
Abstract
Background:
Quality of life is a multidimensional concept that involves physical, social, emotional, and functional well-being. Spirituality represents a potentially influential factor in the quality of life. This study aimed to evaluate the quality of life and spirituality among cancer patients.
Methods:
A cross-sectional study was carried out on 354 cancer patients in Palestine. A self-administered questionnaire was used for data collection. The questionnaire was made up of 4 sections: sociodemographic factors, clinical data, FACT-G, and FACIT-sp.
Results:
A total of 354 cancer patients with a mean age of 46.4 ± 15.3 years were enrolled in the study. The spiritual well-being of patients reported in this study was measured by using the median FACIT-Sp total score, and it was 35 (IQR: 29-42). The quality of life of patients was measured using the median of the FACT-G total score, and it was 63 (IQR: 52-85). The FACT-G score was significantly variable based on several factors including age, marital status, cancer type, presence of metastasis, presence of treatment side effects, and the period since diagnosis (P-value < .05). The FACIT-Sp total score had a significantly strong positive relationship with FACT-G total score (r = .705, P < .001). Moreover, moderate to strong significant correlations were found between spirituality and quality of life subscales.
Conclusions:
Quality of life among cancer patients is affected by their basic and clinical characteristics and is highly correlated with their spirituality level. Thus, addressing palliative support through spiritual care besides primary clinical treatment is of great importance to improve the quality of life among cancer patients.
Introduction
Quality of life (QOL) is a multidimensional concept that encompasses physical, social, emotional, and functional well-being. It reflects the individual’s perception of their position in life, relying on both subjective and objective measures.1,2 While objective measures are crucial for evaluating health, subjective ones provide a more accurate assessment of the quality of life. 3 Despite recent advances in treatment strategies, it is widely observed that diseases, particularly chronic ones, significantly impair patients’ quality of life.4 -6 Consequently, more comprehensive domains are now being considered during patient treatment to enhance their quality of life. 2 An extensive evaluation of clinical outcomes, physiological body functions, and patient subjective satisfaction should be particularly emphasized, especially among those with chronic diseases. Several disease-specific measures have been validated to assess patients’ evaluation of their health-related quality of life.3,7,8
It is not uncommon to place greater emphasis on the quality of life of patients rather than on healthy individuals, as disease symptoms and treatment side effects negatively affect physical, social, emotional, and functional well-being.9,10 Cancer represents one of the leading causes of death worldwide and a challenging disease to treat. 11 Cancer patients often experience psychological distress, and misconceptions about cancer can negatively influence their adherence to treatment and treatment efficacy.12,13 Moreover, the aggressive nature of the disease and its treatment can lead to cognitive impairment, depression, and physical disabilities.14 -16
Spirituality is the belief that provides meaning, purpose, and direction in life. 17 It extends beyond the concept of religiosity; however, religious practices are considered organized practices of spirituality. The greater spirituality one has, the greater his inner peace and well-being and thus greater life satisfaction. 18 In Palestine and other Islamic countries, several spiritual practices are routinely practiced as part of religious beliefs, such as prayers and attending religious talks at mosques or churches. Additionally, people often seek support from religious figures whenever they are dissatisfied with their lives to reinforce their connection with God and to find satisfaction with their fate and destiny. In general, religious individuals tend to engage in extensive religious rituals and avoid certain actions to cope with their significant life events. 19 It has been illustrated that spirituality is not limited to the causal effect of religiosity and some people consolidate their ultimate beliefs about the meaning of life, purpose of life, and experience connections with self, family, and nature.20,21
Numerous studies have shown that spirituality is associated with the quality of life.22 -24 Although the impact of clinical care on a patient’s health and, consequently, their quality of life cannot be disregarded in any disease, it is crucial to consider the patient’s spirituality. The influence of spiritual beliefs and practices on physical and mental health has been suggested, prompting increased interest in developing spirituality-based medical interventions.25,26 However, the relationship between cancer patients’ spirituality and their quality of life has not been extensively studied in Palestine as a means to enhance their quality of life.
