
Abstract
Objective:
The aim of the present study is to determine the relation between the satisfaction of parents of children with cancer with the social support received and provided from a multidimensional perspective (sources and types of support) and the disruptions that take place in different areas of their lives (partner, children, family, social relations, and economic and employment situation)
Method:
One hundred twelve parents of children diagnosed with cancer who received treatment at the Mother and Child Hospital of Málaga (Spain) were recruited. Data were gathered through self-reporting measures. The instrument used includes a questionnaire about socio-demographic variables, a questionnaire about parents’ adjustment to the situation and a questionnaire about social support received and provided based on the different sources and types of support.
Results:
There is a negative and significant relation between satisfaction with support received and provided and the magnitude of disruptions in parents’ lives.
Conclusion:
Satisfaction with emotional support received from the partner and family, and support provided to these sources, relate to lower disruption in different areas of parents’ lives. These results can have significant practical implications for the psychosocial care provided to parents of children with cancer.
Keywords
Introduction
Childhood cancer is both a medical and a family and social issue. 1 Once the child’s cancer is diagnosed, family dynamics are altered, leading on some occasions to disruptions that make some families require special care in facing such complex situations.2,3 Childhood cancer affects deeply the family system for long periods of time, and it also affects the quality of life of such families.4-6 These disruptions can remain throughout time 7 and affect parents’ relation with the rest of family members.8,9 The family life experiences a disruption 10 and the whole family system “falls ill,” 11 since the everyday life of such families must adapt to a new reality.12,13
These disruptions do not take the same form in families in the same way and there are some variables that can affect how the child’s disease is faced. 14 Improving support networks and the perception of support can help parents to cope better with stressful situations, particularly when avoiding or reducing the source of stress is unviable and even not recommended. 15 Social support is an interactive concept that is defined as an inter-personal transaction of help that takes place between 1 source (partner, family, friends, community) and the recipient of such help, and which involves emotional, material, and informational support in a specific context. 16 Based on the structural dimension of social support, it is necessary to consider the support network, the frequency of the contact with this network and the reciprocity of the contact.17,18 This reciprocity of support is related to the balance of support received and provided. 19 Balance is key for the maintenance of the network and the lack of it can cause overload or guilt issues. 19 This is the reason why it could also be interesting to know the role played by the support parents provide to their own networks and how this support affects parents’ adjustment to different areas of their lives. The functional dimension of social support is also worth mentioning. Social support is more beneficial when it is more specific to solve the issue for which such support is being provided, and the more it adapts to the issue that needs solving, the more effective it will be.20-22 The different types of support have specific functions, such as emotional, material and informational help. 16 Emotional support makes individuals feel loved and valued 23 and provides them with the possibility to express emotions and concerns to a confidant. Material or instrumental support is related to providing direct help, which can take the form of economic help, services, domestic help, etc. Support provided on a regular basis by close relatives or friends can contribute to a significant reduction of the burden of daily life tasks. Individuals who receive informational support can solve their questions or issues through advice and information from different people. This definition of social support, which is based on a multidimensional perspective is related to Bronfenbrenner’s 24 ecological model of human development. Bronfenbrenner’s 25 ecological model of human development (EMHD) has been widely studied and applied to different study fields such as education, family, sociology, and health. This model considers the development of a person within an ecosystem in which the person lives and interacts. According to this approach to human development, all systems in which a person is integrated must be studied. These assumptions can be extrapolated to the context of parents of children with cancer. When a child is diagnosed with cancer, in some way, the entire family falls ill. 26 When this occurs, parents activate a series of strategies to face the child’s disease, which are largely determined by the context of the family itself.27,28 For this reason, the ecological model is the theoretical framework of the present study, since it can interrelate a large number of factors and contexts involved in how parents face childhood cancer and its effects. The ecological model provides a vision of the complexity and constant interaction between individuals and their environments, between which support dynamics and transactions generate constantly. The ecological model is applied as theoretical model in the field of psychooncology given its ability to assess and intervene with all variables which affect patients both directly and indirectly. 29 By analyzing the support received and provided by parents of children with cancer based on the sources of support (partner, family, friends, and community) and the types of support (emotional, instrumental, and informational), we are considering parents’ ecological contexts.24,30
