
Abstract
Background:
Subjects with head and neck cancer (HNC) often experience post-treatment side effects, particularly radiation-induced oral mucositis (RIOM). This study aimed to explore the association of Chinese herbal medicine use with the sequent risk of RIOM among them.
Methods:
This cohort study used a nationwide health insurance database to identify subjects newly diagnosed with HNC, aged 20 to 60 years, who received treatment between 2000 and 2007. Among them, a total of 561 cases received CHM after HNC onset (CHM users); the remaining 2395 cases were non-CHM users. All patients were followed to the end of 2012 to identify any treatment for RIOM as the end point. Cox proportional hazards regression was used to compute the adjusted hazard ratio (aHR) of RIOM by CHM use.
Results:
During the follow-up period, 183 CHM users and 989 non-CHM users developed RIOM at incidence rates of 40.98 and 57.91 per 1000 person-years, respectively. CHM users had a lower RIOM risk than the non-CHM users (aHR: 0.68; 95% Confidence Interval: 0.58-0.80). The most potent effect was observed in those taking CHM for more than 1 year. Use of Baizhi, Danshen, Shao-Yao-Gan-Cao-Tang, Gan-Lu-Yin, Huangqin, Shu-Jing-Huo-Xue-Tang, and Xin-Yi-Qing-Fei-Tang, was significantly related to a lower risk of RIOM.
Conclusion:
Findings of this study indicated that adding CHM to conventional clinical care could be helpful in protecting those with HNC against the onset of RIOM. Further clinical and mechanistic studies are warranted.
Introduction
Head and neck cancer (HNC), affecting the oral cavity, pharynx, and larynx, are the eighth most prevalent cancer type in the world. 1 Radiotherapy is a mainstay of treatment administered to more than two-thirds of HNC patients. 2 Nevertheless, they often encounter a common and debilitating complication characterized by pain and erythema or ulceration of the oral mucosa due to altered inflammatory response, namely radiation-induced oral mucositis (RIOM). 3 Research showed that severe RIOM may lead to swallowing impairment that impacts nutritional intake and treatment noncompliance, thus leading to placement of feeding tubes and hospitalization. 4 Faced with these dire adverse effects, it is important to seek out appropriate treatments that could lessen the likelihood of RIOM or reduce its severity.
To date, no definite intervention has been identified to efficiently prevent RIOM incidence. Though some supportive modalities, included improving oral hygiene, eliminating local irritants, and frequent rinsing with combination therapies have been noted; all of these appeared to merely reduce either the discomfort or the severity of symptoms after RIOM onset.5,6 However, based on the assertion that prevention is preferable to mitigation, efforts should be made to identify active interventions which could reduce the risk of RIOM and minimize its associated morbidity after diagnosis of HNC.
As of now, Chinese herbal medicines have recently attracted global attention due to the reliable therapeutic efficacy toward chronic diseases, especially in managing the symptoms associated with RIOM. 7 A herbal formula, Hangeshashinto, was found to be related to the reduced infiltration of neutrophils and ofcyclooxygenase-2 in irradiated mucosa, alleviating the discomfort caused by RIOM.8,9 Also worth noting is the fact that previous reports usually are based on relatively small samples of patients, thus threatening findings’ representativeness. 7 This paucity of data may be an obstacle to facilitating treatment and prognosis in such cases. Accordingly, this study aimed to assess the association over time of CHM use with the onset of RIOM among HNC patients, using a nationwide medical claims database.
Methods
Data Source
For this study, we used a publicly-released cohort dataset from the Longitudinal Health Insurance Database (LHID) in Taiwan. The LHID is a sub-dataset of the National Health Insurance (NHI) program made up of 1 million randomly sampled patients from 1996 to 2012. Constructed using a multistage stratified systematic sampling method, it is a representative sample, on both sex and age, of these 1 million insured individuals and of the general population of Taiwan.10,11 This cohort database includes (i) personal information; (ii) health insurance claims data; (iii) diagnostic codes; (iv) prescription drugs registry; (v) socioeconomic data; and (vi) medical examination information on persons covered under the NHI program. This study was conducted in accordance with the Helsinki Declaration, and was approved by the local institutional review board and ethics committee of Buddhist Dalin Tzu Chi Hospital (No. B10004021-2).