The purpose of this study is to assess the relationship between spirituality and quality of life among cancer patients. In addition, the study sought to ascertain how the patient’s clinical information and personal traits affected their quality of life.
Methods
Ethical Consideration
This study was officially approved by the Institutional Review Board at An-Najah National University located in Nablus/Palestine. The study abided by “the Declaration of Helsinki (DOH).” The human subject confidentiality and rights were preserved throughout the study and informed consent was obtained from all patients. The patients were fully informed that participation in the study was voluntary and anonymous and that no penalty would be enforced in case of non-participation.
Study Design and Sample
A cross-sectional study was carried out from November 2021 to April 2022 on 354 cancer patients attending 2 hospitals in Palestine; Al-Watani Hospital and An-Najah National University Hospital. The sample size was calculated by using the Raosoft sample size calculator by applying a margin of error of 5% and a confidence interval (CI) of 95%. The minimum recommended sample size for the study is 341 participants. Patients were accessed during their treatment sessions and voluntarily participated and completed the study questionnaire.
Inclusion and Exclusion Criteria
The inclusion criteria included cancer patients attending the oncology department at Al-Watani Hospital and An-Najah National University Hospital during the study period, and that they accepted to participate in the study. The patients were over 18 years old, aware of their illness, without any mental disorder or dementia, and they could complete the self-administered questionnaire without the aid of any family member or healthcare worker to obtain reliable and unbiased data. The exclusion criteria included cancer patients who refused to participate; those who were under 18 years old, those with mental problems, or unable to fill out the questionnaire independently.
Study Instrument
A self-administered questionnaire was used for data collection. The questionnaire was made up of 4 sections: the first section was sociodemographic factors including age group, gender, marital status, and level of education. The second section was about clinical data including cancer location, the presence of metastasis, the presence of treatment side effects, and the period since cancer diagnosis. The third section measured the level of spirituality using the Functional Assessment of Chronic Illness Therapy-Spiritual Well-Being (FACIT-Sp) questionnaire. The last section measured the patient’s quality of life using the Functional Assessment of Cancer Therapy-General (FACT-G). The questionnaire was in Arabic and the translation was used after being licensed by the source of the tools ( https://www.FACIT.org).
The FACIT-Sp is a 12-item questionnaire designed to provide an inclusive measure of spirituality that can be employed in research with people with chronic and/or life-threatening illnesses. Responses are rated on a five-point Likert scale (0 = Not at all, 1 = little bit, 2 = Some-what, 3 = Quite a bit, 4 = Very Much). Three subscale scores can be obtained: meaning, peace, and faith. Higher scores indicate greater existential or faith well-being. This measure has been widely used in research on chronic diseases and spirituality and has established validity and reliability (Cronbach’s alpha is 0.79 for the total scale and ranges from 0.73 to 0.85 for the subscales). 27 The Cronbach’s alpha of .85 was calculated on the studied sample and indicated acceptable internal consistency within the spirituality scale.
The FACT-G is a 27-item scale of general questions divided into 4 domains: physical well-being (PWB), social well-being (SWB), emotional well-being (EWB), and functional well-being (FWB). Each item is rated on a five-point format ranging from 0 (not at all) to 4 (very much). Higher scores indicate better QOL. The reported internal consistency was excellent to good for all the FACT-G domains (Cronbach’s alpha of the total scale is .89 and the subscales range from .69 to .82). 28 The Cronbach’s alpha of .93 was calculated on the studied sample and indicated acceptable internal consistency within the quality of life scale.
