
Abstract
Introduction:
This is a phase II pilot study to evaluate the efficacy of a nutraceutical compound composed of nervonic acid, curcuma rizoma, and l-Arginine to prevent the onset of bortezomib-induced peripheral neuropathy (BIPN) in 16 newly diagnosed multiple myeloma (MM) patients treated with bortezomib (BTZ) over 6 months.
Materials and methods:
Assessments included neurological examination and electroneurography, Common Terminology Criteria for Adverse Events (NCI-CTCAE), reduced version of Total Neuropathic Score (TNSr), pain evaluation, functional autonomy scales, self-perceived symptoms and quality of life questionnaires at baseline and after 6 months.
Results:
No patients were symptomatic at baseline, despite neurophysiological data and TNSr evidence of peripheral neuropathy (PN) in 11 of them. After 6 months, only 9 patients completed the study. All had modifications in neurological examination with 8 out of 9 showing neurophysiological data of PN (2 of which had a NCI-CTCAE grade of neurotoxicity ≥2); 4 patients dropped out due to BIPN, 2 because of MM progression, 1 for scarce compliance.
Discussion:
In our study, the compound was not adequate to prevent BIPN. The incidence of subclinical PN in MM patients is a risk factor for the development of severe neurotoxicity during BTZ treatment. For this reason to evaluate the efficacy of any preventive compound, as well as to manage MM patients, it should be mandatory to include neurophysiological study as a standard procedure.
Keywords
Introduction
Peripheral neuropathy (PN) is a frequent and significant complication of MM (MM associated Peripheral neuropathy-MM-PN) that can be cause by the disease per sè in 20% of newly diagnosed patients.1-7 Moreover, MM-PN may be triggered or exacerbated by potentially neurotoxic MM treatments in 75% of cases (Chemotherapy induced PN-CIPN) which can worsen symptoms and pain already present.1,4,8 The chemotherapeutic agents used for the treatment of MM include novel immunomodulator agents (ie, thalidomide, lenalidomide) and proteasome inhibitors (ie, bortezomib-BTZ) that exert a pleiotropic action on nerve fibers, which could induce CIPN.7,9-12 BTZ and thalidomide have become the predominant cause of CIPN in MM with an estimated incidence of 37% to 83%.7,9-12 CIPN experienced by patients treated with BTZ (bortezomib-induced peripheral neuropathy-BIPN) is predominantly sensory or sensorimotor, and typically characterized by segmental demyelination and distal axonal degeneration.2,13 Reported symptoms are usually symmetric and include paresthesia, numbness, burning or tingling and weakness.2,13 These are generally mild symptoms, but in rare cases can be disabling or even life-threatening.1,13 BIPN may induce impairment consequently having an adverse impact on the quality of life and is one of the most important factors that lead to a dose reduction or discontinuation of chemotherapy, potentially affecting patient survival.4,5,8,13-15 For this reason, much effort has been put toward developing strategies to prevent and treat BIPN. Prevention should be the preferred approach in maintaining a stable level of functional autonomy of daily activities and a good quality of life, and in preserving future options for anti-myeloma treatment. 6 Nevertheless, to date evidence-based recommendations for any neuropathy preventative agent are still lacking.1,16
Published data indicate that nutraceuticals with antioxidant and axonal regrowth action may be useful in reducing inflammation and favoring the formation of new axons and intersynaptic connections.17,18 There are new lines of evidence suggesting that other compounds, such as nervonic acid, curcumin, and L-arginine may play an important role against oxidative stress, favoring normal myelin function in neurodegenerative diseases as well as mitigating or preventing neuropathic and postoperative pain.19-25 Nervonic acid is a monounsaturated fatty acid and exists in nature as an elongation product of oleic acid. It is also implicated as an intermediate in the biosynthesis of nerve cell myelin.19-21 Curcumin has been demonstrated to have a variety of biologic activities, including anti-inflammatory activities and anticancer properties.22,23 L-Arginine is an α-amino acid that is used in the biosynthesis of proteins. It guarantees greater bioavailability of the nervonic acid but also of curcumin.24,25
On this basis, we conducted a phase II pilot study to evaluate the efficacy of a new nutraceutical compound composed of nervonic acid, curcuma rizoma, and l-Arginine to prevent the onset of BIPN in 16 newly diagnosed MM patients over their first 6 months of BTZ treatment.
