
Abstract
Background:
Women with gynecological cancer often experience psychological distress, particularly in response to surgical procedures. The impact of mandala art therapy (MAT) during the perioperative period for gynecological cancer patients remains uncertain. We aimed to examine the effects of the MAT program in women with gynecological cancer.
Methods:
Employing a quasi-experimental design, we recruited 126 gynecological cancer patients from a university hospital through convenience sampling. Participants were assigned to either receive the MAT program or standard perioperative care. The interventions comprised a three-session MAT program guided by a team of trained mandala psychologists. Generalized estimating equations (GEE) were employed to analyze the effects of MAT over time.
Results:
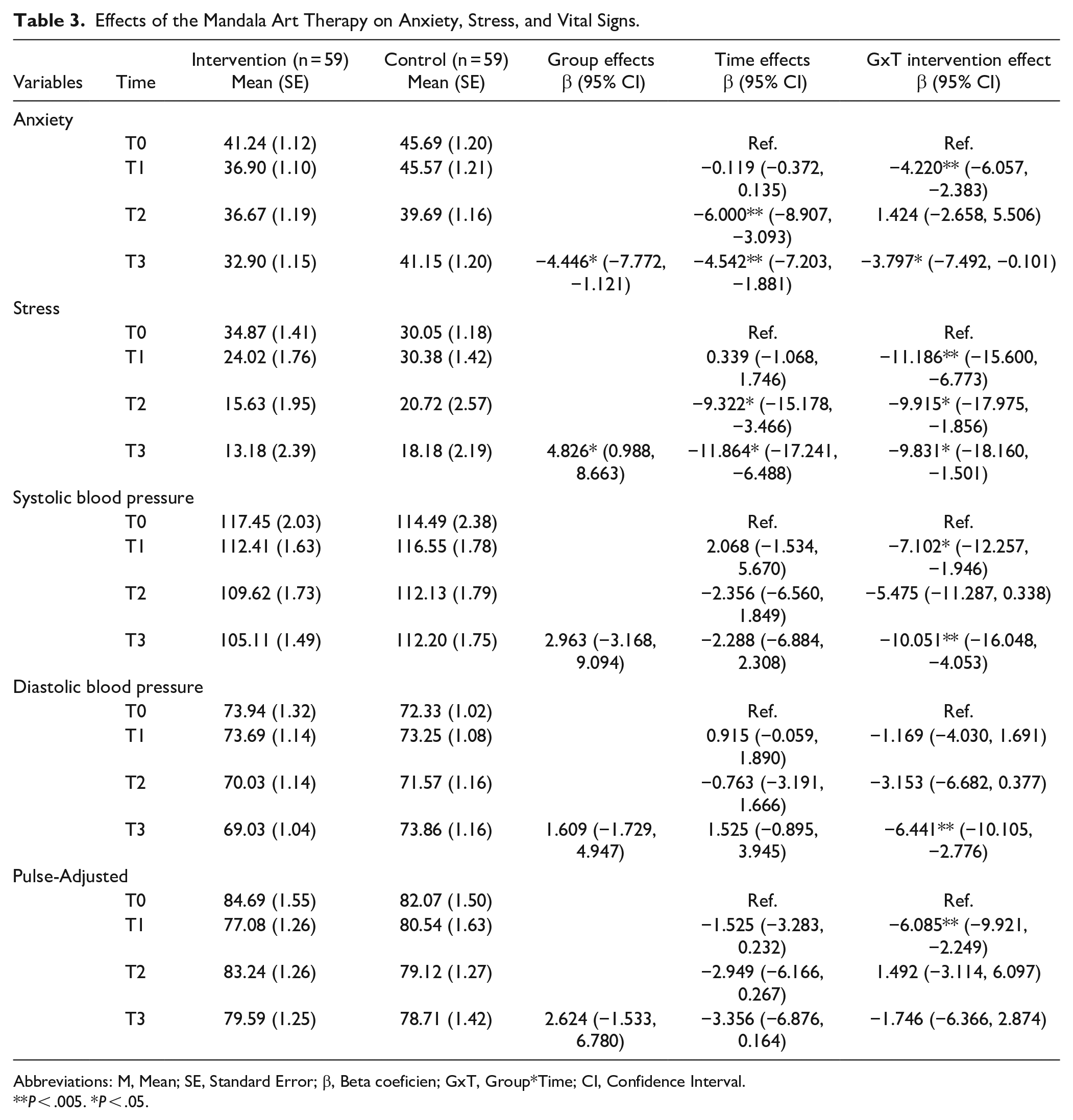
A total of 126 patients were enrolled, and 118 completed the entire study. Over 90% of participants completed the perioperative MAT interventions, reporting relatively high satisfaction with the program (7.70 out of 10). Individuals in the MAT group exhibited improved therapeutic effects on STAI-S, VASS, and vital signs over time. Notably, significant group*time interaction effects were noted in STAI-S scores at both the first evaluation, T1 (β = −4.220, P < .005) and the third evaluation, T3 (β = −3.797, P < .05), and VASS scores at T1 (β = −11.186, P < .005), T2 (β = −9.915, P < .05) and T3 (β = −9.831, P < .05). Regarding vital signs, the multivariate GEE model revealed significant interaction effects in systolic blood pressure values at both T1 (β = −7.102, P < .05) and T3 (β = −10.051, P < .005), diastolic blood pressure values at T3 (β = −6.441, P < .005), and pulse values at T1 (β = −6.085, P < .005). No significant differences were observed between groups for pain, hope, or self-acceptance.
