
Abstract
Background:
Yoga is an evidence-based mind-body practice known to improve physical and mental health in cancer patients. We report on the processes and patient-reported outcomes of one-on-one yoga therapy (YT) consultations delivered via telehealth.
Methods:
For patients completing a YT consultation between March 2020 and October 2021, we examined demographics, reasons for referral, and self-reported symptom burden before and after one YT session using the Edmonton Symptom Assessment Scale (ESAS). Changes in ESAS symptom and subscale scores [physical distress (PHS), psychological distress (PSS), and global distress (GDS)] were evaluated by Wilcoxon signed-rank test. Descriptive statistics summarized the data.
Results:
Ninety-seven initial YT consults were completed, with data evaluated for 95 patient encounters. The majority were women (83.2%) and white (75.8%), The mean age for females was 54.0 and for males was 53.4; the most common diagnosis was breast cancer (48%), 32.6% had metastatic disease, and nearly half (48.4%) were employed full-time. Mental health (43.0%) was the most common reason for referral, followed by fatigue (13.2%) and sleep disturbances (11.7%). The highest symptoms at baseline were sleep disturbance (4.3), followed by anxiety (3.7) and fatigue (3.5). YT lead to clinically and statistically significant reductions in PHS (mean change = −3.1, P < .001) and GDS (mean change = −5.1, P < .001) and significant reductions in PSS (mean change = −1.6, P < .001). Examination of specific symptom scores revealed clinically and statistically significant reductions in anxiety (mean change score −1.34, P < .001) and fatigue (mean change score −1.22, P < .001). Exploratory analyses of patients scoring ≥1 for specific symptoms pre-YT revealed clinically and statistically significant improvements in almost all symptoms and those scoring ≥4 pre-YT.
Conclusions:
As part of an integrative oncology outpatient consultation service, a single YT intervention delivered via telehealth contributed to a significant improvement in global, physical, and psychosocial distress. Additional research is warranted to explore the long-term sustainability of the improvement in symptoms.
Keywords
Introduction
A cancer diagnosis and the ensuing treatment-related adverse effects can negatively affect patients’ quality of life. Patients often turn to complementary health approaches to manage cancer-related physical and psychosocial distress. 1 These approaches include music therapy, massage therapy, acupuncture, yoga, and other mind and body practices, as well as nutrition, physical activity, and herbs and supplements combined with conventional cancer care. In the general United States population, the use of yoga increased from 9.5% to 14.3%, and the use of meditation increased from 4.1% to 14.2% between 2012 and 2017.2,3 There is growing interest in yoga as a mind and body approach, especially among cancer patients. 4 Originating from India, yoga incorporates asanas (physical postures), pranayama (controlled breathing), relaxation, and meditation, which are easily adaptable to meet individual needs.5,6
Yoga can be used throughout the cancer experience from diagnosis to survivorship as well as alongside end-of-life care. 7 The increase in the utilization of yoga is due to the increased understanding of how chronic stress leads to worse cancer outcomes and the extensive evidence suggesting that yoga improves the quality of life, physiologic outcomes, and biological processes.8-10 A review of 29 clinical trials found that low-intensity forms of yoga, specifically gentle Hatha and restorative yoga, are safe and effective for relieving sleep disruption, nausea, fatigue, pain, psychosocial distress, and musculoskeletal symptoms. 11 Yoga may also reduce cognitive impairment associated with cancer treatment. 12 Yoga has been associated with decreased cortisol response, increased cell-mediated immunity, and decreased pro-inflammatory biomarkers.13-15 The National Comprehensive Cancer Network (NCCN) has endorsed yoga in managing cancer-related fatigue and anticipatory nausea/vomiting and suggests “considering” yoga for distress (anxiety/depression/trauma), pain, cognitive function, and menopausal symptoms.16,17 According to the joint Society for Integrative Oncology (SIO) and American Society of Clinical Oncology (ASCO) guidelines for the use of integrative therapies during and after breast cancer treatment, yoga is recommended for reducing anxiety and improving quality of life, mood, symptoms of depression, fatigue, and sleep disturbance. 18
Despite the strong evidence base and inclusion in several symptom control clinical practice guidelines, yoga is not part of routine clinical practice at many cancer centers. The extensive research on the benefits of yoga in cancer exists predominantly in the clinical trial setting9,19 or examining group program effectiveness.20,21 Yet there is limited real-world data on the delivery of yoga and no reports on the provision of one-on-one yoga integrated alongside conventional cancer care. At the University of Texas MD Anderson Cancer Center, yoga therapy (YT) is available to patients and caregivers through the Integrative Medicine Center in inpatient and outpatient settings.
