
Abstract
Background:
At present, simple reminiscence has been widely used in the field of neurocognitive disorders, life review/life review therapy has been widely used in the field of cancer, and both simple reminiscence and life review/life review therapy are suitable for psychological disorders such as depression and anxiety. However, the efficacy of reminiscence in treating cancer-related symptom has not been fully assessed.
Objectives:
To evaluate the effect of reminiscence therapy (RT) on relieving cancer-related symptoms such as anxiety and depression in cancer survivals.
Methods:
China National Knowledge Infrastructure (CNKI), VIP database, Wanfang Data Knowledge Service Platform, China Biomedical Database, PubMed, Cochrane Library, Embase, EBSCO, Scopus, and Ovid databases were searched. To collect clinical randomized controlled trials (RCT) on RT and cancer-related studies published from the establishment of the database to October 05, 2021. Two researchers independently evaluated the articles that met the inclusion criteria, meta-analysis was performed using RevMan5.4 software.
Results:
A total of 20 RCTs published in 2010 to 2021 were included, with a total of 1853 cancer patients. Meta-analysis results showed that the anxiety scale (HADS-A and HAMA and SAS) and depression scale (HADS-D and HAMD and SDS) scores of the RT group were significantly lower than those of the control group (HADS-A: P = .0002; HAMA: P < .00001; SAS: P = .0010; HADS-D: P = .01; HAMD: P < .00001; SDS: P = .0001). Meta-analysis results showed that RT can improve overall quality of life of cancer patients of RT group to a certain extent hope (P < .00001). Meta-analysis results showed that the scores on the hope and dignity were significantly increased, and the difference were statistically significant (P < .001).
Conclusion:
This review indicates that RT has significant efficacy on cancer-related symptoms such as anxiety and depression. RT for cancer survivals can effectively improve quality of life, self-hope, and self-esteem. The findings of this meta-analysis can provide direction for future symptom management research.
Introduction
Cancer is one of the public health problems that threaten human health. 1 According to the statistical report of the International Agency for Cancer, new cancer cases worldwide are expected to rise by 50% from 18 million in 2018 to 27 million in 2040. 2 Significant physical and psychological changes will occur as a result of long-term treatment in cancer survivors. 3 About 30% to 45% of cancer survivors experienced depression and anxiety, 4 which affects cognitive functioning 5 and may persist after treatment. 6 In addition, incurable cancer also has a direct impact on cognition7,8 and makes it difficult for patients to deal with social and existential issues. This affects the patient’s self-esteem, quality of life, and hopes for the future. 9
Psychosocial care is one of the important approaches for cancer survivors to alleviate negative emotions and psychological symptoms like anxiety and depression.10,11 Psychosocial care commonly includes cognitive behavioral therapy (CBT), 12 mindfulness therapy, 13 music therapy, 14 and reminiscence therapy (RT), 15 and others. RT, a common method of social psychological intervention, mainly refers to discussing past activities, events, and experiences under some tangible cues (such as photos, familiar objects, music, and recordings). 16 RT can reduce depression and anxiety symptoms in patients with dementia and improve cognitive function, 17 and it can reduce negative reminiscence and increase positive reminiscent function. 18 It is a popular non-pharmacological treatment for Alzheimer’s disease, stroke-related cognitive impairment, or depression.19 -21
There are 3 main types of RT: simple reminiscence, life review, and life review therapy. 22 Simple reminiscence usually focuses on the individual’s own pleasant and happy memories, 23 and can be carried out in groups, pairs, or one-on-one by nurses and social workers in the community, nursing homes, and other places. Life review is used for the exploration of both positive and negative life experiences. 24 It is usually conducted individually by an advanced interventionist, such as a psychiatrist or a senior nurse. Life review therapy requires a psychotherapist with relevant professional skills to reevaluate negative memories and reconstruct them in chronological order with a more optimistic outlook on life. 25 Each form of RT has its advantages and is alternative to pharmacological interventions that are provided during long-term care. Numerous studies have demonstrated that it is beneficial for improving the mood, cognition, and overall well-being of various populations.26 -30 However, little attention has been paid to the effects of different types of RT in cancer patients and whether different intervention Settings (hospital, home, and online) affect the effects of RT in cancer patients.
