
Abstract
Purpose:
The study aimed to (1) examine the feasibility of providing a training course on auricular point acupressure (APA) for clinical oncology nurses to integrate APA into real-world nursing care settings, and (2) examine the effectiveness of APA on cancer-related pain (CRP) under usual inpatient oncology ward conditions.
Methods:
This was a 2-phase feasibility study. Phase 1, an in-person, 8 hour training program was provided to oncology nurses. Phase 2, a prospective and feasibility study was conducted to evaluate the integration of APA into nursing care activities to manage CRP. Oncology patients were included if their pain was rated at ≥4 on a 0 to 10 numeric rating scale in the past 24 hours. Patients received 1 APA treatment administered by the nurses and were instructed to stimulate the points for 3 days. Study outcomes (pain intensity, fatigue, and sleep disturbance), pain medication use, and APA practice were measured by a phone survey daily.
Results:
Ten oncology nurses received APA training in phase 1. APA had been added to the hospital’s electronic health records (EHRs) as a pain treatment. In phase 2, 33 oncology patients received APA treatment with a 100% adherence rate (pressing the seeds 3 times per day, 3 minutes per time based on the suggestion). The side effects of APA were minimal (~8%-12% felt tenderness on the ear). After 3 days of APA, patients reported 38% pain relief, 39% less fatigue, and 45% improvement in sleep disturbance; 24% reduced any type of pain medication use and 19% reduced opioid use (10 mg opioids using milligram morphine equivalent). The major barrier to integrating APA into routine nursing practice was time management (how to include APA in a daily workflow).
Conclusion:
It is feasible to provide 8-hour training to oncology nurses for mastering APA skill and then integrating APA into their daily nursing care for patients with CRP. Based on the promising findings (decreased pain, improved fatigue and sleep disturbance, and less opioid use), the next step is to conduct a randomized clinical trial with a larger sample to confirm the efficacy of APA for oncology nurses to treat CRP in real-world practice.
ClinicalTrial.gov identifier number: NCT04040140.
Introduction
Cancer-related pain (CRP) remains one of the most distressing symptoms for cancer patients and survivors, leading to significant functional disability and a negative impact on quality of life.1,2 Pain affects an estimated 55% of persons during anticancer treatment, up to 66% of individuals with advanced cancer,2,3 and persists in half of cancer survivors after the completion of treatment. 4 Pain has long been recognized as one of the most common reasons for emergency care 5 and cancer patient hospitalizations, and currently accounts for up to 28% of unplanned and potentially preventable hospitalizations. 6 Both pain specialists and cancer communities recognize a significant need for pain control that is effective and well tolerated and for multimodal therapies to reduce not only suffering from pain but also subsequent hospital admissions for pain control.
Clinical guidelines advocate nonpharmacologic therapies and self-management (SM) of chronic pain,7 -9 but nonpharmacologic and SM options for CRP are challenging for providers and patients alike. Acupuncture is included in the current guidelines for chronic pain10,11 and, as of 2020, is covered by Medicare. 12 Auricular acupuncture (also called battlefield acupuncture)13,14 using the ear acupoints is easier to learn and administer than body acupuncture. 15 The Department of Defense and Veterans Affairs (VA) developed a curriculum of auricular acupuncture to train over 2700 VA providers with pain management responsibilities since 2016. 16 Despite these advances, widespread implementation is hindered by frequent office visits, high costs, patients’ misconceptions, and a lack of access to licensed acupuncturists.17,18
Auricular point acupressure (APA) is the application of acupuncture-like stimulation to specific points on the ear (acupoints). In APA, small pellets (2 mm in diameter) are taped on specific ear points, and patients press on the pellets to stimulate the ear points 3 times daily, 3 minutes per time, for a total of 9 minutes per day (Figure 1).19,20 APA is a noninvasive (needleless) and active treatment for patients with pain, whereas acupuncture is invasive (using needles) and a passive treatment (administered by a licensed practitioner).21,22

Placement of APA seeds.
