
Abstract
Background:
Shenling Baizhu San (SBS), a well-known Chinese medicine herbal formula, has been widely used for treating chronic diarrhea for thousands of years. However, the efficacy and safety of SBS in treating chronic diarrhea have not been fully assessed.
Objective:
This study evaluates the efficacy and safety of the herbal formula SBS in symptomatic relief of chronic diarrhea.
Methods:
English and Chinese language databases (PubMed, Cochrane Library, China National Knowledge Infrastructure, China Science and Technology Journal Database, Wanfang Data, and SinoMed electronic databases) were searched through April 2020 for relevant randomized controlled trials (RCTs). The outcomes in these RCTs included stool frequency, stool consistency, patient-reported satisfaction of chronic diarrhea treatment, quality of life and adverse events. Paired reviewers independently extracted data and conducted qualitative and quantitative analyses. The Cochrane revised risk of bias RoB-2 tool was applied to assess the risk of bias for each trial whereas the RevMan 5.3 software was used for outcomes data synthesis and meta-analysis. Mean difference (MD) and the 95% confidence interval (CI) were used to measure continuous data. The dichotomous data were analyzed via the relative risk (RR) with 95% CIs.
Results:
Fourteen RCTs including 1158 participants (54% males) with chronic diarrhea were included. Shenling Baizhu San combined with or without conventional medicine (CM) was associated with greater patient-reported satisfaction than CM alone. There was no increased risk of adverse events (AEs) during treatment.
Conclusion:
Treatment with SBS was associated with significant improvement in patient-reported satisfaction, irrespective of conventional medicine use. Rigorous and powered RCTs with objective outcome measures are needed to confirm the effects of SBS in specific gastrointestinal disease populations with chronic diarrhea symptoms.
Systematic review registration number (PROSPERO):
CRD42020178073
Keywords
Introduction
Chronic diarrhea is defined as loose/watery stools with increased frequency (≥3 times/200 g per day) persisting longer than 4 weeks,1,2 and affects up to 5% of the global population.2,3 A key element in standard of care is the identification and treatment of any underlying etiology. In addition, symptomatic relief of diarrhea should be provided when clinically appropriate, as per clinical practice guidelines from the American Gastroenterological Association—for example, using opiates to slow down intestinal peristalsis and prolong the time of fluid absorption.2,4 However, opiates and adsorbents have limitations, including adverse effects5-7 and unsatisfactory treatment effect.7,8 In recent years, an increasing number of patients have sought complementary treatments, such as herbal formulas and dietary supplements, to alleviate chronic diarrhea.9,10
Herbal formulas have a long history of use for relieving gastrointestinal symptoms.11,12 One such formula, Shenling Baizhu San (SBS, Ginseng and Atractylodes Formula, Samryungbaekchul-san in Korean; Jinryobyakujutsu-san in Japanese), is frequently used for chronic diarrhea by clinicians in the Asia-Pacific region.13,14 The classic SBS formula is composed of 10 herbs (Table 1) but in clinical practice, minor modifications may be made based on a patient’s presentation. In addition to its clinical use, research shows that components of SBS may alleviate intestinal inflammation and alter the gut microbiome to improve water absorption and diarrhea.15-17
Constituent Herbs of Shenling Baizhu San.

Shenling Baizhu San has been evaluated in clinical studies as a treatment for patients with chronic diarrhea.14,18 Evidence of efficacy, however, is mixed. A systematic review of currently available data, and a pooled analysis of efficacy and safety data from RCTs can help inform clinical practice. Here we summarize the current clinical evidence for SBS in the management of chronic diarrhea.
Methods
This study was registered under PROSPERO (CRD42020178073).
