
Abstract
Objective:
This study retrospectively examined the association between cancer-related fatigue (CrF) and the number of falls during the last 12 months in patients with myeloproliferative neoplasms (MPNs).
Methods:
A multicenter, 1-time anonymous survey was conducted using analog and digital questionnaires. Sex-stratified multinomial logistic regression analysis was applied to investigate the association between CrF and number of falls. All analyses were adjusted for age, school education, body mass index, MPN subtype, and quality of life.
Results:
The final sample comprised 688 patients (mean age 57.4 ± 13.8, 62.4% women). The fall rate was 16.2% in women and 12.2% in men (P = .153). There were no differences between women and men in terms of CrF between individuals with more than 1 fall, whereas women with 1 fall had a higher CrF compared to those without a fall (RRR = 1.019; 95% CI [1.002-1.039]), respectively.
Conclusion:
CrF increases the risk of falls in women with MPN. Physicians should evaluate and manage CrF symptoms and implement fall prevention strategies for those who are at increased risk. Further research is needed to better understand the effects of CrF on gait performance and associated fall risk.
Keywords
Introduction
One potential sequela of cancer is an increased risk of falling. 1 Falls in adults with cancer are more common than in non-cancer controls. 2 Disease- and treatment-related side effects (DTrSEs) of cancer are known to impair the body′s system. 3 DTrSEs comprise limited physical and cognitive functions, impairment of balance and gait performance as well as (joint-) pain. These DTrSEs were found to be associated with the risk of falling, independent of age.4-6 Further, cancer-related fatigue (CrF) is one of the most common and distressing side effects during and after cancer treatment. 7 CrF is described as a multi-dimensional phenomenon, showing physical, emotional, and cognitive manifestations such as tiredness, diminished concentration, and decreased motivation for or interest in engaging in daily activities.7,8 To date, little is known about the association between and the susceptibility to falls in cancer patients. Therefore, the aim of this study was to investigate (1) the prevalence of moderate to severe CrF, (2) the rate of falls within the last 12 months, and (3) the association between CrF and falls in a sample of 688 patients with myeloproliferative neoplasms (MPNs). As secondary outcomes, we examined the associations between DTrSEs, including CrF, age, body mass index (BMI), and patients’ health-related quality of life (QoL).
Methods
Study Design, Setting, and Participants
The study was designed as a retrospective, multicenter cross-sectional study. Adult patients (≥18 years) from 12 treatment centers of the East German Study Group Hematology and Oncology (OSHO; Supplemental Table 1) with an MPN were asked to fill in a paper-pencil questionnaire during consultation. Data were collected between January 2021 and September 2021. The opportunity to fill in an online version of the survey was added in April 2021. The sample includes patients of the LeukaNET/Leukaemia-Online patient network as well as the German, Austrian, and Swiss MPN patient network.
Sample Size
MPN diagnoses are rare among hematological diseases. Further, it was assumed that retrospective falls within the last 12 months are rare events too. Therefore, an exploratory survey was designed as a multicenter study with a target sample size of N ≥ 500.
Variables and Data Measurements
For the analysis of the primary outcome, the association between CrF and falls was assessed by means of the MPN Symptom Assessment Form (MPN-SAF), 9 ranging from 0 (absent) to 100 (worst imaginable), and the prevalence and severity of CrF were recorded. Likewise, the number of falls in the last 12 months was inquired.