Methods
The primary objective of the study was to assess whether nutraceutical compounds could be effective in preventing the onset of grade 2 CIPN or higher according to the National Cancer Institute-Common Terminology Criteria for Adverse Events (NCI-CTCAE) 26 in newly diagnosed MM patients. Grade II cutoff of neurotoxicity on the NCI-CTCAE was chosen according to guidelines for supporting care in MM13 which recommend BTZ withdrawal and discontinuation when PN reaches grades 3 and 4 of NCI-CTCAE. The secondary objectives were to assess whether the nutraceutical compound could prevent the onset of mild PN according to the reduced version of Total Neuropathic Score-TNSr (range score: 1-10),27,28 without painful symptoms or modifications of functional autonomy and perceived quality of life during the first 6 months of BTZ treatment.
Subjects
Newly diagnosed MM patients according to the International Myeloma Working Group Criteria,1,29,30 who were planned to receive subcutaneous BTZ were consecutively enrolled in the study. Patients were treated according to the current standard of care and no additional diagnostic or therapeutic procedures were performed. The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institute’s Ethics Committee (RS1219/19); informed consent was obtained from all subjects involved in the study.
Inclusion criteria were as follows: newly diagnosed patients (both genders) with MM and naïve to chemotherapy, aged between 18 and 85 years old who gave written informed consent; a baseline normal neurological evaluation without symptoms of peripheral neuropathy, NCI-CTCAE scale score = 026 and Visual Analog Scale-VAS = 031 indicating absence of painful symptoms.
Exclusion criteria were: patients aged <18 years >85 with any other neuropathies (eg, diabetic neuropathy) and any other hematological disorders, patients currently or previously treated with chemotherapy, patients not able to comply with the study procedures (ie, completing questionnaires), history of alcohol abuse or documented severe vitamin deficiency, as well as patients who are hypersensitive or allergic to any of the components of the nutraceuticals medically proven or referred by patients.
Study treatments
The nutraceutical compound was composed of: curcuma rizoma (Curcuma longa L.) e.s. tit. 88% in curcuminoids/68% curcumin (100 mg), nervonic acid (50 mg), and l-Arginine (100 mg). The dosages of the components were chosen on the basis of the increase in bioavailability of curcumin and nervonic acid due to a micellar technology that increases their enteric bioaccessibility. Moreover, the presence of basic l-arginine in the form of a free base increases the bioavailability and solubility in water of the compound 32 Pill bottles were given to patients at each visit. Patient compliance was verified by checking the number of pills returned. The study treatment was then taken orally, one tablet twice daily for 6 months.
Tolerability and incidence of adverse events (AE) during treatment with BTZ and the nutraceutical compound were assessed using the NCI-CTCAE. 26 An AE is any unfavorable and unintended sign, symptom, or disease temporally associated with the use of a medical treatment or procedure that may or may not be considered related to the medical treatment or procedure. Progression of disease was not considered an AE. All the patients who consumed at least one drug dose were included in the analysis of toxicity. All spontaneously reported, or observed AE were recorded along with details of time of onset and resolution, intensity, need for concomitant treatment, and the investigator’s opinion of a possible relationship with study treatment.
