
Abstract
Background:
Chemotherapy-induced peripheral neuropathy (CIPN) is an adverse event of taxanes, with no effective prevention or treatment available and a highly negative impact on patient quality of life. The aim of this study is to asses that the constant application of cooled cuffs on the hands and feet prevent and mitigate CIPN.
Methods:
Patients with breast, gynecologic, and pancreatic cancer who received weekly paclitaxel (PTX), PTX/carboplatin, and nab-paclitaxel (nab-PTX)/gemcitabine for any indication at the therapeutic scheduled dosage were included in this prospective study. Hilotherm Chemo care device forms a closed-loop system with cuffs and tubes through which a coolant flows at a temperature of 10 °C. CIPN was monitored using the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (edition 3.0), and the tolerability and side effects were scored by using the Common Terminology Criteria for Adverse Events (T4.03 2017).
Results:
To date, we have enrolled 64 patients. Of these, 54 (84%) completed all cooling cycles. Continuous cooling was well tolerated by all patients. No patients had grade >2 CIPN or had serious or lasting adverse events as a result of Hilotherapy. The median time to CIPN onset was 77 days for the entire population.
Conclusion:
Hilotherapy has good effectiveness and tolerability and seems to be able to prevent or reduce the symptoms of CIPN. We are still recruiting patients to obtain more data and to collect data at 3 months after the end of chemotherapy. Prospective studies seem to be warranted.
Introduction
Background
Peripheral neuropathy (PN) is a disease or injury that leads to peripheral nerve dysfunction or damage, and it is frequently related to chemotherapy treatment, with a prevalence from 19% to over 85%. 1 In recent years, cancer treatments have improved survival but also led to many adverse events (AEs) that have worsened the quality of life (QoL) of cancer patients. Chemotherapy drugs aim to arrest cancer progression by eliminating rapidly dividing cancer cells, but their targets and mechanisms of action unfortunately affect normal cells and body structures, causing different side effects, such as anemia, diarrhea, nausea, vomiting, infections, neurological changes, fatigue, hair loss, infertility, pain, and PN. 2 Due to these AEs, sometimes it is necessary to stop the treatment or reduce the drugs dosage, which limits the efficacy of cancer treatment. Chemotherapy-induced peripheral neuropathy (CIPN) is one of the most serious side effects and has also become one of the biggest concerns of chemotherapy treatments.3,4
Different classes of drugs affect the nervous system in various way, depending on their physical and chemical properties and if they are administered in single or cumulative doses. 3 For example, platinum-based drugs could induce CIPN in 70% to 100% of patients, taxanes in 11% to 87% of patients, and thalidomide and its analogues in 20% to 60% of patients. 3 The intensity, duration, and range of the symptoms vary from acute transient thermal sensations to permanent changes in peripheral nerves accompanied by chronic pain and irreversible nerve damage. 4
CIPN manifests as sensory peripheral neuropathy (SPN) and peripheral motor neuropathy. 5 The sensory symptoms generally involve the feet and hands first, presenting as a “glove and stocking” neuropathy with major deficits in the most distal parts of the limbs. The symptoms comprise numbness, tingling, hypoesthesia, altered proprioception, loss of toe and finger dexterity, paresthesias, and dysesthesias. Moreover, painful sensations, including spontaneous burning, shooting, or electric shock–like pain as well as mechanical or thermal allodynia or hyperalgesia, frequently occur.5-8 In severe cases, these symptoms can progress to a complete loss of sensory perception. Motor symptoms may present as distal weakness, gait and balance disturbances, and impaired movements. These symptoms strongly interferer with the QoL of patients; for example, these symptoms cause significant problems with everyday activities, such as fastening shirt buttons or opening a bottle, as well as walking or driving.9,10 CIPN has implications for health-related QoL9,11,12 and has different and pervasive psychological consequences. 13 In fact, the presence of chronic pain or distress can significantly increase the risk of depression, 14 so the management of CIPN, even with nonpharmacological approaches, improves QoL and promotes mental health for patients.14-19 In our study, we enrolled patients who received taxane-based chemotherapy regimens. The prevalence of CIPN induced by taxanes was approximately 84% after just 1 or 2 cycles and up to 97% after completion of therapy, 6 68.1% 1 month after the end of chemotherapy, 60.0% 3 months after, and 30.0% 6 months after. Taxanes-induced CIPN is predominantly an SPN that is rarely accompanied by motor and autonomic changes. 4 The symptoms may start days after the first dose and are dose dependent but tend to improve after stopping the treatment. Unfortunately, there is substantial interindividual variability in the prevalence, severity, and onset during the chemotherapy course; no specific signs of CIPN suggest a dose reduction, and none of the indications warrant a mitigation of the symptoms when they arise. Moreover, pain and sensory abnormalities may persist for months or even years after the cessation of chemotherapy and can sometimes last for the patient’s entire life. 7 Different studies have tried to identify predisposing risk factors of CIPN, such as older age, co-occurrence of neuropathy (eg, diabetic neuropathy), smoking history, impaired renal function, exposure to other neurotoxic chemotherapeutic agents, paraneoplastic antibodies, and cumulative dose of chemotherapeutic agents.20-25 The only certain risk factor is the dose administered, with increases in risk proportional to the cumulative dose. In studies with patients treated for breast cancer, grade 3 or 4 SPN occurred in 20% to 35% of patients receiving 250 mg/m2 of paclitaxel (PTX) every 3 weeks and in 5% to 12% of patients using doses <200 mg/m2 every 3 weeks. 