
Abstract
Background and Purpose:
Qigong is used by cancer patients, but its effect is not adequately evaluated to date. The aim of this study was to investigate the effects of Qigong for the management of a symptom cluster comprising fatigue, dyspnea, and anxiety in patients with lung cancer.
Methodology:
A total of 156 lung cancer patients participated in this trial, and they were randomized to a Qigong group (6 weeks of intervention) or a waitlist control group receiving usual care. The symptom cluster was assessed at baseline, at the end of treatment (primary outcome), and at 12 weeks, alongside measures of cough and quality of life (QOL).
Results:
There was no significant interaction effect between group and time for the symptom cluster overall and for fatigue and anxiety. However, a significant trend towards improvement was observed on fatigue (P = .004), dyspnea (P = .002), and anxiety (P = .049) in the Qigong group from baseline assessment to the end of intervention at the 6th week (within-group changes). Improvements in dyspnea and in the secondary outcomes of cough, global health status, functional well-being and QOL symptom scales were statistically significant between the 2 groups (P = .001, .014, .021, .001, and .002, respectively).
Conclusion:
Qigong did not alleviate the symptom cluster experience. Nevertheless, this intervention was effective in reducing dyspnea and cough, and improving QOL. More than 6 weeks were needed, however, for detecting the effect of Qigong on improving dyspnea. Furthermore, men benefited more than women. It may not be beneficial to use Qigong to manage the symptom cluster consisting of fatigue, dyspnea, and anxiety, but it may be effective in managing respiratory symptoms (secondary outcomes needing further verification in future research). Future studies targeting symptom clusters should ensure the appropriateness of the combination of symptoms.
Trial registration:
ClinicalTrials.gov Identifier: NCT02977845. Registered November 30, 2016. https://clinicaltrials.gov/ct2/show/NCT02977845?term=Qigong&cond=Lung+Cancer&draw=2&rank=1
Introduction
Symptom management for patients with lung cancer (LC) should be a priority because of the high symptom burden in this population. However, symptom control in this population is still suboptimal. 1 Dyspnea, fatigue, and anxiety are distressing symptoms for LC survivors. 2 While symptoms often occur simultaneously, yet treatment or intervention strategies is usually focused on a single symptom. 3
The literature suggests that Qigong would be an appropriate approach to ease the patients’ symptoms. In a systematic review, 22 trials including various cancer populations on the efficacy of Qigong in symptom management were evaluated. 4 The findings indicated that the Qigong group had a significant improvement in symptoms at post-intervention compared with the control group or there was an observed positive trend from pre- to post- intervention scores for physical symptoms (fatigue, pain, dyspnea, weakness, lack of energy, nausea, dry mouth, constipation, early satiety, vomiting, and anorexia) or psychological symptoms (depression, anxiety, and mood disturbance) and quality of life. 4 These results are promising. However, the findings from those studies still require further affirmation due to their methodological shortcomings such as small sample sizes, differences between control and experimental groups, and high attrition rates. 5 Furthermore, Qigong is not a vigorous exercise which may make it more appropriate for a typically older cancer population, and in the context of this trial it is a culturally-relevant and accepted exercise programme.
While traditional interventional symptom research has typically focused on a single symptom, the realization of the interrelationships between co-existing symptoms has shifted more recently the focus of such interventions on symptom clusters 6 on which interventions may provide a stronger effect on symptom management. Studies by Cheville et al 7 and Molassiotis et al 8 have highlighted a symptom cluster of fatigue, dyspnea, and cough in the LC population, named the respiratory distress symptom cluster. 8 However, poor patient outcomes were associated only with fatigue and dyspnea. Another study conducted by Chan et al 9 on patients with LC receiving palliative radiation treatment identified the symptoms of breathlessness, fatigue, and anxiety as a cluster. Brown et al 10 explored symptom clusters in women with lung cancer and showed that participants suffered from several clusters which consisted of 4 to 6 concurrent symptoms. Although these clusters were different, fatigue and dyspnea were essential parts of all. Theoretically, it is hypothesized that the integration of dyspnea, fatigue, and anxiety, being the 3 central and most distressing lung cancer symptoms, would enhance the effectiveness of an intervention without bringing any burden to the participants. 11 However, there is no empirical evidence about the effectiveness of such integrative interventions.