Assessment tools
Neurological examination: included a medical history specifically addressing symptoms of numbness, tingling or pain, weakness in the extremities, in addition to a complete neurological examination focused on tendon reflexes, strength, and sensory modalities, assessed with Rydel Seiffer tuning fork. 33
Electroneurography (ENG): Nerve conduction was examined using conventional procedures and a standard electromyography machine (Medelec Synergy®). To examine motor nerves, the right median and right peroneal nerves were evaluated. To examine sensory nerves, right median and bilateral sural nerves were evaluated. Compound muscle action potentials (CMAPs) were recorded from the abductor pollicis brevis, and sensory nerve action potentials (SNAPs) were recorded from the second digit. Skin temperature was measured near the stimulation site and maintained above 32.0°C. Median SNAPs were recorded from the index finger after antidromic stimulation at the wrist, and sural SNAPs were noted at lateral malleolus after antidromic stimulation delivered 14 cm proximal to mid-calf. 34 Diagnostic criteria are based on the presence of ≥1 abnormal attribute in ≥2 separate nerves (using ≤5th / ≥ 95th percentile cut-off), including assessment of the sural nerve. 28
National Cancer Institute-Common Terminology Criteria for Adverse Events (NCI-CTCAE) is an oncology toxicity scale that grades CIPN according to symptoms and disability; the severity of sensory and motor peripheral neuropathy was graded from Grade 1 (mild) to 4 (disabling). 26
Reduced version of Total Neuropathic Score-TNSr can be used to assess the severity of CIPN effectively and is a composite score that includes an evaluation of motor, sensory and autonomic symptoms and signs, quantitative determination of the vibration perception threshold, and neurophysiological examination of 1 motor and 1 sensory nerve in the leg. TNSr ranges between 0 and 32 points and the severity of CIPN can be classified according to the following neuropathy scale: 1 to 10 mild, 11 to 20 moderate, >20 severe.27,28
Visual Analog Scale for pain (VAS) to evaluate self-perceived pain through a visual scale ranging from 0 (no pain) to 10 (unbearable pain) in patients. 31
Activity of daily life (ADL) and Instrumental activity of daily life (IADL) scales to assess patients’ functional autonomy/self-care and performances of daily life activities. 35
European Organization for Research and Treatment of Cancer Quality of Life Core-30 (QLQ-C30) Scale to assess the functional status, tumor-related symptoms, and self-perceived quality of life in cancer patients. 36
European Organization for Research and Treatment of Cancer Chemotherapy-induced Peripheral Neuropathy-CIPN20 module to assess the possible onset of sensory, motor, and autonomic symptoms induced by chemotherapy. 37
European Organization for Research and Treatment of Cancer: Multiple Myeloma-MY20 module to assess multiple myeloma symptoms and possible variation in in disease stage and treatment modality. 38
Visits schedule
The following assessments were performed at baseline (T0) and final follow-up (T1) at 6 months: informed consent signature, neurological examination, electroneurography (ENG), evaluation scales for the assessment of: CIPN (NCI-CTCAE and TNSr), pain (VAS), and functional autonomy/self-care (ADL, IADL), completion of self-perceived symptoms and quality of life questionnaires (QLQ C-30; CIPN-20; MY-20).
At baseline, blood levels of vitamin B12 were measured, and after eligibility assessment, nutraceutical compound was given to patients 13 .
All enrolled patients received 3 different therapy regimes with subcutaneous BTZ. VMP for transplant-ineligible patients, fit: treatment comprised nine 6-week cycles of VMP (Bortezomib 1.3 mg/m2 on days 1, 4, 8, 11, 22, 25, 29, and 32, cycles 1-4, and days 1, 8, 22, and 29, cycles 5-9, plus Melphalan 9 mg/m2 and prednisone 60 mg/m2 on days 1-4, cycles 1-9). VMP for transplant-ineligible patient, unfit: treatment comprised nine 5-week cycles of VMP (Bortezomib: 1.3 mg/m2, on days 1, 8, 15, 22 every 35-day cycle, plus Melphalan 9 mg/m2 and prednisolone 60 mg/day on days 1-4 every 35-day cycle).39,40 VTD for transplant eligible patients: treatment comprised 4 to 6 cycles every 21 days (Bortezomib 1.3 mg/m2 on days 1, 4, 8, 11, plus 200 mg/day Thalidomide administered orally (escalating doses in the first cycle: 50 mg on days 1-14, and 100 mg on days 15-28), dexamethasone 40 mg, on days 1, 2, 4, 5, 8, 9, 11, 12.41,42
Each patient underwent monthly neurological visits according to normal clinical practice in order to monitor the occurrence of any adverse event. No diagnostic or therapeutic procedures were applied that are different to or in addition to the standard.
Efficacy variables
Primary efficacy variable: CIPN less than grade 2 of NCI-CTCAE 26 at final follow-up.
Secondary efficacy variables: TNSr27,28 within the range of 1 to 10 (mild PN), stability in questionnaire scores related to painful symptoms (VAS), 31 functional autonomy (ADL/IADL), 35 and perceived quality of life (QLQ C-30; CIPN-20; MY-20)36-38 at final follow-up compared to baseline.