During COVID-19 restrictions, many yoga classes transitioned to telemedicine, yet there remain few published reports.21-24 Among these, 2 studies transitioned from in-person to online intervention delivery during COVID-1922,23 and a third study offered a variety of mind-body sessions to support psychological coping. 24 All these studies were conducted in group or dyad setups and found virtual yoga delivery acceptable and beneficial during COVID-19 social distancing restrictions. There are no studies reporting one-on-one yoga via telehealth in cancer populations during COVID-19.
At MD Anderson YT is provided by a yoga therapist and is available in group programs as well as one-on-one consultations. We previously reported on the benefits of YT group programs. 20 Our current study examined the clinical application of a one-on-one outpatient YT consultation delivered via telemedicine during the early stages of the COVID-19 pandemic as part of routine care. The primary aim of this study was to describe the processes and demographic and clinical characteristics of patients presenting for an outpatient YT consultation. The secondary aim was to describe the reasons for the referral and the short-term changes from before to after the YT intervention.
Methods
We conducted a retrospective analysis of cancer patients seen for yoga therapy (YT) between March 1, 2020, and October 30, 2021, in an Integrative Medicine Center within a large comprehensive cancer center. Consecutive patients being seen for their first outpatient YT consultation were asked to complete a series of assessments as part of the standard of care. Only patients ≥18 years of age and with a cancer diagnosis were eligible for the review. Patients with missing data and non-cancer diagnoses were excluded. Data were stored in a secure, Health Insurance Portability and Accountability compliant, FileMaker Pro database as part of an IRB-approved protocol (DR11.0149). As a part of the initial evaluation for YT, patients completed the modified Edmonton Symptom Assessment Scale (mESAS) both before and after the YT session.
Intervention
Patients referred to the Integrative Medicine Center are first evaluated by an integrative oncology physician to guide development of an integrative oncology care plan. An integrative care plan may consist of YT for patients to integrate before, during, and/or after cancer treatment. A referral for YT may be placed by integrative medicine providers, including physicians, advanced practice providers, or health psychologists. The reasons for referral are listed as orders in electronic medical records, and multiple reasons can be selected by the providers. The referral reasons to choose from are: insomnia, fatigue, anxiety, stress reduction, mood disturbances, depression, nausea, quality of life, dyad/couple practices, help modifying an existing Yoga practice, or “other referral reasons/comments.” In addition, patients were referred if they did not have a prior yoga practice. A certified yoga therapist with over 10 years’ experience with specialized training in an oncology setting provided the YT interventions.
The International Association of Yoga Therapists defines YT as: “the process of empowering individuals to progress toward improved health and well-being through the application of the teachings and practices of Yoga.” 25 Critical differences between yoga teachers and yoga therapists are training and session goals. While yoga is a healthy pursuit that can benefit its practitioners in its general form, YT is used to help treat a specific condition or symptom. Yoga therapists also have more extensive training than yoga teachers. A formal yoga teacher training in the US requires a 200-hour certification, while YT certification requires an additional 800 hours of training (1000 hours total) or a master to a doctoral-level degree in YT. While a yoga teacher’s goals focus on teaching the techniques, a yoga therapist focuses on applying specific practices to help clients or patients treat a certain condition or symptom(s). Yoga therapists are also qualified to assess an individual’s need for YT and create a yoga practice list considering the safety precautions and contraindications to improve their overall well-being. 26 YT is typically taught one-on-one or in small groups.