Conclusion:
This study posited that MAT could serve as a valuable complementary approach in perioperative care for addressing the psychological needs of women with gynecological cancer. Subsequent research employing more robust methodologies and larger, more diverse participant samples will be necessary to validate these conclusions.
Introduction
Gynecological malignancies encompass cancers originating in women’s reproductive organs, including cervix uteri, corpus uteri, ovary, vulva, and vagina cancers, collectively ranking among the leading causes of female mortality globally. In 2020, 1 398 601 women were diagnosed, and 671 875 succumbed to gynecological cancers worldwide, 1 while in China alone, there were an estimated 252 010 new cases and 115 096 deaths in 2020. 2 The standard treatment for women with gynecological cancers often involves surgical procedures, such as hysterectomy, bilateral salpingo-oophorectomy, omentectomy, and pelvic lymphadenectomy. However, women diagnosed with gynecological cancers endure prolonged physical and mental burdens. Psychological challenges, including anxiety, depression, distress, heightened nervousness about the diagnosis and treatments, and even suicidal ideation are common.3 -5 Physical burdens encompass pain, fatigue, and memory loss. 5 Tumor resection, resulting in the partial loss of organs, can lead to functional and psychological disorders, characterized by alterations in body image, diminished self-esteem, and sexual dysfunction. 6 Psychological disorders directly impact treatment adherence, endocrine and immune function, and overall survival rates in cancer patients.7,8
The advent of art therapy, within the realm of complementary and alternative medicine, has significantly improved psychological outcomes for cancer patients. Expressive arts, which includes various forms such as music therapy, dance/movement therapy, poetry therapy, drama therapy, writing therapy, and mandala therapy, aim to enhance psychological well-being and inner peace through artistic expression. Individuals in the process of creating art explore their feelings, express emotions and thoughts, recharge and rediscover themselves, and achieve inner calm through artistic symbols and signs. Art therapy has gained recognition as a practical and applicable approach in addressing a variety of physical and psychological conditions, providing benefits such as improved affective conditions, relief from anxiety and depression symptoms, remission of cancer-related fatigue, enhanced quality of life, and increased perception of well-being and helpfulness in cancer patients.9,10
Mandala, originating from Sanskrit, represents a circle, center, integrity, and completion. Drawing a mandala involves starting from a fixed point in the center and gradually expanding to cover the entire circle of the mandala, offering a meditative approach for relaxation, release, and rejuvenation. The creation of a mandala is categorized into 2 broad types: coloring a given template inside or outside a circle (structured mandala), and drawing free figures in a blank circle (unstructured mandala). Mandala art therapy (MAT) is practiced in various settings, including hospitals, psychiatric centers, community health centers, long-term care centers, care homes, and schools. 11
In recent years, the application of MAT as a complementary approach for cancer patients has gained recognition. Studies have shown significant effects of an 8-session MAT program in alleviating anxiety and distress symptoms and promoting emotional awareness and acceptance.12,13 Additionally, a single-session MAT was found to alleviate anxiety and distress in breast cancer women undergoing chemotherapy. 14 A randomized controlled study demonstrated that mandala drawing effectively relieved anxiety and depression symptoms in hospitalized adolescents with cancer. 15 Women with gynecological cancer often experience psychological distress, particularly in response to surgical procedures. However, rapid rehabilitation shortens hospital stays, which may overlook the mental burdens experienced by patients. Therefore, a short complementary or alternative therapy during hospitalization is vital for establishing psychological well-being in gynecological cancer patients. Moreover, MAT intervention is simple and accessible, and requires no special equipment or artistic ability of individuals. However, the effects of MAT during the perioperative period in gynecological cancer patients remain uncertain due to a lack of evidence-based support from relevant studies.
