
Abstract
Background:
Branched-chain amino acids (BCAAs; leucine, isoleucine, and valine) are essential amino acids involved in immune responses, and may have roles in protein malnutrition and sarcopenia. Furthermore, certain liver diseases have been associated with a decreased Fischer’s ratio (BCAAs to aromatic amino acids; phenylalanine, tyrosine, and tryptophan). We aimed to evaluate the safety and efficacy of BCAAs use in patients with cancer undergoing surgery.
Methods:
MEDLINE, Embase, and CENTRAL were searched (inception to July 24, 2020) for randomized controlled trials (RCTs) and comparative observational studies in English evaluating BCAAs (alone or in combinations) during the oncological peri-operative period. Study selection, data extraction, and quality appraisal were done in duplicate. RCT risk-of-bias was appraised using Cochrane Risk-of-Bias tool, and observational studies’ quality assessment was conducted with Newcastle-Ottawa Scale. Meta-analyses were conducted when appropriate.
Results:
20 articles were included comprising 13 RCTs and 6 observational cohort studies in 7 reports and 2019 total participants overall. Among 13 RCTs, 77% involved liver cancer. Methodological study quality scored substantial risk-of-bias across most RCTs. Meta-analysis of RCTs found a 38% decreased risk of post-operative infections in BCAAs group compared to controls (RR = 0.62; 95% CI = 0.44 to 0.87; P = .006; number of RCTs, k = 6; total sample size, N = 389; I2 = 0%). BCAAs were also found to be beneficial for ascites (RR = 0.55; 95% CI = 0.35 to 0.86; P = .008; k = 4; N = 296; I2 = 0%), body weight (MD = 3.24 kg; 95% CI = 0.44 to 6.04; P = .02; k = 3; N = 196; I2 = 24%), and hospitalization length (MD = −2.07 days; 95% CI = −3.97 to −0.17; P = .03; k = 5; N = 362; I2 = 59%). No differences were found between BCAAs and controls for mortality, recurrence, other post-operative complications (liver failure, edema, pleural effusion), blood loss, quality of life, ammonia level, and prothrombin time. No serious adverse events were related to BCAAs; however, serious adverse events were reported due to intravenous catheters. No safety concerns from observational studies were identified.
Conclusions:
Branched-chain amino acids during the oncological surgical period demonstrated promise in reducing important post-operative morbidity from infections and ascites compared to controls. Blinded, placebo-controlled confirmatory trials of higher methodological quality are warranted, especially using oral, short-term BCAAs-enriched supplements within the context of recent ERAS programs.
PROSPERO registration:
CRD42018086168.
Keywords
Introduction and Background
Advanced malignant disease paired with persistent physiologic stress from surgery can lead to systemic catabolism. A catabolic state induced by disease and surgery may cause malnutrition and weight loss. This phenomenon is commonly observed in both patients with cancer and those undergoing surgery with an estimated >50% of hospitalized surgical patients having or being at risk for malnutrition, and >50% of patients with cancer experiencing weight loss.1,2 Furthermore, these issues are epitomized most severely in certain subgroups of patients, such as those with liver disease who are more often in a hypercatabolic state. Liver cirrhosis is a common underlying condition among most patients with hepatocellular carcinoma due to the high rate of carrier status of hepatitis B surface antigen. 3 Liver cirrhosis is associated with an increase in basal energy expenditure, and this may be related to increased sympathetic nervous system activity, decreased glycogen stores, and impaired glycogenolysis. 4 Malnutrition is prevalent among cirrhotic patients, and negatively affects prognosis. 5 Liver cirrhosis is often associated with increased protein breakdown in the body and also a decreased protein synthesis response following a meal. 6 In addition, protein-energy malnutrition has been found to be common among patients with end-stage liver disease undergoing liver transplantation. 4
The branched-chain amino acids (BCAAs) leucine, isoleucine and valine are essential amino acids in humans, meaning that an exogenous intake is required for normal cellular function. 1 BCAAs are essential substrates for maintenance of protein synthesis and they are also important regulators of protein turnover. 7 Additionally, the requirement for BCAAs often increases as a result of certain disease states, such as is observed in patients with liver disease. 8 A number of studies have explored the utility of BCAAs and examined multiple possible mechanisms of action, including in liver diseases, and these may elucidate the rationale for their potential use in oncological surgery. A selection of these studies is briefly outlined here, and they suggest that BCAAs’ effects are multifactorial and are suggestive of complex effects in various body systems and pathology.
BCAAs were shown to improve immune system responses in several cell culture and animal feeding studies by facilitating protein synthesis and enhancing lymphocyte function. 9 In cirrhotic patients, BCAAs improved the phagocytic function of neutrophils and natural killer cell activity.10,11 Moreover, a study on chemically-induced cirrhotic rats found that BCAAs had stimulatory effects on the local immune systems of the liver. 12 The immunoregulatory effects of BCAAs may be a result of activating myeloid dendritic cell function, as was demonstrated in 2 ex vivo studies with cirrhotic patients.13,14
BCAAs have also been shown to be crucial for regulating protein metabolism and play a key role in protein synthesis, acting as precursors in the replenishment of alanine and glutamine that are depleted in catabolic states such as prolonged surgical stress and advanced malignant disease. 1 In a chemically-induced rat model of liver injury, BCAAs-enriched nutrients stimulated antioxidant DNA repair. 15 And in a study of food-deprived rats, leucine was unique among the BCAAs in its ability to stimulate protein synthesis in muscle. 16 Furthermore, BCAAs circumvent metabolism by the liver, so they are available in the circulation for protein synthesis, which is advantageous in patients with compromised liver function. 17
There has been a long debate on the usefulness of BCAAs supplementation in patients with liver cirrhosis due to inconsistent results. 18 Advanced cirrhosis is often accompanied by alterations in amino acid metabolism resulting in low plasma levels of BCAAs, whereas the molar concentrations of aromatic amino acids (i.e., phenylalanine, tyrosine, and tryptophan) and methionine are high, resulting in a decreased “‘Fischer’s ratio.”19 -23 Therefore, BCAAs administration might correct this imbalance and confer benefits.6,24,25 In addition to some of the potential effects in cirrhosis already noted above, 2 studies in cirrhotic patients found that BCAAs improved cerebral circulation.26,27