Prior to the consultation, the YT reviewed the patient’s medical record to determine: the cancer stage, past and ongoing cancer treatments, cancer-related symptom burden, physical limitations, prior yoga experience, mental health, mESAS scores, notes, and PROs from the integrative medicine consultation. The actual YT consultation, which lasts for an hour, focuses on counseling patients using specific yoga techniques for their situation and teaches the actual yoga poses/techniques. The YT consultation included approximately 45 minutes of actually practicing yoga postures, breathing exercises, and meditation. The patients were also provided recordings for independent home practice; no prior yoga experience was necessary. Each session may have one or more goals, such as anxiety reduction, fatigue management, relaxation, pain reduction, or overall mood improvement. The YT guided the patients on the appropriate practices for their unique symptom profiles, medical condition, and goals. For example, guided yogic relaxation would be introduced and recommended before bedtime to help with sleep disturbances. Due to the COVID-19 pandemic, all YT consultations were delivered via a Zoom online portal integrated into the hospital’s electronic health system. Patients joined the sessions through the MyChart health record port using phones, tablets, or computers.
As this is a retrospective study of an individualized YT clinical service, there was no pre-defined set of yoga practices. Instead, the yoga therapist provided practices based on the evidence and per the needs of the individual patient. The main components of the YT program included joint loosening and gentle stretching (Sukshma Vyayama), postures (Asana), breath energization (Pranayama), relaxation techniques (Yoga Nidra), and meditation (Dharana, Dhyana) practices.6,27 A detailed description of these practices is included in Supplemental Material A. Modifications were done using a chair, cushion, or blanket that a patient can easily find at home. Along with physical yoga techniques such as asanas, patients were coached on connecting with self and mindfulness in daily living. Written instructions were given to help patients with independent practice after the sessions.
Measures
We collected data on consecutive patients evaluated by a yoga therapist as part of an integrative medicine outpatient consultation service. Data extracted from the patient medical record included demographics, cancer diagnosis, and reasons for referral as documented by the referring integrative oncology physician and advanced practice provider. YT data was collected in a database as an IRB-approved protocol.
Modified Edmonton Symptom Assessment Scale (mESAS)
Patients completed the mESAS28-31 as part of the routine PRO (patient reported outcomes) both before and after the YT session. The ESAS measures symptom burden using self-reported responses and has a reported Cronbach alpha of 0.79. 32 Patients reported on 16 items: 10 core symptoms including pain, fatigue, nausea, depression, anxiety, drowsiness, loss of appetite, sense of well-being, shortness of breath, and sleep, and an additional 6 items: spiritual distress, financial distress, numbness/tingling, hot flashes, dry mouth, and memory, as experienced in the last 24 hours.
Responses were on a numeric scale of 0 to 10, with 0 indicating no symptom or best and 10 indicating worst symptom burden. Generally, ESAS scores of 1 to 3 are considered mild, 4 to 6 as moderate, and 7 to 10 as severe in clinical practice. 33 Based on this categorization, a symptom score of ≥4 represents a clinically significant level of the symptom.
The mESAS also included the following subscales: Global distress score (GDS, range: 0-90) sum of pain, fatigue, nausea, drowsiness, appetite, shortness of breath, anxiety, depression, and well-being scores; Physical distress score (PHS, range: 0-60) sum of pain, fatigue, nausea, drowsiness, appetite, and shortness of breath; Psychological distress score (PSS, range: 0-20) sum of anxiety and depression. A change in GDS and PHS of ≥3 and PSS ≥ 2, and individual symptoms scores of ≥1 indicates a clinically meaningful changes. 34
Statistical Analyses
Descriptive statistics were used to summarize the demographic and clinical characteristics of the patients. Reasons for referral were evaluated, summed, and percentages presented. Percentages could add up to more than 100% because some respondents reported more than one referral reason. mESAS scores were summarized with means and standard deviations calculated. Wilcoxon signed-rank t-tests 35 was used to compare mESAS post-session to pre-session scores. In order to adjust for multiple comparisons of the mESAS individual items, a P-value of ≤.003 was considered statistically significant for the primary outcome analyses. Exploratory analyses examined the subset of patients reporting mESAS individual symptom scores ≥ 1 and ≥ 4 before YT. The statistical analyses were performed using SPSS version 24 and Microsoft Excel for Office 365 MSO.
Results
Figure 1 describes the flow of participation in the study. A total of 208 patients were referred for YT outpatient consultation between March 1, 2020, and October 30, 2021, of which 116 visits were scheduled. Of the 116 patients, 15 canceled, and 4 did not show up for their appointment. We included 95 out of 97 unique patients who completed the YT consultation (2 declined completing the mESAS measure).

CONSORT diagram showing the study flow and the total number of patients included in the final analysis.
