
Abstract
Background:
Current treatment for head and neck cancers (HNCs) have led to an improved survival. However, the sequelae of cancer treatment often result in trismus, or reduced mouth opening. The purpose of this report is to identify interventional studies for trismus management in HNC patients.
Methods:
A search of PubMed, Embase, Cumulated Index to Nursing and Allied Health Literature, and the Cochrane Library was conducted in March 2020 for randomized controlled trials (RCTs) involving interventions for trismus for head and neck cancer within 10 years. Intervention could involve the use of an exercise regime, jaw rehabilitation device, technological device, medication or massage therapy. The primary outcome was the measurement of mouth opening.
Results:
Eleven RCTs involving a total of 685 patients with HNC were included. Six RCTs evaluated the effectiveness of a jaw mobilization device with exercises; there was no significant benefit of an exercise regime with a jaw mobilization device either initiated before, during or after treatment compared to no exercise. Two RCTs compared 2 intervention groups that involved exercises only, with 1 study assessing the benefit of weekly supervised physical therapy with gum chewing and another evaluating the benefit of immediate (1-2 days) versus delayed (7-10 days) initiation of exercise post-surgery; there was no significant difference between groups in either study. One RCT that recruited only patients with trismus demonstrated that an exercise regime in combination with low-level laser therapy or low-intensity ultrasound had superior results in mouth opening measurements compared to exercise alone. Two RCTs compared intervention groups with and without follow-up reminders; both studies showed a significant improvement in mouth opening measurements in groups with follow-up reminders.
Conclusion:
This systematic review did not convey a clear consensus as to optimal intervention for trismus in HNC patients. A variety of exercise regimens and jaw rehabilitation devices appear to have comparable effectiveness. However, efforts focused on increasing adherence to a particular intervention protocol may positively impact mouth opening measures in head and neck cancer patients. Also, low-level laser therapy and low-intensity ultrasound coupled with exercise may be beneficial for patients with trismus.
Keywords
Introduction
Head and neck cancers (HNC) are a heterogenous group of cancers that originate from the oral cavity, oropharynx, hypopharynx, and larynx and are twice as likely to happen in men than in women. HNC is currently the eighth most common cancer in men in the United States. 1 With surgery and/or radiotherapy (RT) as standard treatments in HNC coupled with chemotherapy (CT) as neoadjuvant or adjuvant therapy in advanced stage HNC, the survival of HNC has significantly improved since the late 20th century; the relative 5-year survival rate is 65% for all HNC and up to 84% for local cancers.1,2 Despite improved survival, post-surgical scarring and radiotherapy induced fibrosis in the pterygoid or masseter muscles and temporomandibular joint (TMJ) can result in adverse functional outcomes related to mouth opening, voice, speech and swallowing. These impairments may start as early as during treatment and persist for up to many years after treatment,3-5 causing acute decline in quality of life (QoL) 6 that may not return to pre-treatment levels. 7
Trismus is one of the common side effects of HNC treatment, along with dysphagia, xerostomia, mucositis and radiation dermatitis. 8 Trismus is a disorder in which patients have decreased range of motion of the muscles of mastication, resulting in inability to in opening the mouth more than 35mm.9,10 The incidence of trismus in HNC post-treatment is high and persistent; it has been found to affect up to 30.7% of HNC patients treated with chemoradiotherapy (CRT) 11 and 39% of HNC patients treated with RT and surgery at 6 months post treatment, even with preventive exercises.10,12
According to the existing literature, rehabilitation aimed at preventing trismus consists of either passive or active stretches to the mandible and may involve jaw mobilizing devices such as the TheraBite (Atos Medical, Horby, Sweden), Dynasplint (Dynasplint Systems, Inc., Maryland, USA) or stacked tongue depressors. Recent advances in treatment such as the use of intensity modulated radiation therapy (IMRT) have greatly decreased the prevalence of trismus and resulted in better functional outcomes.11,13 However, there remains a need to develop an evidence-based approach for trismus prevention and management given the condition’s debilitating nature. Preventative and therapeutic rehabilitation for trismus is considered the standard of care but there is currently no consensus regarding rehabilitation protocol.12,14,15
The purpose of this systematic review is to (1) robustly identify interventional studies for trismus management in HNC patients, (2) assess methodological quality of the identified studies, (3) summarize results of these studies, and (4) propose future research directions in this area.