Accumulated extensive evidence has demonstrated the effects of APA on pain.23 -26 Evidence of APA as pain relief points to several potential biological mechanisms: (1) direct (ie, stimulation of trigeminal and vagus nerve innervation distributed on the ear) or indirect effects (eg, ear point stimulation as a conscious behavior) 27 , (2) modulation of inflammatory cytokine levels (decreased proinflammatory cytokines [IL-1β, IL-6, TNF-α]) or stimulation to release anti-inflammatory cytokines (IL-13 and IL-4) in the peripheral serum19,28 -30, and (3) modulation of nerve sensitivity, transmitting APA stimuli into neuronal signals to modulate pain in the central nervous system. 29
Nurses are the patient’s first line of support in managing inpatient CRP; however, nurses have limited tools to deliver this support. To address this dilemma, patients and nurses need access to a therapy that can quickly relieve pain, which, in turn, reduces analgesic use and encourages patients to engage in other pain interventions. APA is one possible solution for unmet challenges in CRP management.
Although patients with pain are interested in complementary and integrative management approaches,31,32 clinicians’ lack of knowledge sometimes limits their use. Thus, due to the noninvasive characteristics of APA, we assessed the feasibility of providing an APA training workshop for clinical oncology nurses to integrate APA into real-world nursing care settings. We hypothesized that nurses could learn APA and incorporate it into their practice to provide pain relief. The aims of this study were to (1) examine the feasibility of providing an APA training course for clinical oncology nurses to integrate APA into real-world nursing care settings and (2) examine the effectiveness of APA on CRP under usual inpatient oncology ward conditions.
Research Design and Methods
A 2-phase feasibility study was used to examine the effectiveness of an APA training course for nurses that can be integrated into real-world clinical settings to manage CRP. All human subject procedures were approved by the Johns Hopkins Medicine Institutional Review Board (IRB00183805: approved date: 10/08/2019).
Phase 1—Training
In collaboration with a Comprehensive Cancer Center in Maryland, USA, an APA training course was provided to 10 nurses who worked with oncology patients. After a written inform consent was signed, nurses completed the APA training, which included 5 hours of didactic presentations and 3 hours of personal hands-on training, to ensure a deeper understanding of APA and how to integrate it into nursing practice. At the conclusion of training, nurses received a completion certificate upon passing the examination and 7.2 continuing education credit hours.
Participants
Oncology nurses practicing at a Comprehensive Cancer Center in Maryland, USA signed a written informed consent, and received approval from their supervisors to attend the training workshop. Ten oncology nurses (8 females and 2 males) completed the APA training.
Workshop (APA Training)
The course included 5 hours of didactic presentations and 3 hours of personal hands-on training, to ensure a deep understanding of APA. The didactic training comprised content derived from textbooks, articles, and websites, presented in 5 lectures: (1) overview and theoretical perspective of auricular therapy, (2) anatomical terminology for the external ear, (3) auricular master points, musculoskeletal and sensory ear points, (4) auricular diagnosis and treatment procedures, and (5) commonly used APA protocols for CRP. For the hands-on training, learning was reinforced through immersive learning, demonstration, and return-demonstration. Nurses practiced identifying the appropriate ear points by placing a pin on silicone ear models. Then they practiced using a probe to identify the ear points on selected area of CRP and placing APA seeds on a nurse volunteer while being observed and mentored by the APA educator (Yeh). To successfully complete the practicum course, the nurses had to demonstrate APA competency via a skills checklist, including the use of the probe to find the points corresponding to body pain, seed placement, and stimulation of the ear points.
Measures
Knowledge of APA treatment
An assessment to examine the nurses’ knowledge of APA was developed by the team, based on the APA workshop content (the test is available upon request). The knowledge test consisted of 43 multiple choice questions and 7 open-ended questions (the score ranged from 0 to 100, with 100 indicating a perfect score). Questions covered the theoretical perspective of auricular therapy, anatomical terminology for the external ear related to the body, auricular diagnosis procedures to locate the ear points, master points of the treatment effects, musculoskeletal and sensory ear points, and how to stimulate the ear points.
Confidence scale to practice APA
Nurses’ confidence in practicing APA was assessed before and after the training via a self-report measure comprising 1 item adapted from the Confidence Scale 33 : Overall how confident are you that you are able to practice APA successfully? The item was measured via a 10-point Likert scale ranging from 0 (not at all confident) to 10 (extremely confident).
Practice treatment log
After completing the training workshop, each nurse was required to submit a treatment log for 5 friends or peers in order to receive APA practitioner certification. The log included the body map to mark the pain location, auricular photos marking the points for treatment, pain details (descriptions from the participants), and the pain intensity (0-10 scale) before APA, immediately after APA, and 24 and 48 hours post-APA treatment.