Eligibility Criteria
This review included RCTs published in any language. The interventions include SBS, with or without modifications, used alone or in combination with conventional medicine. Studies where SBS was combined with non-conventional therapies, such as acupuncture, massage, far infra-red physical therapy, thermotherapy, magnetic therapy, or pulse physical therapy were excluded. Studies that compared the effects of different modifications of SBS were also excluded as this is not the focus of this review. Our primary outcomes were stool frequency (measured by the exact number of defecations recorded per day) and stool consistency (changes from baseline assessed using the Bristol Stool Form Scale). Secondary outcomes were: (1) patient-reported satisfaction of chronic diarrhea treatment (percentage of patients who reported satisfaction of recovery from chronic diarrhea measured by either “cured cases” or “symptom relief rate” in the outcomes of included RCTs); (2) quality of life (score change from baseline); and (3) AEs.
Search Strategy, Study Selection, and Data Extraction
A literature search was conducted using PubMed, Cochrane Library, China National Knowledge Infrastructure (CNKI), China Science and Technology Journal Database (VIP Data), Wanfang Data, and SinoMed electronic databases through April 20th, 2020 with no language restrictions. Chinese translations of the search terms were used for Chinese databases. Two reviewers (HW and YNH) assessed the eligibility of each record. Initially, the title and abstract were screened. Studies that were not RCTs, did not include data on human subjects, chronic diarrhea, or orally administered pharmaceuticals, as well as those that did not refer to SBS or modified SBS were excluded at this stage. Further, the literature search has been updated to August 30th, 2021, and eligibility screening was assessed in reading the full text with the same criteria. Any disagreements over the selection of studies were resolved by a third reviewer (MXY). Detailed data were extracted from each study using a data-extraction form predefined by RevMan 5.3.
Risk-of-Bias Assessment
The risk of bias for each study was assessed independently by 2 reviewers (HW and YNH) using the Cochrane revised risk-of-bias RoB-2 tool. Before assessing, the reviewers were trained, and milestones and quality checks were reviewed by a senior researcher (MXY). Any disagreements were resolved by a third reviewer (MXY).
Statistical Analysis
The extracted efficacy data were entered in RevMan 5.3 for data synthesis and meta-analysis. Continuous data were analyzed using the mean difference (MD) and the 95% confidence interval (CI). Dichotomous data were analyzed using the relative risk (RR) with 95% CIs; and P < .05 indicated statistical significance according to the Cochrane Handbook. 19 For each pooled analysis, a heterogeneity test was performed using the chi-square statistic. The fixed-effect model was utilized to perform meta-analysis, except when I2 > 50%. In such a case, the random-effect model was used. When substantial heterogeneity was found, a subgroup or sensitivity analysis was carried out to identify the cause. 20 Possible publication bias was determined with a funnel plot test if 10 or more studies were included in 1 meta-analysis. A descriptive report was made for any undetermined sources of heterogeneity.
Results
Search Results
The initial database search yielded 5651 records. After screening the titles and abstracts, 157 full-text studies were further evaluated for eligibility criteria. In total, 14 trials met the inclusion criteria (Figure 1).

Flow diagram of systematic review.
Study Characteristics
This study included 14 RCTs with a total of 1158 participants (54% males) from South Korea 13 and China.21-33 The sample size of each trial was relatively small with the largest including 150 participants. 26 Among the 1158 adults who met the chronic diarrhea definition, 605 (52% males) were diagnosed with diarrhea-predominant irritable bowel syndrome according to ROME III guidelines 13,22,24,25,28,31-33; and 148 (59% males) were diagnosed with ulcerative colitis based on the Chinese Medical Association guidelines.21,27 The remaining 405 (59% males) participants had no specific diagnosis.23,26,29,30 The duration of diarrhea ranged from 4 weeks to 2 decades.