This study hypothesized that individuals receiving MAT would experience an improvement in psychological distress through both subjective and objective measures. The primary objective was to assess whether MAT could alleviate perioperative anxiety and stress, relieve postoperative pain, and promote hope and self-acceptance in women with gynecological cancer.
Materials and Methods
Study Design and Participants
This was a prospective, non-randomized, controlled trial designed to evaluate the effects of mandala art therapy on the psychological well-being of gynecological cancer patients during the perioperative period. This trial was conducted at a university hospital in Chengdu City, Sichuan Province, China, which is one of the largest women's and children's hospitals in southwest China. A convenience sampling technique was used.
Women were considered eligible if they met all of the inclusion criteria: (1) diagnosed with any type or stage of gynecological cancer; (2) undergoing surgery; (3) aged 18 years or older; (4) capable of participating in this intervention; and (5) able to complete questionnaires in Chinese. Exclusion criteria included: (1) a serious physical or mental disease that could interfere with the intervention; (2) intellectual or cognitive impairment; (3) current engagement in mandala art therapy (MAT) practice; (4) severe perioperative medical complications; and (5) early withdrawal from the study. All participants provided written informed consent, and ethical approval was granted by the Ethics Committee of West China Second University Hospital, Sichuan University (Approval No. 2021-189).
Procedure
Recruitments spanned from October 2021 to November 2022 at the Jinjiang District of the West China Second University Hospital, Sichuan University, employing a convenience sampling technique. Research assistants screened potential participants for interest and eligibility. If a woman satisfied the inclusion criteria, showed an interest in this study, and was available for the scheduled activities, an enrollment visit was carried out to sign the informed consent and complete the admission assessments. On enrollment, participants were given the choice to participate in the MAT program. Participants who did not select to participate in MAT formed the control group and received standard care.
Methods
Formation of the mandala art therapy team
The MAT program was executed by a team comprising 4 clinical nurses, among whom 2 had received training in professional psychological counseling techniques, and 3 had completed accredited coursework in mandala drawing or drawing psychotherapy and obtained a drawing certificate. Prior to the intervention, all team members received unified training to ensure the homogeneity of implementation. Researchers also participated in each training.