Study Participants and Variables
We identified patients with HNC using the corresponding code in the International Classification of Disease, Ninth Revision, Clinical Modification (ICD-9-CM) in the diagnosis field. We selected patients 20 to 60 years old with newly diagnosed HNC and treated with radiotherapy only between 2000 and 2007 (ICD-9-CM codes: 140, 141, 143-148, and 161). To ensure the identification of HNC patients, only those patients who also had a Catastrophic Illness Certification (CIC) due to HNC were included in the study. In Taiwan, insured citizens with a major disease (eg, schizophrenia, mood disorders, immune disease, and cancer) can obtain free care for their illness, or related medical conditions, during the certificate’s validity period. We counted the index date for HNC as the date on which the patient gained CIC approval. In order to confirm that all enrolled HNC subjects in this study were incident cases, only new-onset HNC cases were included (n = 3651). Among them, a total of 402 patients diagnosed with RIOM before the date of HNC onset were excluded. The diagnostic algorithm to determine RIOM required at least 3 outpatient visits, or at least 1 inpatient claim for the ICD-9-CM codes of 528.01 during the study period. We also excluded those with missing data and those who were not followed for a minimum of 1 year after HNC diagnosis (n = 293). After this filtering process, a total of 2956 new-onset HNC cases were selected for further analysis (Figure 1).
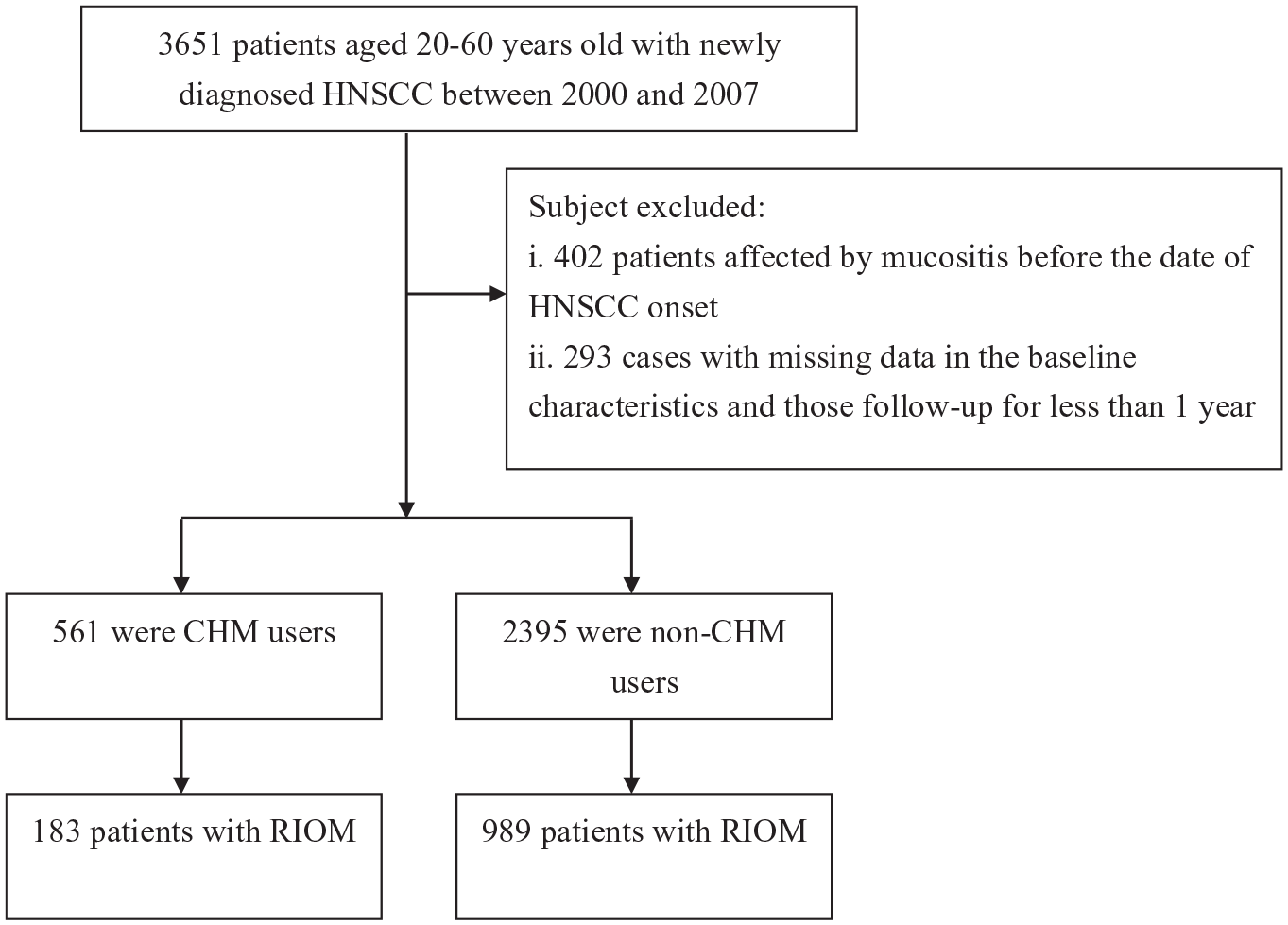
Flowchart of selection and follow-up of study subjects.