Shenling Baizhu San was administrated as an intervention in the form of concentrated granules,13,24,25,31,32 patented herbal medicine, 21 and herbal decoction.22,23,26-30,32 Only 1 trial used a standardized extract whose quality was ensured using a high-performance liquid chromatography array. 13 Four trials13,21,25,33 used the classic SBS formula while 10 trials22-24,26-32 used modified SBS formulas. The duration of treatment ranged from 10 days 29 to 24 weeks. 27 The comparators in the 14 included trials were pinaverium bromide,22,31,32 mesalazine,21,27 otilonium bromide, 13 paroxetine, 24 norfloxacin, 26 montmorillonite,25,29,30,33 sulfasalazine, 23 trimebutine maleate, 28 and placebo. 13 Patient-reported satisfaction, AEs, and quality of life were reported as clinical outcomes. All studies were conducted in a real-world clinical setting, including both outpatient and inpatient hospital departments. The main characteristics of the included studies are summarized in Table 2.
Characteristics of studies included.
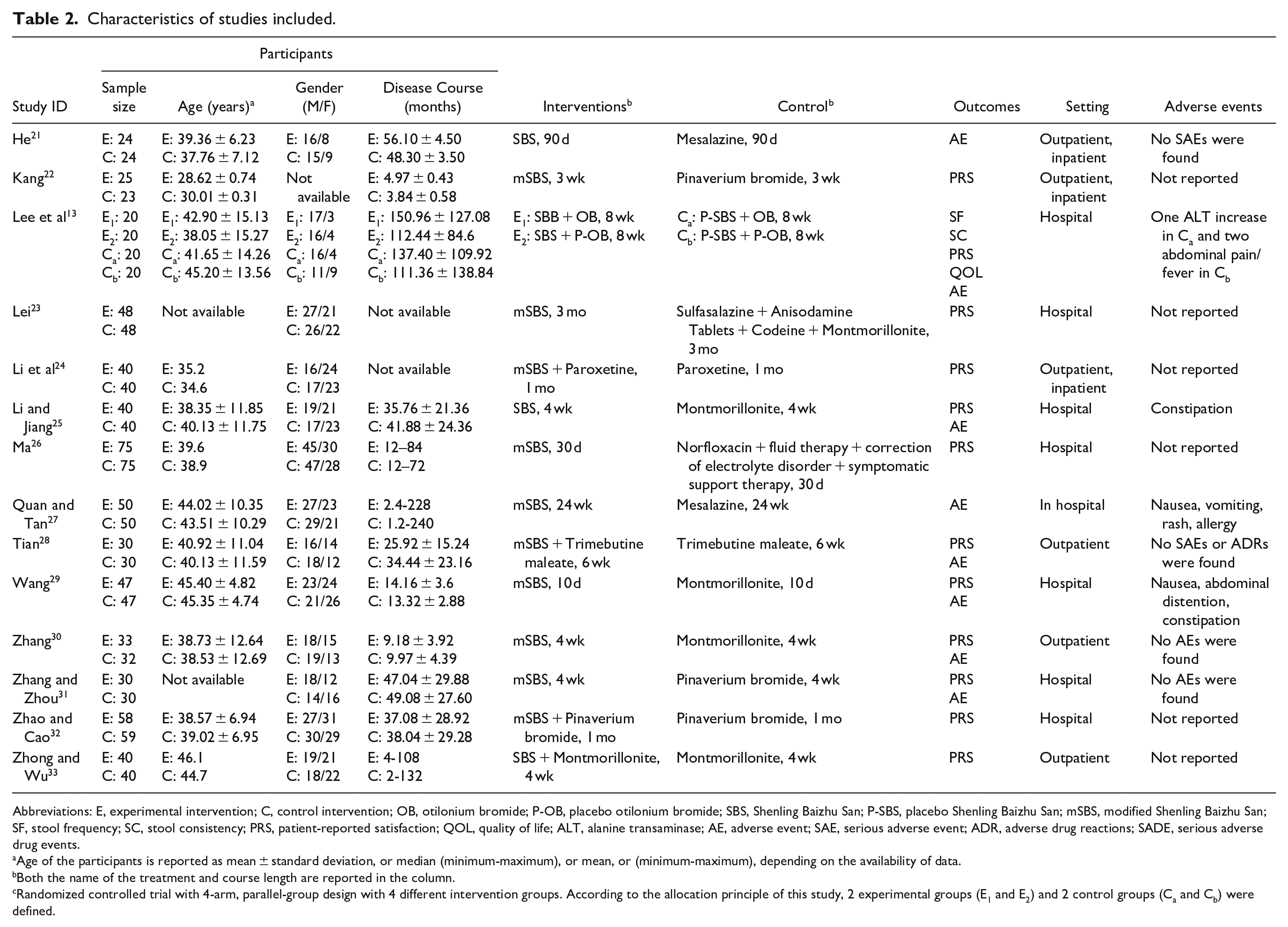
Abbreviations: E, experimental intervention; C, control intervention; OB, otilonium bromide; P-OB, placebo otilonium bromide; SBS, Shenling Baizhu San; P-SBS, placebo Shenling Baizhu San; mSBS, modified Shenling Baizhu San; SF, stool frequency; SC, stool consistency; PRS, patient-reported satisfaction; QOL, quality of life; ALT, alanine transaminase; AE, adverse event; SAE, serious adverse event; ADR, adverse drug reactions; SADE, serious adverse drug events.
Age of the participants is reported as mean ± standard deviation, or median (minimum-maximum), or mean, or (minimum-maximum), depending on the availability of data.
Both the name of the treatment and course length are reported in the column.
Randomized controlled trial with 4-arm, parallel-group design with 4 different intervention groups. According to the allocation principle of this study, 2 experimental groups (E1 and E2) and 2 control groups (Ca and Cb) were defined.
Quality Assessment