To enable the description of the sample and analysis of secondary outcomes (associations between DTrSEs, including CrF, age, BMI, and patients’ QoL), the following variables were collected: demographic information (gender, age, and school education), height, and weight. Based on the German school system, years of schooling were categorized as less than 10 years, 10 years, or more than 10 years. BMI was calculated by dividing self-reported body weight in kilograms by self-reported height in meters squared. Clinical information: MPN subtype, year of diagnosis, potential side effects of MPN such as splenomegaly. The QoL was assessed using a visual analog scale ranging from 0 (very poor) to 100 (very good). DTrSE including concentration problems, bone and muscle pain were assessed by the MPN-SAF. All DTrSEs were categorized according to the scoring of the MPN SAF as follows: 0 = none, 1 to 30 = mild, 31 to 70 = moderate, and 71 to 100 = severe. 10
Statistical Analysis
Descriptive participant characteristics (mean, standard deviation, and percentages) were calculated. In addition, continuous data were tested for normal distribution using the Shapiro-Wilk test. The Spearman correlation was used to determine the strength of linear correlations (interpretation of correlation coefficient r: .10 to .30 = weak, ≥.30 to .50 = medium, ≥.50 = strong). To meet the study objectives, sex-stratified multinomial logistic regression analysis was undertaken. The sample was divided into 3 groups based on how frequently falls were reported in the last 12 months (no fall, 1 fall, and >1 fall). Regression models were adjusted for age, school education, BMI, MPN subtype, and QoL.
The statistical software SPSS 25.0 (SPSS Inc., Chicago, IL, USA) and Stata 14.2 (StataCorp 2015, College Station, TX, USA) were used for analyses. Statistical significance was assumed for P < .05. Cases with missing values were excluded list-wise.
Ethical Considerations
This study was approved by the Ethics Committee of the University of Rostock (A 2020-0274), and registered with the German Registry of Clinical Trials (DRKS00023698).
Results
Sample Characteristics
The flowchart for the study is presented in Figure 1. In total, 750 questionnaires were received, of which n = 300 (40%) were analog and n = 450 (60%) digital. Reasons for exclusion of questionnaires were missing information on diagnosis or a diagnosis other than chronic myeloid leukemia, polycythemia vera, essential thrombocythemia, or myelofibrosis. This was because the MPN subtype was adjusted in the regression model. Other reasons for exclusion were missing information on QoL, side effects, and falls. The final sample comprised 688 questionnaires.

Flow chart of the study.
The individuals were diagnosed between 1981 and 2021. The median age of onset was 50 ± 14 years. Data indicated significant gender-specific differences in MPN subtype (P < .001).
Prevalence of Moderate to Severe Cancer-Related Fatigue
CrF showed the highest prevalence among DTrSEs at 87% and was rated as moderate to severe (scale >30) by 55% of respondents.
Prevalence Rate of Falls
Falls occurred at a rate of 14.7%. Almost half of those with at least 1 fall during the last 12 months reported more than 1 fall (range: 1-18; Table 1).
Cohort Characteristics and Reported Symptoms (n = 688).

Data are presented as mean ± standard deviation for continuous variables and as number (%) for categorical variables. Presented P-values for comparisons between women and men are based on Mann-Whitney U test and chi-square test for categorical variables.
Abbreviations: n, number of patients; BMI, body mass index; CML, chronic myeloid leukemia; PV, polycythemia vera; ET, essential thrombocythemia; MF, myelofibrosis; DTrSE, disease- and treatment-related side effects.
Adjusted MPN Symptom Assessment Form, range 0 to 100, higher values represent more discomfort.
Visual analog scale, range 0 to 100, higher values represent high quality of life.
Bold: statistically significance, *P ≤ .05. **P ≤ .01.
Association Between Cancer-Related Fatigue and Falls
In adjusted sex-stratified multinomial logistic regression analysis, CrF was not associated with falling more than once in either gender when compared to no incident of falling (Tables 2 and 3). Women who reported 1 fall had a significantly higher CrF than those without a fall (RRR = 1.019; 95% CI [1.002-1.039]; Table 2). There was an association in men between the history of more than 1 fall compared to no fall and severe concentration problems (RRR = 1.051; 95% CI [1.020-1.084]; Table 3). These results remained stable after adjusting for time since first diagnosis (Supplemental Tables 2 and 3).
Association of Falls, Symptoms, and Demographic Characteristics in Women (n = 398, Multinomial Logistic Regression Analysis a ).