A Cochrane review of 16 randomized trials concluded that BCAAs have a beneficial effect on hepatic encephalopathy. 28 The hypothesis for this effect is that BCAAs compete with aromatic amino acids (AAAs) to cross the blood-brain barrier, and they may facilitate ammonia detoxification.7,29 One in vivo and 2 in vitro studies with cirrhotic rats found that BCAAs promote albumin synthesis in the liver, likely due to a normalization of the low Fischer’s (BCAAs/AAAs) ratio and via mTOR (mammalian target of rapamycin) signal transduction.23,30,31 Finally, preclinical studies have also found that BCAAs may have a role in liver regeneration. Two controlled studies on partially hepatectomized rats showed favourable effects on liver repair with BCAAs administration.32,33 It has been suggested that BCAAs’ effects on liver regeneration are related to their effect on protein synthesis (along with an inhibitory effect on proteolysis), stimulation of hepatocyte growth factor (HGF) secretion, and glutamine production.7,34 Inconsistent results have also been observed regarding possible adverse effects from long-term, high-dose, or excessive BCAAs use, particularly in patients with non-alcoholic fatty liver disease, alcoholism, diabetes, epilepsy, and certain cancers such as pancreatic, ovarian, and breast.35 -41
The wide array and complexity of this literature suggests a need to summarize and critically assess the evidence to inform healthcare providers, researchers and patients. To our knowledge, a comprehensive synthesis of the evidence from human controlled studies on the supplemental use of BCAAs during the oncology peri-operative period has not been published. Our objective is to evaluate the safety and efficacy of the adjunctive use of BCAAs in patients with cancer undergoing surgery by conducting a rigorous systematic review and meta-analysis.
Methods
Protocol details were registered a priori on the PROSPERO website (CRD42018086168). This systematic review was conducted following the main guidelines advised by the Cochrane Collaboration. 42 The report was written following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guidance. 43 This project is part of a large endeavour to prepare a suite of 10 systematic reviews that was based on a prioritization exercise 44 conducted by our institute to refine our research agenda in which preliminary scoping research mapped target evidence points from systematic reviews of the integrative oncology literature. 45 The current report describes the BCAAs stream of this larger research agenda.
The study inclusion criteria (PICOS) for this systematic review were: patients undergoing cancer-related surgery, and evaluating branched-chain amino acids (i.e., leucine, isoleucine, and/or valine), using any route of administration, dose, duration, and formulation (i.e., used alone or in combinations), compared to placebo, active control, or no adjunctive treatment (e.g., usual care, standard nutrition). The primary outcomes of the review were: mortality, cancer treatment response, recurrence, remission, metastasis/disease progression, and stable disease. Secondary outcomes of interest were: adverse events, post-operative infections and other post-operative complications (i.e., ascites/edema/pleural effusion, liver failure/flapping tremor/encephalopathy, ammonia and albumin levels, and prothrombin time), bleeding, length of hospitalization, quality of life/performance status, wound healing, pain, weight/body mass index (BMI)/arm and waist circumferences, fatigue, and cancer biomarkers (e.g., PSA, CEA, AFP, etc.), immune cells, and inflammatory markers levels. Eligible study designs were differentiated between assessing efficacy outcomes and safety signals. Only randomized controlled trials (RCTs) were included for evaluation of efficacy. For only the safety evaluation, a broader evidence base was synthesized of RCTs, non-randomized and quasi-randomized controlled clinical trials, controlled observational cohort and case-control studies. Both published and unpublished reports were eligible. Exclusion criteria were studies with concomitant chemotherapy, radiation or radiofrequency ablation, and non-English reports.
The MEDLINE, Embase, and Cochrane CENTRAL databases were searched for English language records without date limits. The search was initially executed on April 6, 2018 and subsequently 2 update searches were conducted on August 14, 2019 and then on July 24, 2020. The literature search was peer reviewed by an expert librarian (JM) using the Peer Review of Electronic Search Strategies (PRESS) checklist. 46 The MEDLINE search strategy is available in Supplemental Appendix 1. A supplemental gray literature search was also conducted of the clinicaltrials.gov trials registry, the Natural Medicine (formerly Natural Standard) database, and Health Canada’s Natural Health Product Monographs. In addition, the reference lists of all included studies along with of related systematic reviews were scanned for other potentially relevant studies.
Study selection and data extraction were done independently in duplicate. Discrepancies were resolved by a third person or consensus. Screening of titles/abstracts and full-text articles and data extraction were conducted after pilot calibration exercises with the review team. Data items collected into a pre-specified MS Excel form included: study characteristics (study design, sample size, follow-up time, funding source, country, year of publication, etc.), patient characteristics (cancer type/site, cancer stage/severity, age, sex, concomitant therapies, etc.), intervention details (substance, dose, duration, timing around surgery, route of administration, comparator, etc.), and data on relevant outcomes, including variance measures.
Risk-of-bias (ROB) was appraised for RCTs using the original Cochrane Risk-of-Bias tool,47,48 and quality assessment of observational studies was conducted with the Newcastle-Ottawa Scale. 49 This stage of the systematic review was done in duplicate after pilot testing, and discrepancies were resolved by consensus or a third person.
Results were first synthesised descriptively and evidence summary tables created. Meta-analyses were conducted when possible and appropriate using STATA 12. 50 Heterogeneity was first assessed clinically and methodologically, and then statistically with the I2 measure of inconsistency and the P-value of the Chi2 test. A random effects model was employed when there was substantial heterogeneity, a fixed effects model was used for low heterogeneity, and moderate heterogeneity was dealt with following guidance from Cochrane and the Council for International Organizations of Medical Sciences (CIOMS Working Group X).42,51 The main meta-analysis results were presented graphically using forest plots. The summary effect measures used were relative risk (RR) for binary outcomes and mean difference (MD) for continuous outcomes. When appropriate, missing measures of variance were derived or imputed following methods advised by the Cochrane Handbook. 42 Studies with “all-zero” results in all relevant study arms were not included in the meta-analysis for that outcome (i.e., when no events of interest were observed). Zero events in 1 arm were replaced with a fixed value (i.e., 0.5) for the meta-analysis based on accepted methods.42,51 Pre-specified possible subgroup analyses were not feasible due to the limited number of studies in each meta-analysis. 42 Publication bias was explored with visualisation for funnel plot asymmetry, created using Review Manager 5 (RevMan5.4.1).42,52
Results
Included Studies
The literature search for the overarching project of 10 natural health products (NHPs) produced 4171 total records after duplicates were removed. After title and abstract screening, 404 full-text articles were assessed for eligibility. The reasons for study exclusions are described in the study flow diagram in Figure 1. A total of 276 studies were included in the larger project, with 20 relevant BCAAs articles included here reporting on 19 studies. These comprised 13 RCTs53 -65 and 6 observational cohort studies in 7 reports66 -72 on BCAAs, and included 2019 total participants overall across the studies.