Based on the RoB-2 tool, the risk of bias associated with each outcome is reported individually (Figure 2a–c). One study reported stool frequency and stool consistency but was associated with concerns of risk of bias. The bias was mainly caused by an inadequate randomization process and/or improper outcome measurement, or improper reporting of results. For quality of life, the overall risk of bias was low, although only 1 study evaluated quality of life. 13 Both patient-reported satisfaction and AEs were associated with high risk of bias, especially in the missing data, blinding assessment, and outcome reporting domains. Considerable bias also originated from the randomization process.

Risk-of-bias assessments using the revised Cochrane Risk-of-Bias 2 tool.
Outcome Measures
Stool frequency and stool consistency
We chose stool frequency and stool consistency as our primary outcomes because they are objective measurements. Only one of the 14 studies included in this analysis reported these outcomes.
Lee et al, 13 using a 2 × 2 design of SBS or otilonium bromide (OB) versus placebo SBS or placebo OB, did not find statistically significant improvement in stool frequency between the SBS and placebo SBS group but reported a significant difference in stool consistency during week 12 (SBS + OB: −1.33 ± 0.59; SBS + placebo OB: −1.41 ± 0.94; placebo SBS + OB: −0.65 ± 0.61; placebo SBS + placebo OB: −0.80 ± 0.68; P = .003) using the Bristol Stool Form Chart scale.
Patient-reported satisfaction with chronic diarrhea treatment
Pooled analysis from 8 trials13,22,23,25,26,29-31 showed SBS alone is associated with improved patient-reported satisfaction in chronic diarrhea treatment compared to conventional medicine (RR, 2.34; 95% CI, 1.84-2.97; P < .00001; I2 = 0%) (Figure 3a). Further analysis from 5 trials13,24,28,32,33 indicated that SBS in combination with conventional medicine is associated with improved patient-reported satisfaction in chronic diarrhea treatment compared to conventional medicine alone (RR, 2.15; 95% CI, 1.40-3.29; P = .0004; I2 = 0%) (Figure 3b). Heterogeneity test findings are consistent across all trials showing no significant heterogeneity. Of the 14 included studies, only Lee et al 13 used placebo control. The study found that SBS was more likely to positively affect patient-reported satisfaction compared with placebo at week 4 follow-up (P = 0.049); however, the effect was not statistically significant at the end of the 8-week study period. Publication bias with funnel plot test was not conducted because fewer than 10 studies were included in each meta-analysis.