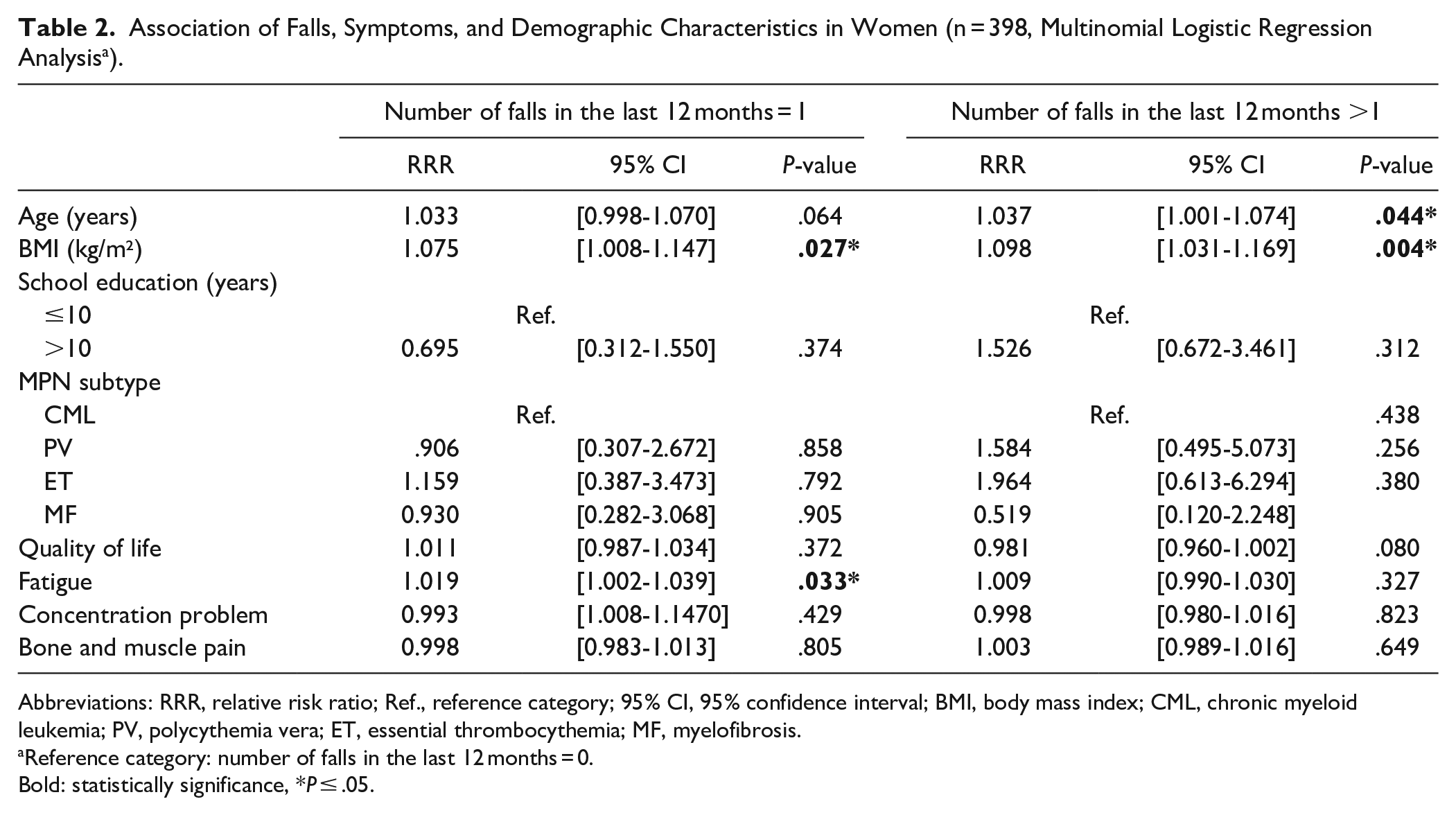
Abbreviations: RRR, relative risk ratio; Ref., reference category; 95% CI, 95% confidence interval; BMI, body mass index; CML, chronic myeloid leukemia; PV, polycythemia vera; ET, essential thrombocythemia; MF, myelofibrosis.