Development of the mandala art therapy protocol
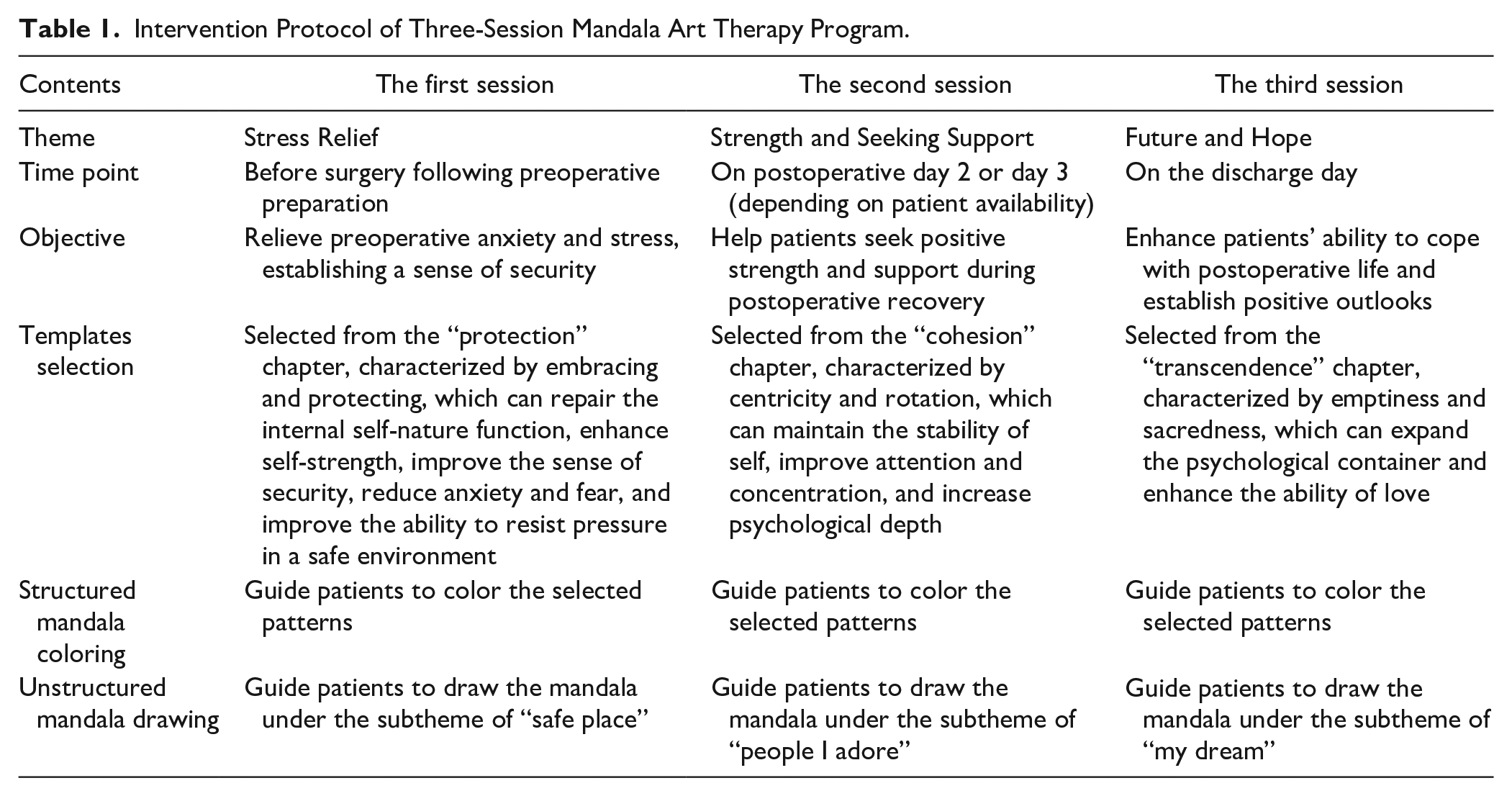
The three-session MAT protocol was developed under the guidance of Prof. Chen Canrui, a leading figure of mandala art in China and a senior consultant psychiatrist from Guangzhou Medical University. The interventions took place before surgery following preoperative preparation (T1), on postoperative day 2 or day 3 (depending on patient availability) (T2), and on the discharge day (T3). The mandala templates were selected from “The Road of Mind: Mandala Growing and Healing Picture Book,” 16 which was compiled by Prof. Chen Canrui. According to the different stages of psychological differentiation, it is organized into 7 chapters, namely, protection, differentiation, cohesion, integration, guidance, transcendence, and enlightenment. Considering the limited art-making experience of most patients, a structured mandala was initially chosen to improve the involvement of patients and provide a sense of security. In addition, 10 patients were selected for the trial test and their feedback was collected to modify the study protocol. The pilot data were not included in the final data analysis due to the revision of the protocol after the pilot study. The final intervention protocol is listed in Table 1.
Intervention Protocol of Three-Session Mandala Art Therapy Program.
Implementation of intervention and control
Participants in the control group received standard perioperative care as suggested at West China Second University Hospital, and completed measurements at 3 time points (T1, T2, and T3), mirroring the intervention group’s schedule. Standard perioperative care included basic nursing and caring, medication and parenteral treatments, diet and nutritional care, symptom management, illness and health education, and maintenance of psychological integrity at patients’ bedsides. For the intervention group, the MAT program was implemented alongside standard care. The MAT program comprised the following steps:
(a) Releasing and Relaxing the Body: Participants followed a music-based progressive relaxation.
(b) Selecting a Pre-drawn Mandala Template: Patients chose a mandala template prepared in advance.
(c) Coloring the Mandala: Colored pencils with 36 colors, A4 picture books, and erasers were provided for participants to color the mandala.
(d) Drawing Free Figures in a Given Circle: Patients engaged in free-form drawing within a designated circle.