In responding to the question raised by symptom management theorists on the efficacy of interventions with a focus on a group of interrelated symptoms, or symptom clusters, the current study, therefore, was set out to investigate the effects of Qigong on the symptom cluster of dyspnea, fatigue, and anxiety in patients with LC. Key aims of the study included: (1) to assess the effect of Qigong on managing dyspnea, fatigue, and anxiety (as a cluster) in patients with LC (primary aim); and (2) to explore the effect of Qigong on cough, which is another common symptom linked with dyspnea, fatigue, and anxiety as a cluster in lung cancer patients 8 and QOL dimensions (secondary aim).
Methods
This was a randomized, single blinded, parallel group, waitlist-controlled trial conducted from January 2017 to December 2017. It was registered with ClinicalTrials.gov, NCT02977845. The study subjects included patients living with a diagnosis of LC. As shown in Figure 1, a total of 156 eligible patients with LC were randomized to a Qigong group (n = 78) or a waitlist control group (n = 78). The study was conducted at the National Lung Hospital and Nam Dinh General hospital in Vietnam. Patients in the Qigong group completed 6 weeks of Qigong practice, while patients in the waitlist control group received usual care during the study period and were offered Qigong sessions afterwards.

CONSORT Flow Diagram showing the number of participants through the trial.
Inclusion Criteria
Patients were included if they were:
(a) Aged 18 or above;
(b) Diagnosed with invasive lung cancer [Non-small cell lung cancer (NSCLC) or Small cell lung cancer (SCLC)];
(c) Completed chemotherapy and/or radiotherapy at least 4 weeks before participating in the study;
(d) Physically able to participate in activities of daily life (ECOG score 0-2)
(e) Patients reporting all 3 symptoms of the cluster (dyspnea, fatigue, and anxiety) in the previous week and ranking the severity of at least 2 of these symptoms as ≥3 on a 0- to 10-point numeric rating scale at the time of recruitment.
Patients were excluded for the following reasons:
(1) Known history of major psychiatric illness;
(2) Presenting with risks associated with physical activity, including severe cachexia (muscle loss and weakness, which doctors believed would prevent patients from completing a set of exercises); frequent dizziness; bone pain; or severe nausea;
(3) Having past or current experience with mind-body practices that blended movement with meditative practices, such as Yoga, Tai Chi, or Qigong;
(4) Estimated life expectancy being less than 6 months (as determined by their physicians).
(5) Having visual problems or deafness.
Randomization
After the completion of baseline measurements, eligible patients were randomly assigned to either the Qigong group or the waitlist control group following block randomization procedures and according to the ID assigned to each patient in the order of enrolment against a computer-generated randomization list with a 1:1 allocation ratio and a block size of 6. For the block randomization, the online application Research Randomizer was used to produce the randomization block number, which was done immediately after consent. The randomization table was prepared independently by an academic person who did not know the design of the trial and was not involved in the study. While blinding of the intervention was not possible for the participants and the Qigong master delivering the intervention, the research team, the research assistants who collected the data from the participants and the clinicians treating the participants were all blinded to the group allocation. The researcher who analyzed the data and the statistician who supported the researcher in the analysis were also blinded to the allocation until after the completion of the data analysis.