RT has been introduced into the cancer care in recent years.15,31 Anh et al 32 explored whether life review can modulate anxiety and depression in cancer survivors and improve their quality of life. However, Kleijn et al 33 found that life review has little effect on anxiety and depression in cancer patients. Therefore, the purpose of this study was to assess RT’s effectiveness in managing cancer-related symptom and understand the effects of different types of RT and the influence of care settings on RT. Meanwhile, the study aims to provide an evidence-based foundation for patient rehabilitation and nursing care.
Method
The Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines were followed for the methodology of this review. The review was registered in the INPLASY database and the registration number is: INPLASY202210053.
Data Sources and Search Strategies
Computer-based Chinese databases include SinoMed, China National Knowledge Infrastructure (CNKI), Wan Fang Data Knowledge Service Platform, and VIP Database; English databases include PubMed, Cochrane Library, Embase, EBSCO, and Scopus databases. A combination of subject headings and free words are used for retrieval, supplemented by manual retrieval. Search terms are neoplasms; cancer; tumor; malignancy; malignant neoplasms; neoplasms, malignant; reminiscence, RT, reminiscence treatment, reminiscence nursing, reminiscence intervention, life review therapy, life review; randomized controlled trial, controlled clinical trial, randomized, placebo, drug therapy, randomly, trial, groups, etc. The time span for retrieval is from the establishment of the database to October 5, 2021.
Studies Selection
Inclusion criteria include (1) research type: randomized controlled trial (RCT) in Chinese or English; (2) study population: cancer patients diagnosed with pathological tissue and imaging (aged 18 years and up); types of RT are not limited. Exclusion criteria consisted of (1) repeated published articles and (2) papers with no access to full text and raw data.
Data Extraction
Two researchers independently read the full text and recorded the first author’s name, year of publication, country, patient’s cancer type and course of the disease, patient age, sample size (number of intervention/controls groups), measures and time for intervention, outcome indicators (mainly), and follow-up time. For articles published on different aspects of the same trial or for duplicate publications, only the most comprehensive reports were included. Those with incomplete important data were requested from the authors by email. If the results of the literature were expressed in terms of median and interquartile ranges, an online calculator would be used to estimate and convert to mean ± standard deviation. 34
Methodological Quality Assessment
The quality of the literature reports was evaluated using the Cochrane Manual of Systematic Reviews, and 2 researchers independently evaluated the studies that met the inclusion criteria. If the original literature met the criteria, it shows that the occurrence of various biases may be minimal and that the study may have low risk (L); the partial satisfaction of the above quality criteria indicated that the possibility of bias occurrence is moderate and unclear (U); if the original study failed to meet the above-mentioned criteria, it means a high risk of bias (H).
Statistical Analyses
Data merging analysis and statistical heterogeneity test were performed using RevMan 5.4 software. 35 Data in the studies were analyzed using mean differences (MD) when using the same measurement tool and standardized mean differences (SMD) when using different measurement tools, and 95% confidence interval (CI) was calculated for each effect size. If P > 0.1 and I 2 ≤ 50%, the heterogeneity was insignificant, and the fixed-effects model was used for meta-analysis. Otherwise, the random-effects model was used. To ensure heterogeneity, subgroup analyses could be performed by dividing all data into smaller units and comparing within each subgroup. We undertook subgroup analysis by types (simple reminiscence versus life review) and intervention location (hospital vs home vs online). The descriptive analysis was applied if the heterogeneity was too high to be combined. If the combined statistic result was P < .05, the combined statistic of multiple similar studies was considered to be statistically significant.
Results
Study Selection and Characteristics
Initially, 347 articles were retrieved, and 196 were retained after duplication-checking. Later, 48 articles were pre-screened after reading the titles and abstracts, and 20 articles ultimately met the inclusion criteria. The literature screening process is shown in Figure 1.

Flowchart of systematic review.
All the 20 RCTs,33,36 -54 including 12 Chinese and 8 English articles, published in 2010 to 2021 totaled 1853 cancer survivors. Among the 20 RCTs included, there were mainly studies from China, Japan, the Netherlands, and Australia. The intervention types of RT were simple reminiscence and life review, but there was no life review therapy in the included articles. Due to the different selection of intervention topics, the duration of intervention varied from 1 week to a year, but majority of interventions took place once a week. Only 4 studies had further follow-up, with only 1 article employing a 36 months follow-up; the rest were all 1 month. Among the locations of sessions, 1 was held in the home, 2 were held through internet and the others were all held in the hospital. The basic characteristics of the included articles are shown in Table 1.