Statistical Analysis
All statistical analyses were conducted using Statistical Package for the Social Sciences version 22 (SPSS 22) (IBM Corp., Armonk, N.Y., USA). Descriptive analyses were used for sociodemographic and clinical characteristics. The mean, median, and interquartile ranges were used to describe spirituality and quality of life scores. The mean rank values were used to determine the relationship between sociodemographic variables and the quality of life. Bivariate Pearson correlation was used to determine the correlation between spirituality and quality of life total score and within the subscales of the 2 measures. Multivariate linear regression was used to determine the independent variables affecting the quality of life. A P-value of <.05 was considered statistically significant.
Results
Sociodemographic and Clinical Data
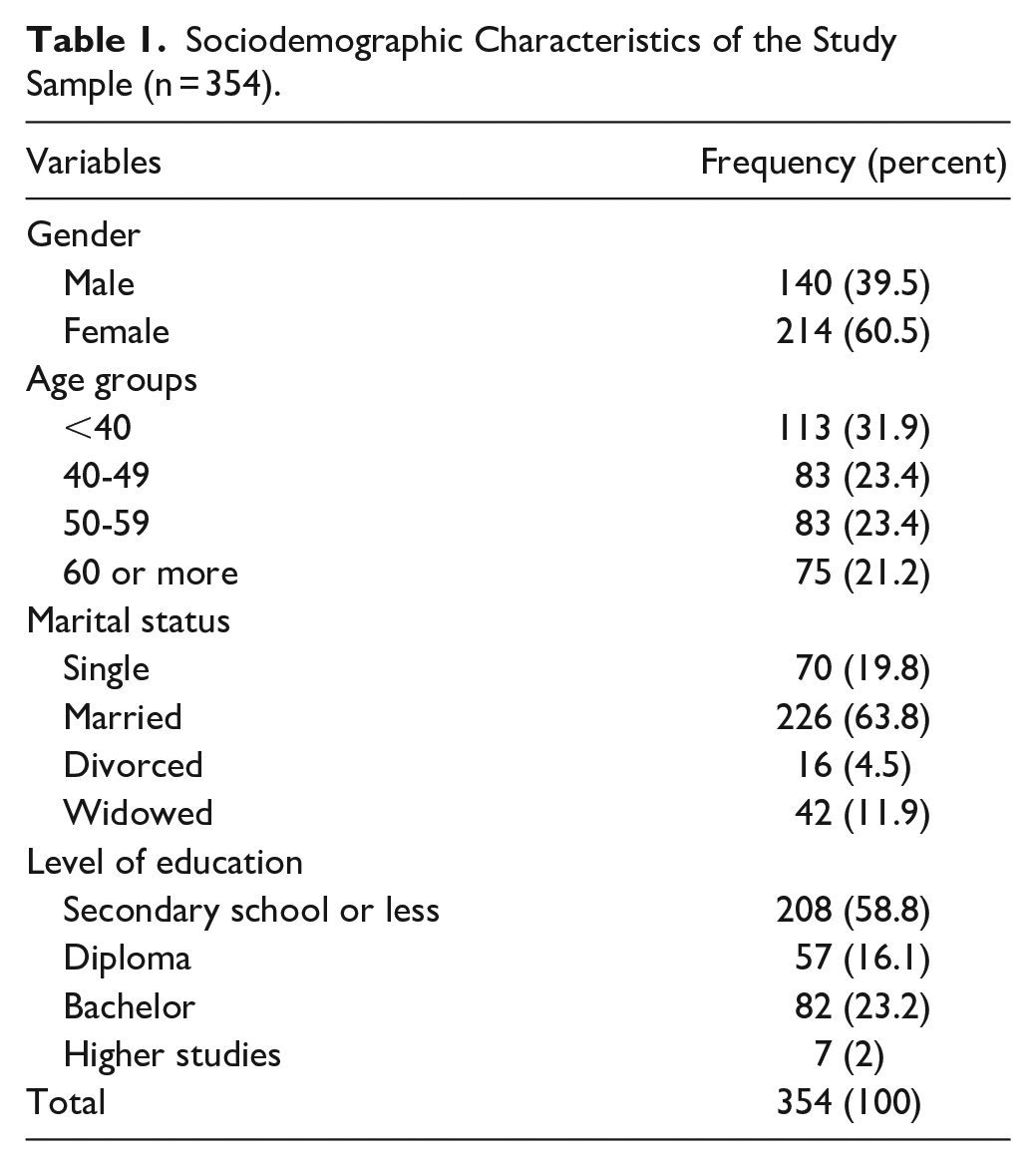
This study involved 354 cancer patients with a mean age of 46.4 ± 15.3 years. Initially, 380 patients were interviewed, but only 354 of them completed the whole questionnaire and were included in our study with a response rate of 93.16%. Two hundred fourteen patients (60.5%) were females, while men accounted for 140 patients (39.5%). One hundred thirteen patients (31.9%) were younger than 40 years old, 46.8% of patients were between 40 and 59 years old, and the rest were older than 60 years old. Most of the patients (63.8%) were married, and 58.8% had a secondary school education or less. Patients’ sociodemographic data are shown in Table 1.