Intervention
In addition to usual care, Qigong training was provided to participants in the intervention group. A professional coach with 12 years of experience in teaching Qigong was employed to guide the participants’ training. The training protocol was developed according to the “Qigong Standard” enacted by the Chulalongkorn University, Thailand. 12 The training involved a series of simple, repeated practices including body posture/movement, breathing practice, and meditation performed in synchrony. It mainly consisted of gentle movements designed to bring about a deep state of relaxation and included 7 postures. This Qigong protocol produced small-to-large effects on symptom management in various populations and medical conditions. 13
Participants in the intervention group (6 persons in each Qigong training section) received a 90-minute Qigong training, twice per week for the first 2 weeks to intensify their learning of Qigong intervention. For the next 4 weeks, participants were asked to practice Qigong at their home for at least 30 minutes a day, 5 days per week, and to record the frequency of practice and the number of minutes of practice. The home exercises were the same as those practiced in the training sessions. An instructional DVD which was modified from the original Thai version with the performance of the Qigong master with music and Vietnamese description in the background and a guidebook were provided to each participant for guidance. The researcher called the participants every week to assess their compliance with the home program, to encourage participants to continue practicing and to ensure that the training dose was adequate and recorded in a logbook. After the 6-week intervention period, all participants started an additional 6-week unsupervised practice and kept a log of their daily activity during the follow-up period.
Control Group
The waitlist control group received the usual care provided by the hospitals, health care professionals or caregivers and participated in the Qigong training after the follow-up period. Usual care included a mandatory individual briefing on the LC care procedure (nursing care after completion of medical treatment) and about 5 to 10 minutes of discussion on symptom management (ie, using oxygen for dyspnea) by a registered nurse before discharge. An optional group talk, which was given by a registered nurse and a medical social worker about general care, was available for patients before and/or after they returned to the community. No patient in this group practiced Qigong for the duration of their involvement in the trial.
Outcome Measures
Baseline Characteristics
The participants’ demographic characteristics (eg, age, sex, education, marital status, and occupation) and history of the disease, disease status, and treatments received were obtained from the patients.
Primary Outcome Measures
The Functional Assessment of Cancer Therapy-Fatigue (FACT-F), a subscale of the FACIT questionnaire, consists of 13 items measuring the intensity of fatigue and fatigue-related concerns in the previous 7 days. 14 Each item is rated using a 5-point Likert scale, ranging from 0 to 4.
Cancer Dyspnea Scale (CDS) consists of 12-items and 3 subscales, including “sense of effort,” “sense of anxiety,” and “sense of discomfort.” Patients responded by scoring from 1 “not at all” to 5 “very much” on the 5-point Likert scale. 15
Depression Anxiety Stress Scales 21, anxiety subscale (DASS21-A), has 7 items, assessing symptoms of autonomic arousal, skeletal musculature effects, situational anxiety and subjective experience of anxious affect. 16
All scales have been translated into Vietnamese and the translated versions demonstrated good psychometric properties. 17 These scales were used at baseline (T0), after 6 weeks of the intervention (T1: primary outcome point), and at the end of the follow-up period (T2: at 6 weeks after the intervention). The composite score of the above scales for the symptom cluster, including the vector of means on the transformed (out of 100) scores for fatigue, dyspnea, and anxiety across time was considered as the primary outcome. To reduce the possibility of Type I error, the original alpha value of 0.05 was divided by 3 for a new alpha value of 0.017 or below indicative of statistically significant results. 18
Secondary Outcome Measures
The Manchester Cough in Lung Cancer Scale (MCLCS) is a 10-item, unidimensional scale that measures patients’ experience with cough in terms of its frequency, intensity, and bothersomeness. 19
The European Organisation for Research and Treatment of Cancer—Quality of life questionnaire (EORTC-QLQ-C30), includes both multi-item scales and single-item measures, incorporating 5 functional scales, 3 symptom scales, a global health status/QOL scale, and 6 single items. The Lung Cancer module (LC-13 subscale), focuses on LC-specific symptoms and side effects (dyspnea, cough, site-specific pain, peripheral neuropathy, sore mouth, alopecia). 20
Data Collection
Ethical approval from the 2 hospitals involved in the study and The Hong Kong Polytechnic University’s ethics committee was obtained before data collection. Two research assistants were trained about all issues related to the study and the data collection process. They were required to join training sessions on data collection, which was conducted by the researcher (role-play simulation), before they were fully involved in this study. Participants completed the questionnaires before randomization (baseline assessment), at the end of the last Qigong session (intervention group) and beginning and end of intervention post trial (control group) by themselves, under supervision by one of the researchers in case any clarification was needed. The 12-week assessment for the intervention group was done over the phone.