Reference category: number of falls in the last 12 months = 0.
Bold: statistically significance, *P ≤ .05.
Association of Falls, Symptoms, and Demographic Characteristics in Men (n = 222, Multinomial Logistic Regression Analysis a ).
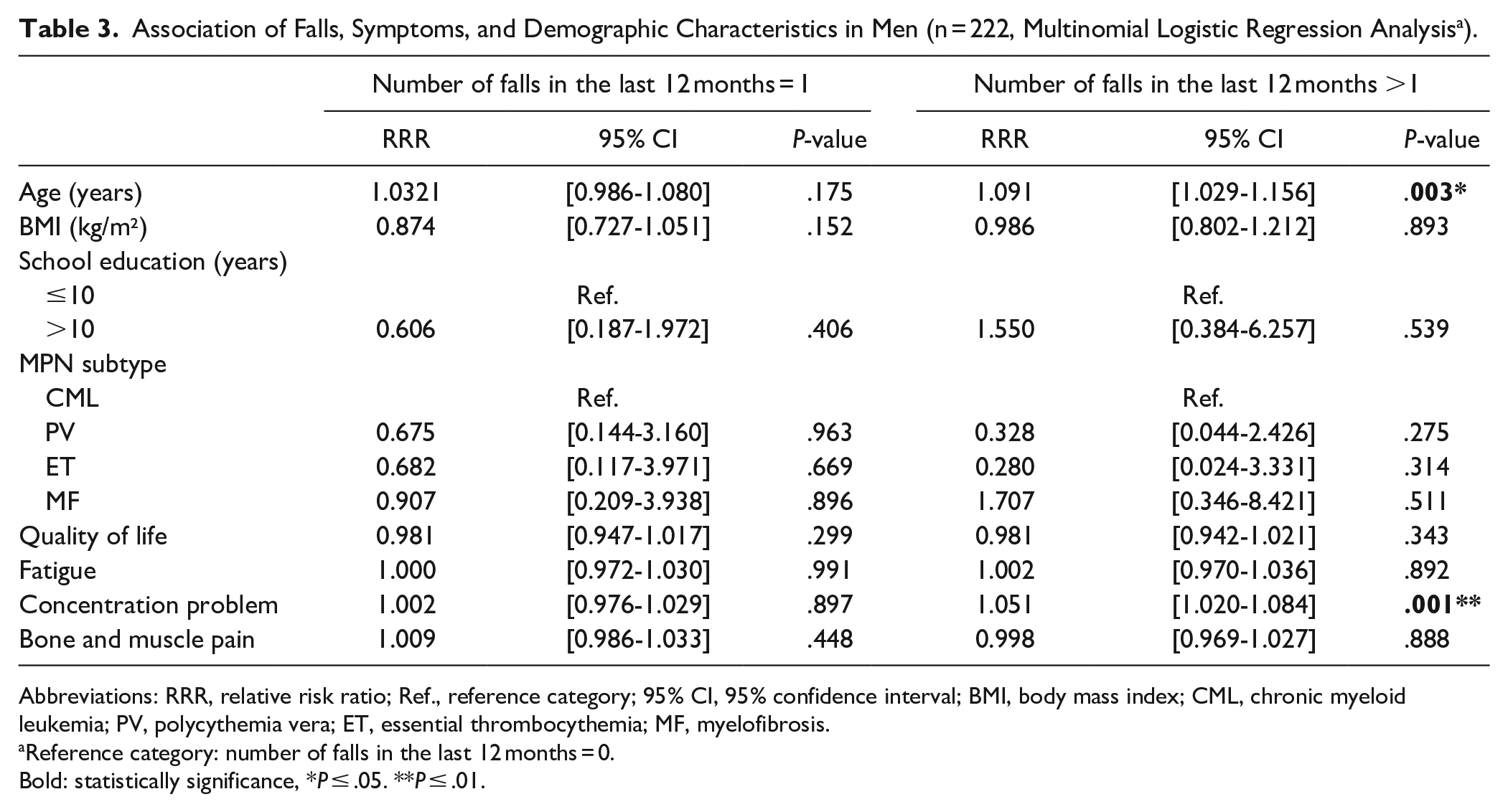
Abbreviations: RRR, relative risk ratio; Ref., reference category; 95% CI, 95% confidence interval; BMI, body mass index; CML, chronic myeloid leukemia; PV, polycythemia vera; ET, essential thrombocythemia; MF, myelofibrosis.