There is great consensus on the positive effects of social support on health and quality of life.31-33 The models of direct effect and buffering effect of stress explain these positive effects. The direct effect model suggests that social support increases well-being and health regardless of the stress experienced. 34 This increase of positive psychological states thanks to contact with support networks sets healthy behaviors in motion and it relates positively to health and well-being. 35 Alternatively, the buffering effect model suggests that social support buffers the negative effects of stress on people. So, if there is no stressor, social support would not have any effect on well-being. 36 These 2 theories are not mutually exclusive, and both are valid when it comes to explaining the benefits of social support. Social support directly protects individuals against the appearance of certain stressors, as well as reducing the weight of present stressors. 37
It is in this respect interesting to note that for the evaluation of social support, the fact of receiving it, which could be evaluated through the frequency with which it is received or provided, does not always correspond to an increase in its perception. Support does not take place just because it is happening, but it must also be perceived as such. For this is reason, it is key to consider the level of satisfaction with social support and along with its frequency. 35 Evaluating the bidirectionality of social support (received and provided) is another important aspect to consider. It is interesting to consider who is evaluating support—the person receiving it or the person providing it. Most studies focus on evaluating the person receiving support, however, there is growing interest in comparing the perception of support from both those who receive it and those who provide it. 38
In the field of childhood cancer, there are previous studies that confirm support provided by the network helps to reduce the stress experienced by parents of children with cancer. 29 Espada and Grau 39 described that one of the most widely used strategy of parents is the search of social support from health professionals, partners, extended family, friends, and spiritual support. Social support received can improve satisfaction with life and reduce the stress of parents of children with cancer. 40 Harper et al 41 analyse the direct and buffering effect of satisfaction with social support received in parents of children with cancer, the dimension or size of the network and depressive symptomatology. These authors conclude that satisfaction with support has a direct alleviating effect on the psychological distress of all parents and in those cases where parents may be at risk of showing depressive symptomatology, they would benefit from the buffering effects of the dimension of their network. Kelada et al 42 analyze the social support that extended family offers to parents and how this support is perceived by parents. Family can provide valuable support to parents, but if such support is not appropriate or it is not as expected, it can be harmful. Support received must be as appropriate as possible based on the type of support needed, which is in line with the theory of the specificity of support. 20 Pozo-Muñoz et al 43 analyzed the impact of social support perceived by parents on their health. The perception of social support was linked to higher levels of health and perception of satisfaction with life.
The study of satisfaction with social support in parents of children with cancer does not place particular emphasis on analyzing the support provided by parents to their own networks. This can be interesting to consider, since the same person can both receive support and provide it, thus leading to a reciprocity that is relevant to the structure of support.
The main objective of the present study is to analyze how satisfaction with social support received and satisfaction with social support provided by parents of children with cancer affects the disruptions they experience during the child’s disease. The practical and clinical implications derived from this objective are considered highly relevant. The innovative contribution of the present study is the detailed analysis of social support based on its multidimensionality (sources and types of support), as well as the analysis of support based on its bidirectionality (received and provided) and its relation to parents’ satisfaction with support in different dimensions of their lives, in which disruptions caused by the disease can take place (partner, children, family, social relations, and economic and employment changes).
According to the study’s objectives, the hypotheses suggested are the following:
There is a negative relation between satisfaction with support (emotional, instrumental and informational) received from the different sources (partner, family, friends, and community) and the different disruptions experienced by parents of children with cancer that take place in various areas (partner, children, extended family, social relations, and economic and employment situation).
There is a negative relation between satisfaction with support (emotional, instrumental, and information) provided by parents to the different sources (partner, family, friends, and community) and the different disruptions experienced by parents of children with cancer that take place in various areas (partner, children, extended family, social relations, and economic and employment situation).
Method
Procedure
Participating parents attended the Mother and Child Hospital of Málaga regularly and they were contacted directly at the hospital (follow-up consultations, day care treatment and hospitalization area) or at play rooms for ill minors at a local NGO located within the hospital, which provides support to families with children with cancer. Social and healthcare professionals informed parents about the study and those who decided to participate voluntarily went to the data gathering point set up at the hospital. An informative poster about the study was placed in the oncology floor to encourage other parents to participate. Participants received an informed consent form about the procedure that would be carried out. The study was approved by the Ethical Committee of Scientific Research from the Regional Government of Andalusia (Spain), CEI 2017. After signing the informed consent, participants could choose between 2 ways of completing the instrument: on paper during one of their visits to hospital or on-line through a computer-based model of the instrument that was anonymously and automatically added to a database once completed.