Results
Feasibility of APA training and training outcomes
We found that delivering an 8 hour training to nurses for APA mastery was feasible. The mean score on the post-course APA knowledge test was 93% (standard deviation [SD] = 6.87). The mean score on the measure of confidence in APA practice increased from 0 before the workshop to 6.5 (SD = 0.84, range 5-10) after the workshop.
Table 1 presents the pain outcomes in the practice treatment log after nurses received APA training and practiced APA treatment on 5 friends or peers. A total of 44 people received APA treatment during the practice. These individuals reported an average 49% decrease in pain intensity immediately after APA, an average 60% decrease 1-day post-APA, and an average 66% decrease 2 days post-APA.
Summary Statistics of Pain Intensity from Practice Logs for Practice After APA Training.

Abbreviation: SD, standard deviation.
=100 × (post APA visit-pre APA)/pre APA.
After the training, APA was added as a non-pharmacological intervention in the hospital electronic health records (EHRs), so that the nurses could document the implementation of APA for CRP management.
Phase 2—Implementation
After receiving APA certification, nurses implemented APA for CRP as part of their nursing care activities. This involved teaching the consented patients about APA and their role in stimulating the seeds by evenly pressing on each seed without rubbing for 3 minutes, 3 times daily (9 minutes total). All patients provided written informed consent before receiving the APA for CRP. The study outcomes were assessed at 4 time points: pre-intervention and daily for up to 3 days either in person for those who were still hospitalized or via phone call for those who had been discharged. The assessments were scheduled according to the patients’ preference. Pain medication was not withheld from the patients, as APA treatment was an addition to prescribed medications.
Participants (Patients)
Patients were eligible to participate if they were (1) cancer patients whose worst pain was rated as ≥4 on a 0 to 10 numeric rating scale in the past 24 hours, which was assessed using the Brief Pain Inventory—Short Form (BPI-sf), 34 (2) able to read and write English, and (3) able to apply pressure to the seeds taped to the ears. Patients were excluded if they (1) were delirious, (2) had ear skin disease, or (3) were allergic to the latex tape used in the study.
Recruitment
The team screened the EHR on the dedicated oncology units to identify patients with a pain intensity ≥4 (0-10 scale). They then obtained consent from the patients, and the nurse was directed to provide the APA treatment. Patients were eligible if they were inpatients and agreed to undergo APA treatment for their CRP. Patients were excluded if they (1) were delirious, (2) had ear skin disease, or (3) were allergic to the tape used for this study. Initially, each APA-trained nurse was expected to treat 20 patients (200 total patients) from within their assigned patients within 6 months. However, mandatory COVID-19 restrictions ended the study before this could be done. Only 33 participants were included in this report.
Measurement
Symptom severity assessment and APA practice
A daily survey link was sent to the patient via text message to collect (1) symptom severity (pain, fatigue, and sleep disturbance) on a scale ranging from 0 (not present) to 10 (as bad as you can imagine), (2) APA practice information (including frequency and duration of pressing the seeds taped to their ears and any side effects), and (3) pain medication use.
Qualitative interviews
Qualitative methods (individual in-depth interviews) were used to elicit nurses’ perspectives of the integration of APA into clinical practice and to identify barriers/facilitators to implementation. After APA had been implemented for 6 weeks, each nurse was contacted for an interview to assess the integration of APA into clinical practice to manage CRP and the nurses’ satisfaction with APA. Participants were interviewed based on their availability in a private setting of their choice. A trained interviewer conducted the semi-structured interviews, which began broadly with general questions, such as “Can you tell me how you feel when you implement APA to treat your patient’s pain?” Then, the interviewer gradually moved to aspects more directly related to nurses’ concerns, such as the challenges to providing APA for patients. The in-depth interviews ranged from 30 to 40 minutes. The interviews were audio recorded and transcribed for analysis.
Statistical Methods
Descriptive statistics were used to present demographic characteristics and study measures. For the nursing APA education outcomes, a paired t-test was used to examine the differences in confidence to practice APA to manage CRP from pre-training to post-training. For the severity of each symptom (pain intensity, fatigue, and sleep disturbance), the mean changes from pre-APA were analyzed using a linear mixed model that included categorical time points (day 1, day 2, day 3 post-APA) as fixed effects and random subject intercept. Due to the nature of self-report questionnaires and participant non-response, missing data were encountered in several variables of interest. Out of the initial sample of 33 participants, 8 participants did not complete the questionnaire in its entirety. Missing data were observed in the outcome measures, representing approximately 19.7% of the total dataset. The analysis was based on observed data (not imputed). The demographic characteristics were summarized for all enrolled patients, while the outcome measures were summarized for patients who received the treatment.