Statistical analysis
According to the National Cancer Institute-Common Terminology Criteria for Adverse Events (NCI-CTCAE) 24 CIPN can occur greater than or equal to grade 2, in 19% of patients treated with VMP schedule (velcade, melphalan, prednisone) and in 35% patients treated with VTD schedule (velcade, thalidomide, dexamethasone).2-9
Assuming that patients were treated 50% with the VTD scheme and 50% with the VMP scheme, the average incidence of neurotoxicity is 27%. In our previous study, 18 we observed a single case of neurotoxicity > grade 2. The hypothesis is that an incidence of 5% versus an incidence of 27% is observed as reported in literature. The primary endpoint is the proportion between the number of patients who have grade 2 (or higher) neurotoxicity and the number of patients enrolled. The study design is based on the binomial distribution. A value of p0 = 27% is therefore assumed (ie, an incidence of toxicity which, if true, would imply that the proposed treatment cannot be considered adequate and therefore does not deserve to be the object of subsequent studies) and a value p1 = 5% (ie, an incidence that, if true, would imply that our treatment has an acceptable toxicity control). Establishing a 5% significance level with 80% power, we will enroll 16 patients in the study. If at least 15 patients do not experience grade 2 or higher toxicity, the experimental treatment will be considered sufficiently adequate to avoid neurotoxicity and may be proposed for a subsequent comparative phase III study. The results for the primary and secondary objectives are reported with a 95% confidence interval. Additionally, patient characteristics and treatments are described by means, medians, standard deviations and ranges if related to quantitative variables and by absolute and relative frequencies for qualitative variables. Paired Student’s t-test was used to compare quantitative variables assessed at different times.
Graphical representations are used to facilitate the interpretation of the data.
Results
Sixteen newly diagnosed MM patients were followed for 6 months: 9 males (56.3%) and 7 females (43.8%) with a median age of 66 years (range: 54-83). Nine patients (56.4%) completed the study, while 7 (43.6%) dropped out: 1 because of scarce compliance, 3 because of neurotoxicity, 2 patients for disease progression, and 1 for both progression of disease and neurotoxicity. All these 3 patients had cytogenetic risk Intermediate -High and stage Durie – Salmon III. Thirteen patients completed the established treatment program. Eleven (68.7%) patients had positive immunofixation for IgG kappa at diagnosis, 5 other (31.3%); 8 (50%) patients ISS-R stage 1, and 8 (50%) ISS-R stage 2 to 3; stage Durie – Salmon 6 (37.5%) IA, 3 (18.7%) IIA, 7 (43.7%) III A-B; 8(50%) standard cytogenetic risk, 7 (43.7%) intermediate – high, 1 patient was negative for the cytogenetic study.42,43 Nine patients (56.2%) received treatment according to the regimen VTD and 7 (43.8%) VMP; 3 patients (18.7%) discontinued therapy for disease progression within 6 months. Patient characteristics are shown in Table 1. 29
Patients’ Demographic and Clinical Features.

Abbreviations: IgG k, Immunoglobulin Ig G k; IgG λ, Immunoglobulin Ig G λ; ISS stage, International Staging System; DS stage, Durie–Salmon stage; VTD, Bortezomib, Thalidomide, Desametasone; VMP, Bortezomib, Melphalan, Prednisone; BTZ, Bortezomib; PD, Progressive Disease; PN, peripheral neuropathy.
At baseline, the whole population had normal neurological examinations and no symptoms or pain were detected or referred by patients (mean VAS score: 0); NCI-CTCAE was equal to 0 in all patients. Functional autonomy (ADL) and ability to perform instrumental activities of daily living (IADL) showed some impairment (ADL: 5.6 ± 1.0; IADL: 6.8 ± 1.4), specifically: 8 patients had a totally preserved autonomy, 5 only subtle limitations in instrumental activities in daily living, while 3 patients reported a significant limitation in both areas (due to MM-related bone lesions). TNSr mean scores were indicative of mild neuropathy (2.2 ± 2.3); considering TNSr values individually for each patient, we found that 11 of them (68.7%) had a score between 1 and 10 indicating mild neuropathy, while 5 patients had a TNSr score equal to 0 (see Table 2). We observed a reduction below normal values of amplitude of compound of motor action potential (CMAP) of right peroneal nerve in 5 out of 16 patients and of amplitude of the sensory potential (SAP) of right sural nerve in 8 patients (see Table 3). EORTC-Quality of life questionnaire (QLQ C30) showed a good self-perceived quality of life, preserved functional autonomy, but slight disease symptoms such as: fatigue, pain, insomnia, constipation and diarrhea. EORTC CIPN-20 showed the presence of subtle sensory, motor and autonomic symptoms, while myeloma specific module (EORTC-MY20) showed the presence of moderate concerns for the future and slight disease-induced symptoms.