The sample was gathered from parents of children and adolescents who received treatment at the Mother and Child Hospital of Málaga and from parents of patients aged between 15 and 21 from the Regional Hospital of Málaga (Spain). The selection of participants was determined by considering all parents who wished to participate voluntarily in the study. Both or just 1 parent could participate, without establishing a limit on this question. Inclusion criteria for the study sample were the following: parents or legal guardians of patients aged from 0 to 21 with cancer disease. Conversely, exclusion criteria were the following: other relatives of patients who were not the parents or legal guardians and parents whose child had deceased. The socio-demographic questionnaire did not include questions about the stage of treatment (on-going or follow-up); however, all participants attended the Hospital for their children to receive treatment related to cancer (follow-up consultations, ambulatory treatment, hospitalization, etc.).
Measures
An instrument with self-reporting measures was created for the collection of data from participants. Questionnaires included in the instrument were the following:
Sociodemographic questionnaire
The sociodemographic questionnaire included questions related to gender, age and marital status of participants (level of qualifications, employment situation, number of children and number of people under their care). This questionnaire also includes questions about the child: gender, type of cancer, and length of time since diagnosis.
Questionnaire for the assessment of adjustment of parents of children with cancer
This questionnaire was designed ad hoc by Hombrados-Mendieta and Martos-Méndez. 44 It was designed to measure different situations that take place in various areas of parents’ lives during the child’s disease. More specifically, participants are asked about their own evaluation of the possible changes or disruptions that can take place in various areas of their lives: partner (items 1-8), children (items 9-16), extended family (17-22), social relations (23-27) and economic and employment situation (items 28-30). The questionnaire includes a total of 30 items. Answer options for each item are 5, which assess the level of agreement-disagreement with each item—“1” meaning total disagreement and “5” meaning total agreement. In order to extract information about the level of parents’ adjustment to the different situations suggested the scores of 7 items were rotated (2, 3, 6, 9, 12, 17, and 23). By doing so, the higher the scores in this scale, the lower the parents’ adjustment to the child’s disease (see Supplemental Appendix 1). Cronbach’s Alpha of the full scale is α = .79. According to each dimension of adjustment, indexes are the following: partner α = .69, children α = .70, family α = .50, social relations α = .54, economic and employment situation α = .64. This instrument has been used in other studies and it has shown high reliability. 45
Questionnaire of frequency and satisfaction with social support (QFSSS)
Questionnaire of Frequency and Satisfaction with Social Support (QFSSS). 46 This questionnaire was used to measure parents’ satisfaction with social support received and provided. More specifically, the type of support (emotional, instrumental, and informational) provided by each source from parents’ social networks (partner, family, friends, and members of the community), as well as the type of support provided by parents to the different sources. The questionnaire comprises 12 items about support received and 12 items about support provided. There are 5 answer options, in which “1” means unsatisfied and “5” very satisfied. Participants were asked about their level of satisfaction with social support received (sources and types) and provided (sources and types). The level of satisfaction with social support is a variable that provides information on the social support perceived by parents, the support they receive and the support they provide. Cronbach’s Alpha of the full scale is α = .96.
Data Analysis
For the development of the present research and considering the objectives and hypotheses previously described a correlational design with self-reporting measures was carried out. Statistical analyses were performed using SPSS (v.25). A Pearson’s correlational analysis was carried to know the degree of the relation between satisfaction with support received and provided, the time since diagnosis and parents’ adjustment. A linear multiple regression analysis was also performed to know in more detail the relations between the study’s variables, including a clinical variable that could be relevant, that is, time since diagnosis. Variables considered for the regression equation were those that reached statistical significance (P < .05). Backward multiple regression analysis method was used to better know the best predicting model from each variable studied. The procedure followed involved introducing all independent variables of satisfaction with support received and provided based on sources and types and time since diagnosis for each dimension of parents’ adjustment. For each dimension of adjustment, a predictive model with satisfaction with support and time since diagnosis that seems more predictive was obtained.