(e) Sharing and Expressing Reflections: Participants shared their work and expressed reflections during the creation process.
The MAT team brought the three-session program to the patient’s bedside, allowing for convenient implementation. After initiating the activity, the researcher periodically left the bedside but returned every 10 to 15 minutes to monitor the patient’s progress and provide further assistance if necessary. Permission was obtained to share mandala drawings and their opinions about the work with the MAT team members. Each session lasted for 40 to 60 minutes, with the music progressive relaxation step taking around 5 to 10 minutes, the mandala coloring and drawing step lasting 30 to 40 minutes, and the artwork expression step spanning 5 to 10 minutes.
Outcome Assessment
Demographic and clinical characteristics were collected at the time of enrollment (T0). Patient-reported outcome measures (STAI-S, and VASS) and vital signs (blood pressure, and pulse) were gathered before surgery (T1), on postoperative day 2 or day 3 (T2), and on the discharge day (T3). Additionally, the Herth Hope Index (HHI) and Self-Acceptance Questionnaire (SAQ) were collected at T0 and T3, perceived waiting time was collected at T1, and pain intensity was collected at T2.
The state-trait anxiety inventory-state scale (STAI-S)
The STAI-S, developed by Spielberger et al 17 in 1970, comprises 20 items measuring immediate anxiety. The Chinese version (C-STAI) was translated by Li W et al 18 in 1995 and scored on a 4-point Likert scale (1 = almost never, 4 = almost always), with high reliability and validity among Chinese populations. 19 Overall, sufficient evidence of the reliability and validity of the STAI-S has been reported.18 -21
The visual analog scale for stress (VASS)
A single-question tool recommended by Mitchell et al 22 in 2008, the VASS uses a 100 mm line labeled from “no stress at all” to “most stress imaginable.” Participants rate their perceived stress on this ruler, providing a subjective score between 0 and 100. The evidence on the reliability and validity of the VASS has been well verified.23 -25 It is a reliable and valid tool widely used in both clinical and research settings.25 -27
Herth hope index (HHI)
Originally developed by Herth 28 and translated by Zhao et al, 29 the HHI comprises 12 items divided into 3 dimensions: temporality and future, positive readiness and expectancy, and interconnectedness. The Chinses version of HHI has been verified among Chinese patients and also showed good reliability and validity. 30 Scores range from 12 to 48 points, with higher scores meaning greater psychological hope. The HHI is a multi-dimensional scale, widely used in cancer patients.31 -33
Self-acceptance questionnaire (SAQ)
Developed by Cong et al 34 in 1999, the SAQ is a 16-item self-report scale with 2 dimensions: self-evaluation and self-acceptance. Scores range from 16 to 64 with higher scores meaning better self-acceptance. It has indicated good reliability and validity in Chinese populations and is frequently used in cancer patients.35,36
Pain intensity and satisfaction with MAT
Pain intensity was measured by the Visual Analogue Scale (VAS), a 10 cm line, where participants mark the severity of their pain from 0 (no pain) to 10 (most extreme pain imaginable). 37 The benefit of MAT was also assessed using the VAS, scoring from 0 (no benefit with MAT) to 10 (full benefit with MAT).
Perceived waiting time
Perceived waiting time was assessed by inquiring about patients’ feelings when waiting for surgery after preoperative preparation. Patients indicated their perceived waiting time on a 30-minute scale when the actual waiting time was 30 minutes.
Statistical Analysis
The sample size, determined using G*Power 3.1.9 38 and preliminary study data, indicated that 102 patients would provide sufficient power (α = .05, 1 − β = .8) to observe a moderate effect (f = 0.5) of MAT. With an estimated 20% loss to follow-up, 122 patients were enrolled.
Continuous variables were presented as mean (SD) or median (IQR) based on distribution, while categorical variables were expressed as numbers and percentages. Differences in baseline characteristics were assessed using the Pearson Chi-square or Fisher’s Exact test.
For single measurement data, independent t-tests or Mann–Whitney U tests were applied to compare between-group changes in continuous variables. For repeated measurement data, generalized estimating equations (GEE) were employed to assess MAT effects over time. Dependent variables included anxiety, stress, and vital signs (systolic and diastolic blood pressure, pulse). Independent variables comprised groups (intervention vs control), time points (T0, T1, T2, and T3), and group*time interactions. All multivariable models were adjusted for potential confounders, including demographic variables (age, education level, marital status, residence, and diagnosis), and baseline variables imbalanced between groups (surgical mode and stress).