Methods
Search strategy
A comprehensive literature search was conducted between March 19, 2020 and March 26, 2020. A professional librarian experienced in health science literature search assisted with formulating, revising, and finalizing a search strategy. The search strategy included 4 major databases: PubMed, Embase, Cumulated Index to Nursing and Allied Health Literature (CINAHL), and the Cochrane library. Dated search records for all 4 databases are available in Supplemental Appendix A. All searches filtered for human studies that were written in English and published within the past 10 years were included.
A search was initially conducted in PubMed. The first set of search terms (see Supplemental Appendix A) yielded 240 articles. After reviewing the titles and abstracts of these articles in collaboration with the librarian, the search terms were broadened to include synonymous words and phrases (see Supplemental Appendix A). The expanded set of search terms yielded an additional 80 articles from PubMed.
Next, Embase and CINAHL were queried (see Supplemental Appendix A) yielding 843 and 198 articles, respectively. The Cochrane library search resulted in 10 systematic reviews and 111 clinical trials. The clinical trials were scanned for relevant articles, of which 12 out of 14 relevant studies were already identified in either PubMed, Embase or CINAHL. The full texts for the remaining 2 studies were requested and assessed.
Screening process
All 1482 article citations were uploaded to a citation manager (ProQuest Refworks). After removing the duplicates, articles were screened according to the evidence-based Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) system. This step-by-step process is outlined in detail in a PRISMA flow diagram (Figure 1). After a review of titles, abstracts, and full texts excluded 1275 articles (Figure 1), 52 articles remained and were considered for inclusion in the systematic review.
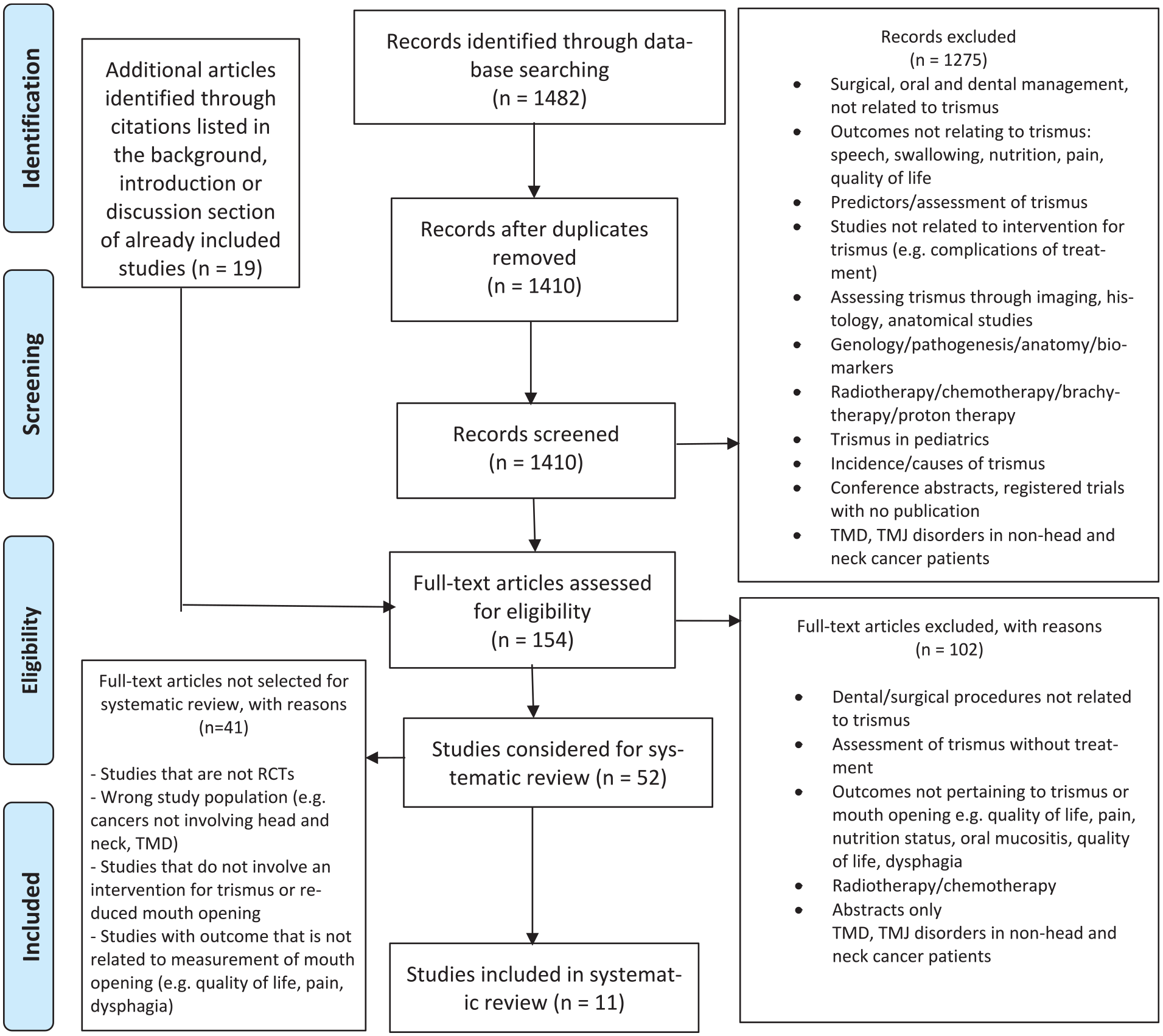
PRISMA 2009 flow diagram.
Inclusion criteria
Studies were included if they satisfied the following criteria:
Study design: Randomized controlled trial (RCT)
Population: Patients with HNC
Intervention: Any management strategies for trismus or reduced mouth opening that involve the use of an exercise regimen, device, technology, medication, or massage therapy
