
Abstract
Introduction
Weight gain after breast cancer is common, and obesity after breast cancer increases breast cancer recurrence and mortality. Mindfulness-based interventions (MBIs) and yoga have been shown to be effective in managing obesity/overweight in people without breast cancer. There is a need to systematically map the extent and range of evidence on yoga and MBIs for managing obesity/overweight after breast cancer in order to aid planning and commissioning of future research.
Methods
We conducted a scoping review informed by methods described by Levac et al. Five electronic databases were searched for any peer-reviewed original research (including systematic reviews) that examined the role of yoga and/or MBIs for managing overweight/obesity after breast cancer. Data were extracted on study, population, intervention, comparator and outcome characteristics, and described narratively.
Results:
We found 18 publications representing 15 unique studies (11 clinical trials, 2 systematic reviews, and 2 observational studies). There were 10 studies on yoga, and 5 on MBIs. Of the clinical trials, only 4/11 examined a weight-related outcome as the primary outcome. The remaining trials examined lifestyle or metabolic outcomes (5/11) or unrelated outcomes such as psychological health (2/11). Gaps in the literature included small sample sizes, lack of cultural diversity amongst participants, inadequate reporting of the intervention, few lifestyle co-interventions offered, lack of active comparator groups, and inadequate safety reporting.
Conclusions:
There is a need for adequately-powered RCTs that adhere to reporting guidelines. The use of gold-standard methods for measuring outcomes, and active comparator groups, is also recommended.
Introduction
Among females, breast cancer is the most commonly diagnosed cancer worldwide at all ages, with 2.3 million cases diagnosed in 2020. 1 Cases are predicted to grow to 3.19M in 2040. 2 With increased detection and treatment, the population of breast survivors is increasing. 3
Concurrently, there has been an increase in rates of overweight and obesity in the general population (defined by World Health Organization (WHO) as having a body mass index (BMI) over 25 kg/m2 and over 30 kg/m2 respectively). 4 It is estimated that more than half of the world’s population was overweight (39%) or obese (13%) in 2016. 4 In Western countries, the prevalence of obesity alone is even higher, for example, 42% of people in the USA were obese in 2017-18. 5
Additionally, weight gain after breast cancer diagnosis and treatment has been reported by numerous studies.6-8 Weight gain after breast cancer is multifactorial, attributable to factors such as systemic therapies and changes in lifestyle.6,9 Studies suggest that obesity at diagnosis leads to a 35% to 40% increased risk of breast cancer recurrence and mortality while weight gain of more than 10% after diagnosis increases all-cause mortality. 10 This is also seen in a 2014 meta-analyses of 82 studies which found for each 5 kg/m2 increment of BMI before, <12 months after, and ≥12 months after diagnosis, increased risks of 17%, 11%, and 8% for total mortality, and 18%, 14%, and 29% for breast cancer mortality were observed, demonstrating how obesity/overweight at time of diagnosis or thereafter leads to poorer outcomes. 11 Moreover weight gain after breast cancer may increase body image distress. 12
Although multimodal interventions incorporating diet, exercise and psychosocial support are effective in reducing body weight in breast cancer survivors, 13 there is evidence that few women are able to maintain regular physical activity in the long term after breast cancer treatment14,15 and face significant barriers to adopting and maintaining healthy lifestyles. 16 Therefore, there is a compelling need to identify effective interventions for managing obesity and overweight amongst females with breast cancer in order to optimize health outcomes. Complementary therapies are widely used by women with breast cancer around the world17-21 with prevalence of use as high as 100% in one small cross-sectional study (n = 85) in Saudi Arabia. 22 Frequently used interventions include dietary supplements, 17 and mind-body therapies.18,19 In one cohort study of women with breast cancer, 64% used mind-body therapies (including yoga and meditation). 23 There is evidence that mindfulness-based interventions24,25 and yoga26,27 may be effective for managing obesity/overweight in people without breast cancer.
Mindfulness-based interventions (MBIs) are a type of meditation-based practice originating from Buddhist philosophy. 28 Mindfulness is defined as “awareness of one’s internal states and surroundings.” 29 Mindfulness-based interventions include but are not limited to the standardized 8-week Mindfulness-Based Stress Reduction (MBSR) program developed by Jon Kabat–Zinn in the 1970s, 30 Mindfulness-Based Cognitive Therapy program (MBCT) developed by Segal, Williams and John Teasdale which is an adaptation of MBSR 31 and others beyond these standardized programs. 32 MBIs have been demonstrated to increase quality of life,33,34 improve mental health35,36 and reduce stress and anxiety33,37 in breast cancer survivors.