Study flow diagram.
Tables 1 and 2 report the study and patient characteristics of the included RCTs and observational cohort studies, respectively. Tables 3 and 4 outline details of the interventions and comparators utilized in the RCTs and observational cohort studies, respectively. Table 5 presents summary characteristics across all studies. The RCTs were published from 1984 to 2016, with 7 (54%) since 2010. All except 1 were conducted in Asia, and 62% of the RCTs were from Japan. Five of the RCTs (38%) did not report funding source, while 5 were publicly funded. Six RCTs (46%) had sample sizes <50, while the largest 3 had 145, 124, and 96 total randomized participants.
Characteristics of Included RCTs.

Abbreviations: BCAAs, branched-chain amino acids; HCC, hepatocellular carcinoma; meds, medications; mets, metastasis; NA, not applicable; NR, not reported; TNM, tumor node metastasis; tx, treatment; UICC, Union for International Cancer Control; var, variance; y, year.
Number randomized.
Denotes how long after surgery the BCAAs were started.
One arm was not randomized so that comparator was not included.
According to Liver Cancer Study group of Japan.
Characteristics of Included Observational Studies.

Abbreviations: BCAAs, branched-chain amino acids; HCC, hepatocellular carcinoma; HPB, hepato-pancreato-biliary; NA, not applicable; NR, not reported; tx, treatment; var, variance; y, year.
Denotes how long after surgery the BCAA was started.
Only the 2 ERAS groups were included (not the pre-ERAS comparisons).
Companion report is Okabayashi, 2008b. 71
Interventions and Comparators Evaluated in the RCTs.

Abbreviations: AAs, amino acids; admin, administration; BCAAs, branched-chain amino acids; BID, twice per day; D5W, 5% dextrose in water; IV, intravenous; MCTs, medium-chain triglycerides; NA, not applicable; NHPs, natural health products; NS, normal saline; PN, parenteral nutrition; Post-op, post-operatively; Pre-op, pre-operatively; TID, 3 times per day; TPN, total parenteral nutrition; tx, treatment.
Exposures and Comparators Evaluated in the Observational Studies.

Abbreviations: AAs, amino acids; admin, administration; BCAAs, branched-chain amino acids; BID, twice per day; IV, intravenous; LCT, long-chain triglycerides; MCT, medium-chain triglycerides; NA, not applicable; Post-op, post-operatively; Pre-op, pre-operatively; TID, 3 times per day; tx, treatment.
Only the 2 ERAS groups were included (not the pre-ERAS comparisons).
Summary Characteristics of Included Studies.
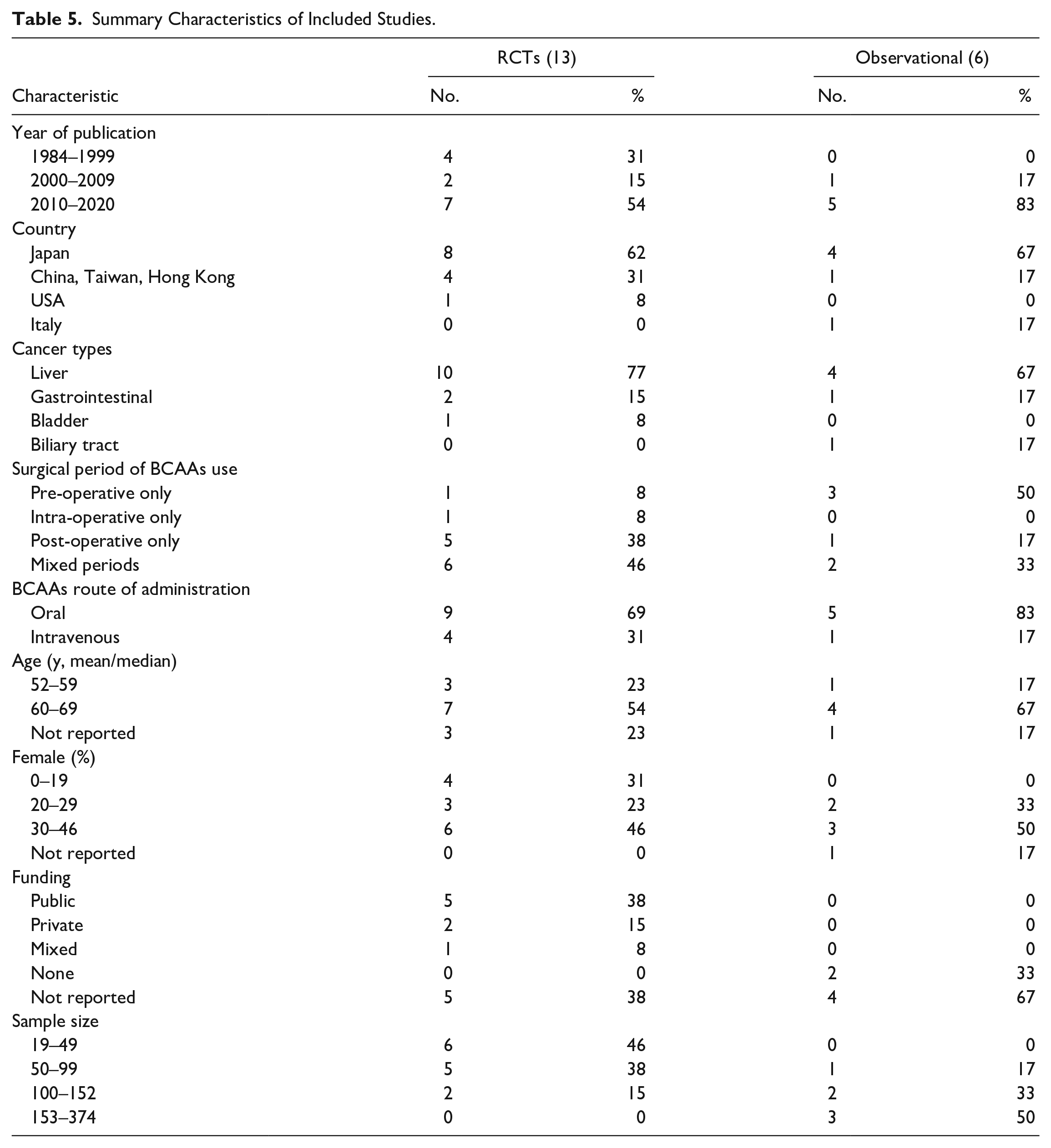
The large majority of the RCTs dealt with liver cancer (10/13, 77%), 2 were on gastrointestinal cancer,63,65 and 1 on bladder cancer. 54 Mean (or median) ages of the study populations were from 53 to 67 years old, and all of the RCTs had a predominantly male population. Nine RCTs (69%) evaluated oral intake of BCAAs and 4 (31%) administered (parenteral) BCAAs intravenously in hospital. Duration of treatment use in the RCTs ranged from intra-operatively (single intravenous administration) up to a maximum duration of 13 months (oral administration). Forty-six percent (6/13) evaluated BCAAs administration during both the pre-operative and post-operative periods, while 5 RCTs (39%) gave BCAAs only post-operatively.
Risk-of-Bias and Methodological Quality
Figure 2 presents the RCT risk-of-bias assessments per study using the Cochrane tool, and Figure 3 reports the aggregate summary across RCTs. The methodological quality appraisals revealed an overall substantial risk-of-bias across most of the included studies. Ten (77%) of the RCTs were judged to possess a high risk-of-bias for at least 1 domain among the 7 assessment elements. The other 3 (23%) RCTs58,63,64 had an unclear risk-of-bias for at least 1 domain, while they scored a low risk-of-bias on 4 or more domains.

