ-C30) developed by the European Organisation for Research and Treatment of Cancer was used to assess quality of life. 20 Additionally, patients filled out the Hospital Anxiety and Depression Scale 21 which records depressive and anxiety symptoms. Furthermore, the Multidimensional Fatigue Inventory 22 was used to determine the severity of the fatigue syndrome. In addition, patient rated their perceived physical condition using the German WKV-questionnaire 23 before and after every WB-EMS exercise session. The WKV-questionnaire contains 1 total score of perceived body constitution with 4 subscales (activated, agility, health, trained) and additional 2 items “physical pain” and “complaints.”
Statistical Analysis
Microsoft Excel (version 16.24, Microsoft Corporation) and the statistical program “SPSS Statistics 25.0” from the software company IBM (USA, Amonk) were used to present and analyzes the data. Mean comparison was performed using the Wilcoxon test or the dependent T-test. A significance level of P < .05 was set for the statistical analysis.
Results
Feasibility
A total of 15 patients were assessed for study eligibility (N = 15) (shown in Figure 1). Two patients (n = 2) could not be included in the study due to contraindications, leaving n = 13 included patients. Baseline characteristics of included patients are shown in Table 1.

Flowchart of the study process. The flowchart shows the number of recruited and enrolled patients, measurement time points, the assessments, and the intervention.
Baseline Characteristics of Included Patients.

Abbreviations: M = mean; SD = standard deviation; Min= minimum; Max = maximum.
No drop-outs were recorded during the study. Furthermore, all patients performed the 4 WB-EMS session during the 2-week intervention period, demonstrating a 100% exercise adherence. Regarding adverse events, 1 patient reported problems falling asleep in the evening after a training session. Apart from slight muscle soreness following an intervention session, no other adverse events were reported.
Body Composition and Physical Performance