Reference category: number of falls in the last 12 months = 0.
Bold: statistically significance, *P ≤ .05. **P ≤ .01.
Correlation Between DTrSEs, Age, BMI, and QoL
Men rated their QoL significantly higher than women (72 ± 21 vs 64 ± 22, P < .001). In all DTrSEs, women showed more discomfort compared to men (Table 1). The highest correlation was found between CrF and inactivity and between CrF and concentration problems in both genders. Age and BMI showed no or weak correlations with QoL and DTrSEs in both genders (Table 4).
Spearman Correlation Analysis Between Age, BMI, QoL, and Side Effects For Women (n = 432, Pink) and Men (n = 254, Blue).

Abbreviations: BMI, body mass index; QoL, quality of life.
Bold: strong correlation (r > |.50|). *P ≤ .05. **P ≤ .01.
Discussion
Main Findings
CrF and falls seems to be very common in MPN patients. The prevalence of moderate to severe CrF was 55% in our sample, and the prevalence of at least 1 fall within the last 12 months was 15%. Further, the occurrence of falling was associated with CrF in women but not in men.
Comparison of the Main Findings With Other Studies
The high prevalence of CrF, which is often reported in combination with symptoms of inactivity, concentration problems, and bone and muscle pain, has already been described in patients with MPN.11-13
The retrospectively reported prevalence of falls at 16.2% for women and 12.2% for men was lower than reported by prospective as well as retrospective studies, which reported prevalence rates between 19% and 35%.2,4,13 There are several explanations for these differences. Firstly, our study group was restricted to patients with hematological neoplasms. In contrast, the proportion of solid tumors in comparable studies was 81% 14 and 100%, 4 respectively. Second, age, particularly age-related changes, are important predictors of falls.15,16 The median age of participants in our study was 57 years, differing from those of other studies.4,2,14 For example, Spoelstra et al 2 and Puts et al 14 included only participants ≥ 65 years in their studies. Third, the proportion of women in this study (62%) was much lower than in the studies of Puts et al 14 and Basal et al 4 (70% and 100%). This might be relevant because women tend to experience more falls than men.15-18
Implication and Explanation of Findings
Our data indicates a direct association between CrF and falls among female study participants. As concentration problems are among the most reported symptoms of CrF, 8 there might be an indirect association in men.
MPNs are chronic diseases. Consequently, MPN patients are burdened with symptoms throughout their lives. Patients included in the study had had their diagnoses for an average of 7.5 years. We assume that MPN patients with moderate to severe CrF are less physically active than healthy individuals or cancer patients without CrF of the same age. The reason for this is that CrF is a barrier to physical activity, 19 which was confirmed by the results of our correlational analyses, with increasing inactivity, a decline in physical performance and consequently a loss of muscle mass and strength,20,21 as well as a reduction in coordination skills, including balance. 22 As a result, the risk for falls increases.23-25
Another possible explanation is that, as a result of physical inactivity, MPN patients, similar to older people, experience neurological deterioration. This is often characterized by a decrease in cognitive performance, such as slower processing and problem-solving speed. This also affects movement, especially when movements are performed simultaneously with cognitive tasks, under so-called dual-task conditions. A certain amount of dual-task interference occurs. The possible changes in muscle activity and balance that occur lead to movement uncertainty and can be explained by a reduction in attention to the movement request.23,26, 27
Strengths and Study Limitations
To our knowledge our study presents the largest cohort to date in which the association between CrF and falls has been studied. Nevertheless, our study has a number of limitations. First, we do not have any information on how many patients were asked to participate in the survey and declined to participate, which may have led to selection bias among the sample. Second, all data were assessed retrospectively. Third, in order to reduce the length of the questionnaire, a VAS scale from 0 to 100 was used for the assessment of QoL, rather than a validated questionnaire. Since a VAS allows a more differentiated assessment of QoL compared to a Likert scale, it can be assumed that the QoL of cancer patients was measured just as adequately. 28 Fourth, other diseases associated with gait impairments (e.g. Parkinson’s disease, stroke, and polyneuropathy) were not recorded. Fifth, the use of BMI does not allow any conclusions about muscle mass or muscle strength. Sixth, we assume a bias towards more women and younger patients due to the high proportion of online questionnaires. In order to verify the results of this study, these data should be assessed in future studies.