Statistical Analysis
An intention to treat (ITT) analysis was used to analyse the data, and multiple imputation methods were used to fill in missing items. Descriptive statistics were used to describe the sample characteristics as well as fatigue, dyspnea, anxiety, cough and QOL. Generalized Estimating Equation (GEE) models were performed to examine the effect of Qigong on the symptom cluster. The analyses of changes in outcome variables between T0 and T1 was the primary focus; data relating to changes between T0 and T2 were only assessed in an exploratory manner to examine longer-term effects. An interaction term (group difference x time) was added to each model to investigate the interactive effects of Qigong and time. SPSS v.23 was used for the data analysis.
Results
Participants were 156 patients with LC, with most being male (74.4%), with a mean age of 56.84 ± 9.45 years, and with the majority having completed secondary education (53.2%). Most of them were in stage IV and III LC (61.5% and 29.5% respectively). They had been treated for a mean of 5.67 ± 2.62 cycles of chemotherapy, and the majority (55.1%) had received at least 4 cycles of chemotherapy (Table 1). Of the 78 participants in the intervention group, 48 (61.5%) completed the 6-week Qigong program, and 66 (84.6%) completed at least half of the 6-week intervention. The practice adherence rate was 61.5% (Figure 1). No Qigong-related adverse reactions were reported by the participants in the intervention group.
Demographic Data, Disease Characteristics, and Symptoms for All Participants in the Qigong and Control Groups (n = 156).
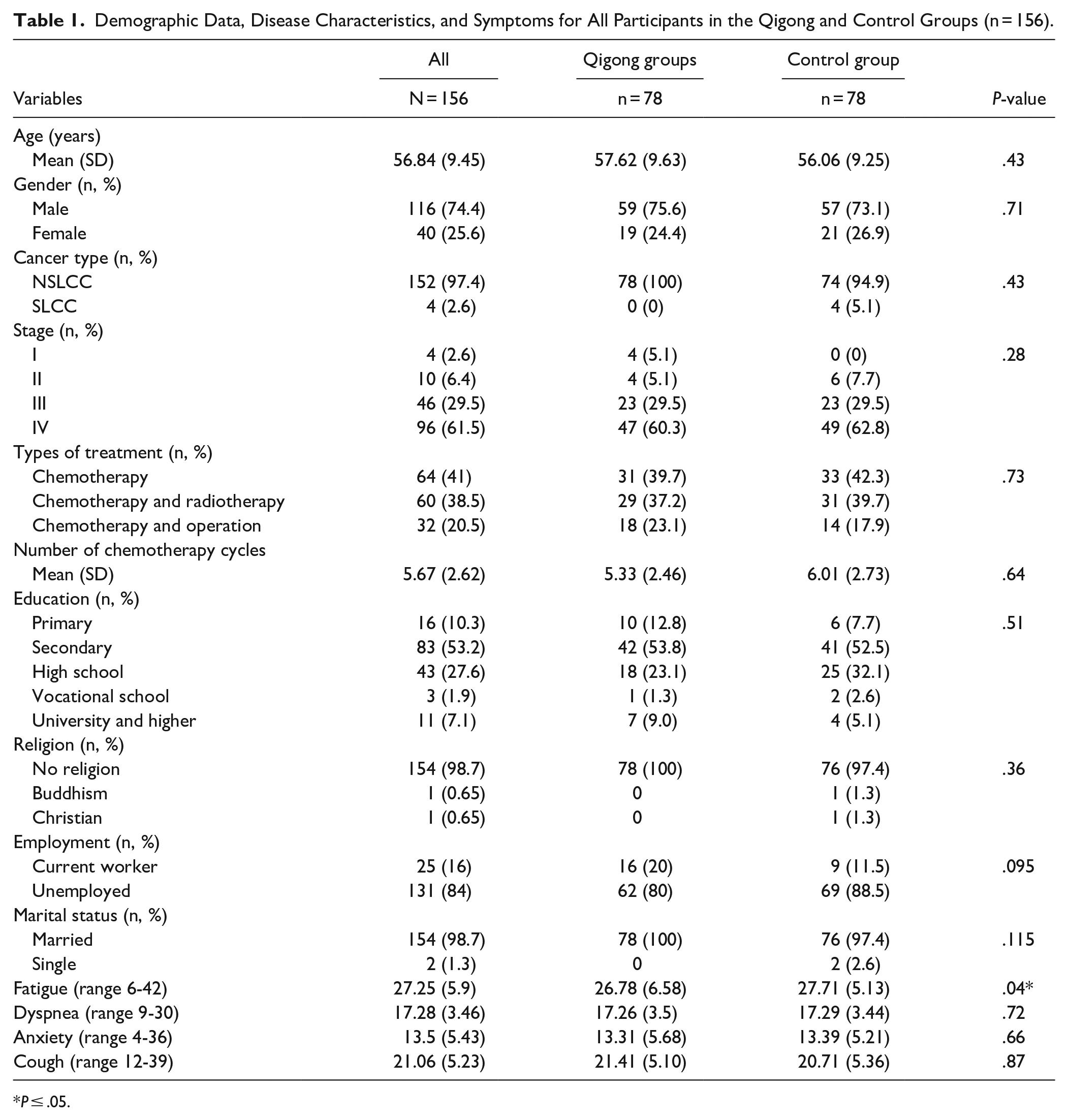