The restricted maximum likelihood method was used to estimate the variance, and an unstructured (co)variance was specified. The Kenward-Roger approximation was used to estimate denominator degrees of freedom. Significance tests were based on the generalized least squares means for the hypothesis of no change from pre-intervention at each time point with a significance level of α = .05. To determine which treatment variables might be associated with the primary outcomes, the mixed model for repeated measures was analyzed by including the continuous, fixed effects of the time each seed was pressed, press minutes, and press total, in addition to the categorical, fixed effects of time points. Milligram morphine equivalents (MME) were determined using established equivalency factors of all opioids taken by a participant daily. 35 For this pilot study, summary statistics (means, SDs, or medians) were emphasized over hypotheses testing.
Qualitative Data Analysis
Data analysis was guided by the techniques suggested by Miles and Huberman. 36 Qualitative content analysis was implemented to code responses (ie, line-by-line coding, constant comparative methods to analyze differences and similarities in responses, and construction of categories and themes). 36 A content analysis summary table was used to summarize similarities and differences in findings. The qualitative interviews were coded line by line, and data was separated based on differences and similarities into categories, which were separated into themes, analyzed, and coded. 36
Results
Participant characteristics
In total, 33 patients were recruited into the study and received APA treatments. Table 2 presents the demographic characteristics. The average age of the participants was 50.2 years (SD = 15.64, range 20-74). Among the 33 participants, the majority were White (n = 18, 55%) and men (n = 19, 58%). Cancer diagnoses included breast cancer (n = 9), colon cancer (n = 2), leukemia (n = 1), and other solid tumors (n = 21).
Demographic and Clinical Characteristics (N = 33).
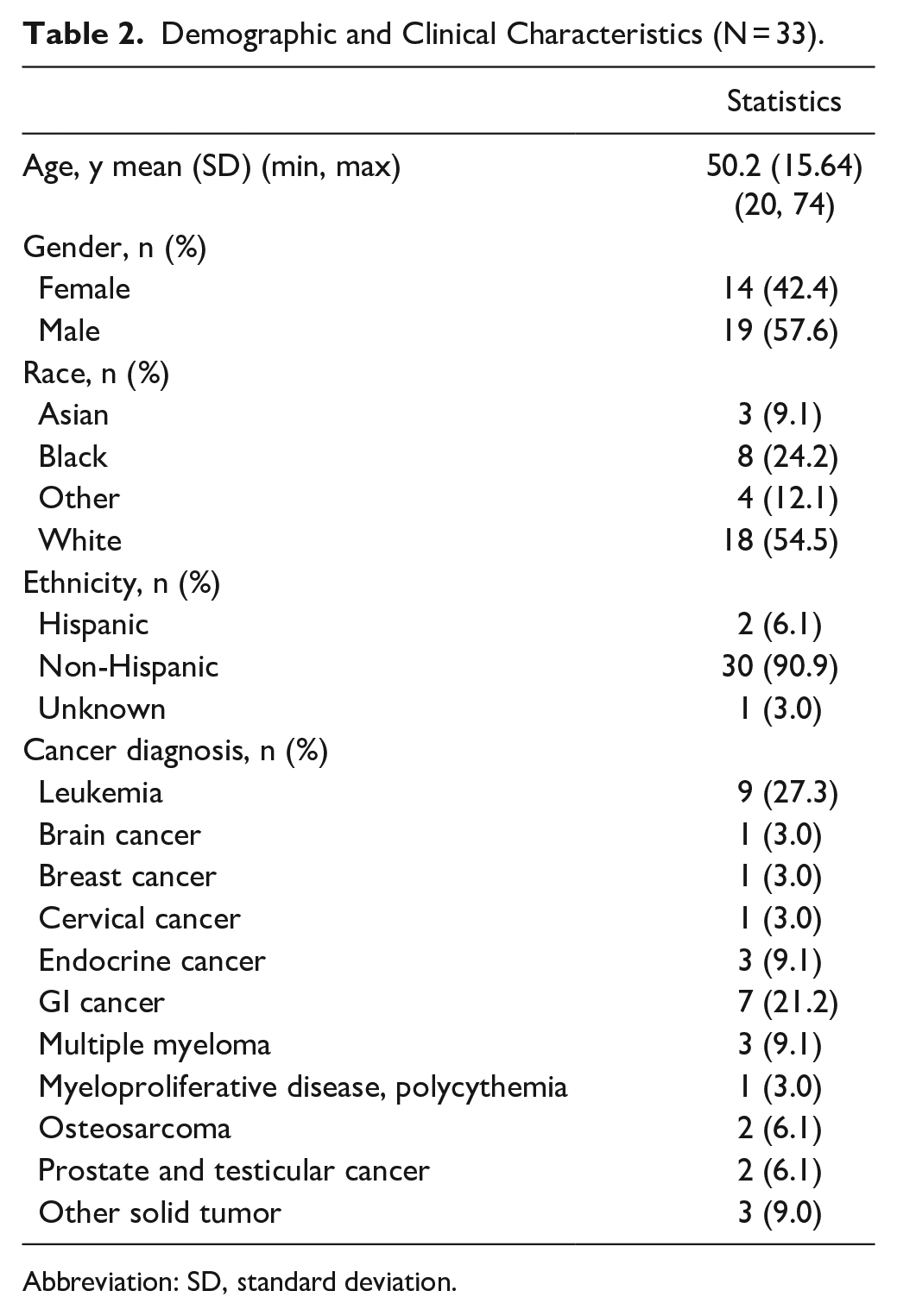
Abbreviation: SD, standard deviation.
Symptom severity
Table 3 shows summary statistics (mean and SD) for the study outcomes (pain, fatigue, and sleep disturbance) at pre-APA and daily post-APA for 3 days. For pain intensity, compared to pre-APA, the participants reported a 28% improvement at day 1 post-APA; they continued to improve and reached a 38% improvement at day 3 post-APA. For fatigue severity, participants reported 33% improvement at day 1 post-APA and reached 39% improvement at day 3 post-APA. For sleep disturbance, participants reported 44% improvement at day 1 post-APA and had 45% improvement at day 3 post-APA. All the improvements in pain intensity (P < .05), fatigue (P < .05), and sleep disturbance (P < .05) were statistically significant, compared to pre-APA. Figure 2 shows the mean and 95% confidence interval of symptom changes on day 1, day 2 and day 3 post-APA among hospitalized oncology patients.
Summary Statistics for Study Outcomes.
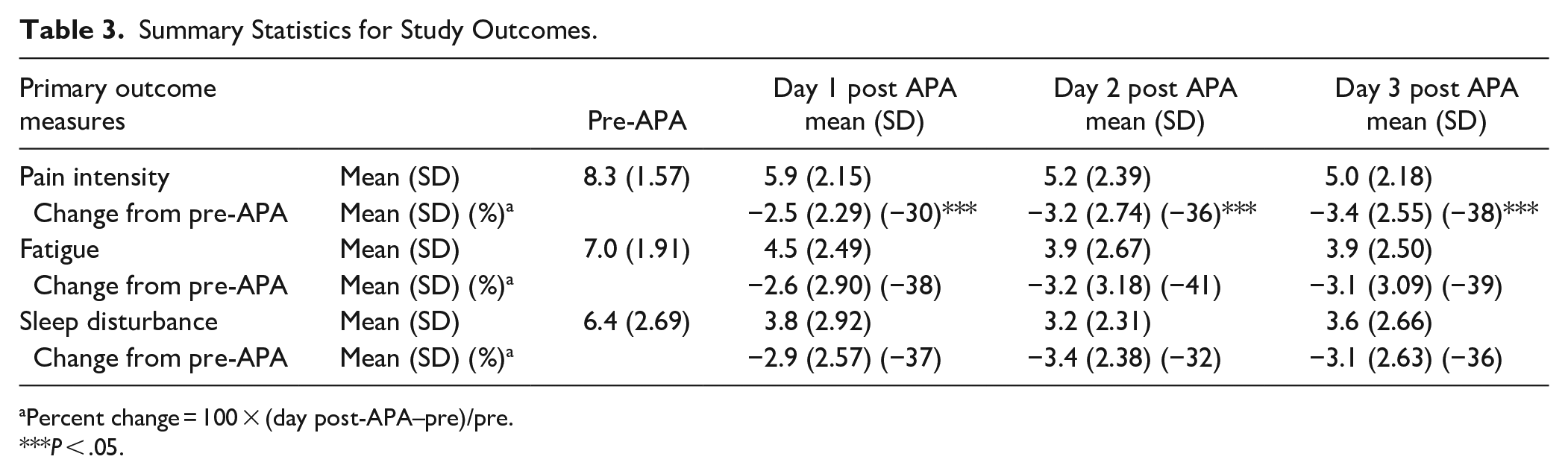
Percent change = 100 × (day post-APA–pre)/pre.