Conclusion, Recommendation, and Outlook
More than half of MPN patients suffer from moderate to severe CrF. Falls are a common phenomenon in MPN patients. More than 1 in 10 of our patients reported at least 1 fall within the last 12 months. Women seem to be more susceptible to falling than men. The association between CrF and occurrence of a fall was significant in women but not in men. It seems that MPN patients who suffer from moderate to severe CrF may be more susceptible to falls.
Due to the rather young age of our patient cohort compared to the participants in other studies, it might be reasonable to assume that the risk of falls also increases with age in this cohort. For this reason, fall prevention strategies should be implemented early in MPN patients at increased risk. Physicians should evaluate and manage CrF, regardless of the patient’s age. To date, physical activity, psychotherapy, or a combination of both are effective measures to reduce CrF. 29
Further research is needed to understand the effects of CrF on gait performance, particularly under dual-task conditions, and the associated fall risk. Moreover, it has recently been shown that the execution of a fatiguing cognitive task impaired dual-task gait performance in older adults and that this effect might be exacerbated in MPN patients depending on the level of CrF. 26
While we examined the association between CrF and more than 1 fall in the last 12 months, it may also be useful to examine the exact number of falls patients have had to determine whether CrF correlates with the number of falls. The results may provide clues to possible preventive measures to maintain mobility in affected patients, which is related to QoL. 30
Since CrF also has a high prevalence in other entities, 7 subsequent studies should investigate whether the results can be transferred to other cohorts. It should be taken into account that it is not only cancer patients undergoing chemotherapy and/or radiotherapy or advanced stage that are frequently affected by CrF, but also patients in follow-up. For example, Wang et al 31 observed a prevalence of 29% for moderate to severe CrF in survivors of breast, prostate, colorectal, or lung cancer.
Supplemental Material
sj-doc-1-ict-10.1177_15347354221143064 – Supplemental material for Association Between Cancer-Related Fatigue and Falls in Patients With Myeloproliferative Neoplasms: Results of a Multicenter Cross-Sectional Survey From the East German Study Group for Hematology and Oncology (OSHO #97)
Supplemental material, sj-doc-1-ict-10.1177_15347354221143064 for Association Between Cancer-Related Fatigue and Falls in Patients With Myeloproliferative Neoplasms: Results of a Multicenter Cross-Sectional Survey From the East German Study Group for Hematology and Oncology (OSHO #97) by Sabine Felser, Martin Gube, Julia Gruen, Philipp Ie Coutre, Susann Schulze, Lars-Olof Muegge, Christian Junghanss and Sabina Ulbricht in Integrative Cancer Therapies
Footnotes
Acknowledgements
This work was supported by the non-profit associations LeukaNET/Leukaemia-Online and the German, Austrian, and Swiss MPN Network.
Author Contributions
SF, CJ, and SU conceived the study idea and analysis plan. JG, PlC, SS, LOM, and CJ collected and organized the data. SU led on the analysis with input from SF and MG. SF, MG, and SU undertook data interpretation. SF and SU drafted the manuscript. All authors read and commented on the draft manuscript, and all authors approved the final submitted version.
Data Availability Statement
The data that support the findings of this study area available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the East German Study Group Hematology and Oncology (OSHO#97).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.