Results
One hundred twelve parents of children with cancer who received treatment at the Children’s Hospital of Málaga (Spain) participated in the study (Table 1). Participants were selected based on their voluntary wish to participate. Participants were at different stages of their children’s cancer disease and treatment. The sample comprised 33.9% men and 66.1% women, with an average age of 41 years (SD = 6.93). Most participants were married or lived with their partners (88.5%). The remaining were single, divorced or widowed (11.5%). Regarding the gender of the children, 58% were boys, and 42% girls, with an average age of 8 years (SD = 5.02). Regarding the type of cancer, 54.5% suffered from leukemia, 9% from Ewing sarcoma, 8% from lymphoma, 4.5% from medulloblastoma, and the remaining suffered from other types of childhood cancer.
Sociodemographic Variables (n = 112).

Data represent %(N) except as noted.
Mean (standard deviation).
The length of time from diagnosis was the following: 18.9% of children had been diagnosed less than 1 year before, 23.4% 1 year, 19.8% 2 years ago, 9.9% 3 years ago, 12.6% 4 years ago, and the remaining 15.3% 5 or more years ago.
There is a negative and significant relation between satisfaction with support received and provided by each source and type of support and parents’ adjustment. This means that the higher the satisfaction with support, the lower the disruptions experienced by parents (Table 2). This relation appears in many dimensions of satisfaction with support received and provided (sources and types) and parents’ adjustment. This result is in line with hypotheses 1 and 2. Time since diagnosis was non-significant.
Correlations of Satisfaction With Support Received and Provided by Sources and Types and Time Since Diagnosis and Parents’ Dimensions of Adjustment.

P < .05. **P < .01. ***P < .001.
If we look at the models of satisfaction with support received and provided based on the sources (Table 3), some specific sources seem to better predict parents’ adjustment. For this reason, different dimensions have been considered within those adjustments that parents must apply to their lives when facing their child’s disease. Regarding the adjustments that parents report as occurring in the couple, satisfaction with support received from the partner (R2 = .30, F = 42.95, P < .001) and satisfaction with support provided by parents to their partner (R2 = .23, F = 30.78, P < .001) predict better adjustment in this dimension. Regarding adjustment to the relationship with their children, satisfaction with support received from family (R2 = .08, F = 4.56, P = .010) and satisfaction with support provided to family (R2 = .04, F = 4.20, P = .043) predict the lowest disruptions with children. Regarding extended family, satisfaction with support received from partner (B = −0.18, P = .052) and family (B = −0.37, P = .000) predicts the lowest disruptions with extended family (R2 = .22, F = 13.93, P < .001). Additionally, satisfaction with support provided by parents to their family (B = −0.41, P = .000), and friends (B = −0.37, P = .007), predicts better adjustment with extended family (R2 = .25, F = 11.17, P < .001). Adjustments also take place in parents’ social relations (R2 = .23, F = 14.86, P < .001). Support provided by parents to their family (R2 = .06, F = 6.93, P = .010) improves their adjustment in social relations. It is worth noting that the adjustments that parents must go through in their economic and employment situation due to the child’s disease, no sources of support received nor provided seem to be significant to reduce disruptions based on a significance level of P < .05. Nevertheless, satisfaction with support received from partner would be the one that better explains this type of adjustment R2 = .03, F = 3.15, P = .059).