Table 1 summarizes the demographic and clinical characteristics of patients. The majority, 83.2%, were women, white 75.8%, and nearly half (48.4%) were employed full-time. The mean age for females was 54.0 and for males was 53.4, with the most common diagnosis being breast cancer (48%) and 32.6% having metastatic disease. The patients were in various stages of cancer treatment (undergoing treatment or completed treatment). None of the patients had a prior active yoga practice.
Demographic and Medical Characteristics of Patients Presenting for Ambulatory Yoga Therapy Consultation.

Table 2 summarizes reasons for YT referral by integrative oncology providers. The most common reason for referral was mental health (47.9%; stress, anxiety, depression, lack of relaxation, and adjustment disorder). Next was fatigue (13.2%), sleep disturbances (11.7%), to adapt/modify prior yoga practice (9.8%), nausea (4.9%), lack of physical exercise (4.2%), dyad/caregiver practice (3.8%; however, all patients attended alone) and other reasons (4.5%) consisting of pain, appetite, and decreased libido.
Reasons for Referral to Yoga Therapy.

The sum of N is greater than the number of evaluable patients (95) as there was often more than one reason for referral. For example, a patient could be referred for fatigue and pain.
Other reasons included pain, appetite, and decreased libido.
Table 3 shows the results of the mESAS before and the average change in scores after the YT intervention among all patients, as well as among patients with mESAS ≥ 1 at baseline for that particular symptom. Change scores indicated both clinically and statistically significant reductions in anxiety (mean change score = −1.34, P < .001), fatigue (mean change score = −1.22, P < .001), PHS (mean change score = −3.11, P < .001), and GDS (mean change score = −5.14, P < .001). Statistically significant reductions were also observed for pain (mean change score = −0.90, P < .001) and PSS (mean change score = −1.6, P < .001). In the subgroup analyses of patients with ESAS ≥ 1 for a particular symptom, we observed statistically and clinically significant reductions for most symptoms, and for PSS, PHS, and GDS. The largest symptom reductions were seen for anxiety, drowsiness, fatigue, and pain.