Outcome: Measurement of mouth opening
Two independent reviewers evaluated the 52 articles and identified a total of 11 articles that met the inclusion criteria were included in the final systematic review (Figure 1).
Data extraction and analysis
Data were extracted from the 11 RCTs by 2 independent reviewers using a standardized spreadsheet. Reviewers recorded study author(s), year of publication, purpose and design, sample and setting, independent and dependent variables, intervention and control conditions, strengths and limitations, and conclusions. The senior investigator then reviewed the extracted data, and consensus was reached by discussion between the 3 parties. The 2 reviewers were also trained by a senior investigator to assess for methodological quality and risk of bias using the validated Physiotherapy Evidence Database (PEDro) scale. 16 Both reviewers then independently assigned PEDro scores to each of the 11 RCTs using a standardized table. Subsequently, the 2 reviewers met and discussed any discrepancies; consensus was reached all on but 1 item. The senior investigator reviewed this single item and made a final independent decision. This method of independent scoring by 2 reviewers with a third reviewer arbitrating a disagreement increases the accuracy of quality rating using the PEDro scale, which otherwise has an acceptable inter-rater reliability. 17 The creators of the PEDro scale report that scores of 0 to 4 (out of 10) are considered “poor,” 4 to 5 “fair,” 6 to 8 “good,” and 9 to 10 “excellent,” and that scores of 8 or above are optimal for complex interventions such as exercise, but these classifications have not been validated. 16
Results
Study selection and characteristics
The combined database searches resulted in 1410 unique articles, of which 154 were assessed for full-text eligibility. In the end, 11 eligible studies were included for systematic review.18-28 Table 1 provides detailed characteristics of the included studies. All studies were published in English, used a randomized control design, and reported the effect of interventions to improve trismus following HNC treatment. The sample sizes ranged from 27 patients to 132 patients, with a mean age ranging from 42.3 years to 67.8 years. Cancer stage varied from I to IV, and treatment modalities included radiation, surgery, chemotherapy, or combinations of the former.