Statistical analyses were performed using Statistical Package for the Social Sciences software (SPSS) ver.23, and significance was set at 2-sided P < .05.
Results
Patients Characteristics
A total of 126 patients were enrolled, with 118 completing the study (59 in the intervention group and 59 in the control group; Figure 1). Baseline characteristics were largely similar between groups, except for surgical mode (Table 1). Predominantly, the patients were married (84.7%), lived with family or friends (91.5%), and possessed a lower education level (51.7% with junior high school or below). Almost a third of patients had open laparotomy (31.4%). Of the included patients, 54 (45.8%) patients had cervical, 30 (25.4%) had ovarian, 21 (17.8%) had endometrial, and 13 (11.0%) had other gynecological cancer. Baseline comparison of outcome variables showed no significant differences between groups, except for the Visual Analog Scale for Stress (VASS) score. Detailed characteristics are summarized in Tables 2 and 5.

Flowchart on the study participants over the study period.
Demographic and Clinical Characteristics at Baseline.

Abbreviations: M, mean; SD, standard deviation.
Fisher Exact Test.
Mann–Whitney U-test.
P < .05. **P < .001.
Anxiety, Stress, and Vital Signs Changes During Interventions
As shown in Table 3, the multivariate GEE model revealed a significant group*time interaction effect in the STAI-S score at T1 and T3. The STAI-S score was reduced more in the intervention group than in the control group from baseline at both T1 (β = −4.339, 95% CI = −6.158, −2.520; β = −.119, 95% CI = −0.372, 0.135) and T3 (β = −8.339, 95% CI = −10.903, −5.775; β = −4.542, 95% CI = −7.203, −1.881).
Effects of the Mandala Art Therapy on Anxiety, Stress, and Vital Signs.
Abbreviations: M, Mean; SE, Standard Error; β, Beta coeficien; GxT, Group*Time; CI, Confidence Interval.
P < .005. *P < .05.
VASS score showed a significant group*time interaction effect at each time point, with greater reductions in the intervention group than in the control group at T1 (β = −10.847, 95% CI = −15.031, −6.664; β = .339, 95% CI = −1.068, 1.746), T2 (β = −19.237, 95% CI = −24.775, −13.699; β = −9.322, 95% CI = −15.178, −3.466), and T3 (β = −21.695, 95% CI = −28.057, −15.333; β = −11.864, 95% CI = −17.241, −6.488).
Systolic blood pressure (SBP) value exhibited a significant group*time interaction effect at both T1 and T3, indicating greater reductions in the intervention group than in the control group from baseline at both T1 (β = −5.034, 95% CI = −8.723, −1.345; β = 2.068, 95% CI = −1.534, 5.670) and T3 (β = −12.339, 95% CI = −16.192, −8.486; β = −2.288, 95% CI = −6.884, 2.308). Diastolic blood pressure (DBP) value showed a significant group*time interaction effect at T3, with more reduction in the intervention group at T3 (β = −4.915, 95% CI = −7.667, −2.164; β = 1.525, 95% CI = −0.895, 3.945).
Pulse value demonstrated a significant group*time interaction effect at T1, indicating greater reductions in the intervention group at T1 (β = −7.610, 95% CI = −11.020, −4.200; β = −1.525, 95% CI = −3.283, 0.232).
These findings suggest that the MAT program had positive effects on anxiety, stress, and certain vital signs during the perioperative period for gynecological cancer patients.