Risk-of-bias appraisal of each RCT.
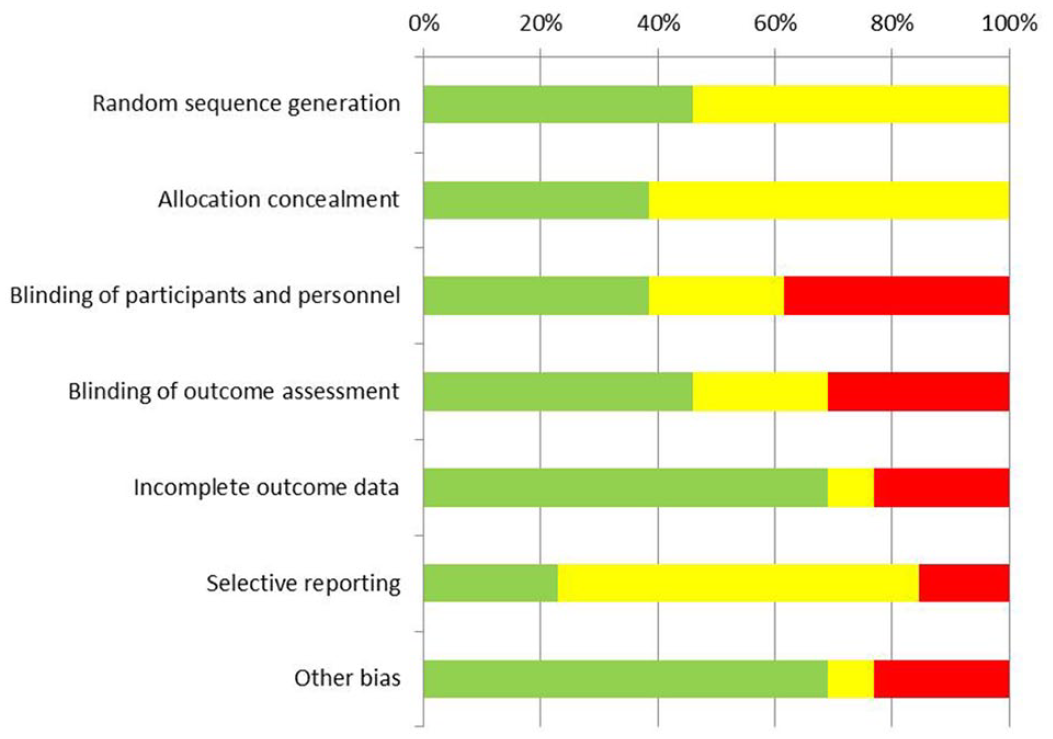
Aggregate risk-of-bias across studies.
The risk-of-bias element that scored worst among the (10/13) RCTs was selective reporting (Figure 3). Most of the RCTs did not report on allocation concealment and random sequence generation, suggesting potential selection bias. The majority of the studies were unclear or high risk regarding blinding of participants and personnel and blinded outcome assessment, indicating performance and detection biases. Additionally, 4 of the 13 (31%) RCTs scored high/unclear risk for incomplete outcome data, suggesting possible attrition bias.
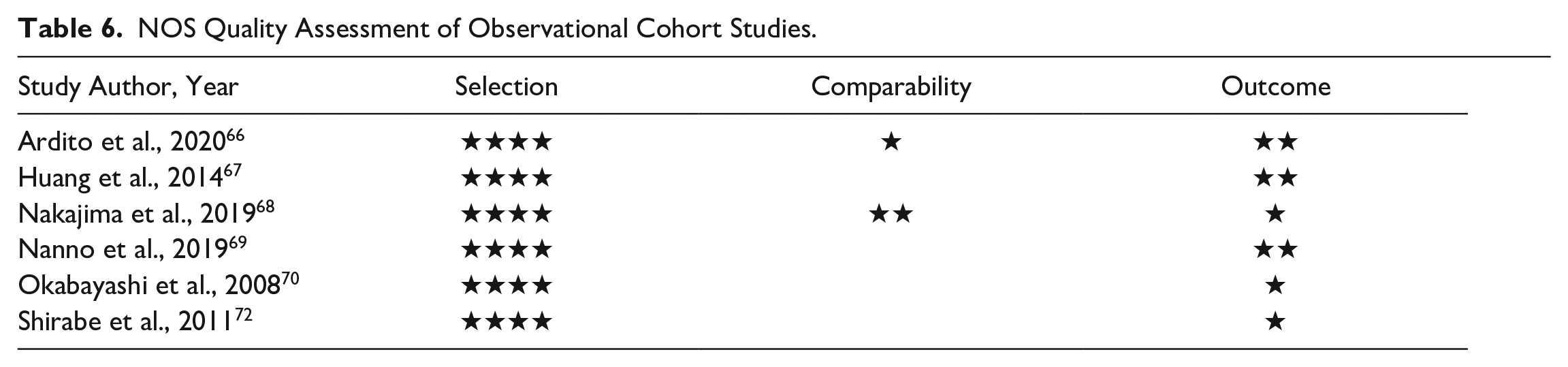
Table 6 presents the quality assessment of the observational cohort studies using the Newcastle-Ottawa Scale (NOS). Overall, these were of low methodological quality. In particular, the “comparability of cohorts on the basis of the design or analysis” item was inadequate in the majority (4/6; 67%) of studies that did not control for important potential confounding. Two (33%) observational studies66,68 used propensity score matching, and both of these studies received higher NOS scores of 7 out of 9 total stars.
NOS Quality Assessment of Observational Cohort Studies.
Mortality and Recurrence
Comprehensive tables of outcome results per study from the RCTs and observational cohort studies are reported in the journal’s online Supplemental Appendices 2 and 4, respectively.
Supplemental Table S2.1 describes the RCT results per study for mortality data. This outcome was evaluated in 9 (69%) of the included RCTs. Follow-up times varied substantially from 1 week to 4 years. Three RCTs reported no deaths, so 6 RCTs were included in the meta-analysis. Figure 4 displays the forest plot of the meta-analysis. There was low statistical heterogeneity between studies (I 2 = 0%) in the mortality outcome, and a fixed effects model was utilized. There was no evidence of a difference between the BCAAs and control groups for mortality (number of studies, k = 6; total sample size, N = 497; RR = 0.98; 95% CI, 0.72 to 1.34; P = .92).