Basic Features of the Studies That Were Included.

Outcomes: ① HADS-A; ② HAMA; ③ SAS; ④ HADS-D; ⑤ HAMD; ⑥ SDS; ⑦ QLQ-C30; ⑧ HHI; ⑨ PDI; ⑩ SESS.
Quality and Risk of Bias Assessment
Two researchers used the Cochrane evaluation manual to conduct a strict quality evaluation of the included literature, and a third researcher intervened until all reached agreement after discussion. Of the 20 included pieces of literature, 11 generated random numbers using random number tables or computers. For the random number sequence, 5 papers reported the use of allocation concealment and another 5 ones used the intention-to-treat analysis. The overall quality of the studies was acceptable. The specific evaluation indicators and results are shown in Table 2.
Literature Quality Evaluation Form.

Abbreviations: Item 1, randomization; Item2, allocation concealment; Item 3, blindness of participants and personnel; Item 4, blindness of outcome evaluator; Item 5, outcomes measured reliably; Item 6, selective reporting; Item 7, Other bias. L, Low Risk; U, Unclear Risk; H, High Risk.
Overview of RT to Relieve Cancer-Related Symptoms
RT for anxiety
Anxiety was measured by the Hospital Anxiety and Depression-Anxiety (HADS-A), Self-Rating Anxiety Scale (SAS) and Hamilton Anxiety Rating Scale (HAMA) in this study. A total of 11 RCTs were included in the pooled meta-analysis to assess the effects of RT versus control group on anxiety in cancer patients. Three