P < .05.

Mean and 95% confidence interval of pain, fatigue and sleep disturbance changes in hospitalized oncology patients.
Pain medication use
Table 4 presents the use of pain medication (including the names of opioids). At pre-APA, 79% (n = 26) patients reported the use of pain medications, which reached a 24% decrease by day 3 post-intervention (55%, n = 18). Twenty-two patients (n = 67%) reported using at least one type of opioid at pre-APA, which reached a 19% decrease (48%, n = 16). MME dosages decreased from 110 mg at pre-APA to 101 mg after 3 days of APA.
Pain Medication Use.

The denominator used to estimate % change of “any type of opioid” was the total number of subjects (N = 33). Dosage was converted using the MME conversion factor with the subjects had available dosage for all 4 days.
Abbreviations: SD, standard deviation; IQR, interquartile range.
n is less than the total N (33) due to missing data.
APA practice
Table 5 presents daily APA practice by the participants. The results indicate that participants pressed the seeds approximately 4 times per day (3 times suggested), >3 minutes per time (3 minutes suggested), and 10 minutes per day (9 minutes suggested). Participants exhibited an 100% adherence rate throughout 3 days post-APA. The side effects of APA were minimal (~8-12% felt some tenderness of the ear).
APA Practice and Adverse Effect.

Abbreviation: SD, standard deviation.
Association between APA practice and symptom severity
Table 6 presents the results of the frequency of seed pressing per day (eg, number of times), the duration of each pressing time (minutes), and the duration of total pressing per day (minutes) on the primary outcomes, respectively (pain, fatigue, and sleep disturbance). The frequency of seed pressing was significantly associated with the changes in the score from pre-APA in pain (P = .04) and fatigue (P = .002), but was not significantly associated with the changes in the score in sleep disturbance (P = .12); the duration of total pressing per day (minutes) on the ear was significantly associated with changes in the scores from pre-APA in fatigue (P = .007) and sleep disturbance (P = .007), but was not significantly associated with changes in the score for pain (P = .31). The duration of each pressing time was not significantly associated with any of the 3 primary outcomes (P > .05).
Relationship Between Treatment Variables and the Primary Outcomes.

Abbreviation: ref, baseline.
Qualitative finding (major themes)
Our interview data revealed 3 themes: time management, patient interest, and confidence.
Theme 1: Time management
This theme captured the nuances of time management for the nurses. They identified the time needed to administer the treatment as the biggest barrier. They felt more time was available on the night shift, but at that time, the patients were sleeping. A few nurses noted that patients needed time to think about agreeing to the intervention and they had a “hard time selling it to the patient.”
Theme 2: Patient interest
The nurses found that patient interest varied, as some patients were skeptical, but most were intrigued by a different treatment option. They also noted that some patients were just overwhelmed with treatment altogether and that considering APA was difficult. One nurse said, “Some people are more open and others are like ‘I want to think about it.’”
Theme 3: Confidence
All of the nurses reported that their confidence in providing APA increased after the training but greatly increased after practice. Some nurses noticed improvement in finding the tender points on the ears and their confidence increased when patients were happy with the treatments. The nurses who attended this training were enthusiastic about learning a new technique that they could provide independently to help control patients’ pain.
Discussion
To our knowledge, this is the first study to provide APA training to oncology nurses to be implemented in clinical practice to manage inpatients’ CRP. Our study findings indicate that it is feasible to provide an 8-hour workshop for the oncology nurses to learn APA and implement it in clinical nursing practice to manage CRP. The findings from the cancer patients who received APA treatment from the trained nurses are promising. APA in this pilot trial provided quick, sustained, inexpensive, and easily achieved relief, reflected in improvements in not only pain intensity, but also in fatigue and sleep disturbance. Unrelieved pain is a common occurrence in cancer patients and reduces quality of life and even lifespan,37,38 and new methods need to be considered to treat it.