Forest plot of RCTs meta-analysis on mortality.
Supplemental Table S2.2 presents the results on cancer recurrence, which was reported in 5 RCTs. Follow-up times varied from 12 to 36 months. Figure 5 provides the forest plot of the meta-analysis. There was moderate statistical heterogeneity between studies (I2 = 39%) in this outcome, and a fixed effects model was utilized. There was no evidence of a difference between the BCAAs and control groups for recurrence (k = 5; N = 371; RR = 0.83; 95% CI, 0.64 to 1.07; P = .15). Similar results were also found with a random effects model (Figure 5).

Forest plot of RCTs meta-analysis on recurrence.
None of the included RCTs specifically reported extractable data on the following other primary outcomes of the review: cancer treatment response, metastasis, remission, and stable disease.
Liver Failure
Outcome measures of liver failure, including post-operative encephalopathy and flapping tremor, were reported in 4 RCTs (Supplemental Table S2.3). Follow-up ranged from 1 to 1.4 years. One RCT had no events, and another 60 reported the percentage change from baseline in flapping tremor at 12 months was borderline significant (P = .047) favouring BCAAs compared to usual care. The other 2 RCTs were included in the meta-analysis of post-operative liver failure. There was low statistical heterogeneity (I2 = 22%), and a fixed effects model was utilized. There was no evidence of a difference between the BCAAs and control groups for liver failure (k = 2; N = 121; RR = 1.22; 95% CI, 0.39 to 3.76; P = .73).
Post-Operative Infections
Table 7 below presents the RCT results for all post-operative infections, which were reported on in 7 RCTs. Study follow-up times varied from 7 to 513 days. Infections reported included: wound infection, sepsis, biliary fistula (septic), central-catheter sepsis, infected ascites, post-operative pulmonary infection, post-operative subphrenic abscess, urinary tract infection, surgical site infection, liver abscess, infectious complications, chest infection, intra-abdominal abscess, and pneumonia.
Post-Operative Infections (RCTs).

Abbreviations: BCAAs, branched-chain amino acids; No., number; NR, not reported; PN, parenteral nutrition; TPN, total parenteral nutrition; tx, treatment.
Number of patients with infections was 11 (BCAAs) versus 22 (Control) total since some had multiple infections.
Defined as positive culture of the catheter tip in the presence of a febrile episode.
Defined as presence of pneumonic or atelectatic changes on radiographs associated with a positive sputum culture.
Defined as a collection of pus with or without necrotic material associated with a positive bacterial culture.
Defined as erythema and induration of a wound associated with purulent discharge that was positive on bacterial culture.
Median value.
One study reported no infections, so the remaining 6 RCTs were included in the meta-analysis. Figure 6 presents the forest plot of the meta-analysis. There was low statistical heterogeneity between studies (I2 = 0%), and a fixed effects model was utilized. The BCAAs group had a 38% decreased risk of post-operative infections compared to controls (k = 6; N = 389; RR = 0.62; 95% CI, 0.44 to 0.87; P = .006).

Forest plot of RCTs meta-analysis on post-operative infections.
Ascites, Pleural Effusion, and Edema
Ascites, pleural effusion, and edema results were reported in 5, 4, and 2 RCTs, respectively (Supplemental Table S2.4). Follow-up times varied from 7 to 513 days across these studies. One RCT 64 had 1 case of post-operative edema at 12 months in the BCAAs group compared to none in the controls (P > .05), and the other study 60 reported no change from baseline in edema in both groups.
One RCT, 60 which only reported percentage change from baseline, found ascites within the first 3 months was significantly less common in the BCAAs group compared to usual care (P < .0001), however, this effect was not statistically significant during the remainder of the 12-month follow-up. The other 4 RCTs were able to be included in a meta-analysis, and these all included patients with liver cancer. Figure 7 provides the forest plot for ascites, which had low statistical heterogeneity between studies (I2 = 0%) so a fixed effects model was utilized. The BCAAs group had a 45% decreased risk of ascites compared to controls (k = 4; N = 296; RR = 0.55; 95% CI, 0.35 to 0.86; P = .008).

Forest plot of RCTs meta-analysis on ascites.
The meta-analysis for pleural effusion had low statistical heterogeneity between the RCTs (I2 = 0%) and a fixed effects model was run (Supplemental Appendix Figure S3.1). There was no evidence of a difference between the BCAAs and control groups for pleural effusion (k = 4; N = 269; RR = 0.75; 95% CI, 0.47 to 1.18; P = .21).
Hospitalization Length
Supplemental Table S2.5 presents the RCT results on the length of stay in hospital, which was reported in 5 of the included RCTs. Figure 8 provides the forest plot of the meta-analysis. There was substantial heterogeneity between studies (I2 = 59%) and a random effects model was employed. Hospital length of stay was found to be 2 days shorter in the BCAAs group compared to controls (k = 5; N = 362; MD = −2.07 days; 95% CI, −3.97 to −0.17; P = .03).

Forest plot of RCTs meta-analysis on hospital length of stay.
Quality of Life
Supplemental Table S2.6 reports results of 2 RCTs that reported on quality of life measures. One study 60 using the Karnovsky scale found the percentage change from baseline in the rate of performance status ≤70 at 12 months was borderline significant (P = .047) in favour of the BCAAs group compared to usual care. The other RCT, 62 which used the SF-36 health survey, only reported on intra-group changes compared to their pre-operative scores (not between group differences). At the 12 month follow-up time point, the control group had no significant change in any of the 8 parameters, while in the BCAAs group all parameters improved significantly compared to baseline.
Anthropometrics
Supplemental Table S2.7 presents the RCT anthropometric measurements results reported across 6 RCTs in total. Follow-up times ranged from 1 week to 1 year. All 6 RCTs reported on body weight, and 4 of them additionally presented results for arm circumference, BMI, and triceps skin-fold thickness outcomes. Three of the RCTs54,55,60 were not feasible for inclusion in the body weight meta-analysis (due to outcome measure or variance reporting). Two of these RCTs55,60 found the BCAAs group had significantly greater body weight compared to controls, while one study 54 reported there was no difference found between groups (Table S2.7). Figure 9 presents the forest plot of the meta-analysis on body weight. There was low statistical heterogeneity (I2 = 24%), and a fixed effects model was utilized. Body weight was 3 kg greater in the BCAAs group compared to controls (k = 3; N = 196; MD = 3.24 kg; 95% CI, 0.44 to 6.04; P = .02).