indicators of anxiety in cancer patients were significantly improved by RT (HADS-A:MD = −1.11, 95% CI: (−1.69, −0.53), P = .0002; HAMA:MD = −9.61, 95% CI: (−12.19, −7.03), P < .00001; SAS:MD = −6.12, 95% CI: (−9.76, −2.48), P = .0010; Figure 2). The fixed-effect model was used in HADS-A because of the insignificant heterogeneity (I 2 = 27%, P = .25) and the random model was used in HAMA (I 2 = 91%, P < .0001) and SAS (I 2 = 91%, P < .0001).
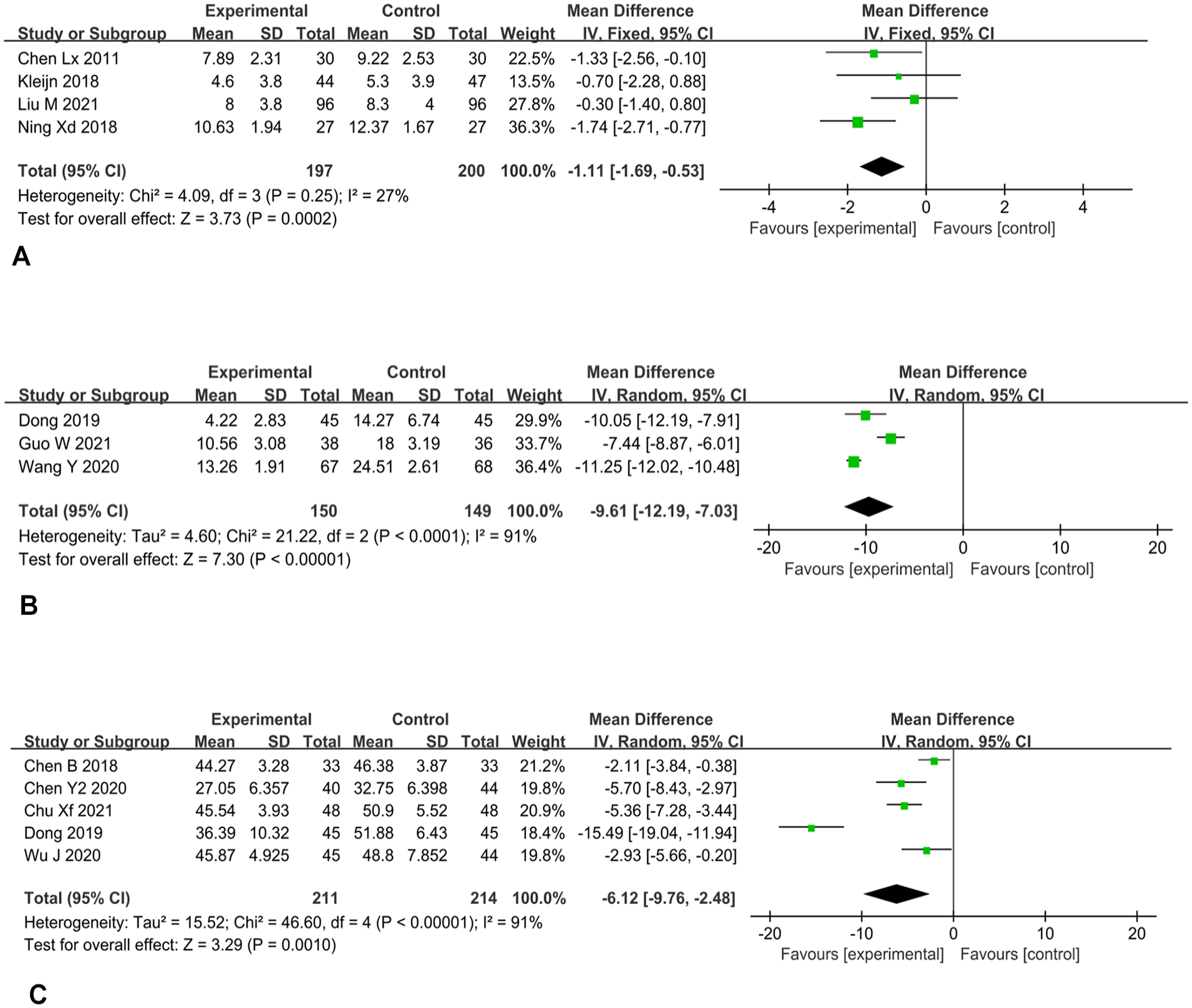
Effect of reminiscence therapy on anxiety in cancer patients. (A) HADS-A was used as an indicator of anxiety. (B) HAMA was used as an indicator of anxiety. (C) SAS was used as an indicator of anxiety.
RT for depression
Like anxiety, depression was also measured by 3 indicators in this study: Hospital Anxiety and Depression-Depression (HADA-D), Self-Rating Depression Scale (SDS) and Hamilton Depression Rating Scale (HAMD). A total of 12 RCTs exploring the effect of RT on depression among cancer patients were included for a pooled meta-analysis. RT did significantly alleviate depressive symptoms in patients with cancer (HADS-D:MD = −1.51, 95% CI: (−2.71, −0.31), P = .01; HAMD:MD = −10.45, 95% CI: (−14.58, −6.33), P < .00001; SDS:MD = −6.63, 95% CI: (−10.05, −3.21), P = .0001; Figure 3). The random-effect model was used because of the significant heterogeneity (HADS-D: I 2 = 71%, P = .02; HAMD: I 2 = 98%, P < .00001; SDS; I 2 = 90%, P < .0001).