Sociodemographic Characteristics of the Study Sample (n = 354).
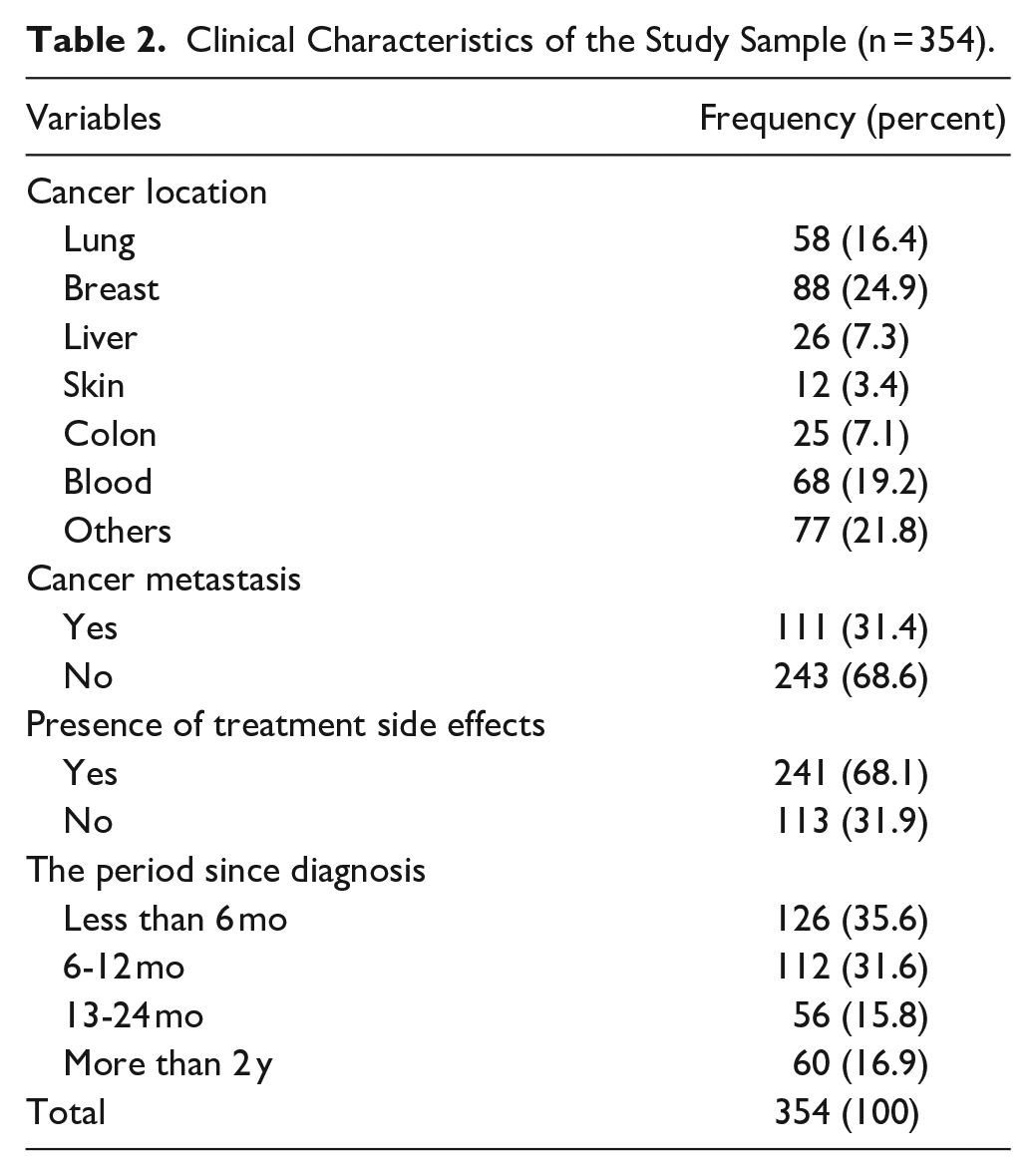
As shown in Table 2, 88 patients (24.9%) had breast cancer, 19.2% of patients had blood cancers, and 16.4% had lung cancer. The majority of patients (68.6%) did not have metastasis, 68.1% had experienced side effects, and 67.2% were diagnosed in the last 12 months.
Clinical Characteristics of the Study Sample (n = 354).
The Spirituality Scores Using the FACIT-Sp Scale
The spiritual well-being of patients reported in this study was measured by using the median FACIT-Sp total score, which was 35 (IQR: 29-42). FACIT-Sp subscale median scores were: meaning 12 (IQR: 9-15), peace 10 (7-13), and faith 15 (12-16). Table 3 shows the FACIT-Sp scores results.
The Spirituality Scores Using the FACIT-Sp Scale.

The Quality of Life Assessment Using the FACT-G Scale
The quality of life of patients assessed in this study was measured by using the median FACT-G total score, which was 63 (IQR: 52-85). FACT-G subscale median scores were: physical well-being 14 (IQR: 8-21), social well-being 23 (18-27), emotional well-being 15 (10-20), and functional well-being 16 (11-21). Table 4 shows the FACT-G scores results.
The Quality of Life Assessment Using the FACT-G Scale.

Association Between Patient Characteristics and Quality of Life
The patient’s quality of life was evaluated to determine whether there was an association with the patient’s spirituality or not. The results of FACT-G score correlations are listed in Table 5. There was a significant difference between FACT-G score with age intervals (P = .02), marital status (P = .001), cancer type (P < .001), presence of cancer metastasis (P < .001), presence of treatment side effects (P < .001), and the period since diagnosis (P = .001).
FACT-G Association With Patient Characteristics.

The Correlation Between FACIT-Sp and FACT-G
The findings of the FACIT-Sp and FACT-G scales and their subscales were analyzed to investigate their relationship. The subscales and the total score were investigated against each other, as shown in Table 6.
The Correlation Between FACIT-Sp and FACT-G.

Correlation is significant at the .05 level.
Correlation is significant at the .01 level.
