
Abstract
Objective:
To examine the feasibility and usability of EnergyPoints™, an innovative mobile health app that teaches and guides people with cancer to implement daily acupressure to self-manage their fatigue and sleep disturbances.
Methods and Intervention:
The study used an integrated agile, human-centered approach. Adults (age 18 years and over) with cancer experiencing at least moderate fatigue, and living in the Greater New York City community, were recruited from social media, patient advocacy groups, and referrals. Twenty participants (in 3 sprints of 3, 5, and 12) were video-recorded thinking aloud while using the app for the first time. They then used the app at home to self-administer acupressure (twice daily for 1 week) while continuously wearing a fitness tracker. Each participant completed an exit interview and modified Computer System Usability Questionnaire post-participation.
Results:
Participants were ages 40 to 76 years and 65% female; 65% were non-Hispanic white. Mean pass rates per ritual exceeded 80%. Users completed (totally or partially) greater than 90% of stimulating acupressure and 70% of relaxing acupressure rituals. Sprint 3 SPs totally completed at least 1 ritual 87% of the time. The majority agreed or strongly agreed the app was easy to use (90%), easy to learn (85%), easy to understand (75%), and effective in helping perform self-acupressure (85%). In an analysis of ease of completing 5 key tasks, all successfully completed the tasks; 3 users required some assistance. Of 654 usability statements, those coded as personal experience/context (197), content related to acupressure learning (105), and content related to the onboarding/profile (71) were most frequent. The design team integrated recommendations into the app before the next sprint.
Conclusions:
Findings supported feasibility and usability, as well as acceptability, and led to significant alterations and improvements. EnergyPoints™ offers an opportunity to mainstream acupressure and help cancer survivors self-manage their symptoms.
Introduction
This study examined feasibility and usability of EnergyPoints™, an innovative mobile health (mHealth) app that teaches and guides cancer survivors (adults with cancer during and following treatment) to practice daily self-acupressure to manage their symptoms. Fatigue and sleep disturbances, which are common, distressing, and debilitating symptoms of cancer and its treatment, negatively impact physical, emotional, and social health.1 -3 Up to 90% of cancer patients undergoing treatment experience fatigue; 30% may experience long-lasting fatigue. 1 Sleep disturbances affect up to 75% of patients and may exacerbate fatigue.1,4 -7
The therapeutic effects of acupuncture and acupressure on fatigue and sleep deficiency are based on Traditional Chinese Medicine meridian theory; stimulating specific points along meridians, a complex network of energy pathways throughout the body, increases flow of Qi (bioenergy) and alters the symptom experience. 8 The mechanisms for these effects are not fully understood but mounting evidence supports neurohormonal, immunomodulatory and connective tissue pathways.9,10 Acupuncture can improve cancer-related fatigue (CRF) regardless of cancer type, during or post-treatment, and frequency or duration of sessions11 -13 and is recommended for cancer survivors experiencing fatigue post-treatment. 14
Evidence also supports efficacy of acupressure for CRF and sleep deficiency.12,15 -20 A meta-analysis (14 trials, 776 participants) found acupressure significantly reduced general fatigue in cancer survivors (during and post-treatment), with a large effect size of −0.87, (95% CI, −1.19 to −0.55; P < .001). 19 Reviews of acupressure in numerous clinical populations including cancer indicated improvement in sleep quality.20 -23
Acupressure involves stimulation of acupoints without needles, is easy to learn and use, and can be performed anywhere after brief training.1,19 Traditionally, acupressure requires instruction by a skilled practitioner and is not covered by insurance—potential critical barriers to adoption. mHealth technology can inexpensively teach and guide cancer survivors to practice and sustain simple acupressure protocols24 -26 to be used alone or with other approaches to manage CRF and sleep deficiency.