Forest plot of RCTs meta-analysis on body weight.
Immune Cells and Inflammatory Markers
Supplemental Table S2.8 presents the RCT results for the immune cells and inflammatory markers outcomes, which were reported on in 2 RCTs. Follow-up times were from 7 to 15 days. One study 55 found no difference between groups for serum IgA, IgG, or IgM levels (P > .05). The other RCT 63 reported significant improvements in C-reactive protein levels (P = .004) and WBC counts (P = .002) in the BCAAs group compared to controls.
Ammonia Level and Prothrombin Time
Supplemental Table S2.9 presents ammonia level results reported in 2 RCTs. Supplemental Appendix Figure S3.2 provides the forest plot of the meta-analysis. There was low statistical heterogeneity between the studies (I2 = 0%) and a fixed effects model was used. There was no evidence of a difference between the BCAAs and control groups for ammonia level (k = 2; N = 156; MD = 1.61 mcg/dL; 95% CI, −6.24 to 9.47; P = .69).
Supplemental Table S2.10 reports the results for prothrombin time, which was reported in one study. 58 This RCT found there was no difference between groups (P > .05).
Blood Loss
Supplemental Table S2.11 lists the surgical blood loss data from 6 RCTs after BCAAs administration. Figure 10 presents the forest plot of the meta-analysis. There was high heterogeneity between studies (I2 = 83%), therefore a random effects model was employed. No evidence of a difference was found between the BCAAs and control groups for peri-operative blood loss (k = 6; N = 383; MD = 208.34 ml; 95% CI, −107.76 to 524.44; P = .20). These inconsistent results also included 1 outlier study 55 of surgeries performed in the early 1990s that used a multi-component formulation including IV lipids, vitamins, etc. (Table 3).
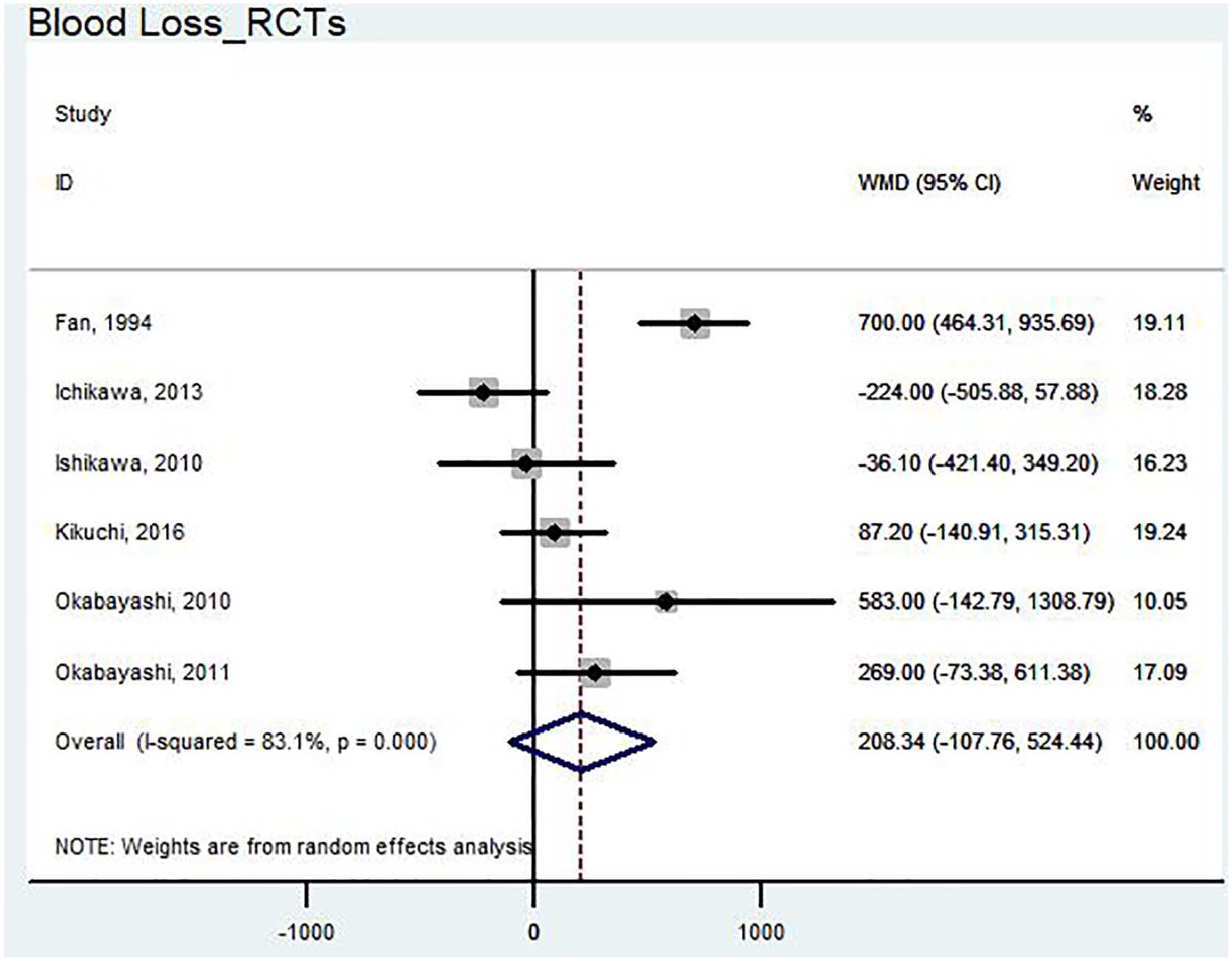
Forest plot of RCTs meta-analysis on blood loss.
Other Complications and Adverse Events
Table 8 presents the RCT results per study for other post-operative complications not already reported on above and adverse events. One RCT 55 reported 2 (3%) adverse events related to the use of nutritional intravenous catheters implanted in the superior vena cava, 1 each of pre-operative catheter sepsis and of a badly positioned catheter pre-operatively.
Other Complications and Adverse Events (RCTs).