Yoga is a mind-body therapy that originated in India and has been practiced for over 5000 years. 38 The word yoga is literally defined as “joining of body and mind.” 39 There are several schools/styles of yoga practiced world-wide. 40 Practice of yoga involves various components such as breathing techniques, physical postures, and meditation. 41 According to a recent survey study, more than 60% of breast cancer survivors reported using yoga during and/or after their cancer diagnosis. 42 Yoga was perceived to help reduce various symptoms such as breast/chest wall pain and anxiety, joint pain, muscle pain, fatigue, headache, hot flashes, nausea/vomiting, depression, insomnia, lymphedema, peripheral neuropathy, and improve quality of life. 42 Systematic reviews of RCTs have demonstrated the effectiveness of yoga interventions in reducing distress, anxiety and depression, and fatigue, improving emotional wellbeing, while increasing quality of life among breast cancer survivors.43-47 A meta-analysis of RCTs found that yoga can help improve cancer-related fatigue (18 studies) and quality of life (10 studies) compared to non-physical activity. 48
Yoga and MBIs may be potentially effective for managing obesity/overweight after breast cancer, given the promising evidence from non-breast cancer populations. However, there is a paucity of clinical trials exploring the effect of MBIs and yoga on weight management and loss. We conducted a scoping review, based on that described by Levac et al, 49 to systematically map the extent and range of evidence, synthesize findings, and identify gaps in the literature specifically focused on MBIs and yoga for weight gain prevention, weight loss, body recomposition and weight maintenance for women with breast cancer, in order to aid planning and commissioning of future research. We chose to focus on MBIs and yoga because of the relatively high prevalence of use in breast cancer survivors, and the evidence for effectiveness for managing overweight/obesity in the general population. Additionally, both yoga and MBIs to a group of therapies often referred to as mind-body therapies 50 or contemplative practices, 51 involving the cultivation of interoceptive awareness through attention to body sensations or areas of the body. Mindfulness-based interventions may include yoga as a component, and the practice of yoga includes meditation components. Last, research on yoga and MBIs has grown significantly over the last 2 decades and they are among the most well-researched mind-body therapies. 51 Therefore, we proceeded to explore the body of research that has been conducted on both these interventions concurrently in order to inform future research in the field of managing overweight/obesity after breast cancer.
Methods
The aims of this scoping review were to:
➢ Systematically map the extent and range of evidence on mindfulness-based interventions and yoga for managing obesity/overweight after breast cancer according to type of study and year of publication, population, type of MBI and yoga, and outcomes collected
➢ Identify gaps in the literature to aid planning and commissioning of future research.
The research questions were: (1) What is the type, extent and range of research on MBI and yoga for managing obesity/overweight after breast cancer? and (2) What are the gaps in the literature? This was explored through analysis of number of studies, study design, year of publication, sample characteristics, type of MBI and yoga, and study outcomes.
Study Design
Scoping reviews examine the extent, range and nature of evidence of broad or emerging research areas. They can summarize findings, identify gaps and act as a precursor to systematic reviews in order to aid planning and commissioning of future research.49,52,53 A scoping review was the most appropriate study design for our objectives given we aimed to systematically map the extent and range of evidence on mindfulness-based interventions and yoga for managing obesity/overweight after breast cancer due to the paucity of clinical trials surrounding this area of research. In this process, we are able to identify gaps in literature and discuss the effectiveness, feasibility and safety of the intervention to inform research, policy and practice. This scoping review is reported according to the Joanna Briggs Institute (JBI) based PRISMA Extension for Scoping Reviews (PRISMA-ScR). 53 A protocol was developed a priori.
Eligibility Criteria
Selection criteria for selected papers were based off the PICO (Population, Intervention, Comparison, Outcomes) framework outlined in the Supplemental Table 1. The PICO framework was developed by VV and CE and was informed by a literature review and consultation with an expert librarian.
As we intended to explore the extent and range of research available for MBI and yoga for managing obesity/overweight after breast cancer, an extensive range of studies were included as long as they were peer-reviewed or were a published conference abstract. This includes all quantitative and qualitative studies that were original research. Non-original research, for example, editorials, opinion pieces were excluded. Quantitative studies include systematic reviews, meta-analyses, RCTs, non-randomized controlled studies, case/control studies, pre/post uncontrolled and pilot studies, and observational studies including surveys and case studies. We included systematic reviews because we were interested in the range of all types of original research in this area and considered that systematic reviews are a form of original research, albeit not reporting primary data. All types of qualitative studies were included as long as they explored an aspect of the role of yoga or MBIs in managing overweight/obesity after breast cancer.
Our population includes only females with breast cancer. While males are also susceptible to breast cancer, 54 due to the scarcity of clinical trials on male breast cancer, the team made the decision to limit the scope of the target populations to females only, or studies that enrolled a majority female population.
We included studies that examined the role of mindfulness and/or yoga as a standardized program on weight gain prevention, weight loss and/or weight maintenance for females diagnosed with breast cancer. These could be of any type of delivery, frequency and duration of sessions/practice, including group and individual, in-person face-to-face, retreats, smartphone apps, and online. MBIs had to be based around formal mindfulness meditation techniques as the main component. These are defined as practices where an individual sets aside time to engage in mindfulness meditation practices such as the body scan, sitting meditation, and mindful movement. 55 Mindfulness was defined as present moment awareness and non-judgment. 56 Papers that explore solely mindfulness as a psychological trait or psychotherapy without an explicit focus on mindfulness meditation techniques were excluded. Where studies utilized an intervention where the cultivation of mindfulness was not the primary aim or focus of the intervention (for example, in Acceptance and Commitment Therapy which draws on mindful principles within a larger suite of techniques) we excluded them. Any yoga-based study where yoga and its various aspects are the main component of the intervention such as yoga asanas, yoga stretching, yoga meditation, yogic mindfulness, pranayama, yogic breathing practices, yoga nidra, yoga-based lifestyle as the main component were included. We excluded any allied health or healing arts that are similar to yoga, but do not refer to the intervention as yoga.