Pain Intensity, Perceived Waiting Time, and Satisfaction with MAT
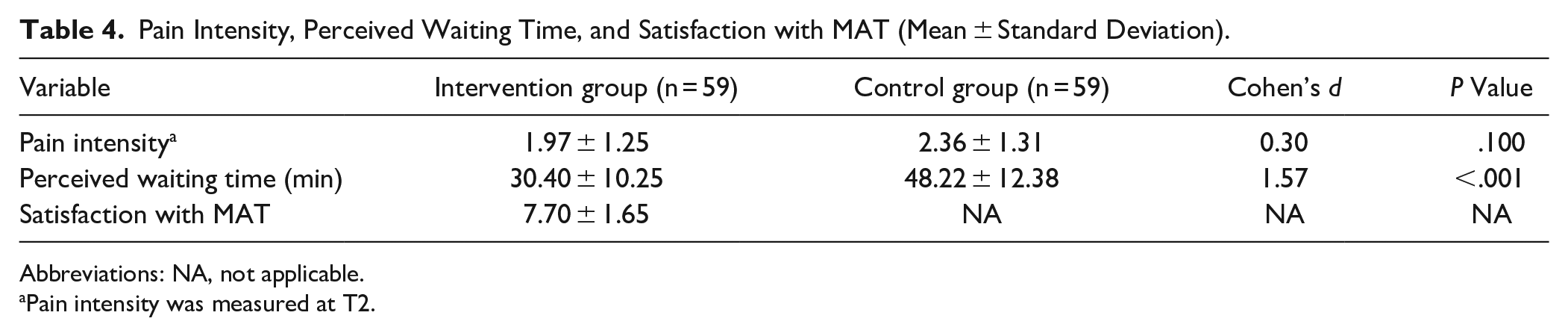
The intervention group experienced significantly shorter perceived waiting time compared to the control group (30.40 minutes [SD 10.25] vs 48.22 minutes [SD 12.38]). No significant differences in pain intensity at T2 between groups. The mean patient satisfaction score was 7.70 ± 1.65 (Table 4).
Pain Intensity, Perceived Waiting Time, and Satisfaction with MAT (Mean ± Standard Deviation).
Abbreviations: NA, not applicable.
Pain intensity was measured at T2.
Hope and Self-acceptance Outcomes
No statistical difference in Herth Hope Index (HHI) and Self-acceptance Questionnaire (SAQ) scores between groups, though the intervention group showed higher average HHI scores (Table 5).
Hope and Self-Acceptance Outcomes (Mean ± Standard Deviation).

Discussion
This study is the first clinical examination of the MAT program’s impact on perioperative anxiety, stress, pain, and hope in gynecological cancer patients. The findings indicate positive effects, with patients experiencing lower anxiety and stress scores, reduced vital signs (systolic and diastolic blood pressure, and pulse values), and shorter perceived waiting time.
Positive Effects of the MAT on Perioperative Anxiety, Stress, and Vital Signs
The MAT program significantly reduced anxiety in the intervention group as compared to controls, consistent with previous studies on breast cancer patients12 -14 (Table 3). Mandala coloring in early-stage breast cancer patients undergoing chemotherapy demonstrated a significant reduction in state anxiety scores. 14 A randomized clinical trial found MAT to be a feasible intervention for improving emotional processing in breast cancer patients. 13 MAT has also shown effectiveness in reducing anxiety in pediatric populations, as observed in hospitalized adolescents with cancer. A study performed by Gürcan et al 15 showed that mandala drawings had positive benefits on anxiety and other psychological symptoms. A qualitative study revealed that unstructured mandala drawings could help patients cope better with cancer, with respect to hope for healing and psychological growth. 39
Stress scores decreased significantly over time in the MAT group, aligning with the therapeutic goals of the intervention (Table 3). This result adds to the very limited evidence on stress relief in gynecological cancer patients. Only 2 reports suggest effectiveness in relieving stress in management employees with chronic widespread musculoskeletal pain 40 and multiple sclerosis patients. 41
The MAT group exhibited lower diastolic and systolic blood pressure, and pulse values compared with the control group (Table 3). Art therapy is associated with relaxation, increasing parasympathetic tone, and decreasing sympathetic activity. 42 Anxiety and stress are identified to increase blood catecholamine concentrations 43 and cause sympathetic hyperactivation and parasympathetic withdrawal. 44 Excitement of the sympathetic nerve is usually characterized by increased heart rate and blood pressure, while parasympathetic excitation is associated with a relaxation response. The perioperative period for gynecological cancer patients is marked by psychological distress, making MAT a valuable complementary therapy. MAT’s positive impact on psychological well-being and physiological responses suggests its potential as part of comprehensive perioperative care.
Impact of MAT on Perceived Waiting Time, Hope and Self-Acceptance
MAT participants showed significant improvements in stress and anxiety, aligning with the study focus. Perceived waiting time for surgery also significantly improved in the MAT group (Table 4). Long perceived waiting time is strongly associated with overall dissatisfaction. 45 Prolonged waiting time could induce greater uncertainty, which in turn affects patients’ anxiety. 46 Preoperative anxiety, generated by the unpredictable and threatening situations of surgery procedures, is highly frequent in patients awaiting surgery. 47 A higher degree of preoperative anxiety is associated with a surgical delay or cancellation, severe postoperative pain, frequent readmission, and even higher mortality.48,49 During the MAT program, preoperative anxiety significantly co-varied with perceived waiting time, with both manifesting an improvement in emotional burden.