Abbreviations: AAs, amino acids; AE, adverse events; BCAAs, branched-chain amino acids; IV, intravenous; N, number; NR, not reported; OC, other complications not already reported on above; PN, parenteral nutrition; TPN, total parenteral nutrition; tx, treatment.
2 patients experienced occasional diffuse abdominal pain after ingestion and 1 suffered from transient diarrhoea, which all stopped spontaneously.
Intervention was started 7 days after surgery in this RCT.
Regarding adverse events related to BCAAs, Fan et al., 55 who administered a parenteral nutrition combination of amino acids, lipids, dextrose, vitamins and trace minerals, reported 2 (3%) cases of post-operative hyperglycemia and diuresis in the absence of a history of diabetes mellitus. Nagasue 60 reported that 7/67 (10%) patients experienced adverse events with the oral Aminoleban EN formula, including nausea and vomiting in 4, diarrhea in 1, abdominal distension in 1, and hypertension in 1. Three (5%) of these patients discontinued BCAAs due to side effects. Meng et al. 59 found no significant adverse reactions associated with oral Aminoleban EN, and 3 (14%) adverse events deemed by the authors as not significant, including occasional diffuse abdominal pain after ingestion and transient diarrhea, which all resolved spontaneously. Four RCTs56,61,62,64 reported that there were no side effects to the BCAAs interventions out of 100 total patients. Six RCTs did not report on adverse events related to BCAAs.
None of the RCTs reported usable data on the secondary outcomes of fatigue, pain, general wound healing, and cancer biomarker levels. Albumin level was removed as a review outcome since in several studies it was unclear whether exogenous albumin had been administered (i.e., participant contamination) during the surgical period.
Observational Studies
Supplemental Appendix Table S4.1 includes the observational study results for mortality, which was reported on in all 6 cohort studies. There was no evidence of a safety concern regarding mortality from these observational studies.
One observational study reported on liver failure (Supplemental Table S4.2), and there was no evidence of a safety concern regarding liver failure in this cohort (P = .37).
Supplemental Table S4.3 outlines the observational study results for post-operative infections, which were reported on in 3 studies. There was no evidence of a safety concern regarding infections from the observational data.
One observational study reported on ascites (Supplemental Table S4.4). There was no evidence of a safety concern regarding ascites in this cohort.
Supplemental Table S4.5 includes the observational study results for hospitalization length, which was reported on in 4 studies. There was no evidence of a safety concern regarding hospital length of stay from these cohorts.
One observational study reported on anthropometrics (Supplemental Table S4.6), and there was no evidence of a safety concern regarding BMI.
Supplemental Table S4.7 includes the observational study results for lymphocyte counts, which were reported on in 2 studies. There was no evidence of a safety concern for lymphocyte counts.
Surgical blood loss results were reported on in the 4 observational studies presented in Supplemental Table S4.8. There was no evidence of a safety concern for blood loss from these cohorts.
Table 9 provides the observational cohort results per study for other post-operative complications not already reported on above and adverse events. None of the 6 observational studies reported on adverse events related to BCAAs. Meta-analyses of the observational studies were not feasible due to heterogeneity.
Table of Other Complications and Adverse Events in Observational Studies.