Information Sources
The following electronic databases were used to identify relevant published literature:
PUBMED
EMBASE
Cochrane
PsycInfo
CINAHL
Search
An initial search was performed to identify any comprehensive systematic reviews on the topic prior to commencing the review. No systematic reviews were identified. A systematic search was performed based on the selection criteria and combining MeSH terms and text words to the above databases (see Supplemental Table 2 for full search strategy). The search strategy was limited to English language papers and there were no limits on year of publication. We also hand-searched the reference lists of all included studies, and performed forward citation searches to ensure we had not missed relevant studies. Where we identified systematic reviews, we only reported on studies which met our inclusion criteria and cross-checked reference lists to identify any potential studies missed by our search. The date of the last search was 1st of February 2022.
Selection of Sources and Evidence
Endnote 57 was used to manage search results. Titles, abstracts and keywords of articles retrieved were assessed by 2 independent reviewers (VV and CE) on a random sample of 20% of studies according to the selection criteria, to achieve consistency on at least 80% of the sample, with the remainder appraised by one reviewer (VV) and verified by another (CE). This process was repeated with screening of full-text articles. Any disagreement was resolved through discussion, and consistency was achieved on >80% of titles/abstracts and full-text articles screened.
Data Charting Process
Data for outcomes according to the selection criteria were extracted from included studies using a specially developed data extraction form. Two review authors (VV and CE) extracted data independently from the first 5 studies found and met to discuss any changes to the data charting form. The remainder was extracted by one author (VV) and verified by the second author (CE). Any disagreement between reviewers was resolved through discussion.
Data Items
Information was collected on general details (title, authors, year of publication, country, setting, study design, study aim, type of article), participant characteristics (inclusion and exclusion criteria, number of participants enrolled/completed or number of studies included, age and demographics, classification of breast cancer and time since diagnosis, level of treatment received and how long post-treatment and baseline BMI of intervention group and control group when relevant), nature of intervention (type of mindfulness-based intervention eg MBSR, MBCT and/or yoga, definition of mindfulness and/or yoga, description of the intervention components and development, aim of intervention in relation to weight related outcomes, delivery method, frequency and duration of program, duration of practice sessions, intervention provider training and experience, co-interventions, self-monitoring and/or home practice details, details of the control method, and outcomes (primary outcome of the study, weight-management related outcomes, prevalence of use, implementation, eg, feasibility, acceptability, whether adverse events were collected, and reported adverse events). Where trials were described as pilot RCTs we reported them as such, otherwise if they were described as randomized controlled trials and stated that their main aim was to assess effectiveness of the intervention against a comparison group (with no mention of piloting the method for a future RCT or collection of data for feasibility assessment) we classified them as RCTs regardless of sample size.
Synthesis of Results
We provided a descriptive numerical summary and narrative synthesis of the findings from the included studies, structured around the study design, location, population characteristics, intervention, control group and outcome. We grouped yoga and MBI findings separately and summarized the type of study design, type of yoga/MBI and aim of the intervention with regard to weight-related outcomes into tables.
Results
Our search yielded 1134 articles, excluding duplicates, which were screened according to our inclusion and exclusion criteria (see Figure 1). The final number of included publications was 18. Three of the included studies58-60 had 2 publications61-63 related to each study thus totaling to 15 unique included studies. Ee et al’s conference abstract 61 and Parma’s pilot RCT 63 share the same methods and outcomes as their original papers and thus will not be further referenced. Cadmus-Bertram et al ’s pilot RCT 59 evaluates the feasibility of Littman’s study.

Flowchart of study selection.
See Table 1 for a summary of the type of studies available for different forms of yoga and MBIs. The details of the studies are summarized in Supplemental Tables 3 and 4. We first describe the year of publication, study type, intervention (yoga, MBIs or both), and outcomes that were evaluated in all included studies, followed by a description of the characteristics of the studies by intervention (yoga or MBIs).
Summary of Included Studies.

Abbreviations: MA, meta-analysis; MBIs, Mindfulness-Based Interventions; MBSR, Mindfulness-Based Stress Reduction; NA , not applicable; NR, Not reported; RCT, randomised controlled trial; SR, systematic review
Year of Publication
The vast majority of studies in this field (13/15) were published in the past 10 years. There was an increase from the period 2011 to 2015 and 2016 to 2020 with 3 more studies published in the latter period than in the former. Figure 2 charts the total number of studies per 5-year period, with a breakdown of types of studies depicted.