Neurological Evaluation at Baseline and at 6 Months Follow-Up.
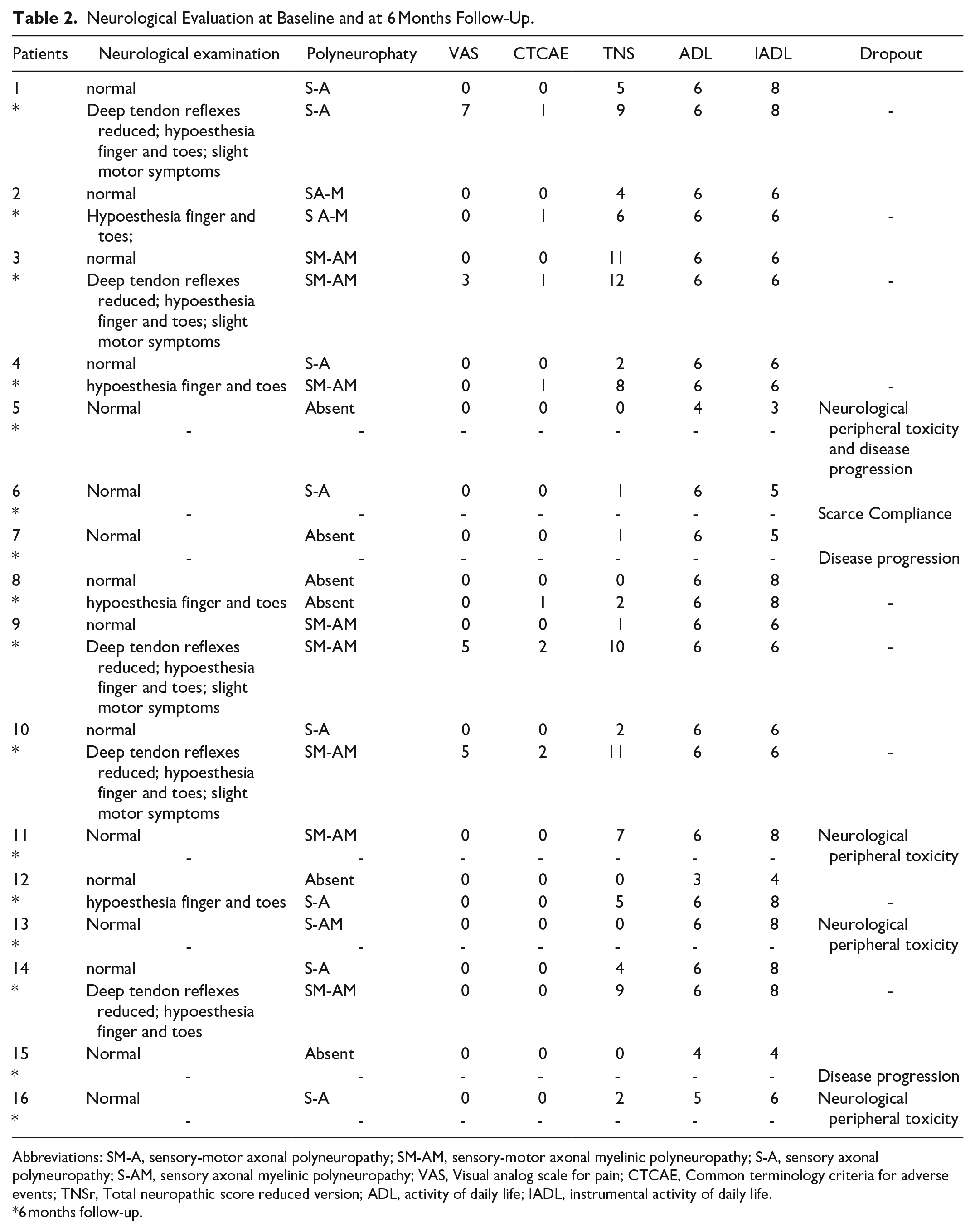
Abbreviations: SM-A, sensory-motor axonal polyneuropathy; SM-AM, sensory-motor axonal myelinic polyneuropathy; S-A, sensory axonal polyneuropathy; S-AM, sensory axonal myelinic polyneuropathy; VAS, Visual analog scale for pain; CTCAE, Common terminology criteria for adverse events; TNSr, Total neuropathic score reduced version; ADL, activity of daily life; IADL, instrumental activity of daily life.