Cumulative incidence of RIOM among HNC patients with and without CHM use.
We then utilized the frequency of visits to Chinese medicine physicians to verify the CHM exposure of each enrollee, because only certified Chinese medicine physicians are allowed to prescribe CHM in Taiwan. Based on former methods, CHM users were identified as those who had received CHM to treat HNC for more than 30 days, whereas those treated for 30 days or less were considered to be non-CHM users.12-14 In this study, for the CHM user group, the time period between the date of HNC diagnosis and the date of first CHM use after HNC represented the immortal time, thus inducing an overestimation of the intervention’s beneficial effect. To reduce this bias, we calculated person-years (PYs) starting from the initiation of CHM usage to correct for immortal time for subjects who received CHM. 15 Therefore, the index date of the follow-up period for HNC subjects, classified as non-CHM users, was assigned to the date of the first HNC diagnosis, whereas the index date of the follow-up period for CHM users was assigned to the first date of the initiation of CHM prescription. The end date of follow-up period for both groups was assigned as the date of the earliest of the following: a diagnosis of RIOM, the date of withdrawal from the insurance program, or the date of December 31, 2012.
Covariate Assessment
Sociodemographic variables in this study included age, gender, income (for estimating insurance payments), and urbanization level of the individual’s residential area. Monthly income was clarified by the individual insurable wage and separated into 3 groups, which contained New Taiwan Dollars (NTD) ≤ 17 880, NTD = 17 881 to 43 900, and NTD ≥ 43 901. Urbanization levels were divided into urban (levels 1-2), suburban (levels 3-4), and rural (levels 5-7) areas. Level 1 refers to the “most urbanized” communities and level 7 refers to the “least urbanized” communities. 16 Baseline comorbidities for each enrollee were assigned using the established Charlson-Deyo Comorbidity Index (CCI), 17 and based on the individual’s medical records 1 year prior to initial entry into the cohort. To avoid double counting and possible over-adjustment in the regression model, HNC was excluded from the CCI score.
Data Analysis
Categorical variables were reported as percentages, and continuous variables presented as mean values and their standard deviations (SD). An independent t-test and a Chi-square test were used, as appropriate. To assess the independent influence of CHM use on the risk of RIOM, we conducted a Cox proportional hazards regression analysis to calculate the hazard ratio (HR) after adjusting simultaneously for age, insurance premium, urbanization level, and CCI. To further clarify the relation between CHM use and RIOM risk, we separated the CHM users into those who used CHM for 31 to 365 days and those who used CHM for >365 days. The Kaplan-Meier method was then employed to plot the cumulative incidence of RIOM for each cohort during the follow-up period, and the log-rank test was performed to assess the differences between the 2 curves. Finally, plot values for the log(−log[survival]) versus the log of survival time were inspected to verify the proportional hazards assumption. All analyses were conducted using SAS software version 9.3 (SAS Institute Inc., Cary, NC, USA). Differences of P < .05 were determined to be statistically significant.