EnergyPoints app (see Figure 1), for iOS and Android devices, educates and guides users to implement 2 evidence-based rituals: Stimulating Acupressure (SA) and Relaxing Acupressure (RA). These point combinations are usually prescribed to treat low energy/weak immunity and stress/insomnia respectively.27,28 A randomized controlled trial (RCT) supports efficacy of these 2 protocols for CRF and sleep deficiency. 29 A follow-along format guides administration of correct point stimulation for 3 minutes per point. There are 10 points in SA and 9 points in RA. The learning platform provides 3 approaches: video, image, and text. A timer monitors duration of pressing each point; there is an optional dong at the end of 3 minutes. At the end of each point, a pop-up asks about the deqi experience (a feeling of tenderness or soreness at the point indicating energy flow). The app syncs symptom self-reports using NIH PROMIS® (Patient-Reported Outcomes Measurement Information System) measures 30 with fitness tracker (eg, an Apple Watch or Fitbit) sleep and activity data, 31 allowing evaluation of response to acupressure.

Sample EnergyPoints app screen shots.
This human-centric, agile study examined the feasibility and usability of EnergyPoints.32,33 The first aim (feasibility) was to confirm survivors could use the app to self-administer 2 acupressure rituals accurately (greater than 80% pass rate) and consistently (greater than 70% adherence over a week). The second aim was to assess the usability of the app and the fitness tracker. The criterion for acceptability was that more than 80% of patients would find key features of the app and fitness tracker as efficient, easy to use, likable, relevant to task, and acceptable (or easily modifiable). Results informed iterative improvements based on user experience.
Methods
The study followed ethical guidelines from the Helsinki Convention and was approved by the University of Utah Institutional Review Board (IRB) (protocol #142766, approved 6/10/21) which agreed to serve as a Single IRB under a reliance agreement.
Design
The agile approach included 3 sprints of user experience evaluation (n = 3, 5, and 12); a sprint is a time-limited cycle in which user feedback is used to make improvements. In this observational study, data were collected within each sprint in 3 steps over 8 to 10 days. In Step 1 (in-person session with Research Coordinator), participants (a) set-up a provided fitness tracker (Fitbit or Apple Watch) and linked it to EnergyPoints, (b) completed a video-recorded think-aloud walk-through of the app prototype while their screen was captured and recorded, (c) used the app learning platform and guided acupressure session to locate the acupoints (with a colored dot sticker) for 2 rituals (SA and RA), and (d) provided feedback in a short debriefing interview. In Step 2 (at home), participants used the app for 1 week with instructions to perform acupressure twice daily (SA in the morning and RA in the evening) and wear the fitness tracker 24/7 (except when charging). In Step 3 (online and video-call), participants completed an online survey and exit interview to provide feedback on their experience and make recommendations to improve the app. Improvements to the app were made before beginning a new sprint.
Setting and Sample
Participants completed Step 1 in the 5 Point App offices in New York City, NY and Steps 2 and 3 remotely. Sample inclusion and exclusion criteria are detailed in Table 1. After Sprint 2, some of the screening questions were clarified. Participants (n = 20) were recruited from social media, patient advocacy groups, and referrals. Interested cancer survivors completed an online screening survey. Research staff contacted them to confirm eligibility (with verbal consent), sent the informed consent document for review, and set up an in-person appointment during which the Research Coordinator obtained written informed consent.
Sample Inclusion/Exclusion Criteria.

After Sprint 2, several of the criteria were modified to increase participation; changes were approved by the IRB and implemented in Sprint 3.
In this type of feasibility and usability testing, a sample size of at least 10 has been recommended; similar research has shown that the minimum percentage of problems identified rose from 55% to 82% and the mean percentage of problems rose from 85% to 95% when the number of users was increased from 5 to 10. 34
Data Collection
The team used multiple methods of data collection, both quantitative and qualitative: video-recordings, app data, fitness tracker data, and a modified Computer System Usability Questionnaire (CSUQ) 35 and exit interview (see Box 1). Participants received $300 compensation for the 2 data collection episodes and kept their fitness tracker.
Details of Data Collection.

Data Analysis
All quantitative data were exported into Excel or SPSS© and analyzed primarily with descriptive summary statistics. We explored changes in symptom reports using paired t-tests. Interrater (acupuncturists) reliability for point location accuracy was assessed using percent agreement and intraclass correlation (ICC). Pass rate was calculated by (1) computing for each participant a percent pass score (correct response across 3 raters) for each point, (2) then computing the ritual pass rate for each participant (mean across points), and (3) computing the group mean of pass rates for each Sprint. We set an a priori milestone of an 80% pass rate for Sprint 3; this allowed for improving the learning platform based on Sprint 1 and 2 results. Similarly, a percent completion score was created for each ritual for each participant. These were coded as total (100% completion) and partial (at least 1 point missed). The frequency of total and partial were computed for the week. The assessment of fitness tracker data focused on feasibility of collecting the data and synchronizing it with the app.