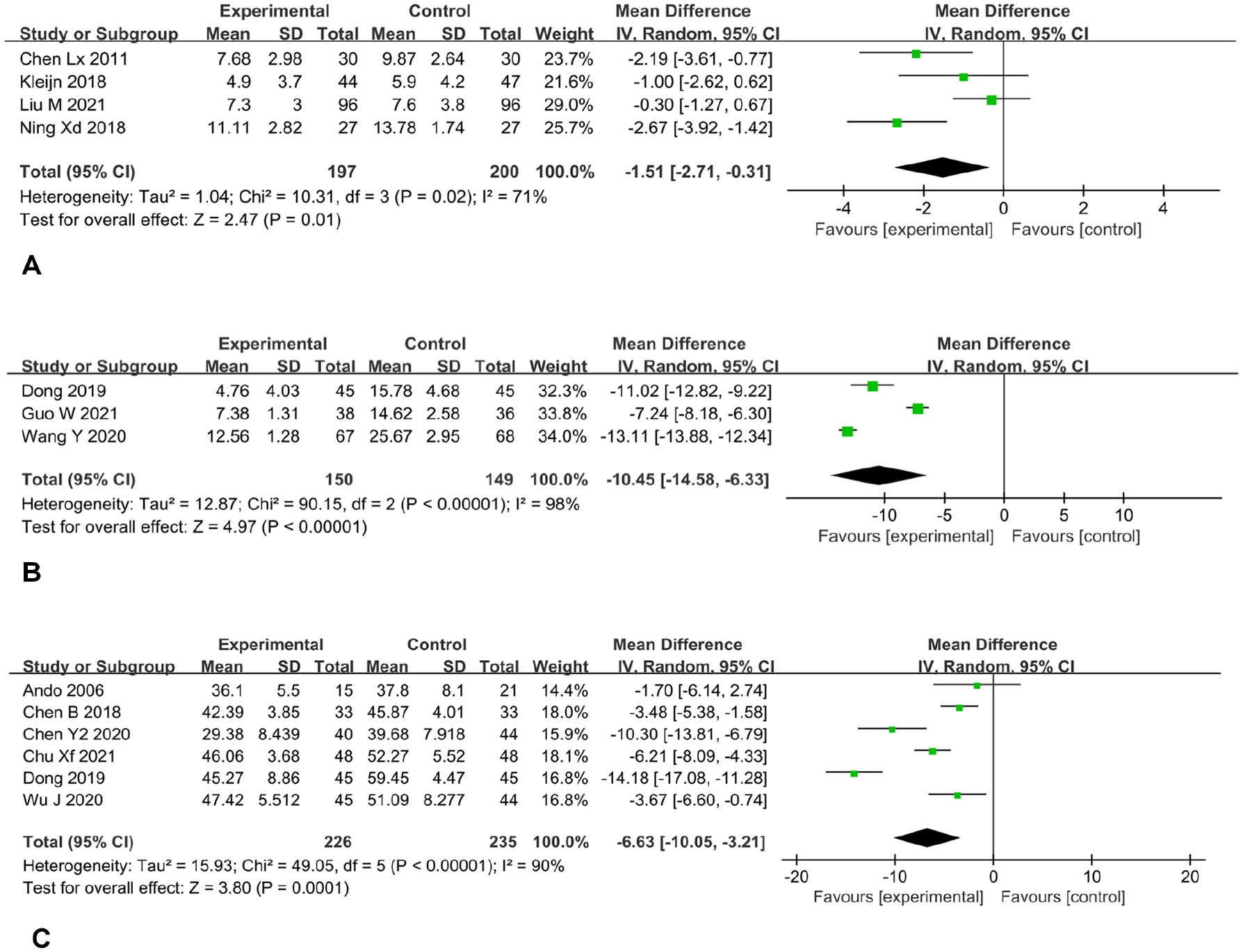
Effect of reminiscence therapy on depression in cancer patients: (A) HADS-D was used as an indicator of depression. (B) HAMD was used as an indicator of depression. (C) SDS was used as an indicator of depression.
RT for quality of life
Four studies investigating the effect of RT on the ability of daily living in cancer patients were included for a pooled meta-analysis. RT showed significant effect in improving the quality of life in patients with cancer (MD = 7.77, 95% CI: (4.62, 10.93), P < .00001; Figure 4). The random-effect model was used (I 2 = 89%, P < .00001).

Effect of reminiscence therapy on living quality in cancer patients.
RT for hope and self-esteem
Four studies evaluated the hope of participants using the Herth Hope Index (HHI). Pooled results revealed significant difference between groups (MD = 5.36, 95% CI: (2.72, 8.00), P < .00001; Figure 5). The random-effect model was used (I 2 = 92%, P < .00001).

Effect of reminiscence therapy on hope (HHI) in cancer patients.
Self-esteem was measured by the Patient Dignity Inventory (PDI) and the Social Self-Esteem Scale (SSES) in this study. A total of 5 RCTs were included in the pooled meta-analysis to assess the effects of RT versus control group on self-esteem in cancer patients. Two indicators of self-esteem in cancer patients were significantly improved by RT (PDI:MD = −8.38, 95% CI: (−14.21, −2.55), P = .005; SSES:MD = 7.32, 95% CI: (2.67, 11.96), P = .002; Figure 6). The random-effect model was used in PDI (I 2 = 84%, P = .01) and MMSE (I 2 = 83%, P = .003) because of the significant heterogeneity.