Results
We identified 2956 patients with HNC during the period from 2000 to 2007. Of these, 561 received CHM treatment and 2395 were non-CHM users. Table 1 shows the demographic and clinical characteristics of the 2 groups. Compared to the non-CHM users, CHM users were more likely to be male, younger, and have higher CCI scores (all P < .01).
Demographic Data and Selected Comorbidities of Study Subjects.

Abbreviations: CHMs, Chinese herbal medicines; SD, standard deviation; CCI, Charlson-Deyo comorbidity index.
Among all enrollees, 1172 first episodes of RIOM occurred, 183 in CHM users and 989 in non-CHM users, during follow-up periods of 4465.69 and 17 078.67 PYs, respectively. The incidence rate of RIOM was lower among CHM users than among non-CHM users (40.98 vs 57.91, respectively, per 1000 PYs), with an adjusted HR of 0.68 (95% Confidence Interval [CI]: 0.58-0.80; Table 2). Of note, use of CHM for more than 1 year was associated with a 36% decreased risk of RIOM (95% CI: 0.49-0.85). The Kaplan-Meier analysis of survival by days of CHM use revealed a significantly difference in the survival rate free from RIOM across the three groups (P < 0.01).
Risk of RIOM for HNC Subjects Receiving or Not Receiving CHM Use.

Abbreviations: CHMs, Chinese herbal medicines; PYs, per 1000 person-years; HR, hazard ratio; CI: confidence interval.
Model adjusted for age, gender, urbanization level, monthly income, and CCI scores.
Table 3 presents the results from this analysis stratified by age and gender. Multivariable stratified analysis verified that the benefit of CHM therapy in treating RIOM was more predominant in females than in males, with an adjusted HR of 0.65 (95% CI: 0.53-0.78; Table 3). Additionally, a more significant beneficial effect of CHM use was observed among younger subjects (adjusted HR: 0.55; 95% CI: 0.44-0.68). The 10 most commonly prescribed herbal formulae for those with HNC are summarized in Table 4. Among them, 4 were single-herb products and the rest were multiple-herb products. Cox proportional hazards regression analysis showed that the use of Baizhi, Danshen, Shao-Yao-Gan-Cao-Tang, Gan-Lu-Yin, Huangqin, Shu-Jing-Huo-Xue-Tang, and Xin-Yi-Qing-Fei-Tang was significantly associated with lower risk of RIOM (Table 4).
Incidence and Risk of RIOM for HNC Patients Receiving or Not Receiving CHM in the Stratification of Sex and Age.

Abbreviations: CHMs, Chinese herbal medicines; PYs, person-years; HR, hazard ratio; CI, confidence interval.