Analysis of qualitative data focused on usability analysis.36,37 Research staff (SB, JM, and KB) listened to and corrected Otter 38 artificial intelligence transcriptions of each video highlighting relevant text. They forwarded suggested modifications to the development team after each sprint. Each text unit yielded a unique usability statement that was coded for location and type of problem. Specific data regarding task completion, previous use of health apps and integrative medicine, and any problems encountered were analyzed separately.
Results
Of the 82 completing on-line screenings, 27 (33%) were eligible. Main reasons for exclusion were living outside the greater New York area (n = 25) and previous use of acupressure (n = 17). Of the 27 eligible, 20 (74%) consented to participate; 100% of those enrolled completed the study.
Demographic characteristics are summarized in Table 2. Participants were aged 40 to 76 years; 65% female; 65% non-Hispanic White. Participants had ten types of cancer (40% had breast cancer) and included all cancer stages at diagnosis. Time since diagnosis ranged from less than 6 months to more than 10 years. Most (65%) were on active treatment. A majority (60%) reported no comorbid diseases known to affect fatigue and sleep. Of the 8 with comorbid conditions, arthritis was most common (n = 4). Most (85%) were taking medications that might affect fatigue or sleep, from 1 to 6 with a mean of 2.35 (SD = 1.84). Use of other nonpharmacologic strategies for fatigue and sleep ranged from 0 to 9, Mean 4.00 (SD = 2.75). The most common nonpharmacologic strategies used were increasing rest by napping (55%), meditation, (50%), relaxation exercises including deep breathing (50%), regular exercise (45%), and acupuncture (40%).
Sample Demographic Characteristics (n = 20).

The first aim was to confirm participants could accurately and consistently self-administer 2 acupressure rituals. Interrater agreement was 92.4% for SA and 92.9% for RA (see Table 3); Intraclass Correlation Coefficient was 0.75 (P < .01), considered Good. 39 Mean pass rate for Sprint 3 was 88% for SA and 81% for RA. A few participants voiced uncertainty about locating specific points and wished there was a process to “check point accuracy.”
Average Pass Rates (n = 20) and Interrater Agreement (k = 3) in Locating Acupoints in Each Ritual.

Pass rate was calculated by (1) computing for each participant a percent pass score (correct response across 3 raters) for each point (2) then computing the ritual pass rate for each participant (mean across points), and (3) computing the group mean of pass rates for each Sprint.
Analysis of Sprint 3 app data for point completion and duration was used to assess consistency of use. Sprint 3 SPs totally completed at least 1 ritual 87% of the time and both rituals 68%. On average, Sprint 3 participants completed 73.8% percent of total SA rituals and 20.2% of partial SA rituals; 52.6% of total RA rituals and 20.2% of partial RA rituals. Results from the CSUQ reflected concern about the daily time commitment (lowest scored item). Only 25% agreed or strongly agreed that “the amount of time involved in using this app has been a good fit for me.” Likewise in exit interviews, 32 statements (4.9%) were coded as “ease of fitting into life” which included many comments about the time commitment. Survivors asked for “an express version” and flexibility in scheduling day-by-day according to the context of what was happening in their life.
The second aim was to assess the usability of the app and the fitness tracker. All users completed the online survey within 3 days of finishing the app usage and took an average of 10 minutes to complete. The majority agreed or strongly agreed that the app was easy to use (90%), easy to learn (85%), easy to understand (75%), and effective in helping perform acupressure (85%). Mean scores on the CSUQ subscales are summarized in Table 4. Most participants did not have previous experience with a fitness tracker and wanted more orientation.
End of Study Questionnaire: Total and CSUQ Subscale Scores.