However, there were no statistically significant differences between groups regarding hope and self-acceptance (Table 5), which is contrary to the findings of the 8-session MAT program by Kim et al. 50 . This indicates that intervention duration is an important influential factor. The intervention’s limited duration during the perioperative period may contribute to the lack of significant differences in hope and self-acceptance, as longer sessions may needed. According to previous studies, at least 8 sessions were recommended for cancer patients.12,13,51 The concept of “Enhanced recovery after surgery” (ERAS) has been increasingly developed in gynecological cancer surgery, aiming to shorten the length of stay and promote perioperative recovery. 52 In such a short hospital stay the psychological burdens of cancer patients could be neglected. In this study, the sessions are limited by the length of stay in perioperative patients, indicating that follow-up with MAT services once discharged is necessary.
Mechanism of the Positive Impacts of MAT
The theoretical foundations of art therapy remain underexplored, with art often seen as a clinical treatment, creative activity, or projective and analytical tool.53,54 The therapeutic process involves the creative interaction between the client and the therapist, 55 utilizing art as a non-verbal medium to gain insight into individuals’ inner worlds. Mandala art therapy, as a drawing language, emphasizes the expression of inner emotions and feelings, allowing individuals to forget past negative experiences and focus on the present. 56
Music progressive relaxation served to relax participants, divert mental focus from unpleasant experiences, and concentrate on the MAT. Tailored MAT programs, based on 3 different themes (“stress relief,” “strength and seeking support,” and “future and hope”), addressed the psychological needs of gynecological cancer patients during the perioperative period. Subthemes like “safe place” aimed at providing a sense of security, while “people I adore” encouraged seeking strength and support, fostering coping strategies with postoperative pain. Meaning-focused strategy is developed as an essential coping strategy during particularly stressful events, 57 by which individuals try to search for the meaning of life and re-establish personal resources. The MAT program represented a progressive process, gradually increasing internal strength and reducing external disturbances. Psychological disorders related to fear of cancer, death, organ loss, and treatment uncertainty were addressed through nonverbal cues and metaphors in the creative process.
Limitations
Despite the promising findings, the study has limitations. The study design, lacking randomization, might introduce selection bias as participants’ willingness and acceptance of the MAT program influenced group assignment. While this approach aimed to improve compliance and reduce withdrawal rates, it may limit the generalizability of the findings. Secondly, this study was conducted in a single university hospital, limiting the generalizability of our results. The relatively small sample size (126 patients) might impact the statistical power and the ability to detect smaller effect sizes. Additionally, the non-blinding of participants and study staff introduces the potential for performance bias. While blinding in behavioral interventions can be challenging, 58 efforts to blind outcome assessors could minimize assessment bias.
Conclusion
This study contributes valuable insights into the potential benefits of the MAT program for enhancing the psychological well-being of gynecological cancer patients during the perioperative period. The findings suggest that the MAT program, implemented by a trained team of clinical nurses, may offer a promising avenue for addressing perioperative anxiety, stress, and physiological responses. While the non-randomized design and single-center focus introduce certain limitations, the high adherence rate among participants in the MAT group underscores a positive acceptance of this complementary therapeutic approach. As this study offers a preliminary understanding of the positive effects, there is room for further investigation into the optimal frequency and duration of MAT sessions to maximize its therapeutic impact.
Footnotes
Acknowledgements
The authors thank all the women for participating in this study and all the nurses in the gynecological ward who delivered the intervention (Jiang Shasha, Tan Yan, and Hou Xinnan). We appreciate Prof. Chen Canrui from Guangzhou Medical University for his guidance on the research protocol of this study.
Author Contributions
Conceptualization: ZMQ, LX, HY, RJH; Design: ZMQ, LX, HY, RJH; Investigation: ZMQ, LX; Data management and analysis: ZMQ, LX; Manuscript first draft preparation: ZMQ, LX; Supervision and Manuscript Revision: HY, RJH. All authors read and approved the final version of the manuscript.
Data Availability Statement
The data from this study are available from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.