6 months follow-up.
Neurophysiological Data at Baseline and After 6 Months of BTZ Treatment in Association with Nutraceutical Compound.

Abbreviations: CMAP, amplitude of the compound muscular potential (normal value >2 mV); SAP, amplitude of the sensory potential (normal value >6 µV). 28
At 6 months, neurological examination was altered in all 9 patients who completed the follow-up; mean VAS score significantly increased compared to baseline, however it remains within low values (basal mean VAS score: 0; final mean VAS score: 2.2 ± 2.8; P = .04); pain was reported by 4 patients, but it had no such intensity to require any pharmacological intervention. Mean NCI-CTCAE score significantly increased at final follow-up (1.0 ± 0.7; P = .003): 5 out of 9 patients (55.6%) progressed from NCI-CTCAE 0 to grade 1, and 2 of them experienced pain; 2 patients (22.2%) progressed to NCI-CTACAE grade 2 with pain and 2 (22.2%) remained to NCI-CTCAE = 0. Functional autonomy and ability to perform instrumental activities in daily living remained stable, except for slight limitations in instrumental activities of daily living, and questionnaire mean scores showed no significant differences at 6 months compared to baseline (ADL: 6.0 ± 0.0; IADL: 6.8 ± 1.1). TNSr mean scores showed a significant increase at final evaluation (basal: 2.2 ± 2.3; 6 months: 7.3 ± 3.6; P = .001), although it remained within the range of a mild neurotoxicity (1-10); considering TNSr values individually for each patient. We found that 7 of them (77.8%) had a score between 1 and 10 indicating mild neuropathy, while 2 patients (22.2%) had a TNSr score of ≥11 points (range 11-20: moderate neuropathy) (See Table 2). ENG mean values significantly worsened at 6 months compared to baseline regarding latency of median sensitive nerve (basal: 50.1 ± 4.6 ms; final: 45.7 ± 4.4 ms; P = .04), right sural nerve velocity (basal: 34.8 ± 19.9 m/s; final: 14.4 ± 21.6 m/s; P = .02), right sural nerve amplitude (basal: 5.1 ± 4.5 μV; final: 1.5 ± 4.1 μV; P = .04), left sural nerve latency (basal: 3.4 ± 1.3 ms; final: 0.4 ± 1.3 ms; P = .001), left sural nerve velocity (basal: 39.1 ± 14.9 m/s; final: 4.9 ± 14.8 m/s; P < .0001), and left sural nerve amplitude (basal: 6.4 ± 5.0 μV; final: 1.7 ± 5.0 μV; P = .02) (See Table 3). EORTC-Quality of life (QLQ C30) and myeloma (MY-20) specific questionnaires were stable, showing no significant difference compared to baseline evaluation. EORTC CIPN-20 showed a significant increase of autonomic symptoms scale at 6 months (basal Autonomic scale mean scores: 9.8 ± 14.0; final Autonomic scale mean scores: 19.7 ± 10.7; P = .03), while sensory and motor symptoms scales remained stable.
Discussion
BIPN in MM patients is a frequent symptom, which has an incidence approximately between 25% and 55%.13,16,44 BIPN could have a significant impact on QoL and may be a relevant issue on pain intensity, leading to dose reduction or discontinuation of chemotherapy in more than 12% of cases,3,4,8,12,18 potentially affecting patient survival.
Despite the importance in preserving these patients from BIPN,13,16,18 recommendations are lacking on the use of a specific neuropathy preventative agent. 13 We therefore decided to verify in a phase II prospective pilot study, whether a nutraceutical compound composed by nervonic acid, curcuma longa, and l-Arginine bid could prevent the onset of BIPN in 16 naive patients with MM at first diagnosis treated with BTZ.