Abbreviations: AE, adverse events; BCAAs, branched-chain amino acids; ISGLS, International Study Group of Liver Surgery; ISGPF, International Study Group of Pancreatic Fistula; mos, months; N, number; OC, other complications not reported on above; PN, parenteral nutrition; TPN, total parenteral nutrition; tx, treatment.
Publication Bias
Figure 11 presents the funnel plot for the largest meta-analysis outcome, post-operative infections, which contained 6 RCTs. Statistical tests for funnel plot asymmetry (e.g., Egger’s test) were not executed as this requires at least 10 studies in a meta-analysis. 42 Visualization revealed asymmetry of the funnel plot indicating small-study effects, which may be due to publication (i.e., non-reporting) bias. 42 Additionally, the outlying point was from a small study with a high risk-of-bias. 57
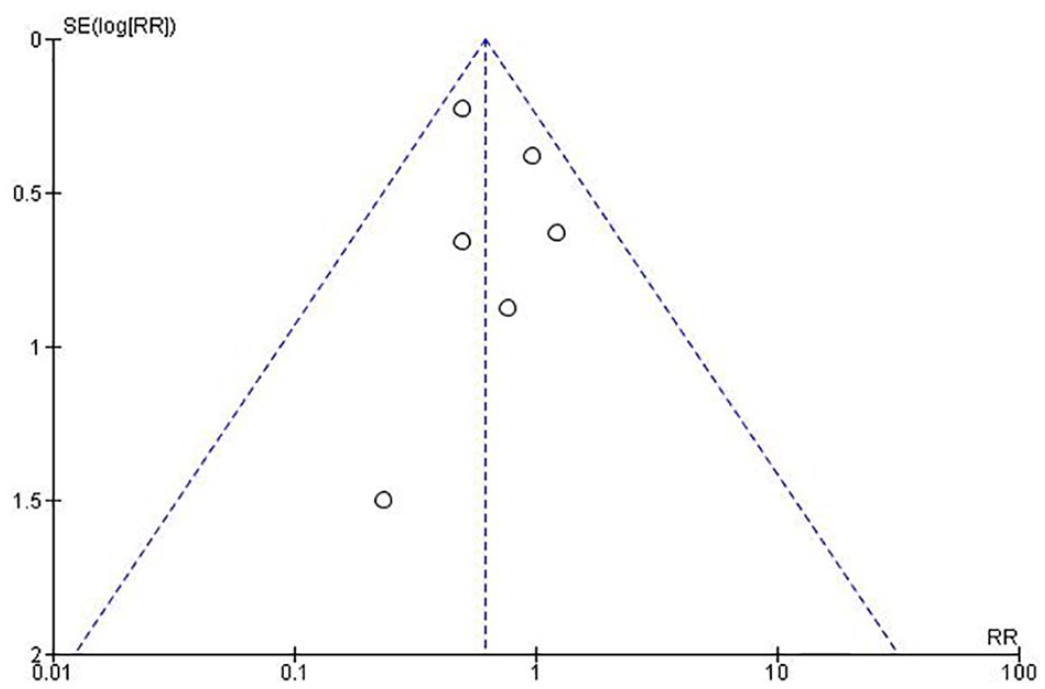
Funnel plot for post-operative infections.
Discussion
This comprehensive systematic review included 20 reports comprising 2019 total participants, of which 13 RCTs were synthesized to evaluate BCAAs efficacy. Our results showed encouraging effects of BCAAs intake in patients with cancer undergoing surgery, especially regarding important surgical morbidity. The risk of post-operative infections decreased 38% (RR = 0.62; 95% CI = 0.44 to 0.87), and there was a 45% reduction in the risk of ascites (RR = 0.55; 95% CI = 0.35 to 0.86) compared to controls. Additionally, promising results were found for body weight (MD = 3.24 kg; 95% CI = 0.44 to 6.04) and also hospital length of stay (MD = −2.07 days; 95% CI = −3.97 to −0.17). None of the included RCTs provided data on: cancer treatment response, metastasis, remission, stable disease, fatigue, pain, general wound healing, and cancer biomarker levels. The other review outcomes did not have evidence of an effect with BCAAs use among these 13 RCTs. The methodological study quality of most of the included RCTs was at high risk-of-bias, thereby weakening the strength of the findings. Our results clearly demonstrate that further investigation of BCAAs in blinded, placebo-controlled trials is warranted.
For the safety evaluation, observational data from 6 identified comparative cohort studies were also included with the aim of providing a broader safety analysis. No BCAAs safety concerns were identified regarding the review outcomes of interest among the 20 reports. One RCT 55 reported 2 (3%) adverse events related to the use of nutritional intravenous catheters, which were implanted in the superior vena cava (catheter sepsis and badly positioned catheter). No serious adverse events were reported related to BCAAs. However, adverse events reporting was generally inadequate, with almost half (6/13) of the RCTs and all 6 observational studies not reporting on adverse events related to BCAAs. The adverse events reported related to BCAAs, or to the investigational combinations containing BCAAs, included: hyperglycemia, diuresis, nausea, vomiting, diarrhea, abdominal distension, hypertension, and abdominal pain.
The strengths of this systematic review and meta-analysis include a priori protocol registration, execution of a comprehensive and up-to-date literature search, critical appraisal of study quality, application of rigorous statistical methods, and transparent reporting of the methods and results. The main review-level limitation of the methodology was the exclusion of non-English reports and not searching Asian databases, which may have introduced language bias. The main study-level limitation of the results was the overall low methodological quality of the evidence due to most of the included RCTs being at high risk-of-bias, thereby weakening the strength of the findings even though clinically relevant effect sizes were found. Additionally, funnel plot asymmetry indicated small-study effects, which may be due to publication (i.e., non-reporting) bias and the inclusion of a small study 57 with a high risk-of-bias. Furthermore, the appraisal of the observational cohort studies also revealed low methodological quality overall. Also, there was generally poor study reporting on adverse events related to BCAAs. In addition, there was substantial heterogeneity observed between the various interventions, comparators, and durations of treatment evaluated. The conduct of exploratory subgroup analyses was precluded due to potential multiplicity issues. Finally, the large majority (77%) of the RCTs were involving liver cancer.
Hospital peri-operative care has undergone significant changes over the past few years, in particular due to the gradual implementation of new Enhanced Recovery After Surgery (ERAS©) guidelines aimed at improving recovery after major surgery and reducing hospital and societal costs.73 -76 ERAS programs are multimodal, interdisciplinary and standardized pathways that are patient-focused and include 23 standard items for a variety of surgical specialties. In 2016, ERAS guidelines were published for liver surgery. 77 Liver cancer surgery is a challenging procedure having statistics of major morbidity of ~27% and an overall mortality risk of up to 5%. 78 Four of the ERAS topics are relevant to our BCAAs review: peri-operative nutrition, pre-operative fasting and carbohydrate load, nasogastric intubation, and post-operative nutrition and early oral intake. Specifically, these new guidelines recommend against prolonged pre-operative fasting (>6 hours for solids), allowing clear fluids up to 2 hours before surgery. 77 They also continued current guidance advice for patients at risk of malnutrition to administer 7 days of oral nutrition supplements pre-operatively. 79 In addition, the 2016 guidelines advise early oral intake of solid foods post-operatively (day 1), with oral nutritional supplementation being reserved for malnourished patients or those with prolonged fasting due to complications and preference in these cases is given to enteral over parenteral nutrition. 77 However, current clinical practice recommendations for the optimal specific types of oral nutritional supplements are unclear. Our results clearly demonstrate that short-term oral BCAAs-enriched nutritional supplements warrant further investigation within the context of recent ERAS protocols, particularly in patients at risk of malnutrition.
To our knowledge, a comprehensive and rigorously executed systematic review of evidence from human controlled studies that also includes methodological appraisal on the safety and efficacy of BCAAs intake during the oncology peri-operative period has not been published. A 2012 Cochrane systematic review of nutritional interventions before or after liver transplantation found that the use of parenteral nutrition plus BCAAs had benefits compared with standard parenteral nutrition. 80 Another Cochrane review of 16 RCTs that was published in 2017 concluded that BCAAs have a beneficial effect on hepatic encephalopathy compared to controls. 28 Moreover, updated guidance from the European Society for Clinical Nutrition and Metabolism (ESPEN) recommends that patients with advanced cirrhosis can use oral BCAAs long-term, and it also states that in hepatic encephalopathy BCAAs-enriched formulas can be used post-operatively when enteral nutrition is needed. 81
Conclusion
The use of branched-chain amino acids during the oncological surgical period showed encouraging effects in reducing important post-operative morbidity from infections and ascites compared to controls. Furthermore, beneficial effects were also found for body weight and hospitalization length. No other effects were observed for the additional systematic review outcomes. Blinded, placebo-controlled confirmatory trials of higher methodological quality are warranted, especially using short-term oral BCAAs-enriched nutritional supplements in patients at risk of malnutrition within the context of recent ERAS programs.
Supplemental Material
sj-pdf-1-ict-10.1177_1534735421997551 – Supplemental material for Are Supplemental Branched-Chain Amino Acids Beneficial During the Oncological Peri-Operative Period: A Systematic Review and Meta-Analysis
Supplemental material, sj-pdf-1-ict-10.1177_1534735421997551 for Are Supplemental Branched-Chain Amino Acids Beneficial During the Oncological Peri-Operative Period: A Systematic Review and Meta-Analysis by Elise Cogo, Mohamed Elsayed, Vivian Liang, Kieran Cooley, Christilynn Guerin, Athanasios Psihogios and Peter Papadogianis in Integrative Cancer Therapies
Footnotes
Acknowledgements
We wish to sincerely thank Dr. John and Mrs. Thea Patterson, Dr. Jessie McGowan, and Dr. Nancy Rawling.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.