After 2 weeks of WB-EMS, no significant differences could be shown in body weight, fat mass, BMI, skeletal muscle mass and phase angle. Significant differences were found in the lean mass (P = .028) and extracellular water (P = .03), shown in Table 2. Patients showed an increased aerobic performance (P = .041) as well as improved maximum strength of the knee-extensor (P = .008). No significant changes were observed in the handgrip strength.
Effects of 2 Weeks of WB-EMS on Body Composition and Physical Performance (P < .5).
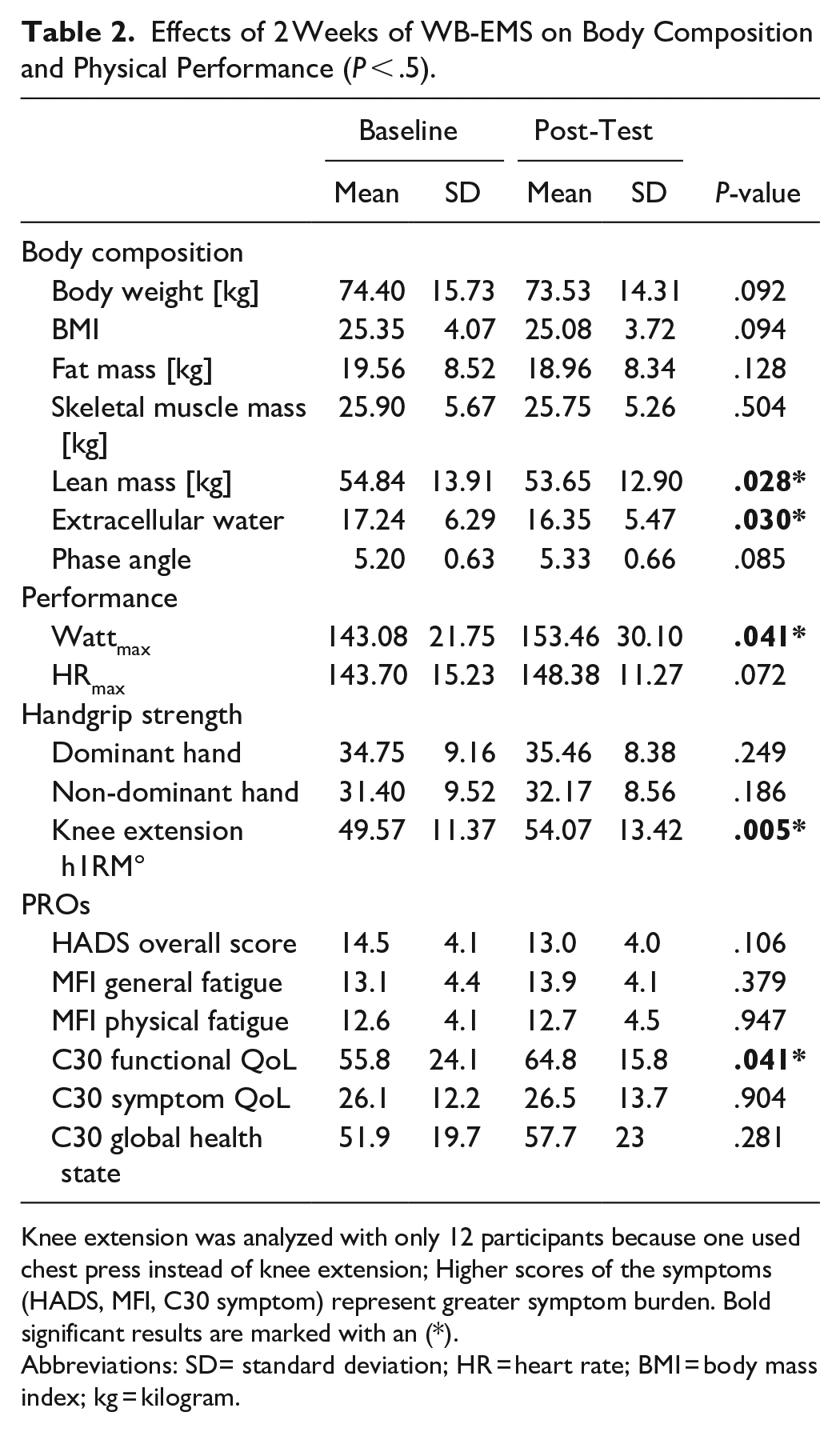
Knee extension was analyzed with only 12 participants because one used chest press instead of knee extension; Higher scores of the symptoms (HADS, MFI, C30 symptom) represent greater symptom burden. Bold significant results are marked with an (*).
Abbreviations: SD= standard deviation; HR = heart rate; BMI = body mass index; kg = kilogram.
Patient Reported Outcomes
The overall quality of life did not change after the intervention period. However, we observed improvements in the functional QoL (P = .041), whereas the symptom QoL did not change. The C30-questionnaire showed a significant reduction of dyspnea-symptom burden (P =.035). No other changes in were observed in symptom scales of the C30-questionnaire. Fatigue, anxiety and depression scores did not chance significant.
Mean Perceived Body Constitution
Patients showed an improved total score following all four WB-EMS training session (P < .08), indicating an increased perceived body condition after exercises (shown in Figure 2). Additionally, the questionnaire items of physical pain (P < .046) and discomfort (P < .026) decreased during each exercise session, that translates into a lower symptom burden. Only the second WB-EMS session was an exeption that showed no significant changes in the discomfort-item (P = .32) (shown in Figure 3).
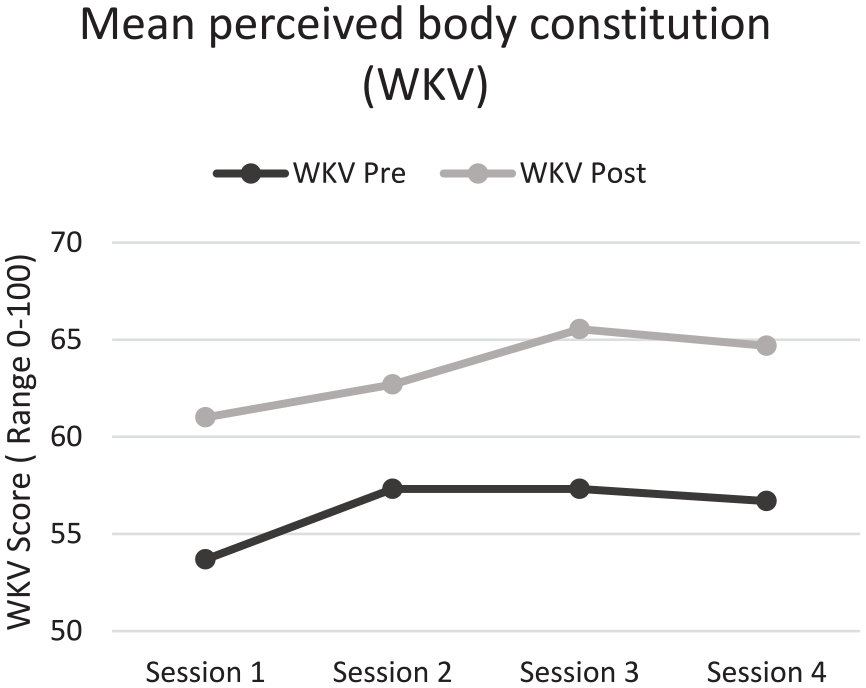
Mean change of overall score of perceived body constitution before and after every WB-EMS session. Scale: 0 (very bad) to 100 (very good).