FACIT-Sp total score had a significantly strong positive relationship with FACT-G total score (r = .705, P < .001). Also, it had a significant moderate positive correlation with the physical well-being subscale (r = .401, P < .001), a significant moderate positive correlation with the social well-being subscale (r = .632, P < .001), a significant strong positive correlation with the emotional well-being subscale (r = .704, P < .001), and a significant moderate positive correlation with the functional well-being subscale (r = .564, P < .001). Furthermore, FACIT-Sp subscales (meaning, peace, and faith) were also significantly positively correlated with the FACT-G total score and its subscales. First, the meaning subscale had a significant moderate positive correlation with FACT-G total score (r = .55, P < .001), a significant weak positive correlation with the physical well-being subscale (r = .331, P < .001), a significant moderate positive correlation with social well-being subscale (r = .504, P < .001), a significant moderate positive correlation with the emotional well-being subscale (r = .491, P < .001), and a significant moderate positive correlation with the functional well-being subscale (r = .458, P < .001). Second, the peace subscale had a significantly strong positive correlation with the FACT-G total score (r = .704, P < .001), a significant moderate positive correlation with the physical well-being subscale (r = .481, P < .001), a significant moderate positive correlation with the social well-being subscale (r = .470, P < .001), a significant strong positive correlation with the emotional well-being subscale (r = .714, P < .001), and a significant moderate positive correlation with the functional well-being subscale (r = .596, P < .001). Finally, the faith subscale had a significant moderate positive correlation with the FACT-G total score (r = .455, P < .001), a significant weak positive correlation with the physical well-being subscale (r = .133, P = .012), a significant moderate positive correlation with the social well-being subscale (r = .599, P < .001), a significant moderate correlation with the emotional well-being subscale (r = .509, P < .001), and a significant moderate positive correlation with the functional well-being subscale (r = .300, P < .001).
Multivariate Linear Regression Analysis of FACT-G
Regression analysis was used to better understand the connection between the variables. The FACT-G total score and FACT-G subscales scores had been used as dependent variables and the rest of the variables connected with each domain as independent variables to identify which variable had the exact correlation.
Regression analysis revealed that patients who had no metastasis were independently associated with higher FACT-G total scores (P < .001). Also, patients who didn’t experience treatment side effects were independently linked with a higher FACT-G total score (P < .001). Moreover, patients with higher meaning subscale scores were independently associated with higher FACT-G total scores (P = .004). Furthermore, patients with higher peace subscale scores were independently associated with higher FACT-G total scores (P < .001). Finally, patients with higher faith subscale scores were independently associated with higher FACT-G total scores (P < .001). Table 7 lists the significantly associated parameters with the FACT-G total score.
Multivariate Linear Regression Analysis of the FACT-G Score Correlations With Patients’ Characteristics and Spirituality Level (R square = .621).

Cancer Type Association With Other Clinical Characteristics
Table 8 illustrates that the presence of metastasis is significantly variable based on the cancer type. It was observed that the metastasis percentage was highest in blood and skin cancer while it was lowest among those with breast and liver cancers. There were no significant variations in the presence of side effects and the period of diagnosis between different cancers.
Chi-square Analysis for the Association Between the Cancer Type and the Presence of Metastasis, Treatment Side Effects, and the Period of Diagnosis.

Discussion
Cancer patients experience a wide range of symptoms as part of the disease progression and treatment side effects. Consequently, their quality of life is usually impaired. 29 The mean total FACT-G score among cancer patients in our study is nearly 66, which is comparable to an Austrian study that also showed lower FACT-G scores among severely and mildly chronically diseased groups compared with healthy individuals. 30 These findings were also supported by another study on gynecologic cancer survivors where the score of the overall quality of life and the 4 subscales; social, physical, physical, and emotional well beings were significantly improved after treatment of cancer. 31 Nearly similar scores were also observed in a study on black patients treated for cancer: the mean scores were 68.33, 14.69, 22.33, 17.54, and 13.87 compared with 66.22, 13.96, 21.97, 14.45, and 15.83 in the current study for the total FACT G, physical, social, emotional, and functional well-being, respectively. 32
In contrast, another Jordanian study on females with breast cancer showed higher FACT-G scores (mean = 79) among patients; however, this variation may be attributed to the enrollment of males and females with different types of cancers in this study. 33
The spirituality total score in our study is 34.83 with the highest score in the faith subscale. Higher total FACIT-Sp and the 3 subscales scores were observed among black cancer patients (Mean FACIT-Sp = 40.47), and similarly, faith was the highest score among them. 32 In Japan, a slightly lower spirituality using the FACIT-Sp (mean = 31), but a greater quality of life (mean FACT-G = 76) were observed among outpatient cancer patients treated with chemotherapy. 34 These variations in spirituality and quality of life could be attributed to the variations in the population characteristics, the country’s prevalent religious beliefs, and the quality of the health system.