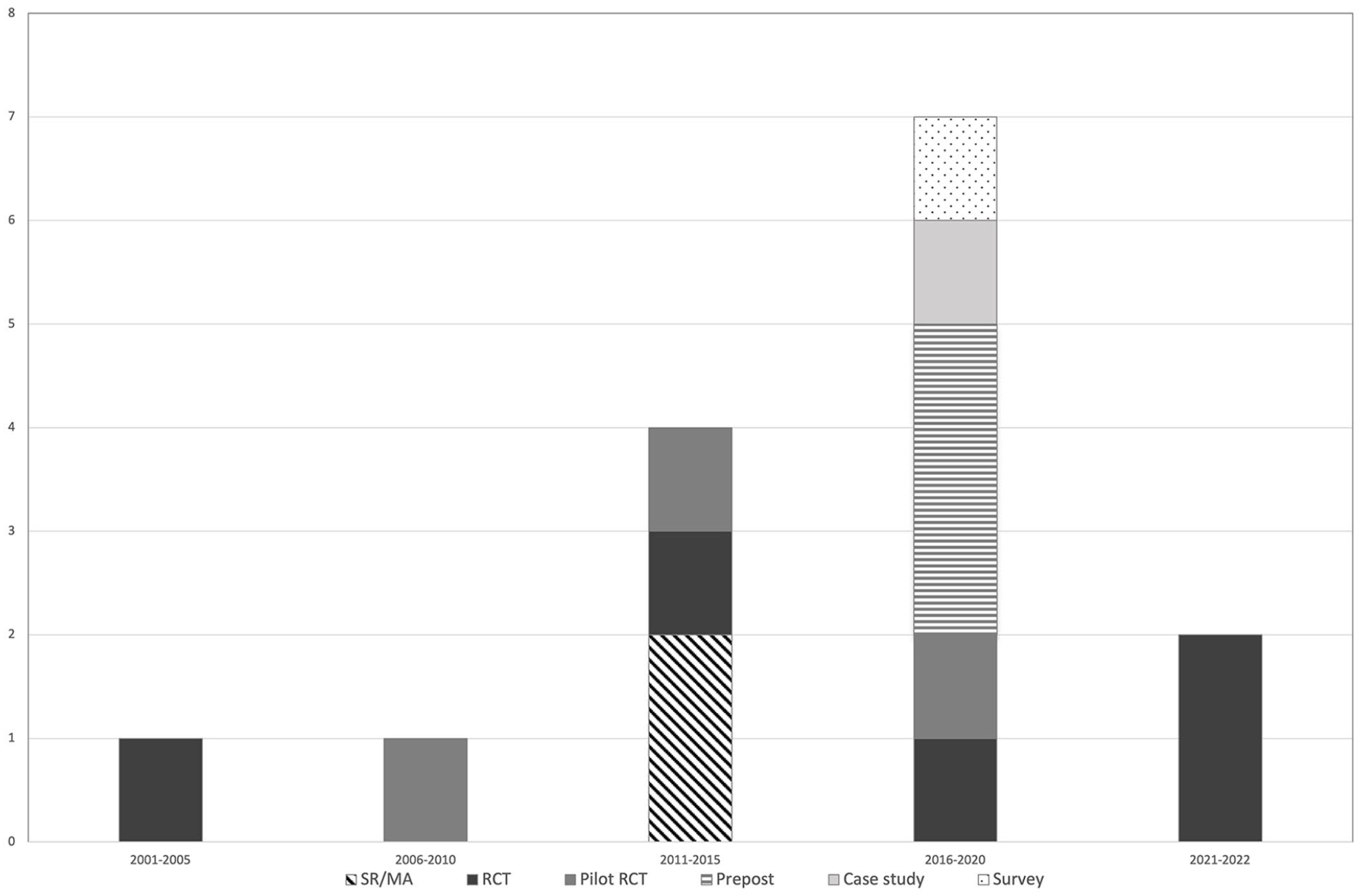
Publication year and study type.
Study Type
Figure 3 depicts the study types included and the interventions they evaluated. The majority of studies were clinical trials (11/15 studies) of which 5 trials were randomized controlled trials, and the remainder were described as pilot RCTs or pre-post clinical trials. There were 2 systematic reviews, both on yoga, and 2 observational studies (a case study and a cross-sectional survey).

Weight-related outcomes.
Outcomes
Of the 11 clinical trials (including RCTs, pilot RCTs, and prepost single-arm trials) less than one-third (3/11) included a weight-related outcome as the primary outcome. Five out of the 11 trials reported on a fitness or lifestyle related outcome for example change in diet, or a metabolic outcome (leptin and insulin). 64 Three trials examined non-weight related primary outcomes such as quality of life or inflammation.
When considering the weight-related outcomes that were reported in each study (whether primary or secondary), the most commonly reported outcomes were weight loss, followed by weight maintenance and body composition. There were just 2 studies that focused on weight gain prevention.
Figure 4 depicts the primary outcome of the included studies by study type, for the clinical trials.

Study type and primary outcome.