Mean change of perceived pain and complaints before and after every WB-EMS session. Scale: 0 (none/low) to 5 (very/high).
Discussion
The here in described study investigated the feasibility of a 2-week whole-body electromyostimulation intervention in cancer patients. Significant improvements were archived in leg strength and aerobic performance (Wattmax) after 2 weeks of WB-EMS training. Body composition showed reductions in lean mass and extracellular water following the intervention. Additionally, patients reported improved functional quality of life after the 2-week of WB-EMS intervention. Every single WB-EMS exercise session resulted in a patient-reported increase of the perceived body condition and reductions of reported complaints and pain. As no previous study examined WB-EMS exercise as a short-term training method, this pilot study aims to address this research gap and consider WB-EMS as potential tool for prehabilitation interventions. Schink et al 24 demonstrated the feasibility and various positive effects of WB-EMS on physical performance and muscle mass in cancer patients following a 12-week WB-EMS intervention.
The 100% exercise adherence, no recorded drop-outs and no occurence of serious adverse events indicate that WB-EMS exercises were feasible and safe in cancer patients. The majority of patients were under chemotherapy and 5 of the participants had a metastatic disease. Contrary to expectations, no appointment was canceled for health reasons. The fact that the patients were already physically active before the study should not be ignored and might have influenced the results in terms of feasibility. Patients were accustomed to regular exercise and exertion. Most likely, the short study duration and time efficiency of WB-EMS training had favorable impacts on the adherence and drop-out rates as well. Comparatively, the 12-week study by Schink et al 14 recorded a drop-out rate of 39.6% in the WB-EMS group. No participant discontinued their involvement in the study due to discomfort or unfavorable incidents associated with WB-EMS training.
Hand strength was recorded using a JAMAR dynamometer. The handgrip strength of the participating patients were in line with reported reference values of 55-59 year old healthy adults.25,26 Due to the cancer disease and ongoing anti-cancer treatment, results below the average of the general population were expected. However, no significant changes of hand-grip strength were observed after the 2-week intervention. A larger sample size and a longer intervention period could confirm a more pronounced effect of WB-EMS on grip strength. On the contrary, endruance performance (Wattmax) and knee-extension strength increased following two weeks of WB-EMS. In the early phase of WB-EMS, force adaptations are primarily caused by neuronal adaptations and less by morphological adaptations. 27 This results in improved inter- and intramuscular coordination, which consequently leads to improved stability and power transmission, as well as stronger contraction within the muscle, which may explain the positive changes after such a short time period. Endurance capacity outcomes such as VO2peak or the results of the 6-minute walking test seem to be predictors of post-operative recovery in some cancer entities.28-30 Additionally, muscle strength in form of hand grip strength is associated with lower post-surgery complications in esophageal cancer patients for instance. 31 The herein observed potential to improve aerobic and strength capacity may indicate a potential use of WB-EMS in cancer care. For instance, an effective, short-term intervention could be useful in the field cancer prehabilitation.