Symptom Burden Before and Changes After Yoga Therapy.
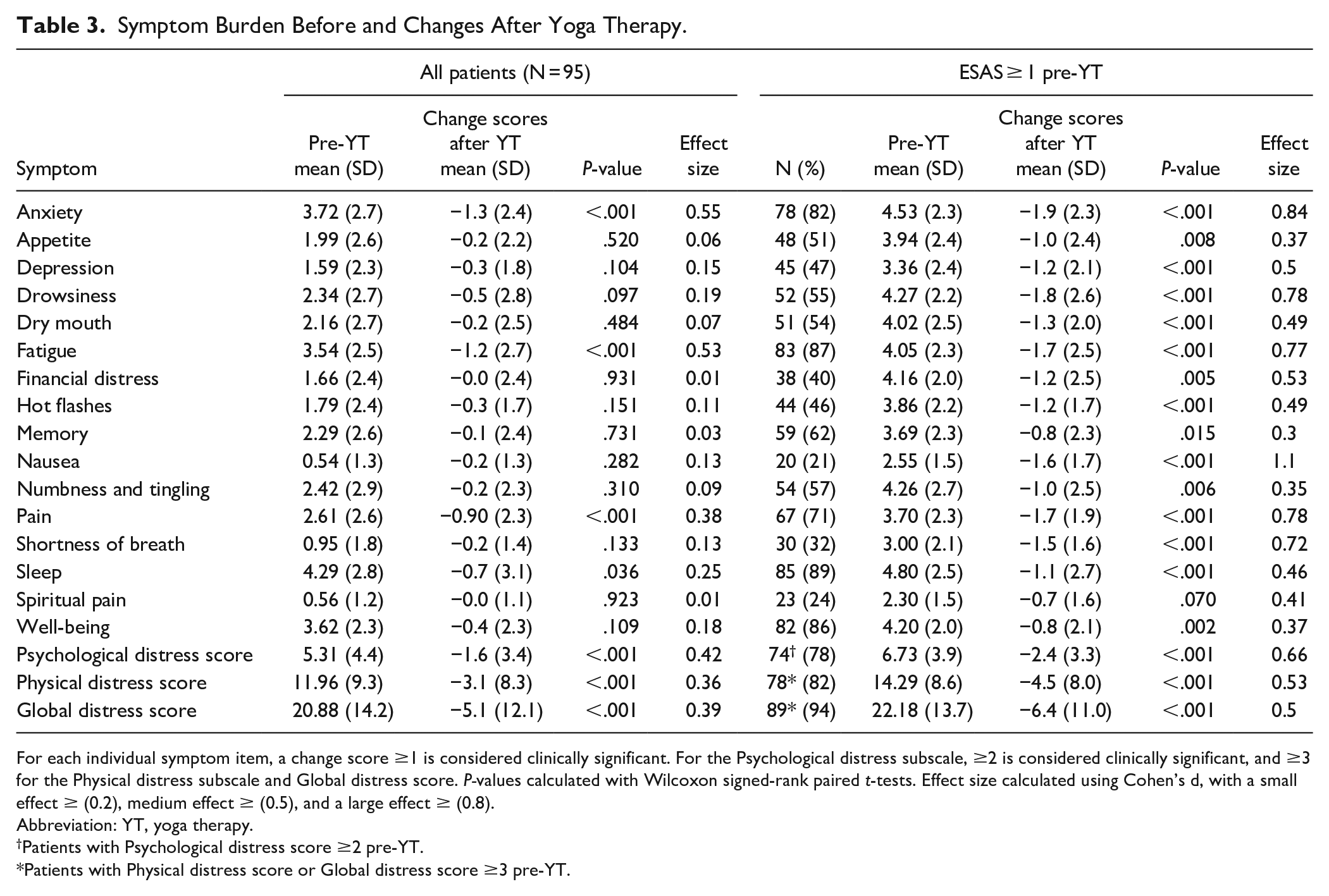
For each individual symptom item, a change score ≥1 is considered clinically significant. For the Psychological distress subscale, ≥2 is considered clinically significant, and ≥3 for the Physical distress subscale and Global distress score. P-values calculated with Wilcoxon signed-rank paired t-tests. Effect size calculated using Cohen’s d, with a small effect ≥ (0.2), medium effect ≥ (0.5), and a large effect ≥ (0.8).
Abbreviation: YT, yoga therapy.
Patients with Psychological distress score ≥2 pre-YT.
Patients with Physical distress score or Global distress score ≥3 pre-YT.
We also examined the subset of patients reporting ≥4 on individual ESAS symptoms at baseline, a level regarded as a clinically significant level of symptoms. The number of patients experiencing ≥4 on an individual symptom varied, with only 5 participants experiencing ≥4 for nausea and spiritual pain and N = 49 reporting ≥4 for anxiety. Figure 2 shows the means before YT and post-YT for each individual symptom where there were 10 or more patients reporting ≥4 before YT (all symptoms except nausea and spiritual pain). Reductions (improvement) in all symptoms were clinically significant and reached statistically significant for 8 of 14 symptoms (P ≤ .003). The greatest mean score reductions were observed for fatigue (change score = −2.93, P < .001), pain (change score = −2.73, P < .001), and anxiety (change score = −2.63, P < .001). The magnitude of reduction is symptoms is notably higher (range 2-4) in patients reporting moderate to severe symptom burden at baseline (symptom scores ≥4) than that of patients reporting symptom scores ≥1 at baseline (range 1-3).

Patients with ESAS ≥ 4 symptom burden on individual items at baseline: mean ESAS scores before and after yoga therapy and effective size estimates.
There were no yoga intervention-related adverse events reported. There were also no issues related to the telemedicine session delivery, as patients had consented to the remote delivery and were aware of the requirements of device and internet connectivity for the same. This could be because patients were referred to the yoga therapist after the physician consultation and screening to determine suitability.