Details of Yoga Studies
Study Type
We found a total of 10 studies addressing yoga for managing overweight/obesity after breast cancer. Most of these were clinical trials (6/10), 2 were systematic reviews (one with a meta-analysis) and 2 were observational in nature. We found a total of 6 clinical trials on yoga. Most of these (5/6) were randomized (3 RCTs,62,64,65 2 were described as pilot RCTs),58,66, 1 was a pre-post single-arm trial. 67 Observational studies included 1 case study 68 and 1 cross sectional survey. 60 Littman et al ’s pilot RCT was included in both systematic reviews, while the pilot RCT by Culos-Reed et al 66 was included in the systematic review conducted by Buffart et al 43 Two publications were conference abstracts.67,70
Studies had been conducted in a range of countries including the United States,58,62 Iran,64,65 Canada, 66 Korea, 67 India, 68 and Australia. 60 The sample size for yoga clinical trials ranged from 1 to 72 participants, while the cross-sectional survey reported 309 responses (of whom 37 women had used yoga for weight management). 60
There was a lack of trials specifically designed to evaluate weight management after breast cancer. We only identified one trial that assessed the role of yoga for weight loss, along with fatigue and quality of life. 58 Three RCTs examined the role of yoga for related outcomes such as insulin and leptin levels 64 and fitness.62,66 Two trials were broader in nature, with examining the physical and psychological benefits of yoga,66,67 while another had a narrower aim to evaluate the efficacy of yoga training combined with high dose Vitamin D on gene expression involved in survival of immune cells. 65 Similarly the systematic reviews were not specifically related to weight management, aiming to evaluate the broad benefits of yoga (both physical and psychosocial) in people with cancer 43 and specifically in women with breast cancer. 45
Population
Of the primary studies, most of the participants were middle-aged with mean age ranging from 47.9 to 60.6 years old. There was a lack of reporting of stage of breast cancer with most trials (4/6)64-67 failing to report this. One trial reported including women with early breast cancer 58 and another included all stages from ductal carcinoma in-situ to metastatic breast cancer. 62 Most of the trials were conducted post-treatment, ranging from 2 months to 5 years post-treatment. Only one study 58 specifically enrolled participants who were overweight (defined as >24 kg/m2, or 23 kg/m2 if of Asian descent) – this was the one trial that was specifically designed to evaluate the role of yoga for weight loss. In the studies conducted in Western countries, there was a gap in inclusion of culturally diverse populations with most studies either including predominantly Caucasian participants or not describing participants’ ethnicity. The exceptions were one RCT that reported in which around one-third of participants were of Hispanic ethnicity. 62 However, our sample does include studies conducted in non-Caucasian populations for example in women in Korea 67 and Iran,64,65 and a case study from India. 68 Studies enrolled female participants except for one pilot RCT 66 that included 5% males.
Interventions
The reporting of details of the yoga interventions that were delivered in the studies was mixed, with a number of studies failing to report adequate details. Hatha yoga was the most commonly delivered type of yoga intervention.62,65,66 However, not all trials reported the type of yoga performed64,67 although Ebrahimpour et al described the type of asanas (postures) that were practised. 64 The remaining pilot RCT 58 delivered Viniyoga as the type of yoga intervention. The case study 68 examined the effects of Raja yoga.
The method of delivery varied with 3 of the trials62,64,66 delivering the yoga intervention face-to-face while one trial 58 had a mix of both face-to-face and at home classes. One was done under no guidance at home 68 while 2 of the studies encouraged home practice by providing audio CDs and booklets58,62 However, reporting was again mixed with one trial failing to specify how the yoga intervention was delivered. 67 Similarly, for details such as frequency and duration of practice, one trial failed to report these data. 67 For the remainder of the clinical trials, duration of the yoga program ranged from 4 weeks 67 to 6 months58,62 for clinical trials, and the case study reported practice for 15 years. Frequency of practice ranged from 5 times a week 58 to once a week 66 for the clinical trials and duration of practice ranged from 60 minutes to 90 minutes. The person in the case study 68 practiced for 45 minutes daily.
The reporting of the expertise of the provider was limited in most trials. One-third (2/6) of trials did not report on qualifications and expertise of the yoga provider at all58,67 while there was limited reporting in another trial which described the instructor only as an exercise physiologist professor, with no details on specific yoga expertise. 64 Only half of the trials62,65,66 described using certified yoga instructors to deliver the yoga program, although it was unclear what certification had been attained.
Only the trial by Ebrahimpour et al included a lifestyle co-intervention (30 minutes of pilates in addition to the 30 minutes yoga practice). 64 None of the other trials delivered a lifestyle co-intervention including Littman et al’s trial which was designed to evaluate weight loss.
Comparison Groups
In the randomized controlled trials, yoga was mostly compared to non-active controls, that is wait-list58,66 or usual care. 64 One trial compared yoga to exercise 62 which consisted of 2 control groups: one performing comprehensive programed exercises while the other performed their own choice of exercise. Another trial 65 compared yoga + vitamin D supplementation to vitamin D supplementation alone.
Outcomes
Weight-related
In terms of weight-related outcomes, the most commonly studied outcome in our sample was weight loss, which was the focus of 1 SR/MA, 62 1 pilot RCT, 58 and 1 RCT. 64 Weight maintenance was also commonly studied, in 2 RCTs72,73 and 1re-post trial. 69 Weight gain prevention was less commonly studied (1 SR 43 and 1 case study) 68 while in 2 studies it was unclear whether weight loss, weight gain prevention or weight maintenance was being evaluated.60,66
The most commonly reported anthropometric outcomes were body weight and BMI which were reported in 5 out of 6 clinical trials58,62,64-66 although Ebrahimpour et al only reported weight and not BMI. 64 There was limited reporting on central adiposity with 2 clinical trials reporting waist and hip circumference58,66, one calculating a waist-hip ratio. 66 Similarly there was limited reporting of body composition, with 3 trials reporting body fat percentage62,65,67 of which skinfold assessments were used in two62,65 and the method used not described in a third. 67 None of the trials used dual energy xray absorption (DEXA) to assess body composition. The cross-sectional survey assessed the perceived usefulness of yoga for weight management on a 7-point Likert scale ranging from “strongly agree” that yoga was effective in managing weight, to “strongly disagree.” Prevalence of use of yoga for weight management was also assessed. 60
Feasibility and acceptability
There was inadequate reporting of acceptability of yoga and feasibility of the intervention in terms of adherence rates. Only one pilot RCT evaluated satisfaction with the yoga program (including home practice and instructor-led classes) using a 10-point scale Likert scale and qualitative assessments (no description provided), 58 and, in a further analysis, explored psychological and physiologic factors associated with adherence to yoga practice. 59 The cross-sectional survey further explored the feasibility of yoga for weight management after breast cancer by asking respondents to choose from a list of pre-specified advantages and disadvantages of using complementary therapies for weight management (such as financial cost, and lack of research for effectiveness). However these factors were in response to complementary medicine in general rather than yoga alone. 60 The study also asked respondents which complementary therapies they would use for weight management should there be sufficient evidence demonstrating effectiveness, with yoga being one of the answer options.