A mean decrease of 1.2% body weight was recorded. One reason for the body weight reduction may be the concomitant decrease of body fat (3,1%). In addition, however, a 0.6% decrease in skeletal muscle mass and a significant 5.2% loss of extracellular water were also noted. Although both study protocols by Schink et al14,24 demonstrated that body composition changed positively concerning skeletal muscle mass, further research is needed to determine the extent to which WB-EMS training can influence body composition in short-term interventions. While some participants were already strength training 2 to 3 times per week prior to the start of the pilot study, it is possible that the intensity of the WB-EMS was too low, so that no increase in muscle mass occurred for this reason. Due to the individual sensitivity of the applied electrical stimulus, it has been additionally difficult to determine the current intensity that finally reaches the muscle. No intensities were deliberately stored after each training session, since especially in this target group the body constitution can vary from session to session. The risk of overestimation or demotivation in case of non-compliance with the previous electricity intensity should therefore be avoided. Studies that reported an increase of skeletal muscle mass and a reduction of fat mass following an WB-EMS intervention used longer intervention periods than the short-term protocol used in this study. 32
Contrary to expectations, we observed descriptive tendencies of increased fatigue and insomnia symptom burden even though it was not significant. Steindorf et al 33 and van Vulpen et al 34 reported positive changes regarding fatigue and insomnia after several weeks of aerobic exercise as well as a strength intervention in cancer patients during oncological treatment. In the 12-week study by Schink et al, 14 which also applied a WB-EMS to cancer patients undergoing acute therapy, there were no significant changes in pain and fatigue, but there were small improvements in these dimensions in this study as well. Our findings were accompanied by a verbal statement in which a patient talked about problems falling asleep in the evening after the WB-EMS training. For this reason and due to the novelty of WB-EMS, this should be considered and clearified in future research using WB-EMS. In the evaluation of the results of the perceived physical condition, it is not only noticeable that the average total score improved from pre- to post after every WB-EMS session, but also a continuous increase of the perceived physical condition in the postmeasurement from intervention unit 1 to 3 could be observed. In the fourth exercise session, the average total score decreased slightly again, but it was still higher than the score in the first and second exercise session. The result could be due to the fact that WB-EMS requires some familiarization, 17 so patients felt more familiar with the method from training session to training session, which may have had a positive effect on perceived physical condition. The control items “pain” and “discomfort” decreased in each exercise session from pre to post, confirming the improvement of the perceived physical condition of each exercise session. However, since these item scores always improved after a training unit, it can be assumed that the worsening of pain and discomfort is due more to the individual therapy phases of the patients than to the acute effect of the WB-EMS. These results are consistent with those of the other questionnaires used to query well-being. Another interpretive approach is to relate the worsening of pain to muscle soreness-like pain. However, participating patients reported the experiences with WB-EMS in a positive way. Already after the first intervention unit, 1 patient reported more stability when climbing stairs, which improved his everyday life. Another participant, who repeatedly complained of nausea, vomiting, and the resulting lack of appetite during the study period, informed the investigator at the end of the study that he had experienced an increased appetite after each training session. Unfortunately, these statements could only be partially visualized in the results. Nevertheless, they should not be disregarded in subsequent research.
To advance future research analyzing the effectiveness of a WB-EMS in cancer patients, the limitations of this pilot study must be listed. Subjects were recruited through the oncological exercise therapy program at CIO Cologne. The patients reported previous exercise history with individual exercising 2-3 times a week prior to the start of the pilot study. Therefore, it must be assumed that the participants were already in a training condition beforehand, which cannot be compared with untrained patients. It can be assumed that this influenced the effects and morphological adaptation phenomena of the training. Furthermore, it is challenging to make a statement about the suitability of this method for preoperative cases, as no patient underwent surgery following the 2-week intervention. Although significant differences could be generated despite the small number of subjects of 13 participants, a higher sample size, over a longer intervention period and an inactive patient collective (comparison or control group) would increase the significance of the pilot study. The study was retrospectively registered with the study registry “ISRCTN registry.”
Conclusion
The pilot-study has shown that WB-EMS is possible and feasible in oncological patients. Two-weeks of WB-EMS application showed positive effects in subjectively perceived physical functionality and quality of life in cancer patients, suggesting the potential of this exercise method even in short-term time-periods. The skeletal muscle mass did not change. We reason that WB-EMS could be of great value as training method in patients’ collectives who may not be able to perform conventional strength training protocols due to medical limitation (for instance: bone-metastasis), time-reasons or already prevalent muscle atrophy or cachexia. These patient collectives would be interesting to focus in future research trials including WB-EMS exercise. Furthermore, the observed effects of this 2-week intervention may suggest WB-EMS as promising approach for prehabilitative exercise interventions.
Supplemental Material
sj-pdf-1-ict-10.1177_15347354241304415 – Supplemental material for Short-term WB-EMS in Cancer Patients: Positive Effects After 2 Weeks of Exercise—A Single-arm Trial
Supplemental material, sj-pdf-1-ict-10.1177_15347354241304415 for Short-term WB-EMS in Cancer Patients: Positive Effects After 2 Weeks of Exercise—A Single-arm Trial by Jane Kersten, Timo Niels, Annika Tomanek and Freerk T. Baumann in Integrative Cancer Therapies
Footnotes
Acknowledgements
We thankfully acknowledge the support of miha-bodytec (Augsburg, Germany) which supplied the WB-EMS technology.
Author Contributions
Contribution JK: investigation, analysis, writing, review, and editing. TN: methodology, data interpretation, review, and editing. AT: investigation, data interpretation, review, and editing. FTB: conceptualization, methodology, supervision, resources, investigation, review, and editing.
Data Availability Statement
The datasets of the WB-EMS study are not public but can be requested from the corresponding author if required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funded professorship of F.T. Baumann is carried by the German Cancer Aid (Deutsche Krebshilfe e.V.)
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.