P ≤ .05.
Primary Outcome
Regarding the symptom cluster, there was no improvement in the between-groups analysis of the 2 groups, but there were within-group significant changes in the Qigong group, which suggests that there were some variations in the effect of the intervention (Figure 2). There was also a trend in improvement in within-group assessment of the Qigong group between the baseline and the 6th week (P = .002), and this remained similar until the 12th week by 5.1 points better from baseline (P = .015) (Tables 2 and 3). Analyzing demographic and pathology factors related to symptoms such as age, gender, occupation, types of LC, stage, type of treatment, and the number of cycles, the results from GEE showed that only gender was a factor influencing the effectiveness of the Qigong intervention (males had more improvement, P = .03). Regarding the symptoms individually, there was a trend in improvement of fatigue within-groups in the Qigong group with a mean difference of 2.25 (P = .004) from baseline to 6th week and also a mean difference of 2.71 (P = .021) from baseline to 12th week. With regards to dyspnea, a significant difference was observed at the 6th week and 12th week between the Qigong and waitlist control groups (P = .014 and P = .025, respectively). There was also a trend in improvement within-groups in the Qigong group on anxiety between the baseline and the 6th week (P = .049) and 12th week (P = .025) (Figure 3).
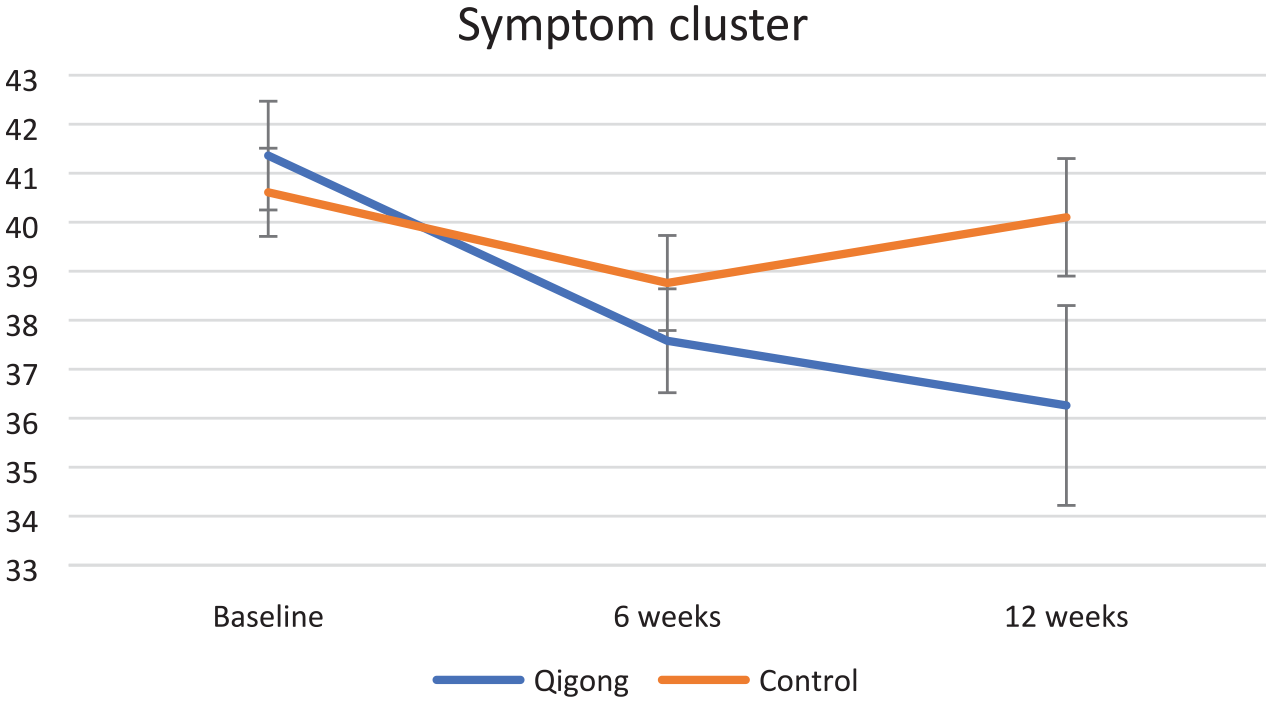
Changes in the symptom cluster of fatigue, dyspnea, and anxiety scores across time (composite score of FACT-F, CDS and DASS).