Safety
There was a significant gap in reporting of adverse events encountered in the clinical trials. Only Littman et al’s pilot RCT specifically stated there were no significant injuries or adverse events as a result of practicing yoga. 58
Findings
Two trials reported positive findings for at least some weight-related outcomes. In the trial that was specifically designed to evaluate weight loss, the intervention group had smaller waist sizes after 6 months (mean difference −3.1 cm) compared to the waitlist control group. However there were no between-group differences in weight or BMI. 58 In the trial comparing yoga and vitamin D to vitamin D alone, there was a significant decrease in body fat percentage in the yoga groups compared to the vitamin D only group. 65 In the remaining randomized controlled trials, there was no difference between groups for outcomes of weight62,66 or BMI 62 noting that Ebrahimpour et al did not report any between-group comparisons, but found that there was no within-group change in weight in the yoga group. Similarly, the pre-post trial found that yoga did not affect body composition, although there was decreased body fat in arms at the end of the intervention. 67
The SR by Buffart et al did not include any meta-analyses on weight-related outcomes due to insufficient number of studies. The 2 included trials58,66 were assessed as high quality studies. The authors concluded that evidence for the physical effects of yoga was generally insufficient to draw further conclusions. Harder et al included one trial on weight 45 which was assessed as fair quality, and concluded that limited results suggest moderate-good evidence that yoga is a useful practice for women with breast cancer, and there is scope for more investigation into the physical benefits of yoga.
Among the observational studies, the case study reported ability to maintain a constant body weight, 68 and the survey reported that 43% of women found yoga to be effective for weight management. 60
Details of MBI Studies
Study Type
All of the 5 studies on MBIs were clinical trials, of which the majority were randomized (2 RCTs,72,73 1 pilot RCT), 71 and 2 pre-post single-arm trials.69,70 Two publications were conference abstracts therefore providing only limited data.61,70 Most (4/5) studies were conducted in United States,69-71,73, one in Spain. 72 Sample sizes ranged from 10 to 146. Unlike the yoga trials, all of the MBI trials were either specifically designed to evaluate weight loss69,71 and or evaluate change in lifestyle habits.70,72,73
Population
Mean age of participants was between 50 and 64.4 years old, with a total range of 29 to 76 years. Reporting of the stage of breast cancer was mixed, with these data not reported in 2 trials.70,71 The trials that reported on stage of breast cancer enrolled women with early breast cancer.69,72,73 Minimum time post-treatment was also not reported in all trials, and ranged from during treatment, 71 3 months, 69 to 12 months 72 where reported. There was a gap in cultural diversity of participants with only one trial 69 was specifically designed for culturally diverse women (from African-American backgrounds). The remaining trials enrolled participants who were predominantly of white/Caucasian ethnicity,70,71,73 or did not report on the ethnicity of the enrolled participants. 72
The majority of trials (3/5) did not specify overweight/obesity as inclusion criteria. Two studies69,71 enrolled participants with a BMI >25kg/m2 (overweight or obese). Half of participants in one study 72 were in the healthy weight range.
Interventions
MBIs were generally mindful eating interventions69,70 or adaptations of MBSR.72,73 The exception was one pilot RCT 71 that delivered an original program named Mindfulness- Oriented Recovery Enhancement (MORE) involving mindfulness meditation. MORE was originally developed to address substance use disorders, and was adapted for this study to treat maladaptive eating behaviors, exercise avoidance and excess adiposity, tailored for cancer survivors. The program included formal mindfulness meditation to promote interoceptive awareness and therefore improve appetite control, as well as regulation of negative emotions through mindful reppraisal, and savoring non-food rewards.
Reporting of the mode of delivery was mixed, with 3 of the MBI clinical trials69,71,73 reporting face to face delivery and method of delivery not specified in 2 trials.70,72 Frequency of MBI delivery was generally once or twice weekly, and duration of practice sessions ranged from 90 minutes to 2 hours. Duration of the programs ranged from 4 to 10 weeks. In contrast to the yoga trials, the reporting of qualifications of MBI providers was more complete with most trials reporting these data. Most trials (3/5) reported that the MBI was delivered by a health professional with Masters level qualifications (psychologists,72,73 or social workers 71 ). One trial reported that the provider was a certified mindfulness instructor. 70 Qualifications of the provider were not described in one trial. 69
Again in contrast to the yoga trials, most trials (3/5) provided lifestyle co-interventions.69,71,72 The most comprehensive of these were a program provided in Thomas et al trial that integrated diet counseling, individualized exercise prescription and self-monitoring (the Personalized Optimism with Exercise Recovery or POWER program) alongside the MBI. 71 The remaining 2 trials provided dietary interventions only. Ruiz-Vozmediano et al provided three 5-hour workshops on healthy eating, 72 and Chung et al provided individual diet counseling 69 alongside MBIs.