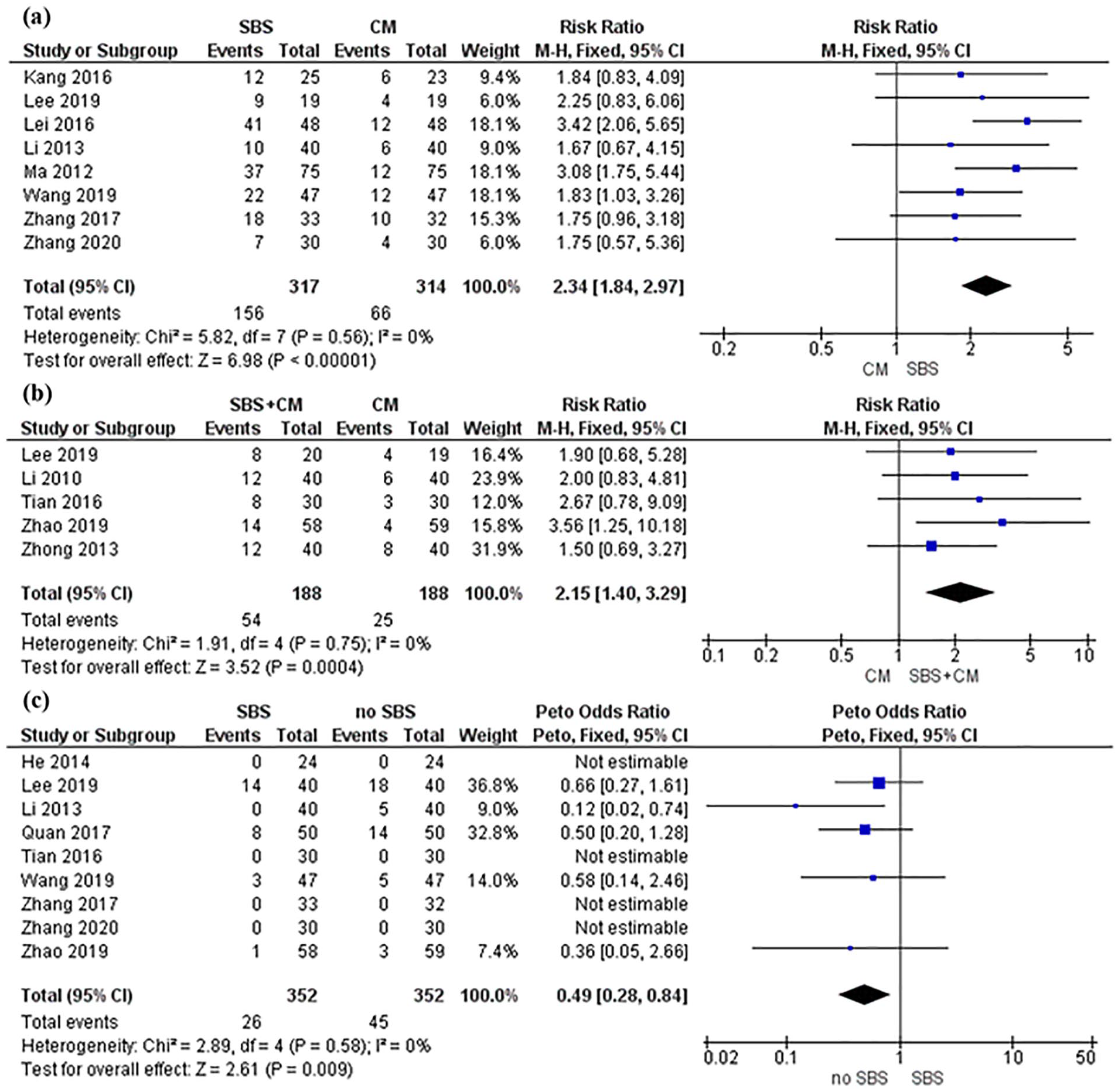
Forest plot of patient-reported satisfaction and adverse events.