Generalized Estimating Equations (GEE) Analysis in the Trial Outcomes.

Higher score indicates higher symptom burden;
Higher score indicates less fatigue.
Higher score indicates better quality of life indicators
Alpha level of .017.
Pairwise Comparisons in the Trial Outcomes (Within-Groups Comparisons [“Qigong” or “Control” Group Rows] and Between-Groups Comparisons [“Qigong and Control” Group Row]).

Higher scores indicate higher symptom burden.
Higher score indicates less fatigue.
Higher score indicates better quality of life indicators.
Alpha level of .017.
P ≤ .05.

Changes in fatigue (FACT-F scale), dyspnea (CDS), and anxiety (DASS) scores across time (individual scales).
Secondary Outcomes
Regarding cough, which was of moderate intensity in this sample, a significant interaction term (group × time) of the cough across time was observed, with P = .001 and P = .017 at the 6th and 12th week, respectively (Table 2). In addition, a significant difference was observed at the 6th and 12th week between-groups of the Qigong and waitlist control groups (P = .001 and P = .039, respectively). There was a change of 4.25 points in the cough score from baseline to the 6th week in the Qigong group (Table 3 and Figure 4). Regarding QOL, between group statistically significant improvements were observed on global health status (P = .021), functional score (P = .001), and symptoms subscale of QOL (P = .002) at week 6 (Table 2). There were no differences between groups over time with regards to LC13 subscale, and in both groups scores increased over time.
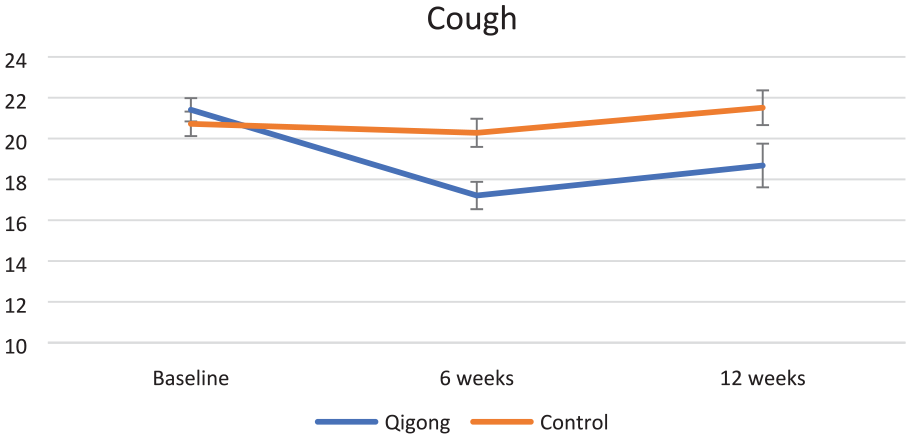
Changes in cough (MCLCS) scores across time.