Characteristics of Included Studies.

Abbreviations: SCC, squamous cell carcinoma; S, surgery; C, chemotherapy; RT, radiotherapy; NPC, nasopharyngeal carcinoma; (C)RT, chemoradiotherapy; CCRT, concomitant chemoradiotherapy; B, brachytherapy; MMO, maximal mouth opening; MIO, maximal interincisal opening; DTS, dynasplint trismus system.
Only some patients received this treatment.
Risk of Bias in Included RCTs
Overall, most RCTs had low risk of bias; with 10 RCTs rated at least a “fair” (≥4/10) and 6 RCTs rated “good” or higher (≥6/10); 16 the results are presented in Table 2. Of note, no consensus cutoff PEDro scores currently exist for acceptable risk of bias. 29 All studies described the eligibility criteria and employed a random allocation approach. However, the majority of the studies failed to blind subjects (n = 10), therapists (n = 10), and assessors (n = 7). There were also a fair number of studies who did not have adequate follow-up (n = 5); either the mouth opening was not measured in at least 85% of the allocated subjects at any time point, or information was missing. 16 At 6 months follow-up,19,23 2 studies reported attrition rates from 30% to 50% in either control or intervention groups and 1 study reported a 56% attrition rate that led to a premature cessation of the study. 21
Quality Assessment of RCTs According to the PEDro Scale.

1 = Yes; 0 = No.
Abbreviations: RCT, randomized controlled trial; PEDro, physiotherapy evidence database.
Data Analysis Method
Due to the heterogeneity in specific interventions used to treat trismus in this patient population, we were unable to perform a quantitative meta-analysis. Thus, we conducted a systematic review. Table 3 highlights the interventions used by each study and a summary of results, among other variables, and can be referred to throughout the remainder of this section. Overall, there were 4 broad categories of treatment strategy employed in the 11 RCTs.
Interventions.

Abbreviations: Jaw rehab device*, TheraBite jaw motion rehabilitation system; Jaw rehab device^, jaw dynasplint system; MMO, maximal mouth opening; RT, radiation therapy; PT, physical therapy; MOD, mouth opening difficulties; MIO, maximal interincisor opening.
Intervention Category 1: Exercise Regimen with Jaw Rehabilitation Device
Six RCTs evaluated the effectiveness of a combination of jaw rehabilitation device and exercises.18-23 Intervention periods ranged from 3 to 12 months, exercise frequency ranged from 3 to 5 times per day. All but 1 RCT studied patients in the acute period (<3 months) after treatment with surgery, RT, or CCRT; the other included patients >36 months after cancer treatment. 21
Out of the 6 RCTs in this category, one had a statistically significant difference in mouth opening between the 2 study arms. 23 In this RCT, patients who used the TheraBite in addition to stretching exercises had higher MIO at 6 months after RT than those who did stretching exercises alone (P = .019). The remaining 5 RCTs did not have significant results.18-22 Their characteristics are described below and in greater detail in Tables 2 and 3:
Two RCTs compared a jaw rehabilitation device (TheraBite) to a control group that did not perform any exercises at all.18,20 Neither showed a significant difference in maximal interincisor opening (MIO) 12 months after RT (P = .264 for 1 RCT and unspecified for the other).
Three RCTs began trismus interventions prophylactically, that is, prior to cancer treatment, in all study arms. Interventions began 1 to 2 weeks before RT, 18 2 weeks before CCRT, 22 or “before RT”. 20 There were no statistical significant differences in maximal mouth opening (MMO) 18 (P = .264) or MIO 20 between the intervention and control groups in any of these studies.
Two RCTs used alternatives to the conventional jaw rehabilitation devices available on the market (eg, TheraBite, Dynasplint). A “hyperboloid device” showed no benefit to mouth opening over a no-exercises control group. 18 Wooden spatulas also did not have significantly different mouth opening outcomes when compared to TheraBite. 19
Intervention Category 2: Exercise Regimen with Ultrasound or Laser Therapy
One RCT evaluated the effectiveness of an exercise regimen with either low intensity ultrasound or low-level laser therapy, compared to a control group with exercises only. 24 Post-intervention mouth opening measurements in both the low intensity ultrasound and the low-level laser therapy groups showed significant improvement compared to the control group (P < .05).