Linear Regression Models of Satisfaction With Support Received and Provided by the Sources and Time Since Diagnosis on Parents’ Dimensions of Adjustment.*
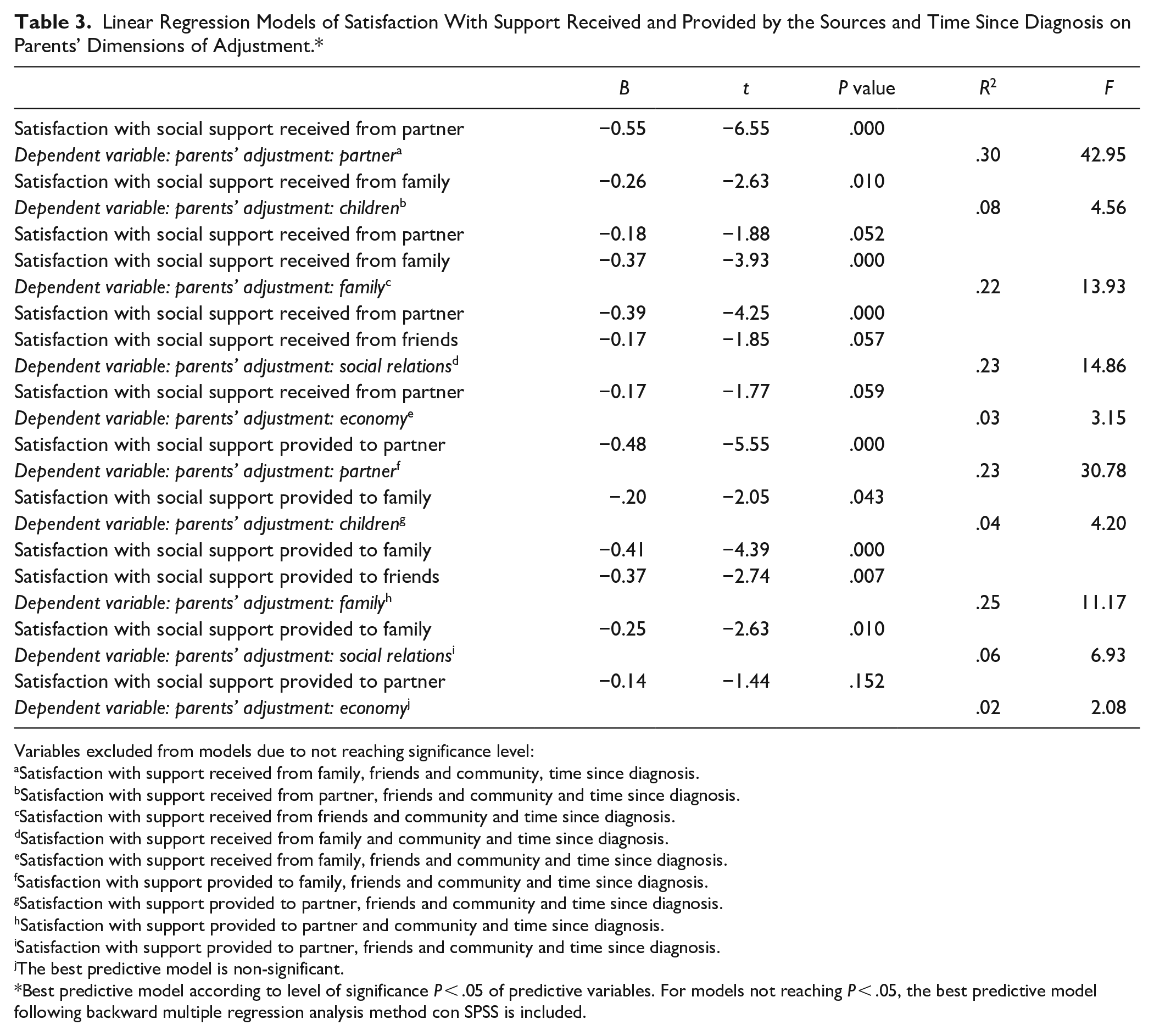
Variables excluded from models due to not reaching significance level:
Satisfaction with support received from family, friends and community, time since diagnosis.
Satisfaction with support received from partner, friends and community and time since diagnosis.
Satisfaction with support received from friends and community and time since diagnosis.
Satisfaction with support received from family and community and time since diagnosis.
Satisfaction with support received from family, friends and community and time since diagnosis.
Satisfaction with support provided to family, friends and community and time since diagnosis.
Satisfaction with support provided to partner, friends and community and time since diagnosis.
Satisfaction with support provided to partner and community and time since diagnosis.
Satisfaction with support provided to partner, friends and community and time since diagnosis.
The best predictive model is non-significant.
Best predictive model according to level of significance P < .05 of predictive variables. For models not reaching P < .05, the best predictive model following backward multiple regression analysis method con SPSS is included.
Models including satisfaction with types of support and time since diagnosis as predictive variables and parents’ adjustments as dependent variables have also been suggested (Table 4). Time since diagnosis was non-significant in all cases. Satisfaction with emotional support received (R2 = .21, F = 26.61, P < .001) and provided (R2 = .13, F = 14.95, P < .001) significantly reduces disruptions that occur in the couple. Regarding adjustments parents experience in the relationship with their children, the best model obtained was non-significant for level P < .05, which happened with satisfaction with support received and provided based on the types of support. Regarding the adjustments parents experience with extended family, satisfaction with emotional support received R2 = .24, F = 24.12, P < .001) and instrumental support provided (R2 = .09, F = 10.18, P = .002) predict better adjustment. Satisfaction with emotional support received (R2 = .24, F = 31.15, P < .001) and provided (R2 = .05, F = 5.29, P = .024) relates to better adjustment in social relations. Regarding parents’ adjustment in economic and employment matters, satisfaction with informational support received (R2 = .06, F = 6.55, P = .012) predicts better adjustment. However, in the case of satisfaction with support provided based on the types of support (emotional, instrumental, and informational), the best model did not reach significance level above P < .05.