Effect of reminiscence therapy on self-esteem in cancer patients. (A) PDI was used as an indicator of self-esteem. (B) SSES was used as an indicator of self-esteem.
Subgroup analysis of anxiety and depression
In this study, we undertook subgroup analysis by types of RT and location of sessions. Subgroup analysis showed that life review improved patients’ anxiety (HADS-A) to a certain extent (MD = −1.11, 95% CI: (−1.69, −0.53), P = .0002); simple reminiscence, single life review, and life review combined with humanistic care/-psychological pain management all relieved anxiety (SAS) of patients to some extent (MD = −6.12, 95% CI: (−9.76, −2.48), P < .00001; Figure 7). Life review improved patients’ depression (HADS-D) to a certain extent (MD = −1.51, 95% CI: (−2.71, −0.31), P = .01). Simple reminiscence, single life review, and life review combined with humanistic care/psychological pain management improved depression (SDS) to some extent (MD = −6.63, 95% CI: (−10.05, −3.21), P < .00001; Figure 8).

Subgroup analysis based on different types of RT in anxiety. (A) HADS-A was used as an indicator of anxiety. (B) SAS was used as an indicator of anxiety.

Subgroup analysis based on different types of RT in depression. (A) HADS-D was used as an indicator of depression. (B) SDS was used as an indicator of depression.
In the aspect of location of sessions, subgroup-analysis showed that different location (hospital vs online vs home) made no differences in anxiety (SMD = −1.29, 95% CI: (−1.90, −0.67), P < .0001; Figure 9), depression (SMD = −1.52, 95% CI: (−2.20, −0.85), P < .00001; Figure 10), and quality of life (MD = 7.77, 95% CI: (4.62, 10.93), P < .00001; Figure 11).

Subgroup analysis based on location of sessions of RT in anxiety.

Subgroup analysis based on location of sessions of RT in depression.

Subgroup analysis based on location of sessions of RT in quality of life.
Discussion
Summary of Evidence
RT originated from Butler’s “Life Review” and “Reminiscence” theory. 55 Based on literature review, Lin et al 56 proposed a theoretical framework for RT, which was divided into 5 stages. Justo-Henriques et al 57 has published a full RT protocol in Portuguese, which includes timing and specific content. What’s more, to clarify and promote the development of the concept, the classification of RT used in the current study was proposed by Webster et al 58 in 2010. Based on different uses of reminiscence function, RT is divided into 3 categories, that is, simple reminiscence, life review, and life review therapy, which is also a mainstream classification method currently. However, several studies59,60 involved also used the classification proposed by Burnside and Haight in the 1990s. They completely differentiated RT and life review: the former focuses on pleasant and happy memories (similar to Webster’s proposal of simple reminiscence, which was considered as an umbrella term including 3 categories), while the latter aims to evaluate and integrate memories. As a kind of psychosocial therapy, RT was commonly introduced to old people in late 1980s due to its simple, comprehensible, low-cost, and risk-free nature.61,62 Also, RT is being used by many nursing researchers to treat patients with various cancers, 63 dementia, 64 and depression. 65 However, although an increasing number of nurses apply RT to improve patients’ mood and quality of life, in the concrete implementation process, Burnside and Haight 66 have shown that due to a mistrust of the operators, life review may need to involve techniques related to psychological counseling, in response to patients’ complex issues like a refusal to share or emotional breakdown.
This updated meta-analysis synthesized the pooled effect of RT in cancer care. Findings of this review indicated that RT had significant efficacy on cancer-related symptoms such as anxiety and depression, which could improve cancer patients’ emotion, hope, self-esteem, and physical well-being.
Discussion of the Main Results
This meta-analysis suggested that RT was more effective than routine care in improving anxiety and depression in patients with cancer and promoting the recovery of their emotional distress. A meta-analysis of Tam et al 67 also observed that RT can alleviate depression and improve life satisfaction in older adults. To interpret these results, several possible factors are as follows. First, RT promotes positive feelings by repeatedly reconstructing life stories with patients, which promotes a positive experience and forms a sense of self-identity, so that their mental health is improved and their anxiety and depression relieved.29,68 Second, accompanying patients and paying attention to them in the process of reminiscence also reduce patients’ loneliness and affect their mood directly. In addition, another possible reason for the changes is related to patients’ improved cognitive impairment. 29 Cancer-related cognitive impairment (CRCI) 69 refers to the occurrence of cognitive dysfunction caused by the damage of functional structure in patients’ brains caused by cancer. At present, research of RT on CRCI is relatively rare. However, several studies have shown that RT can improve cognitive impairment in patient with dementia or stroke.70,71 Given the interactive relationship among anxiety, depression, and cognition in cancer patients, 72 it is reasonable that RT may improve cancer patients’ mood by improving their cognition, a suggestion that needs future research to further support this idea.