Discussion
The results did not support the hypothesis that patients with LC who received Qigong would show greater improvements in fatigue, dyspnea, and anxiety as a symptom cluster across time than those who receive usual care, under the condition that the patients in the Qigong group complied with the protocol. However, it did improve significantly the symptoms of dyspnea and cough as single symptoms.
There was also no significant difference in terms of group × time effect regarding fatigue; this may be explained by the increasing physical activity, doing exercise regularly, and psychological relaxation; an improving trend was found in the Qigong group only. The change in fatigue in the Qigong group in the current study (2.71 points) was close to the published MCID for fatigue. 21 Our finding is supported by past research; for example, Oh et al 22 reported that compared with usual care, a 10-week medical Qigong program reduced fatigue for patients with breast, lung, prostate, and other cancers. Campo et al 23 found that a 12-week Qigong intervention helped prostate cancer survivors with chronic fatigue to lower its level and distress. Yeh and Chung 24 demonstrated that in non-Hodgkin’s lymphoma patients who were undergoing chemotherapy, the average fatigue intensity significantly decreased over time in the Qigong group who exercised 20-minutes twice daily for 21 days. A systematic review and meta-analysis of 22 trials also showed that Tai Chi Qigong improves fatigue, 25 although Tai Chi Qigong may have subtle differences in the exercises used compared to the ones in the current trial.
The findings of the current study support that Qigong significantly improved dyspnea at the 6th week and the 12th week between the Qigong and waitlist control groups with a mean difference of 1.15 (P = .014) and 1.50 (P = .025), respectively; this is not consistent with the findings of other controlled studies. For example, Fong et al 26 evaluated the effects of Qigong on cancer-related symptoms in 52 nasopharyngeal cancer survivors. The experimental group received a 6-month Qigong training program consisting of weekly 1.5-hour face-to-face training and home practice (3 times/week). Qigong training resulted in no apparent improvement in dyspnea. In addition, Oh et al 22 reported no significant difference in symptoms (including dyspnea) in cancer patients who received 8 weeks of Medical Qigong training. The result of the current study can be explained by the type of deep breathing exercises used when practicing Qigong, leading to direct effect on the lung function and a more comfortable breathing. Indeed, in a review of exercise studies that included medical qigong, improvements in dyspnea were shown. 27
A significant difference in the scores of cough was observed at both the 6th and 12th weeks between the Qigong and waitlist control groups, with a mean difference of 3.07 (P = .001) and 2.82 (P = .039), respectively. The cough score was of moderate intensity (maximum score of 40) and similar to past studies.19,28,29 Moreover, a change of 4.25 units from baseline to the 6th week in the Qigong group was close to the minimal clinically important difference score on cough assessment. According to Yorke et al 30 a 4.4-point difference of cough on the MCLC scale is considered to reflect a clinically important difference in LC populations.
The results indicated that Qigong helped manage respiratory symptoms such as dyspnea and cough more than the cluster symptoms. Qigong practice usually is composed of movement with exercises and visualization plus positive expectations. All these elements may have a beneficial effect on psychological well-being. It is acknowledged that the current research findings will not provide answers to whether Qigong (movements with breathing exercise and visualization) alone is beneficial to psychological well-being. Positive expectations may add to effects related to the Qigong intervention, to form a multi-component mind-body practice instead of a single (Qigong) intervention. 31 Therefore, the hypothesis is that the “integrative skill of mindfulness-led breathing with accordant body postures (a critical component) generates mechanical stimuli (mediators) to produce changes on qi and the body-wide meridian network (biological mechanisms) in addition to emotional regulation.” 32
The findings of this study suggest that Qigong has a positive influence on QOL in patients with LC. There was a significant difference within and between groups on global health status at the 6th week, functional well-being at the 12th week and the symptom scales at the 6th week, confirming previous work. Studies have confirmed that Qigong can significantly improve QOL outcomes,33-37 and this was further supported by a systematic review of Tai Chi Qigong. 25 Hence, in future research, the symptom cluster that includes dyspnea and cough (respiratory symptoms) should be considered as the key outcome, particularly for Qigong practice that includes breathing exercises, as used in the current trial.