Discussion
Our study describes the characteristics of the patients attending outpatient telemedicine YT. This retrospective study provides insight into the safety and feasibility, of individualized YT for cancer patients in an ambulatory setting at a comprehensive cancer center. This study suggests that it was feasible to provide YT online during the COVID-19 pandemic. Mental health (stress, anxiety, depression, lack of relaxation, and adjustment disorder) was the top reason for referral followed by fatigue and sleep. We observed statistically and clinically significant improvement across multiple symptoms commonly experienced by cancer patients with just one session of personalized YT. Importantly, improvements were seen across multiple domains including in physical health, mental health, and global distress scores. As we expected, the benefits were more pronounced for patients with worse symptom distress before the YT session. In particular, we found the greatest improvements for pain, fatigue, and anxiety. This is consistent with to previous studies in the breast cancer populations, where yoga interventions showed significant improvement in fatigue,36,37 and another study in breast cancer patients showing reductions in anxiety. 13 Improvements in psychological and physical health align with prior literature on the benefits of yoga in improving quality of life in cancer patients.11,19,36-40 Compared to the patients attending a single group yoga session, 20 patients in this study reported slightly higher symptom burden at baseline for anxiety, fatigue, pain, PSS, PHS and GDS. There was also a higher magnitude of change post YT session, suggesting greater benefit for one-on-one telemedicine sessions versus group for those reporting a symptom burden of ≥1 on ESAS scores. However, future research should examine a more direct comparison of the different delivery formats.
A strength of this real-world study is that the yoga therapist developed a personalized treatment plan to address individual patients’ unique needs. This individual one-on-one attention is not feasible in group yoga sessions. There was also no set standard protocol which might limit the type of yoga techniques taught as in a clinical trial. This gives an opportunity to adapt the practice and meet individual patient needs. We also found that it is feasible to provide YT via telehealth, which can help cancer patients with limited access to YT services living in remote areas.
There are several limitations to this study. The changes from pre- to post-yoga sessions should be interpreted with caution as the effects are likely short-term unless the patients continue their practice with the materials provided. However, creating some symptom relief even in the short-term is a worthy outcome. Our sample also does not have an active attention control group. This is more relevant as cancer patients were socially isolated during the COVID-19 pandemic and the individual attention might have led to improvement in the symptom scores post-session. However, the main purpose of the trial was to document the real-world application of YT alongside cancer care and not to determine efficacy using a conventional RCT approach. We also did not specifically examine the effects of COVID-19 per se. However, a previous publication that examined patients having integrative oncology consultations before and during COVID-19 found no differences in ESAS symptom scores. 41 The patient population was also a convenience sample of patients attending integrative oncology consultation within a comprehensive cancer center and those who followed through on the referral for YT. In addition, of the over 200 patients referred to yoga therapy, only 97 had an actual YT session. Therefore, it may not represent the larger population of cancer patients. The patient’s prior interest in yoga could have aided in the yoga intervention experience, though prior exposure to yoga was only 10%. Administration of intervention via telehealth has its limitations in the selection bias of participants. Patients with barriers such as poor or no internet connection, lack of experience in using the technology, advanced age, and hearing limitations may not have participated. Health disparities and technology barriers need to be considered in future planning of yoga implementation programs in cancer centers.
Conclusions and Future Directions
This study suggests that it was feasible to provide YT online during the COVID-19 pandemic. YT consultations delivered one-on-one by an experienced yoga therapist significantly reduced physical and psychological distress and improved cancer-related symptoms like anxiety, fatigue, and pain. YT was especially beneficial for individuals with moderate to severe symptom burden, suggesting a wide range of patients who can be appropriately referred. Findings from the real-world analyses can help inform clinical practice and the design of future research. Based on our data, we encourage patients and cancer health care providers to incorporate YT to manage cancer-related symptoms. Challenges remain in having access to yoga therapists with proper training to work with individuals affected by cancer. Future research should focus on longitudinal data collection to assess long term effectiveness of YT in cancer care and examine the results based on different demographic and clinical characteristics.
Supplemental Material
sj-docx-1-ict-10.1177_15347354221141094 – Supplemental material for Yoga Therapy in Cancer Care via Telehealth During the COVID-19 Pandemic
Supplemental material, sj-docx-1-ict-10.1177_15347354221141094 for Yoga Therapy in Cancer Care via Telehealth During the COVID-19 Pandemic by Smitha Mallaiah, Santhosshi Narayanan, Richard Wagner, Chiara Cohen, Aimee J. Christie, Eduardo Bruera, Gabriel Lopez and Lorenzo Cohen in Integrative Cancer Therapies
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by the National Institutes of Health through MD Anderson’s Cancer Center Support Grant CA016672, a grant from the Duncan Family Institute for Cancer Prevention and Risk Assessment, and the Richard E. Haynes Distinguished Professorship for Clinical Cancer Prevention at The University of Texas MD Anderson Cancer Center (L Cohen).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.