The quality of life is variable based on the patient’s characteristics such as age, gender, living situation, and diagnoses based on previous population-based surveys35,36 and this is in line with variations observed among cancer patients. The presence of cancer metastasis and treatment side effects were associated with lower quality of life and these findings are consistent with previous studies, that also revealed a lower quality of life in patients experiencing pain and psychological distress. 37 The quality of life was also variable based on the type of cancer, and this could be explained by differences in the disease prognosis, clinical features, and treatment strategies.
In accordance with our results, a strong positive correlation between spirituality and quality of life has been reported.26,33,38 However, the correlations between the subscales were variable. The strongest correlation in our study was between the total quality of life and the peace subscale of spirituality and between the total spirituality and emotional subscale of the quality of life which are likewise the outcomes of an Indonesian study. 39 Spiritual pain was found to be greater among cancer patients with emotional symptoms which were also associated with increased depression and anxiety in a previous study. 40 In contrast, the strongest correlation was between spiritual well-being and functional well-being among breast cancer patients in another study. 33 Consequently, it is vital to incorporate spirituality into the healthcare system to sustain a better quality of life among cancer patients. Interventions could be carried out through healthcare providers and family members to improve the faith, peace, and meaning of life. It was reported that addressing spiritual issues in workshops for nurses had improved their ability to conduct spiritual care. 41
Spirituality among cancer patients should be a focus of attention as a vital part of the treatment and clinical care. Well-organized strategies should be developed to improve cancer patients’ spirituality and subsequently their quality of life such as introducing the concepts of trust, peace, and faith at the cancer units in hospitals besides making the medical staff and patients’ relatives more familiar with the importance of spirituality on cancer patients quality of life. It is also recommended to conduct further studies based on a longitudinal approach to get more insight into the effect of spirituality on the quality of life among cancer patients where individual variations can be excluded.
Limitations of the Study
The study at hand comes with specific constraints, employing a convenience sampling method, making it challenging to extend the findings to a broader context. Some cancer patients were illiterate and others were severely ill and could not fill out the questionnaire independently. A group of cancer patients was not accessible because cancer patients follow variable treatment protocols; some of them have their chemotherapy sessions less frequently and others have oral treatment at home. Moreover, there was some difficulty in comparing the current study findings with studies that used different instruments to evaluate spirituality and quality of life among cancer patients. Additionally, despite the study’s substantial sample size, it’s important to note limitations associated with the survey approach, as questionnaire responses may not precisely represent the patients’ actual conditions.
Conclusions
Spiritual well-being and quality of life have been linked in several studies. The usage of 2 validated scores (FACT-G and FACIT-sp) was useful in assessing the spirituality and quality of life among cancer patients in Palestine. Hence, the current study was able to conclude that spiritual well-being had a positive impact on patients with cancer in Palestine. The more spiritual well-being a patient has the better health-related quality of life they live. The quality of life among cancer patients extends beyond primary clinical care, addressing palliative care through spiritual care is of great importance in chronic diseases including cancer to afford better physical, social, emotional, and functional well-being. It is important to create a multidisciplinary strategy that integrates spiritual care into the healthcare system.
Footnotes
Acknowledgements
Not applicable.
Author Contributions
MJ: Study conceptualization, data collection, and manuscript writing. AD: Study conceptualization, data collection, data analysis, manuscript writing, and editing. MR: Study conceptualization, data collection, data analysis, manuscript writing, and editing. RQ: Manuscript writing, reviewing, and editing. MN: Data collection and manuscript writing. AN: Data collection and manuscript writing. NA: Data collection and manuscript writing.
Availability of Data and Materials
All data are included in the manuscript
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research Ethics and Patient Consent
This study was officially approved by the Institutional Review Board at An-Najah National University located in Nablus/Palestine (Ref: Med. Sep. 2021/20)