Model adjusted for age, urbanization level, monthly income, and CCI scores.
Model adjusted for gender, urbanization level, monthly income, and CCI scores.
Risk of RIOM in Relation to the 10 Most Commonly Used Chinese Herbal Medicines for Patients With HNC.
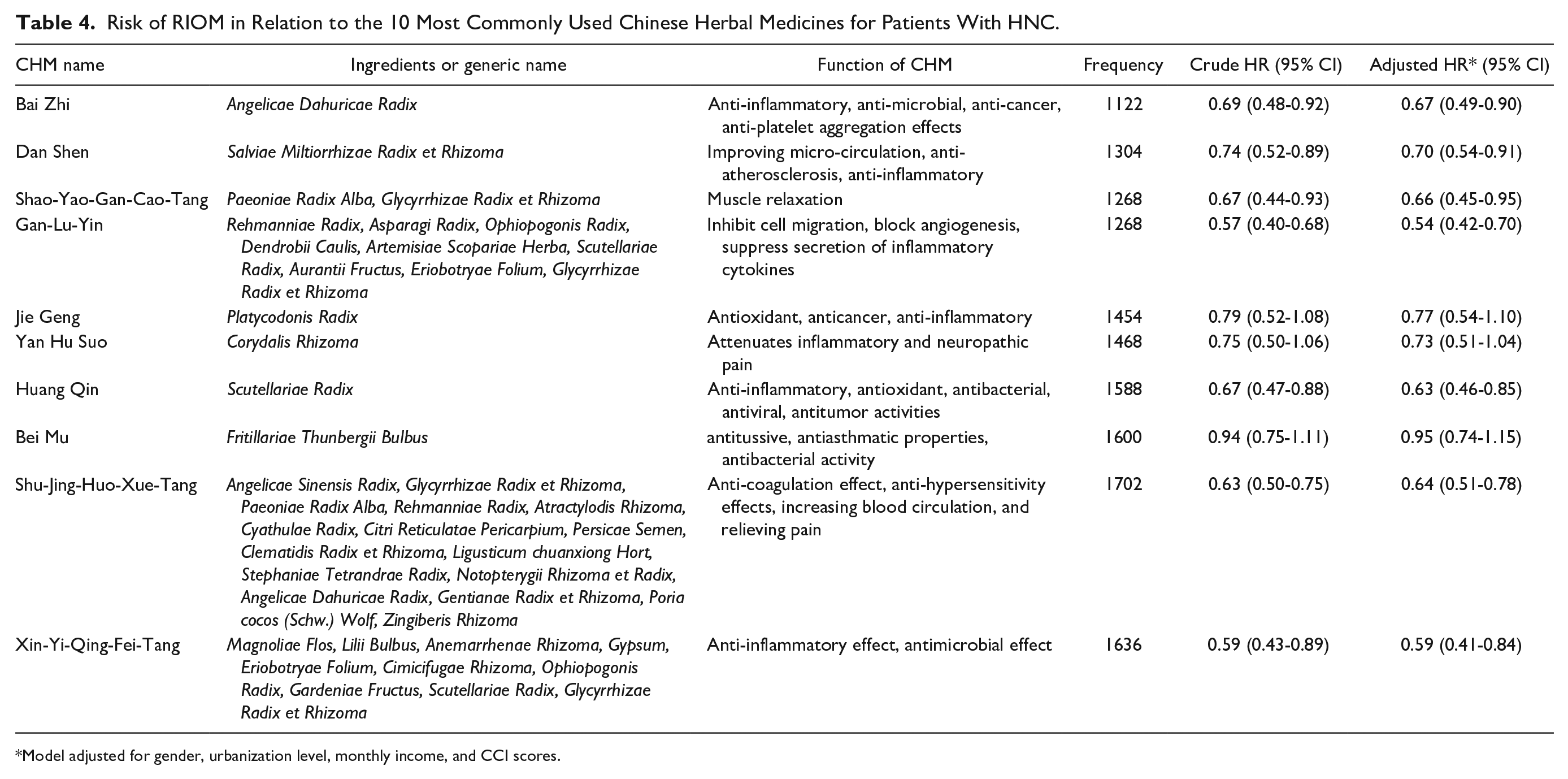
Model adjusted for gender, urbanization level, monthly income, and CCI scores.
Discussion
RIOM is the inflammation of the oral mucosa which presents clinically as edema, erythema, bleeding, ulceration, or pain. Given that the adverse side effect of RIOM may influence subsequent antineoplastic treatment, it is of great significance to prevent or treat RIOM when managing HNC patients. This is the first evidence-based cohort study determining whether the integration of CHM into the conventional therapy could reduce the risk of RIOM in HNC patients using a large nationwide claims-based database. Over a 10-year follow-up study, we discovered that HNC patients receiving CHM had a lower likelihood of RIOM than those not receiving CHM. Furthermore, those using CHM treatment for more than 1 year were found to have a markedly lower risk of RIOM by nearly 40%. As demonstration of a dose-response relationship is considered strong evidence for a causal relationship between exposure and outcome, this finding suggests that adding CHM to conventional treatment may help lower RIOM risk. While related studies on this topic are scarce, this positive therapeutic effect adds to a growing body of literature on the clinical efficacy of CHM use among HNC patients. 7
Findings from this study indicated that younger patients benefited more from CHM treatment in lowering the risk of RIOM, irrespective of other factors. This result may be due to younger people having fewer coexisting medical conditions, having better medical knowledge, having a more positive attitude toward their medical condition, or having more psychosocial and coping resources to rely upon than older patients. 18 These findings also suggest that younger HNC survivors may more easily adapt to the side effects of treatment, and consequently are at reduced risk of RIOM. Furthermore, the reduction in risk of RIOM was higher for females than for males (35% vs 19%). We speculate that women may have better health literacy, more willingness to adhere to strict medical procedures, and more positive attitudes about self-care than men, 19 and accordingly, they were more likely to comply with the prescribed medical regimen to lower risk of RIOM.