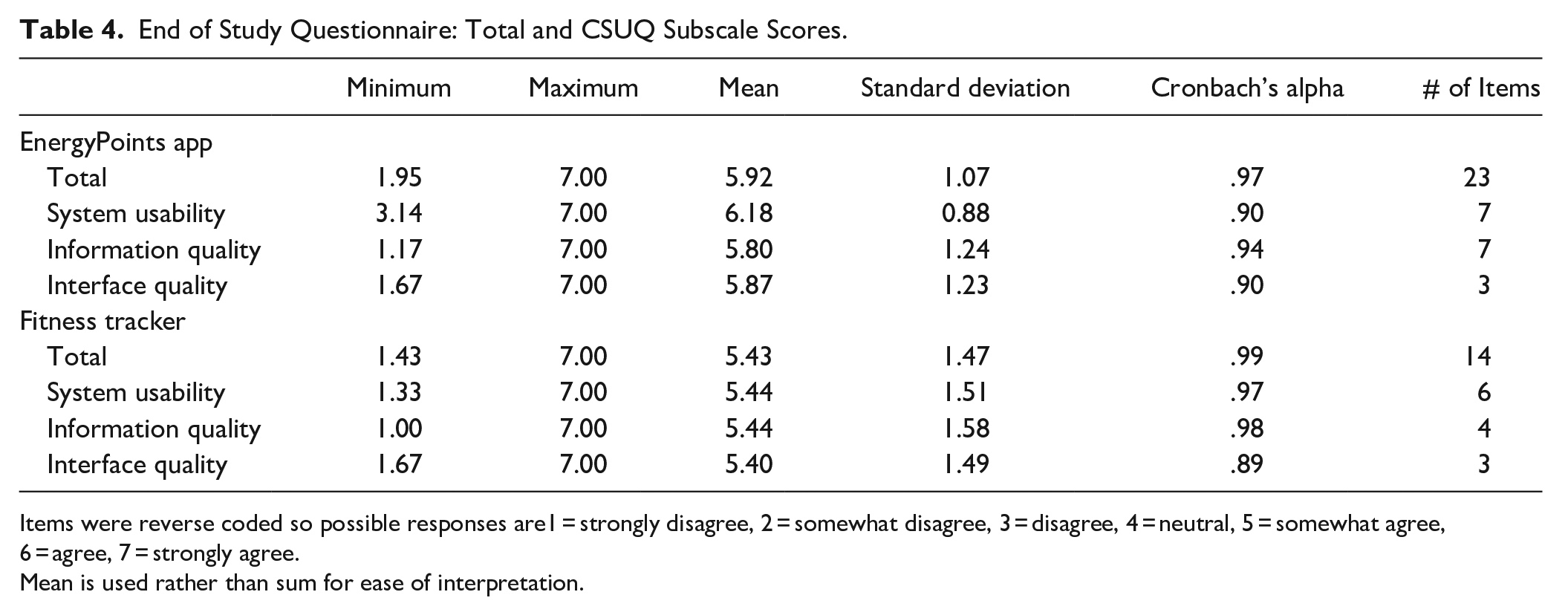
Items were reverse coded so possible responses are1 = strongly disagree, 2 = somewhat disagree, 3 = disagree, 4 = neutral, 5 = somewhat agree, 6 = agree, 7 = strongly agree.
Mean is used rather than sum for ease of interpretation.
Research staff (SB and KB) rated how easily each participant completed 5 key tasks based on the videorecording and transcript from the Think-Aloud session (see Figure 2). All were able to complete the tasks; 3 participants required some assistance. There were 654 usability statements (problems and neutral statements) generated with supporting quotations from multiple sources of qualitative data. The density of codes is represented in Figure 3; statements coded as personal experience/context, content related to acupressure learning, and completing the onboarding and baseline profile, were most frequent. Supplemental Material 1 provides a summary of sample quotes and app modifications for the top 3 occurring subcodes in each major category. Nearly all participants requested music or sound during the 3-minute acupoint “pressing time.” Supplemental Material 2 provides examples of the 319 positive statements by users across ten categories ordered by frequency. Positive comments about the app included that it was “clear,” “well-organized,” “easy to use and learn the points,” “straightforward,” and “intuitive.” One participant did not like the app and had difficulty locating the points, saying he was not a visual person. Most liked the learning platform and commented on the value of having 3 ways to learn each point: video, images, and text.