As a pilot trial designed to gather data to estimate an effect size for a randomized clinical trial, we found patients had achieved almost 40% pain relief, and improvement in fatigue and sleep disturbance within 3 days. Importantly, 24% of patients were able to decrease their pain medications and 19% were able to decrease opioids (less than 10 mg of MME dosages). Further research is clearly warranted to determine whether APA can be integrated into routine oncology inpatient practice.
We found that an 8 hour in-person workshop was sufficient to provide the required APA knowledge and skills. However, scheduling the workshop for 10 nurses was challenging due to their busy clinical responsibilities. To overcome the scheduling conflicts, a hybrid course including online asynchronous didactic presentations and hands-on training could be used to facilitate a deeper understanding of APA. The course could use modules with content presented through article and textbook readings, websites, and video streaming. Learning should be reinforced during in-person hands-on training through didactic approaches, immersive learning, demonstration, and discussions. The training should include required competency for delivering APA treatment, competency testing after the training, and maintaining competency.
To date, few interventions have addressed emerging CRP, fatigue, or insomnia during chemotherapy.39,40 Hospitalized cancer patients in this study were able to adhere to the suggested APA practice. The side effects of the APA were minimal, that is, about 10% of the patients felt tenderness on the ear. The tenderness of the ear points are correlated to the severity of the body symptoms; for example, the greater pain intensity in the body, the more tenderness of the corresponding ear points. 21 Thus, it is important to inform patients of this correlation in the future. Given that healthcare providers have limited tools to help patients manage CRP,41,42 APA has the potential to overcome barriers in pain management at multiple levels by empowering nurses to provide an additional safe, effective and rapid pain relieve intervention, while patients gain some control and ability to manage pain on their own.
Our qualitative findings suggested that the technique used in the APA workshop was successful as a beginning to build APA knowledge and skills. However, 1 barrier identified by nurses was finding time to actually provide the treatment during their shift. As we approach new and innovative ways to help our patients, we need to consider how interventions like APA can be incorporated into nurses’ daily workflow. Being able to document the application of APA in the EHRs will enable tracking ability and providing APA to clinicians as one of alternative options for symptoms relief.
The study was limited by the sample size, which was smaller than the intended sample size due to COVID-19 in-person contact restrictions. Due to the nature of our study, participants were not blinded so potential bias can be a concern and the time for each nurse to administer the APA for a patient was not observed.
We conclude that APA is an ideal tool for training healthcare professionals to provide treatments for patients with pain. APA is a scalable treatment that would benefit from further evidence from a pragmatic controlled trial to evaluate the effectiveness of APA embedded in routine care. We believe that replicating this study in a randomized clinical trial with a larger sample is the next step to confirm the efficacy of APA for treating CRP in real-world practice for oncology nurses.
Footnotes
Acknowledgements
Research reported in this publication was supported by the Brager Humanitarian Award at the Johns Hopkins Kimmel Cancer Center and an Under Armour Women’s Health & Breast Cancer Innovation Grant, Johns Hopkins Medicine. Funding sources were not involved in the preparation, writing, or submission of this paper. It is with heavy hearts and profound sadness that we acknowledge the untimely passing of our esteemed coauthor, Professor Dr. Chao Hsing Yeh. Tragically, Dr. Yeh passed away during the final stages of manuscript submission, leaving an immeasurable void in our hearts and in the scientific community. Throughout the course of this project, Dr.Yeh demonstrated an exceptional commitment to excellence, pushing the boundaries of our understanding and challenging us to achieve new heights. Her insightful perspectives, innovative ideas, and meticulous attention to detail significantly enhanced the quality of this work. The authors would like to thank the following nurses for their work on this project: Kristen Hains, Steve Rutkowski, Hanna Bare, Melanie Cohen, Zoe Gearing, Kyong Golden, James Gonzales, Christina Lai, Brynn Puller, Wendy Wen.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the Brager Humanitarian Award at the Johns Hopkins Kimmel Cancer Center and an Under Armour Women’s Health & Breast Cancer Innovation Grant, Johns Hopkins Medicine. Funding sources were not involved in the preparation, writing, or submission of this paper.
Statement of Data Availability
The authors affirm that all relevant data supporting the findings of this study are available within the manuscript. Additionally, upon reasonable request, and subject to any necessary permissions and compliance with applicable regulations, the authors will provide access to the raw data used during the research process. This is to ensure transparency and facilitate further scientific inquiry and validation. Interested researchers may contact the corresponding author to inquire about data availability and access.