Oral mucositis is any inflammatory mucosal destruction presenting as erythema or ulceration of oral mucosa owing to the use of chemotherapy or radiation therapy to treat cancer.3,6,20 Of the 10 most commonly prescribed herbal formulae for HNC patients, we found that 7 were associated with a significantly lower risk of RIOM. For example, the use of Xin-Yi-Qing-Fei-Tang was found to lessen the risk of RIOM by 41%. We speculate that the major ingredient, Anemarrhena asphodeloides, might produce an appreciable anti-inflammatory effect by abating nuclear factor kappa beta (NF-κB) signaling. 21 NF-κB is well known as a crucial transcription mediator regulating the induction of the inflammatory response. 22 Xin-Yi-Qing-Fei-Tang also showed an effect against a variety of bacteria,23,24 thus minimizing the risk of bacterial colonization after ulceration develops.
Use of Shu-Jing-Huo-Xue-Tang and Shao-Yao-Gan-Cao-Tang were also associated with a lower susceptibility to developing RIOM. Priori studies in a rodent model showed that both compounds can significantly modulate the activity of the alpha-2 adrenoceptor (α2-AR).25,26 Dysregulation of the α2-AR pathway may contribute to the release of inflammatory cytokines, such as tumor necrosis factor-α (TNF-α), interleukin-1 (IL-1), and IL-6; all of these mediators have been implicated in the development of RIOM.6,27
Consistent with the findings of earlier research,14,28 this study revealed that Gan-Lu-Yin was the most frequently used Chinese herbal formula for treating HNC. The positive association between Gan-Lu-Yin use and a lower incidence of RIOM may stem from its reported effects that included reducing cell proliferation and the inhibition of inflammatory cytokines through the NF-kB dependent pathway.29,30 In 1 previous report, relative to untreated controls, rats fed with Gan-Lu-Yin had markedly reduced levels of inflammatory markers. 30 The inhibition of angiogenesis may prevent the expression and survival of cancer cells, thereby decreasing the risk of RIOM after HNC onset.
With regard to the single-herb products used to treat those with HNC, we noted that Baizhi was associated with a reduced risk of RIOM events. Recently, several laboratory-identified, anti-inflammatory, properties of Baizhi have been reported, including antioxidation, 31 anti-inflammatory, 32 and anti-tumor properties. 33 Imperatorin, a candidate compound purified from this CHM product, has been proven to profoundly reduce the release of TNF-α, IL-1β, and IL-6 in lipopolysaccharide-stimulated RAW 264.7 cells via the suppression of NF-κB activation. 32 Additionally, 1 in vitro study revealed that imperatorin could mediate oncogene expression to induce cell cycle arrest. 33
The remaining herbal products suggested as effective in lessening RIOM risk were Danshen and Huangqin. The first belongs to the Campanulaceae family, and its ingredient was discovered to possess antioxidant, anti-tumor, anti-microbial, and immune-boosting properties. 34 As for Huangqin, Wogonin, its main ingredient, has shown anti-neoplastic and anti-inflammatory effects in both in vitro and in vivo studies. For example, 1 study demonstrated that Wogonin can induce AMP-activated protein kinase to inhibit proliferation and induce apoptosis in cancer cells. 35 Wogonin was also found beneficial in suppressing the production of inflammatory mediators by modulating the NF-κB and NF-E2-related factor 2 signaling pathways. 36 These findings may explain the mechanisms responsible for the potent effects of Danshen and Huangqin observed in this study.