Comparison Groups
Comparison groups for the 3 RCTs consisted of either wait-list control 72 /usual care 73 or lifestyle interventions.71,73 The lifestyle interventions included a nutritional educational program 73 and the POWER program alone (dietary counseling, individualized exercise prescription, and self-monitoring). 71
Details of the Outcomes
Weight-related
Trials either focused on weight loss69-71 or weight maintenance.72,73 In terms of anthropometric measures, all collected data on body weight but only 2 reported change in BMI.69,70 There was limited reporting of central obesity and body composition with only 2 trials calculating waist-hip ratio70,71 and 1 reporting body fat percentage (method unspecified). 70 Aspects of mindfulness were also evaluated in 3 studies namely interoceptive awareness using a Multidimensional Assessment of Interoceptive Awareness instrument 71 ; mindfulness using the Mindful Attention and Awareness Scale 70 and mindful eating using the Mindful Eating Questionnaire. 69
Feasibility and acceptability
Most trials did not report on feasibility and/or acceptability and where this was reported, it was generally limited to retention rates71,72 although one trial reported on reasons for not being able to start the mindfulness program or its comparison. 73
Safety
None of the included studies reported on adverse events arising from participating in MBIs.
Key findings
Only one of the 3 RCTs reported positive findings for anthropometric measures. Ruiz-Vozmediano et al reported that an intervention based on MBSR resulted in significant between-group differences for body weight and BMI; notably, measures increased in the wait-list control group and decreased in the intervention group. 72 However, another trial that also compared an intervention based on MBSR with a usual care group, as well as a Nutritional Educational Program group, reported no changes in body weight. 73 Similarly, no between-group differences were reported for body weight in another RCT, nor for measures of central adiposity (waist-hip ratio) although there was a within-group change for WHR only in the intervention group. 71 However, both pre-post single-arm trials reported a decrease in body weight after the intervention. Washington et al also reported a decrease in BMI, but not in body composition (body fat percentage) or central adiposity (waist-hip ratio). 70
Discussion
This is the first scoping review to outline the breadth of current evidence on the role of yoga and/or MBIs for managing overweight/obesity after breast cancer. This is a crucial first step in informing future research on this important topic. By taking a comprehensive approach toward identifying all types of original research in this field, we have been able to identify gaps in the extant literature which can then be addressed in future studies. Our scoping review not only informs subsequent research on managing obesity/overweight after breast cancer, but is also relevant to ongoing research on mind-body therapies.
There is a scarcity of adequately-powered randomized controlled trials in this area, with a greater number of pilot RCTs and pre-post single-arm trials than of RCTs. Moreover, we did not identify any RCTs arising from the included pilot studies. Although it is encouraging that 3 RCTs were conducted relatively recently, we have identified an important gap in that only one RCT had a primary outcome that was weight-related; the other RCTs were indirectly related to weight management (focusing on fitness or lifestyle-related outcomes) or not related at all. Sample sizes for RCTs were also generally small, ranging from 30 to 146 participants. Future research should be developed as comprehensive research programs, with pilot RCTs followed up by subsequent adequately-powered RCTs in order to improve precision and reduce research waste.
Women who participated in the included studies were generally middle-aged and therefore likely to be postmenopausal. There is a need for studies to target younger women who are premenopausal at diagnosis, as weight gain is not only more likely in these women but also tends to be greater.74-79 Additionally, participants were mostly from Caucasian backgrounds, although one trial only enrolled women from an African American/black background 69 and another study was conducted on Korean women. 67 African-American women are more likely to gain weight after breast cancer compared to Caucasian women 80 and while Korean women do not tend to gain weight after breast cancer, certain subpopulations are at higher risk of weight gain (eg, younger women, those who are obese at diagnosis, and women with poor diet quality). 81 Future studies should aim to include a greater proportion of women from culturally diverse backgrounds in order to expand the external validity of the findings.
The yoga intervention characteristics such as type, duration, and frequency varied significantly in the included studies. Out of 6 clinical trials, only 4 reported on the type of yoga intervention used. The remaining 2 trials did not use a specific style of yoga; rather, they incorporated various aspects of yoga such as asanas (physical postures) or meditation. Moreover, reasons for selecting the yoga components were not highlighted. Therefore, a major gap was observed in the development of the yoga protocol. The duration and frequency of the yoga intervention varied tremendously between studies. Reporting on yoga providers was limited with most studies failing to report details on yoga provider’s qualification, training, and expertise in the field.