Besides the types of RT, many factors, including location of sessions, personnel qualification, and duration may affect RT. Woods et al, 64 for example, found that the care home was superior to community in choosing place for dementia patients to reminisce. However, subgroup of the current study did not reach a similar conclusion, finding that choosing home versus hospital had little effect on reminiscence. Thus, further research is needed.
The meta-analysis of results of the 4 covered studies showed that there was significant difference in quality of life between the reminiscence group and the control group, indicating that RT may have effects in improving quality of life in patients with cancer. Moreover, by enrolling 210 colorectal cancer survivors who underwent surgery, a study 15 observed that RT not only remarkably alleviated anxiety but also improved patients’ quality of life. The possible reasons for these results might be that conversational function, boredom reduction, and intimacy maintenance of RT can indirectly help elders improve life satisfaction and reduce perceived stress and enhance their motivation, further improving the QoL in cancer patients.73,74
In addition, reminiscence-based intervention was effective in enhancing self-esteem, and promoting hope. 67 Hope was found to enhance overall health and well-being in cancer survivors undergoing chemotherapy. 75 Moreover, researchers also found that the more social support cancer patients receive, the higher the level of hope they will attain. 76 What is more, almost all patients having trouble with self-esteem may maintain a discrepancy between current and ideal /past self-images. As the mean self-esteem increasesd significantly after the life-review therapy sessions, whereas the scores of the comparison group did not change, this meta-analysis 60 also indicated that RT helps to build higher self-esteem in cancer survivals.
Limitations
Although this study provides some evidence-based proofs against controversies and for future clinical practice, there are still several limitations. First, since few studies have observed long-term results, it is impossible to evaluate the late efficacy and continuity of the effect of RT. Second, as the timing and frequency of interventions vary widely across cancer types and stages, few studies in an acceptable number of included studies could be pooled if various outcome measures, especially those of cognitive function were further considered. Finally, not all patients are willing to share their memories of the past with strangers, which increases the difficulty of RT execution and is also one of the reasons why quality of the existing research is relatively poor.
Conclusion
The efficacy of RT in alleviating anxiety, depression, and improving quality of life, self-hope, and self-esteem in cancer survivals has been preliminarily affirmed. However, choosing location of sessions (home or hospital) had little effect on reminiscence, thus, further research is needed. In addition, although cognition relates closely to anxiety or expression, the study found that there are few original studies on RT for cognitive impairment in cancer patients. Therefore, it is recommended that researchers should conduct original research in future studies to clarify the efficacy of RT in cancer-related cognitive impairment.
Supplemental Material
sj-docx-1-ict-10.1177_15347354221147499 – Supplemental material for The Efficacy of Reminiscence Therapy in Cancer-Related Symptom Management: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-ict-10.1177_15347354221147499 for The Efficacy of Reminiscence Therapy in Cancer-Related Symptom Management: A Systematic Review and Meta-Analysis by Jie Sun, Jieting Jiang, Yiyan Wang, Mingyue Zhang, Lu Dong, Kunpeng Li and Caiqin Wu in Integrative Cancer Therapies
Footnotes
Author Contributions
Search, Data curation, Formal analysis, and Original draft: Jie Sun and Jieting Jiang; Conceptualization and Risk of bias assessments: Yiyan Wang; Data curation: Mingyue Zhang; Formal analysis: Lu Dong; Conceptualization: Kunpeng Li; Manuscript Review & Editing, Supervision, and Project administration: Caiqing Wu. All authors read and approved the final manuscript.
Availability of Data
All the datasets of the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the 2021 Shanghai University of Traditional Chinese Medicine Budget Research Project, No. 2021LK014; School of Nursing Discipline Ability Improvement Project in 2022 (2022HLXK07).
Reporting Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.