Quality of life
Lee et al 13 also reported quality of life as 1 of 8 items in secondary outcomes. The study did not find statistically significant difference when comparing SBS without otilonium bromide versus SBS with otilonium bromide versus placebo (MD, −2.71 ± 2.37, −3.17 ± 2.28, −2.44 ± 2.03, respectively P > .05).
Adverse events (AEs)
Pooled analysis from 9 trials13,21,25,27-32 indicated that SBS is not associated with a higher risk of AEs compared with no SBS (OR, 0.49; 95% CI, 0.28-0.84; P = .009; I2 = 0%) (Figure 3c). However, Lee et al 13 reported serious AEs with 1 case of elevated alanine transaminase in the otilonium bromide plus placebo SBS group, and 2 cases of abdominal pain or fever in the placebo otilonium plus placebo SBS group although the differences between the groups were statistically insignificant (P > .05).
Discussion
Management of chronic diarrhea remains a challenge for clinicians due to patients’ incomplete clinical response to treatment and adverse effects of long-term conventional medicine use. This systematic review analyzed data from 14 RCTs with 1158 participants who had experienced chronic diarrhea for more than 4 weeks. The results show that compared to conventional medicines, treatment with SBS alone or SBS combined with conventional medicines significantly improved patient-reported satisfaction. Furthermore, pooled analysis of safety data showed that SBS did not significantly increase AEs compared with no SBS. However, only 1 trial included our predefined major outcomes—stool frequency and stool consistency— indicating insufficient evidence for determining the effects of SBS on the above outcomes in patients with chronic diarrhea. Although the secondary outcomes of quality of life, satisfaction of symptom recovery, and AEs were collectively evaluated across the included trials, qualitative assessment revealed that these outcomes were associated with at least moderate risk of bias due to methodological limitations.
Clinical Implications
Although no current clinical practice guidelines recommend herbal medicines as therapeutics for chronic diarrhea, several studies provide evidence of chronic diarrhea symptom improvement with herbal medicine use. One systematic review suggests that single herb preparations (curcumin, desert Indian wheat, and wormwood) may improve diarrhea-related symptoms such as chronic diarrhea in patients with gastrointestinal disease. 9 An RCT reported that when compared to placebo, the herbal formula Tong Xie Yao Fang can reduce stool frequency and improve stool consistency in patients with diarrhea-predominant irritable bowel syndrome. 34 In the first systematic review to focus on the herbal formula SBS, we report here that available data favor SBS in significantly improving patient-reported satisfaction of chronic diarrhea treatment—with no increased occurrence of AEs regardless of concurrent use of conventional medicine. We also found insufficient direct evidence linking SBS to improvement in the objective outcome of stool frequency. SBS may improve stool consistency, although there was only 1 study that reported this endpoint.
Mechanistic studies have shown that SBS can modulate the composition of gut microbiota 35 and intestinal absorption as well as the mucosal ultrastructure. 36 Components of SBS, such as Panax ginseng and Atractylodes macrocephala, exhibit numerous biologic effects: Polysaccharides in Panax ginseng can regulate immune cells 37 and promote recovery of mucosa. 38 Atractylenolide III helps attenuate inflammation associated with 2,4,6-trinitrobenzenesulfonic acid-induced colitis. 39 In addition, Lv et al16,40 reported that SBS can enhance the richness and diversity of intestinal microbiota, increase acid metabolism, and reduce diarrhea-related intestinal, immune and infectious diseases.
Based on previous clinical evidence, pathophysiological findings, and evidence synthesized by the current study, SBS appears to be a promising option in the overall management of chronic diarrhea, especially when patient satisfaction is concerned.