Frequency of how easily participants performed 5 key tasks during first time app use (n = 20).

Frequency of categories of usability statements (k = 654).
Potential side effects or adverse events were assessed during the exit interview. One participant with a craniotomy developed a headache about halfway through the study and discontinued acupressure; it was unclear if this was associated with acupressure but was reported to IRB. Although this participant stopped using acupressure, he did not drop-out of the study; he completed the exit interview and end of study questionnaire. Pressing on scars or a sensitive area such as an incisional site or a rash (reported by 1 participant) should be avoided; this warning was added to the app and consent, along with a Skip Point feature. No participants developed bruising. Many described “point tenderness,” which is expected. Several who complained of their fingers getting sore liked the option of using a pencil eraser to press. Several participants complained in the exit interview about annoyance or discomfort wearing the fitness tracker 24/7, especially at night.
The study was not designed or powered for testing efficacy on outcomes as the sample size was small and acupressure use was for only 1 week. When a designer recommended a change from pop-up surveys to a Dashboard reminder that a survey was due, several participants did not respond to the Dashboard, yielding missing self-report data. The team quickly resumed using the pop-up approach. There were 15 complete cases with PROMIS data with no statistically significant differences in these scores over the week. Of interest, the distribution of fatigue scores shifted from 70% who felt tired Often and Always at baseline to 40% who were tired often (0% always) at week’s end. For those with paired data (n = 15) the mean Fatigue Severity item (1 = very severe fatigue, 5 = none) at baseline 2.80 (SD = 0.77) improved to 3.13 (SD = 0.63); P = .07, Cohen’s d = .82.
Overall, the study established feasibility of the app functionality, extracted and analyzed all app data for the users, and confirmed linkages with Fitbit and Apple Health. One significant feasibility challenge was tracker integration. Fitbit data synched completely from the beginning, but there were numerous issues with the Apple Health programming, resulting in missing tracker data during the first 2 sprints. Once resolved, Sprint 3 participants successfully synched Apple Watch data with the app (see Figure 4 for an example graph of fitness tracker data from Sprint 3).
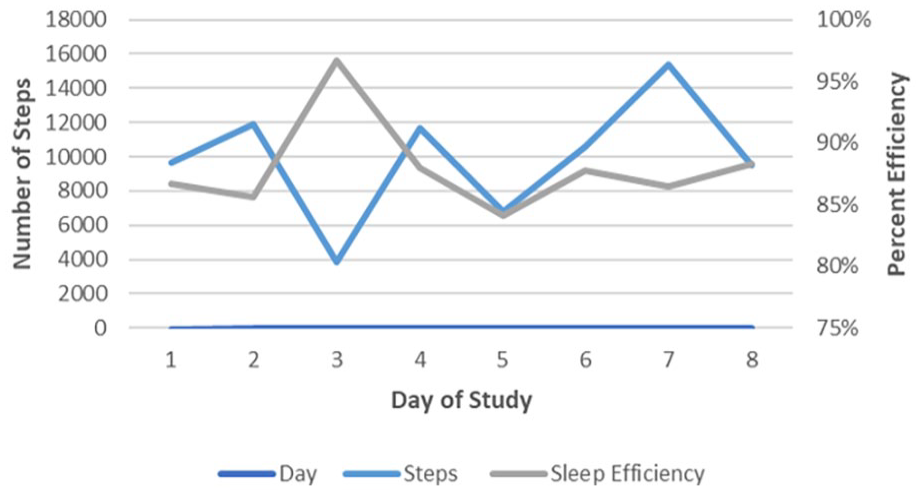
Example of fitness tracker data from 1 participant with complete data.