Linear Regression Models of Satisfaction With Support Received and Provided Based on Types and Time Since Diagnosis on Parents’ Dimensions of Adjustment.*

Variables excluded from models due to not reaching significance level:
Satisfaction with instrumental and informational support received and time since diagnosis.
The best predictive model is non-significant and time since diagnosis.
Satisfaction with instrumental and informational support and time since diagnosis.
Satisfaction with instrumental and informational support and time since diagnosis.
Satisfaction with instrumental and informational support and time since diagnosis.
Satisfaction with instrumental and informational support and time since diagnosis.
The best predictive model is non-significant.
Satisfaction with emotional and instrumental support provided and time since diagnosis.
Satisfaction with instrumental and informational support provided and time since diagnosis.
The best predictive model is non-significant.
Best predictive model according to level of significance P < .05 of predictive variables. For models not reaching P < .05, the best predictive model following backward multiple regression analysis method con SPSS is included.
Discussion
Results obtained suggest that satisfaction with support received and provided relate to the adjustments parents of children with cancer experience in their lives. These results are in line with suggestions from hypotheses 1 and 2.
Analyzing the disruptions parents experience in the different areas of their lives (partner, children, extended family, social relations, and economic and employment situation) and their satisfaction with support based on sources and types shows the importance of understanding the person, in this case parents, as individuals affected by different social systems (partner, children, family, social relations, etc.). 24 Applying the ecological model is innovative because it considers the “ecological environment” of parents, understanding them as agents who interact with their closest environment. This environment also interacts with them in a reciprocal and adaptive manner.24,30
Knowing what type of support and the source is received from or provided to improves the knowledge on how effective specific types of support can be to minimize the impact of the disease on different areas of parents’ lives. This is also explained through the Theory of Specificity of Support by Cohen and McKay, 20 which confirms that the more specific support is, the more effective.
Results shed relevant information on the exchange and balance of support. 19 However, it would be interesting to analyze in future lines of investigation the importance of support provided by parents to increase their adjustment to the disruptions they experience. Some studies suggest that mutual support networks or experiences in which support is received and provided can give people back control over their lives, helping them to become active participants in the development of resources, the coping with problematic situations and the provision of support.47,48 The person would not only benefit from receiving help from others, but also by turning his or her own experience into potential help for his/herself and others. 49 According to results obtained in this study, it seems that a balanced exchange of support could be related to a better adjustment. Results show the importance of keeping a balance between receiving and providing support, for instance in the couple or the family. These are sources of support that have a great impact on parents’ adjustment.42,50 Results are in line with suggestions by Wills and Shinar, 23 according to whom emotional support is significantly positive for many of the disruptions parents experience in their relations with their partner and children.
It is worth noting that support received from and provided to the community did not relate significantly to any adjustment. Previous studies have shown this variable to be significant in the reduction of parents’ stress levels. 40 This can open a reflection on whether community care, understood as neighbor circles, close associations, etc., contributes effectively to make disruptions that take place in the lives of parents as little negative as possible. It could be of interest to pay further attention to this matter in future studies and know the reach of community support in families of children with cancer, given that practical implications are high.
We also see that adjustments related to parents’ economic and employment situations are the least related to social support. It is important not to forget this area in parents’ lives due to the impact it can have on their lives beyond the effects of the disease of their child and consider it in future studies. Previous studies show significant disruptions in this area51-54 and how these relate to parents’ quality of life negatively. Given this strong impact, it would be interesting to analyze in future investigations the relations between economic and employment adjustments and social support.
Results from the present study can be of interest for the planning of interventions that aim at improving parents’ abilities and their environments to cope with the situations they go through due to childhood cancer, as well as increasing their support networks.