While our study is the first to investigate the relationship between CHM use and RIOM risk among patients with HNC, there are several important limitations. First, using secondary health care databases always entails the risk of errors in the coding process. To minimize this bias, we enrolled only patients with new-onset HNC or RIOM, and only after the patients had at least 3 outpatient visits or 1 inpatient admission for HNC. Additionally, HNC cases were further linked to the CIC database to verify their status as patients with a catastrophic disease. It should also be noted that the NHI of Taiwan randomly reviews the charts and audits medical charges to verify the accuracy of claims files. Moreover, the coding approach and data availability were similar for the 2 groups, so that any misclassification bias would have likely been nondifferential. Second, the LHID lacks information on social network relationships, smoking, alcohol intake, personality attributes, laboratory data, and education level. Thus, future research examining these untested variables is needed to better determine the generalizability of our findings. Nevertheless, to thoroughly address the confounding by indication that may arise in this real-world comparative effectiveness study, we attempted to reanalyze the association of CHM use with the risk of RIOM via a propensity score – matched analysis. For each HNC patient who received CHM, 1 control patient was selected by 1:1 matching, based on a propensity score. The propensity score was calculated using logistic regression on the basis of patients’ demographics and baseline comorbidities at enrollment. The results of the reanalysis showed that no significant difference occurred between the 2 groups with regard to age, sex, monthly income, residential area, and number of comorbidities after matching procedure with propensity score, indicating that the 2 groups were comparable on these characteristics (Supplemental Table 1). Furthermore, the use of CHM was still found to be significantly related to reduction risk of RIOM among HNC participants, with the adjusted HR of 0.65 (Supplemental Table 2). Third, information regarding dose-limiting toxicity was not available in this database, and failure to adjust for this factor might bias the results. To address this issue, a sensitivity analysis was performed to more carefully examine the abovementioned association. First, we applied the numbers of radiotherapy utilization after HNC onset to serve as a surrogate of dose-limiting toxicities stemming from the radiation therapy. After considering this variable, in the multivariate analysis, the results indicated that, as compared to HNC patients without CHM use, the selected HNC patients with CHM use, still had a significantly lower risk for RIOM (adjusted HR: 0.70; 95% CI = 0.59-0.82). Therefore, it can be inferred that the level of dose-limiting toxicities did not appreciably impact the relationship reported herein. Fourth, although the findings of this observational cohort study conveyed that the continuous use of CHM may be beneficial, it must be recognized that participants were not initially randomly categorized into users and nonusers. Therefore, well-designed randomized controlled trials are still needed to minimize confounding by covariates not explicitly accounted for by the present design, thus paving the way for further in vivo studies regarding the effects of CHM products on patients with other chronic medical conditions. These limitations notwithstanding, this study also possessed several strengths. One strength of this nationwide register-based study is the completeness of the records of hospital diagnoses and prescription claims; the minimal risk of selection bias and loss to follow-up; and the large population of both men and women, which provide sufficient power to conduct detailed analyses.
Conclusion
In summary, this large-scale nationwide cohort study showed that, during treatment for HNC, the integration of CHM appears to reduce the risk of RIOM by 33%. This finding can provide a reference for healthcare providers seeking therapeutic interventions to improve the prognosis for HNC patients.
Supplemental Material
sj-doc-1-ict-10.1177_15347354211044833 – Supplemental material for Chinese Herbal Medicine to Reduce Radiation-Induced Oral Mucositis in Head and Neck Cancer Patients: Evidence From Population-Based Health Claims
Supplemental material, sj-doc-1-ict-10.1177_15347354211044833 for Chinese Herbal Medicine to Reduce Radiation-Induced Oral Mucositis in Head and Neck Cancer Patients: Evidence From Population-Based Health Claims by Hsin-Hua Li, Hanoch Livneh, Wei-Jen Chen, Ming-Chi Lu, Wen-Yen Chiou, Shih-Kai Hung, Chia-Chou Yeh and Tzung-Yi Tsai in Integrative Cancer Therapies
Footnotes
Acknowledgements
The study is based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health and managed by the National Health Research Institutes, Taiwan. The interpretation and conclusions contained herein do not represent those of the Bureau of National Health Insurance, Department of Health or the National Health Research Institutes. HHL, HL, and WJC contributed equally to this work.
Author Contributions
HHL, HL, WJC, and TYT were involved in the study design and drafted the manuscript. HL, HHL, and TYT contributed to data analysis and revised the manuscript. HHL, HL, WHC, MCL, CCY, and TYT contributed to the interpretation of data and provided comments on the final draft of the manuscript. MCL and CCY provided administrative support and comments on the manuscript drafts. TYT, HL, and HHL were responsible for the study conception, design, data analysis, and drafting. All authors gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.