Discussion
Findings confirmed adults with cancer-related fatigue could accurately learn and consistently self-administer 2 acupressure rituals. Assessment of intervention fidelity was designed to assure that the intervention was performed as prescribed.40,41 Point accuracy improved over the 3 sprints with improvements to the learning platform and exceeded an 80% pass rate milestone in Sprint 3. Rating the accuracy from a video image differs from an in-person session where an instructor uses palpation with a participant one-on-one until a 95% level of accuracy is obtained. 42 Raters had a high level of agreement in judging point accuracy using the video approach. An 80% pass rate in accurately finding the points on the first attempt is judged as adequate. It may have been better to assess the point accuracy at the end of the study allowing for users to gain competency. Consistent with this idea, in the protocol for an RCT of the MeTime acupressure app (RA vs sham vs control), investigators will compare and assess point accuracy via video call at 6 weeks. 26
The app measured consistency of acupressure use for each ritual at the point level which was coded as complete or partial. Partial use, not always measured, may occur when it is necessary to skip a point due to sensitivity, a scar or rash, unable to reach, disruption, or point tenderness. This measurement method, integrated within the app, is an advantage over logs often used in self-acupressure studies.16,19,29 Participants completed SA more than RA which may be because SA was the first ritual to be performed each day. There was also a glitch (corrected) in that 3 times SPs were unable to access RA after midnight as the “day” in the app reset at 12 AM and only allowed the SA option. The mean complete point adherence for SA was similar to the 70% reported in a self-acupressure RCT but complete adherence to RA was less. 29 Two evidence-based rituals were included in the study to test the point accuracy by ritual and to explore feasibility of integrating both rituals into the app. There is no standard yet established for type or minimal doses of acupressure; in previous research, the actual points, number of points, and pressing time have varied.12,16,19,23 Two daily rituals at 3 minutes per point (ie, 2 daily 30-minute sessions) may be too burdensome to sustain. 42 In fact, participants were interested in an express version or opportunities to personalize the app use to their lifestyle and daily demands.
User experience is a “person’s perceptions and responses resulting from the use and or anticipated use of a product, system or service.” 43 A common starting place in studying user experience is assessing perceptions of usability. With 1 exception, users rated the app very positively and shared many positive comments about the experience. Although not a study aim, some findings support the acceptability or satisfaction with the app. It may seem incongruous that participants found the app easy to use but too time-consuming. It is really the time involved in the acupressure itself that is time-consuming. Given that there is not a known minimum effective dose, it could be advantageous to allow users to personalize the app to their lifestyle and symptom management needs by choosing the ritual and time of pressing each point.
The qualitative data from the think-aloud experience and exit interview were essential to the iterative agile approach.32,33 In addition, testing the app using users’ own phones (vs providing tablets 26 ) was extremely valuable. Usability statements led to modifications to address glitches and improve the app after each sprint. Application of the analytic approach to usability analysis used by Georgsson and Staggers 36 was extremely helpful in organizing and summarizing the qualitative data and is recommended as a useful method for analyzing voluminous qualitative data in recorded think-aloud sessions. Findings support usability and guided improvements including adding music and visuals, a video library, and FAQ. Features such as guidance to use aromatherapy with acupressure, 44 and a social engagement feature 45 in which users can communicate with each other also have been added to the app. A weekly live session via Zoom will be integrated into the app to assist users with point location if desired.
Systematic reviews of mHealth studies indicated a positive effect of mHealth applications on a variety of symptoms, including in cancer survivors.46 -49 By using an app such as EnergyPoints, users can treat and monitor symptoms and share progress with their health care provider regardless of location or access to a qualified instructor. In the future, Real-World-Data from the app will advance science, allowing assessment of varying doses, types, and durations on effectiveness of acupressure.50 -52 This first app, focused on acupoints targeting fatigue and sleep deficiency for cancer survivors, will serve as a prototype for future apps targeting other users (eg, children and caregivers), symptoms (eg, pain, constipation, anxiety, and depression), and other medical and psychiatric conditions.
Self-acupressure, performed by trained participants, is considered extremely safe; in this study there was no bruising as has been reported by others. 29 Numerous skin conditions experienced by cancer survivors reinforced the need to include a warning related to when to skip a point. The app Skip feature will record when the user intentionally skips.