Practical Implications and Limitations
Results obtained from the present study can have practical implications. It would be interesting to apply them to everyday tasks of practitioners who provide psychosocial support to families of children with cancer. To know and to boost parents’ support networks can be a good therapeutical strategy, as well as to provide information given to the most effective sources of support in order for them to help parents with specific matters (partner, children, family, social relations, and economic and employment matters), given that not every type of support is equally effective to promote appropriate adjustments. It is also necessary to consider the domains in which adjustments and disruptions take place, as well as to know the weight of emotional, instrumental, and informational support both received and provided by the different sources (partner, family, friends, and community). Some effective strategies to improve parents’ adjustment when facing childhood cancer can be: to promote emotional support through the increase of communication and intimacy with the partner, to receive emotional support from family and friends, to involve the family in the tasks related to the care of the children and to guide parents to provide support to those relatives by giving them information, or to give parents useful information related to matters involving their children and their economic and employment situations.
Some limitations found in the study have already been described throughout the discussion. Regarding future investigation, the analysis of support provided, community support and the adjustments related to parents’ economic and employment situations should be further studied. The cross-sectional nature of the study is also a limitation. In this sense, future research could include longitudinal designs to know in more detail the relations between social support and parents’ adjustment throughout time. It must also be noted that all participants come from Málaga (Spain) or nearby towns, and moved to Málaga due to the child’s disease. This fact can limit the extrapolation of findings to other contexts and cultures. It would be interesting to replicate the study in other countries to know the role of cultural factors in parents’ adjustment and coping with childhood cancer.
Regarding the characteristics of the sample, there were more female than male participants. It would be important to balance the number of mothers and fathers participating in future studies in order to know better the needs for support in a differential manner. It must be noted that this responds to a social reality, where the number of mothers responsible for the care of the ill child as main carers is significantly higher. Additionally, women also tend to be more willing to participate in this type of research. 55 In future research, parents’ adjustment can also be analyzed according to the different stages of the disease (diagnosis, treatment, discharge, etc.) and the different types of cancer.
Conclusion
The important role played by social support in parents’ quality of life and their adjustment to disruptions experienced is the main conclusion of the present research. Particularly satisfaction with emotional support received from the partner and family, as well as support provided to these sources, as they show lower disruptions in various areas of parents’ lives.
Finally, it is important to note that one of the study’s strengths is that it provides innovative insights on the relations between the different types of support and parents’ adjustment to childhood cancer. These relations are deeply involved in the process of coping with a child’s cancer. Analyzing in such detail these relations from an ecological and multidimensional perspective is of great value for parents’ adaptation to their child’s disease and therefore improve clinical practice and action protocols.
Supplemental Material
sj-docx-1-ict-10.1177_15347354211044089 – Supplemental material for Social Support Received and Provided in the Adjustment of Parents of Children With Cancer
Supplemental material, sj-docx-1-ict-10.1177_15347354211044089 for Social Support Received and Provided in the Adjustment of Parents of Children With Cancer by Anabel Melguizo-Garín, Isabel Hombrados-Mendieta, Mª José Martos-Méndez and Iván Ruiz-Rodríguez in Integrative Cancer Therapies
Footnotes
Acknowledgements
The Authors would like to express their gratitude to the Fundación Olivares (Málaga, Spain) and to all the parents who participated in this study.
Author Contributions
Conceptualization, A. M.-G., I. H.-M., and M.J.M.-M.; methodology, I. H.-M. and M.J.M.-M.; formal analysis, A. M.-G and M.J.M.-M.; investigation, A. M.-G., I.H.-M., M.J.M.-M., and I. R.-R.; writing—original draft preparation, A. M.- G. and M.J.M.-M.; writing—review and editing, A. M. -G., I.H.-M., M.J.M.-M., and I. R.-R.; supervision, A. M. -G., I.H.-M., M.J.M.-M., and I. R.-R.; funding acquisition, I.H.-M. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Groups PAIDI, Junta de Andalucía, Spain [Grant Number HUM-590].
Informed and Ethical Consent
Participating parents received an informed consent form about the procedure that would be carried out and the study is approved by the Ethical Committee of Scientific Research from the Regional Government of Andalusia (Spain), CEI 2017.
Supplemental Material
Supplemental material for this article is available online.
Data Availability Statement
In compliance with data protection regulations and ethical rules, the data may be made available on request to the author of the correspondence.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.