There is a need for improved reporting of yoga interventions in future studies. A systematic approach should be adopted in selecting a yoga intervention. 82 Various consensus methods that are available to design an intervention such as Delphi study or focus groups can be utilized to develop a protocol as a priori. 83 Recently the CheckLIst stAndardising the Reporting of Interventions For Yoga (CLARIFY) guidelines have been developed on reporting on yoga interventions, which can be utilized by the future studies for systematic and standardized reporting. 84
A number of trials did not offer lifestyle interventions as co-interventions. We found only 3 trials that delivered dietary interventions, and 2 trials that delivered exercise interventions alongside the yoga or MBI. This is a missed opportunity as yoga and MBIs may act in several ways to facilitate the adoption and maintenance of healthy lifestyles. Lifestyle interventions are effective for managing overweight/obesity after breast cancer,
85
however, there are barriers to adoption and maintenance.
66
Contemplative practices such as yoga and MBIs facilitate acceptance of discomfort, and agency (the ability to effect change).
51
MBIs and yoga may facilitate
Another major gap identified by this scoping review is the lack of active control groups for mind-body therapies. Most clinical trials used wait-list control or usual care groups, with the exception of Hughes et al who used a comparison exercise group to compare with comprehensive exercise and yoga. Active comparison groups control for non-specific factors and expectations, and therefore evaluate the efficacy of the active ingredient in interventions. An active control should be matched the study intervention in non-specific factors such as time and attention, and should be structurally equivalent (ie, providing the same number of sessions/duration as the intervention) but should not contain the “active ingredient” of the intervention (eg, active controls for MBIs would not aim to cultivate mindfulness through formal mindfulness meditation practice). Failure to compare mind-body therapies with active control conditions limits the certainty of the evidence presented.32,89 Future studies should consider using active control interventions such as the Health Enhancement Program (HEP), a validated active control intervention 90 for MBIs, or non-aerobic exercise and sham yoga for yoga interventions,91,92 in order to increase scientific rigor and provide greater certainty in reported findings.
In terms of the outcomes that were evaluated, several gaps are evident from our scoping review. Most of the evidence on yoga was not specific to managing overweight/obesity, but instead explored the broader benefits of yoga (both physical and psychological), or on fitness outcomes. There was only one pre-post trial that was specifically designed to evaluate the role of yoga for weight management. The weight-related outcomes that were collected were mainly anthropometric outcomes. The lack of reporting of body composition outcomes such as change in body fat percentage, fat mass and fat-free mass is evident. Additionally, the gold-standard of dual energy xray absorption (DEXA) to evaluate body composition was not utilized in any of the studies. Key gaps in the literature on weight loss interventions for women with breast cancer include a lack of evaluation of sustainable weight loss (weight loss >10% sustained for >12 months post intervention) or body composition. 93 Future studies on yoga or MBIs for managing overweight/obesity after breast cancer should evaluate not just weight change, but change in body composition using gold-standard measurements, and aim to follow women up for at least 12 months post-intervention. Last, only one trial reported collecting data on adverse events. While yoga and MBIs are generally considered to be low-risk interventions, this is based on limited data due to significant under-reporting in clinical trials.94,95 RCTs have reported an increase in frequency of intervention-related, nonserious adverse events when yoga is compared to psychological/educational interventions, 94 and temporary increase in experience of negative emotions have been reported with MBIs. 95 Adequate reporting of safety data in future RCTs is crucial to advance the field.
Strengths and Limitations
This is the first scoping review to comprehensively identify the research gaps in the area of mind-body therapies for managing overweight/obesity after breast cancer. Our search was comprehensive and our approach was rigorous and informed by expert guides on scoping review methodology. However, given that we did not search for gray literature, we may not have reported on all research that has been or is being conducted in this field. Additionally we restricted the search to English language publications only.
Conclusions
Future research on yoga and/or MBIs for managing overweight/obesity after breast cancer should incorporate active comparator groups, adequate reporting of the intervention, adequate safety reporting, and examine outcomes beyond body weight (such as body composition). Pilot RCTs should be followed up by subsequent adequately-powered definitive RCTs.
Supplemental Material
sj-docx-1-ict-10.1177_15347354221137321 – Supplemental material for Mindfulness-based Interventions and Yoga for Managing Obesity/Overweight After Breast Cancer: A Scoping Review
Supplemental material, sj-docx-1-ict-10.1177_15347354221137321 for Mindfulness-based Interventions and Yoga for Managing Obesity/Overweight After Breast Cancer: A Scoping Review by Vicki Vuong, Vibhuti Rao and Carolyn Ee in Integrative Cancer Therapies
Footnotes
Acknowledgements
Nil
Author Contributions
CE conceived of the original research idea. All authors contributed to design of the study. VV created the protocol, ran the searches, screened the studies together with CE, and extracted and synthesized the data. VV wrote the first draft of the manuscript. All authors contributed to interpretation of the findings and revising the manuscript for important intellectual content.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CE declares that she is the Program Lead of an academic integrative healthcare center that offers mindfulness and yoga services. She does not receive any remuneration from the operation of this center. VR is a yoga instructor. As a medical research institute, NICM Health Research Institute receives research grants and donations from foundations, universities, government agencies, and industry. Sponsors and donors provide untied and tied funding for work to advance the vision and mission of the Institute. All other authors declare that they have no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: VV conducted this research as part of her MD project at Western Sydney University. CE’s academic role is supported by an endowment from the Jacka Foundation of Natural Therapies.
Ethical Approval
NA
Consent to Participate
NA
Consent for Publication
NA
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.