Intervention Category 3: Exercise Regimen Only
Two RCTs compared the effectiveness of various exercise regimens.25,26 Weekly supervised sessions and gum chewing exercises in addition to a standardized exercise regimen did not confer any significant benefit in MIO at 12 months’ follow-up when compared to standardized exercise alone. 25 There was also no significant difference between MIO at 6 months post-operative follow-up in groups who received early exercise therapy (starting 1-2 days post-op) versus late exercise therapy (starting 7-10 days post-op). 26
Intervention Category 4: Exercise Regimen with Increased Contact from Healthcare Provider
Two RCTs assessed the effect of increased direct or indirect contact with providers on mouth opening outcomes. This entailed either use of a smart-phone app 27 or provider phone call 28 to monitor patients’ progress and answer questions. Control groups received standard instructions about post-operative exercise regimen and follow-up appointments, but had less frequent check-ins with providers. Follow up period ranged from 3 to 6 months. Both of these RCTs demonstrated a statistically significant increase in mouth opening in the intervention group compared to the control group.
Discussion
This systematic review analyzed RCTs examining non-operative interventions for trismus in HNC patients, with interventions ranging from use of different rehab devices to specialized exercise protocols. The majority of RCTs did not show a significant difference between the intervention arm and the control arm. The authors therefore conclude that the existing RCTs on intervention for trismus do not provide a strong consensus as to the most effective intervention for trismus in HNC patients. However, our review produced an interesting and unexpected observation: that interventions focused on increasing adherence to a given treatment regimen (as shown in Di & Lee 27 and Wang et al 28 ) may provide a significant benefit even though interventions that change the prescribed treatment regimen itself largely do not.
From the studies that pertained to rehabilitation devices, data were mixed, and there was insufficient evidence to support a superior treatment method. Only one study, which examined the Dynasplint, reported a significant difference in mouth opening between the 2 trial arms at 6 months follow up, with P = .019. 23 However, the effect size was very small (0.5 cm), and the PEDro score for this study was the lowest out of the 11 RCTs reviewed, indicating a potentially high risk of bias. In another study, though the authors randomized patients to 2 arms, they failed to compare mouth opening data between the 2 groups. 30 They did, however, demonstrate a significant improvement in mouth opening within the entire cohort over the length of the study period, suggesting that more than 1 treatment strategy can be effective. The 4 remaining studies18-21 compared rehab devices (eg, TheraBite) to control groups and did not find a significant difference.
Two additional studies examined the effect of either the content or timing, respectively, of exercise-based therapy alone.25,26 Neither found a significant difference between study arms. These results, along with the rehab device results discussed in the previous paragraph, are concordant with the broader literature, including non-RCTs. Case series examining interventions such as devices, exercises, and even medications have shown improvement in mouth opening measurements over the study period, further supporting the claim that multiple methods can be effective.31-34 Case-control studies have shown mixed results, with some showing a significant difference between intervention and control groups, and others not.35-40 The existing body of literature further supports our review’s conclusion that there is still no clear consensus for optimal trismus management.
In some ways a subcategory of its own, Elgohary et al 24 compared exercise therapy plus either low intensity ultrasound (LIUS) or low-level laser therapy (LLLT) with exercise therapy alone. Unlike most other RCTs, results showed a significant benefit in mouth opening in both treatment groups compared to exercise therapy alone. Of note, the study population also included patients who developed trismus and pain, unlike other RCTs in this review, which recruited patients after cancer treatment whether or not they already had restrictions in mouth opening. This result is interesting and deserving of further study, although it could have been confounded by adherence. After receiving LIUS and LLLT, patients in the intervention groups underwent exercise therapy in the office, whereas the control group patients received only home-based exercise therapy. Adherence data for the home-based exercise therapy was not reported. The importance of this possible confounder is supported by results from the last 2 RCTs, which looked at methods to increase treatment adherence.