To consider this compound efficient, 15 out of 16 patients would not have had to experience neurotoxicity grade 2 or higher according to NCI-CTCAE. 24 Four patients dropped out due to BIPN, and 2 out of 9 patients who completed the study experienced a grade of neurotoxicity ≥2 of NCI-CTCAE. 26 The endpoint has to be considered unreached. Different features that may explain the poor result we obtained should be taken into account. First, literature data regarding neurophysiological evaluation in MM naïve patients are very few; the only 2 studies available reported evidence of subclinical PN in approximately 38% of cases.8,45 In our study, despite no patients exhibiting clinical signs of PN or pain at baseline (normal neurological examination, pain and NCI-CTCAE assessment scales equal to 0), neurophysiological data evidenced subclinical PN in 11 out of 16 patients (68.7%) (see Table 2), further confirmed by TNSr. Our results seem to indicate that in naïve MM patients there is a much higher percentage of subclinical PN, evidenced not only by neurophysiological data, but also by a composite clinical tool such as TNSr. Considering that subclinical MM-PN could exacerbate BIPN symptoms during treatment with BTZ in MM naïve patients,1,46 it is extremely important to study neurological and neurophysiological status of all patients at the time of diagnosis, independently from the presence of evident neurological signs. We assume that combining ENG and TNSr in addition to clinical examination, could allow clinicians to identify a higher presence of a subclinical MM-PN, classifying patients as low or high risk of developing CIPN and therefore avoid interrupting cancer therapies.2,3,5,25
The pathogenesis of neural damage underlying BINP is still limited,42,45 however some studies report in animal models that the toxic effect is mainly directed toward satellite cell (Shwan cells, myelin) although axonal degeneration, oxidative stress and inflammation could also be present.42,47,48 On this basis, we assumed that a nutraceutical compound composed of nervonic acid, curcumin and L-arginine, which are implicated in the biosynthesis of nerve cell myelin and exert an anti-inflammatory activity,19-25 could preserve patients against BIPN. The neuroprotective effect that we expected did not occur. Superficial sensation is transmitted along both unmyelinated fibers (C), which are mainly responsible for pain sensation, and thin myelinated ones (Aδ) that propagate thermal and light touch sensation.49-51 We can hypothesize that the re-myelinating action of nervonic acid was not sufficient to protect nerves and preserve patients from pain, both because the fibers were already partially damaged by subclinical PN, and because the damage also involved unmyelinated fibers.
Moreover, regarding the expected antinociceptive action of curcumin, in our study, 100 mg/day was administered, while recent studies on animal models have highlighted its beneficial effect at doses ranging from 10 to 200 mg/kg/day. 22 Studies on humans observe a good efficacy of curcumin at dosages ranging from 80 to 1000 mg/day.52-57 In cancer patients with CIPN, the only study available to our knowledge is from Belcaro et al, in which they observed a good efficacy of curcumin in reducing pain at doses of 500 mg/day, for 2 months. 54 We decided to administer curcumin at dosage of 200 mg/day due to micellar technology of the compound which increased the bioavailability of the various components, and for longer time period (6 months). Despite these aspects, our compound was not effective in reducing pain. For this reason, we believe that future prospective studies with a larger population, using higher dosages of the different components are needed. Finally, to evaluate the efficacy of any CIPN preventive compound, as well as to manage MM patients, it should be mandatory to include the use of neurophysiological study as standard procedure.
Conclusion
The incidence of subclinical PN in MM patients is an important risk factor for the development of severe neurotoxicity during treatment with BTZ, requiring dose reduction or treatment discontinuation, potentially affecting patient survival. An accurate neurological evaluation, which includes neurophysiological study as standard assessment procedure, is paramount. This type of taking care of MM patients includes a multidisciplinary team with hematologist and neurologist working together, with periodic meetings and periodic follow-up for patients.
Footnotes
Acknowledgements
Thanks to Tania Merlino for reviewing the English form of the manuscript.
Author Contributions
MM: conception and design of the study, interpretation of data, drafting, and revising the article; AM: acquisition of data, interpretation of data, drafting the article; FM: acquisition of data, drafting the article; SG: acquisition of data, drafting the article; FP: acquisition of data; EP: acquisition of data; EG: acquisition of data; TK: acquisition of data; GG: acquisition of data; DG: analysis and interpretation of data; AM: revising the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.