Research Implications
This study also revealed methodological issues which should be addressed in future SBS clinical research to obtain more generalizable evidence for the use of SBS in patients with chronic diarrhea. First, most studies are underpowered, and thus, further validation of the effect in an adequately powered sample is needed; and RCT guidelines on randomization and allocation concealment should be followed. Second, diarrhea caused by either functional or organic etiologies is a symptom that is seen in various gastrointestinal disorders. In order to generate generalizable clinical evidence, clinical trials must use the global diagnostic code of gastrointestinal disease under which chronic diarrhea presents in order to reduce heterogeneity and ambiguity of evidence. 2 Third, a standardized SBS intervention with uniform ingredients and dosing regimen is needed to eliminate intervention inconsistencies. 41 Fourth, a valid placebo for SBS should be developed and used consistently. 41 Only 1 trial included in this analysis used a placebo SBS. However, there were validity concerns due to the use of lactose, an ingredient which can affect the digestive system of chronic diarrhea patients. 13 Finally, more targeted and specific outcome measures, such as abdominal pain intensity and stool consistency, should be used as primary endpoints, as per the United States Food and Drug Administration guidance to industry for treating irritable bowel syndrome with diarrhea. 42
Limitations and Strengths
There are several limitations in this study. First, the inclusion of different disease populations with chronic diarrhea symptoms increased heterogeneity, which may hinder the interpretation of data and inhibit the translation of evidence into clinical practice. Further subgroup analysis based on disease category may help address this issue, but it is methodologically limited due to the inadequate number of studies included. Consequently, further in-depth analyses of efficacy data pertinent to clinical practice, such as the optimal treatment dose, administration approaches, and the effectiveness of SBS in comparison with different subclasses of conventional medications, have not been systematically performed, reiterating the need to produce more quality data in the future.
The strength of this study is that it synthesized data from clinical trials to provide efficacy and safety evidence of 1 herbal treatment, SBS, for symptom management of chronic diarrhea rather than investigating several single herbs done in previous studies. This study also focuses on the clinical effectiveness of SBS for symptom relief of chronic diarrhea in real-world practice rather than in an experimental setting.
Conclusion
Shenling Baizhu San is a promising option in the overall management of chronic diarrhea. Current evidence suggests that it may substantially improve patient satisfaction with chronic diarrhea treatment irrespective of conventional medication use. However, the methodological limitations of studies included in this review do not allow for a definitive conclusion on SBS’s effects in reducing stool frequency and consistency in patients experiencing chronic diarrhea. More high-quality RCTs are warranted to evaluate the efficacy of SBS in specific gastrointestinal disease populations with chronic diarrhea symptoms.
Footnotes
Author Contributions
Gary Deng and Jun J. Mao designed the study. Ye Feng, Yi Lily Zhang, Yen-Nien Hou, and Hui Wang collected the data. Hui Wang and Yen-Nien Hou performed statistical analyses. Hui Wang and Yen-Nien Hou wrote the paper. Mingxiao Yang, Colleen M. Smith, Wei Hou and Jun J. Mao critically revised the paper. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jun J. Mao reports grants from Tibet CheeZheng Tibetan Medicine Co. Ltd. and from Zhongke Health International LLC outside the submitted work. Hui Wang, Yen-Nien Hou, Mingxiao Yang, Ye Feng, Yi Lily Zhang, Colleen M. Smith, Wei Hou, and Gary Deng declare no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This manuscript is supported in part by a grant from the National Institutes of Health/National Cancer Institute (P30 CA008748); by the Laurance S. Rockefeller Foundation (supports the MSK Herbal Research and Education in Oncology (HERO) program); and the Translational and Integrative Medicine Research Fund, the latter two at Memorial Sloan Kettering Cancer Center. Hui Wang is supported by a grant from the China Academy of Chinese Medical Sciences in China that supports the program of Evidence-based Research Implementation Scheme Design of Chinese Medicine for Cancer (ZZ13-024-6).