Di & Li developed a smartphone app with (1) reminders for follow-up appointments, (2) educational resources, (3) biweekly opportunities for virtual consultation with physicians. They found that patients who used the app had a significantly lower incidence of mouth opening difficulties at 6 months’ follow-up than a control group with the same prescribed exercise regimen but no app (P = .017). 27 In the other RCT, 28 both intervention and control groups received instructions to complete a particular exercise programs, but the intervention group also received regular phone calls from a provider to monitor progress. There was a significantly greater increase in mouth opening in the intervention group than control, with an effect size of 10.3 mm (P < .001). 28 These results suggest that efforts focused on increasing adherence to a particular intervention regimen may positively impact trismus-related outcome measures. Existing literature may support this concept. For example, Bragante et al 18 conducted a subgroup analysis in which adherent patients had significantly higher mouth opening measurements than nonadherent patients.
Strengths of this systematic review included a broad search of 4 databases, inclusion of only RCTs, and a rigorous review of RCT quality via the validated PEDro scale. Limitations included a small final number of randomized controlled trials, heterogeneity between the studies which precluded a direct comparison of data through meta-analysis and high risk of bias in some of the RCTs due to high attrition rates. Forty-five percent of the trials (n = 5/11) had an >15% attrition rate and thus scored 0 on the PEDro scale. 16 Although there is no particular level of loss to follow-up at which attrition related bias becomes an issue, it is a source of bias if the characteristics of the participants lost to follow up differ between the randomized groups and these characteristics are correlated to the primary outcome measure. 41 High attrition rates in trials involving supportive care for oncology population and have been reported to be 28% for primary endpoint and 44% for end-of-study endpoint; main reasons were patient withdrawal due to high symptom burden and clinical deterioration. 42
Some of the included RCTs also had heterogeneity with regard to primary tumor location, which could have influenced their conclusions. For certain head and neck cancers such as nasopharyngeal or malignant parapharyngeal tumors, trismus may be one of the first signs. 10 Trismus may also be a sequela of lymphedema, an insidious and often neglected adverse effect of HNC treatment. 43 Sandler et al 26 found that patients with oral tumors had overall smaller jaw opening, a difference that was statistically significant at 6-month post-operative assessment. Conversely, primary tumor site had no significant impact in mouth opening at 12 months in Hogdal et al (P = .63). 25 Other authors did not conduct a formal analysis of the impact of primary tumor site, but acknowledged the influence of this heterogeneity on mouth opening and rehabilitation outcomes, and suggested stratification based on primary tumor location and treatment in future studies.
Conclusion
This systematic review demonstrated that, thus far, no superior strategy has emerged for treatment of trismus in HNC patients; a variety of exercise regimens and rehab devices have comparable effectiveness. Interventions focusing on increasing adherence may increase mouth opening progress in HNC patients. Low-level laser therapy and low-intensity ultrasound coupled with exercise may also be beneficial for patients with trismus, but further investigation is needed. Clearly, more rigorously designed, high-quality clinical trials are needed to determine optimal interventions for treatment of trismus in HNC patients.
Supplemental Material
sj-docx-1-ict-10.1177_15347354211006474 – Supplemental material for Interventions for Trismus in Head and Neck Cancer Patients: A Systematic Review of Randomized Controlled Trials
Supplemental material, sj-docx-1-ict-10.1177_15347354211006474 for Interventions for Trismus in Head and Neck Cancer Patients: A Systematic Review of Randomized Controlled Trials by Shuzhen Chee, Yasmeen M. Byrnes, Kevin T. Chorath, Karthik Rajasekaran and Jie Deng in Integrative Cancer Therapies
Footnotes
Acknowledgements
The authors have no other acknowledgments to declare.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Jie Deng, PhD was supported by a Research Scholars Grant, RSG-16-207-01-PCSM, from the American Cancer Society. The American Cancer Society did not have a role in study design, collection, analysis, and interpretation of data and in writing the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.