Limitations
The subjects were mainly recruited from 2 hospitals from the Northern part of Vietnam; only patients with LC and presenting the cluster of 3 symptoms of fatigue, dyspnea and anxiety were included, which may limit the generalisability of our study findings. Also, the rate of drop out was high at the 6th week of intervention and the 12th week follow-up (38%, 60% in the Qigong group and 15%, 40% in the waitlist control group respectively) and the intervention adherence in later weeks was not assessed. This may explain why the differences between the 2 groups were more significant at the 6th week than at the 12th week. While the attrition rate was high, it is not unusual in supportive/palliative care trials involving advanced cancer patients. Indeed a review of 18 trials showed that attrition was 26% for the primary endpoint and 44% at the end of the study, with key reasons being participants feeling unwell or death. 38 There was a higher rate of drop out in the Qigong group and this may indicate that those who remained in the trial were those who perceived a benefit. Due to the nature of the intervention, study subjects were aware of their treatment allocation. The composite score for the cluster, although supported in the literature, may not be an appropriate way to calculate a combined “effect”; this was used only as a numerical score to facilitate the analysis acknowledging that any given change in the total score may not really be informative of what is happening with each symptom. More robust ways of measuring a combined effect of a cluster of symptoms is required to be identified in the future in order to further the science of symptom clusters. Furthermore, we did not have an objective assessment tool to indicate how much the subjects could master the exercise. Additionally, the level of supervision of the exercise regimen, the skills of the Qigong master, and the intensity of the exercises can vary in different groups and can ultimately affect the effectiveness of the exercises, even though in our trial these were controlled through the use of a specific protocol for its delivery and use of only one Qigong master. Finally, although we tried to deal with the problem of non-specific effects by introducing block randomization, we still faced the possibility of the experimenter-expectancy effect.
Recommendations
The empirical evidence of the current study does not support the management of fatigue, dyspnea, and anxiety as a symptom cluster with qigong. However, the findings of this study are encouraging for the management of respiratory symptoms and enrich the practical knowledge about cancer symptom management. Hence, the respiratory distress symptom cluster identified in past studies 8 may be an appropriate target for such an intervention. When designing interventions based on symptom clusters, it is important to combine symptoms that may have “shared” mechanisms in order to improve common symptom experience. Researchers are encouraged to advance the theory, measurement, and management of respiratory symptoms, especially to clarify the mechanisms of the interrelationships between symptoms within clusters, and to evaluate integrative interventions. 30 Clinicians should be prudent when they view some symptoms as a cluster which will be able to exert influence and be influenced with each other.39,40 Management of symptoms as a cluster should be a contemporary approach to quality cancer and palliative care that is effective and efficatious. 41
Conclusions
This study was set out to evaluate the effects of Qigong on dyspnea, fatigue, and anxiety as a symptom cluster in patients with LC. Our findings suggest that Qigong did not alleviate this symptom cluster with a 6-week exercise programme; Qigong, however, was effective in reducing dyspnea and cough, and improving QOL. In addition, more than 6 weeks were needed to detect the effect of Qigong on improving dyspnea. Furthermore, men benefited more than women in the management of respiratory symptoms from the Qigong exercises. The conclusion is that the primary outcome (symptom cluster) had a trend only in improvement, and as those symptoms found to be significantly improved (ie, dyspnea, cough) were secondary outcomes, the effect of Qigong on managing respiratory symptoms needs to be further investigated before concrete conclusions are drawn.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.