Limitations: Enrollment was restricted geographically, which is acceptable for a usability and feasibility study. The sample was diverse in gender, race, and ethnicity. Most participants were college educated and 3 (15%) had a low income. The majority of participants had prior experience with health apps and complementary/integrative medicine; they therefore might have been predisposed to accept and use the app and acupressure. Outreach/education may be needed for millions of cancer survivors who lack those prior experiences. There is also a possibility of social desirability bias due to the location of the research at the offices of 5 Point App and the compensation for time and travel that was provided. Future research should include more participants with low literacy and those who are socially and economically disadvantaged. Their experience may indicate additional modifications to the app. The impact of other non-pharmacological strategies used by study participants is unknown. The app does capture these data which can be included in future studies of effectiveness.
Conclusions
Fatigue and sleep deficiency are some of the most prevalent and severe symptoms that cancer survivors must manage. The study supports the feasibility and usability of a new mHealth app, EnergyPoints, to guide survivors to self-administer acupressure, which is simple, non-invasive, safely practiced, and highly affordable. Although the evidence supports the efficacy of acupressure, this study did not focus on the effect of using the app on outcomes. Findings support the need to personalize the intervention for better adherence and scalability. A decentralized clinical trial is planned to examine effectiveness and sustainability of intervention fidelity of an upgraded EnergyPoints app that will allow the user to tailor their acupressure experience by choosing 1, 2, or 3 minutes to press each point; completing at least 1 ritual per day will be recommended.
Supplemental Material
sj-docx-1-ict-10.1177_15347354231223965 – Supplemental material for Feasibility and Usability of EnergyPoints: A Mobile Health App to Guide Acupressure Use for Cancer Symptom Management
Supplemental material, sj-docx-1-ict-10.1177_15347354231223965 for Feasibility and Usability of EnergyPoints: A Mobile Health App to Guide Acupressure Use for Cancer Symptom Management by Susan L. Beck, Ryan Smith, Janet Mindes, Karl Beck, JungYoon Leah Kim, Matthew Weitzman, Jennifer A. M. Stone, Susan Veleber and William N. Dudley in Integrative Cancer Therapies
Supplemental Material
sj-docx-2-ict-10.1177_15347354231223965 – Supplemental material for Feasibility and Usability of EnergyPoints: A Mobile Health App to Guide Acupressure Use for Cancer Symptom Management
Supplemental material, sj-docx-2-ict-10.1177_15347354231223965 for Feasibility and Usability of EnergyPoints: A Mobile Health App to Guide Acupressure Use for Cancer Symptom Management by Susan L. Beck, Ryan Smith, Janet Mindes, Karl Beck, JungYoon Leah Kim, Matthew Weitzman, Jennifer A. M. Stone, Susan Veleber and William N. Dudley in Integrative Cancer Therapies
Footnotes
Acknowledgements
The authors would like to thank the cancer survivors who participated in the study and guided improvements to the EnergyPoints app. The authors would like to thank Melanie A. Gold, DO, DABMA, DMQ for her review and edits to the manuscript.
Correction Notice (September 2025):
The academic degree of one of the authors, Jennifer A.M. Stone has been corrected in the article.
Authors Contributions
SLB: Writing-original draft, Conceptualization, Methodology, Funding acquisition, Supervision, Data curation, Qualitative analysis (lead), Quantitative analysis (collaborator), Visualization. RS: Writing-review and editing, Conceptualization, Methodology, Educational content (Lead), Funding Acquisition, Project administration, Resources, Qualitative analysis (collaborator). JM Writing-review and editing, Conceptualization, Methodology, Funding Acquisition, Project administration, Interviewer, Qualitative analysis (collaborator). KB: Writing-review and editing, Project administration, Data collection, Qualitative analysis (collaborator). JLK: Writing-review and editing, Project administration, Data collection. MW, JAS, and SV: Writing-review and editing, Expert adviser on educational content, Rating of point accuracy. WND: Writing-review and editing, Quantitative analysis (Lead), Resources, Visualization.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Authors have no conflicts to declare. When it is commercialized, EnergyPoints will be a for-profit product of 5 Point App Inc. All funding for the research was supported by a grant from the National Cancer Institute.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this presentation was supported by the National Cancer Institute of the U.S. National Institutes of Health under Award Number R43CA261446 (Beck, SL, PI). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Supplemental Material
Supplemental material for this article is available online.
Data Sharing
NIH does not require data sharing for Phase I SBIR grants. Sample data collection tools may be obtained from the first author at susie@5pointapp.com.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.