26 Weekly PTX is less myelosuppressive than an every 3-week schedule, 27 but in some reports, a weekly schedule is associated with worse neurotoxicity.28,29 Nab-PTX (nab-PTX) is a nanoparticle albumin-bound form of PTX that was originally formulated to enable lower doses and reduce toxicity, but PN still remains a significant treatment-limiting AE. A phase III randomized trial showed a higher rate of grade 3 sensory neuropathy (10% vs 2%) with nab-PTX 260 mg/m2 every 3 weeks than with standard PTX 175 mg/m2 every 3 weeks. 30 The incidence of SPN may be similar between nab-PTX and docetaxel. In a systematic review of 8 studies, the incidence of taxane-acute pain syndrome with nab-PTX use ranged from 13% to 43% (median 26%), as given in the metastatic disease setting as well as the adjuvant and neoadjuvant settings. 31 The incidence of CIPN with unbound PTX ranged from 0.9% to 86% (median 13%), and that for docetaxel, it ranged from 3.6% to 70% (median 10.5%).30,31
To prevent, treat, or alleviate CIPN symptoms without limiting the potentially life-saving chemotherapy dosage, a number of drugs have been tested, but none of them are currently used. Antidepressants (such as nortriptyline), duloxetine, gabapentin, and a compounded topical gel containing baclofen, amitriptyline, ketamine, lidocaine, tramadol, tapentadol, buprenorphine, and lithium have been tested.32-41 These agents had a record of efficacy for other common neuropathic pain conditions, but CIPN has a different pathologic origin. The America Society of Clinical Oncology does not recommend any agent for the prevention of CIPN. 32 A number of nonpharmacologic interventions, such as acupuncture, limb hypothermia, surgical glove (SG) compression, and electrocutaneous nerve stimulation, have also been investigated. However, the paucity of randomized controlled trial evidence prohibited the inclusion of those studies in this systematic review. Moreover, the studies were often conducted in diabetic populations, with no specific focus on CIPN. 32
Objectives
Considering the enormity of this problem, we tested a constant application of cooling cuffs on the hands and feet to reduce the amount of drugs in the capillaries of the extremities, and to prevent or mitigate CIPN in cancer patients treated with taxane regimens.
Patients and Methods
Study Design
This was a single-center retrospective single-arm study that included patients with breast, gynecological, and pancreatic cancer. The enrolled patients wore cuffs and tubes on their hands and feet with a coolant temperature of 10 °C that worked via the Hilotherm Chemo care device (Hilotherm GmbH, Argenbühl-Eisenharz). The aim of the study was to assess the efficacy and safety of Hilotherapy for the prevention of CIPN and its impact on long-term residual CIPN. The primary endpoint was the overall incidence of grade 2 or higher PTX/nab-PTX–induced SPN in patients who used Hilotherapy, as evaluated by Common Terminology Criteria for Adverse Events (CTCAE) version 4.0. The incidence of PTX/nab-PTX–induced PN in published literature was used as the control group. The secondary endpoints included the incidence of withdrawal from Hilotherapy due to cold intolerance and the impact of CIPN on patient QoL. The ethics committee of the participating institution approved the study protocol (Approval Number 4034, date: April 21, 2020).
Patients
The study population comprised breast, gynecological, and pancreatic cancer patients scheduled to receive neoadjuvant, adjuvant, or palliative taxane-based chemotherapy during the period from April 2019 to November 2019. The inclusion criteria were as follows: age range, 20 to 80 years; and ECOG (Eastern Cooperative Oncology Group) performance status, 0 to 2; the exclusion criteria were as follows: no chemotherapy cycle carried out, disease progression before the start of treatment, and need to change hospital to continue treatment. The patients with other pathologies that may give PN have not been excluded.
Interventions
The patients were treated with different intravenous chemotherapy schedules: weekly PTX (80 mg/m2) for 12 cycles following standard anthracycline-based chemotherapy for breast cancer; 3-week PTX (175-225 mg/m2) plus carboplatin for 6 cycles for gynecological cancer; and weekly nab-PTX (125 mg/m2) plus gemcitabine (on days 1, 8, and 15 of each 28 days) for a maximum of 6 cycles for pancreatic cancer. During every cycle of chemotherapy, premedication drugs (corticosteroids, H1-antagonist/H2-antagonist, and antiemetics) were administered 30 minutes prior to PTX infusion. A total of 80 mg/m2 PTX per week was administered as a 1-hour infusion; 175 to 225 mg/m2 of PTX was administered in 3-hour infusion followed by carboplatin; and 125 mg/m2 nab-PTX was administered over a 30- to 40-minute cycle followed by gemcitabine (infused over 30-40 minutes).
Regional Cooling Method
Regional cooling was performed using a regional hands and feet cooling system, which works with the Hilotherm and forms a closed-loop system with large mittens, that cover the hands up to the wrist, socks, that cover the feet up to the ankles, and tubes, through which a coolant flows at a temperature of 10 °C (Figure 1). The insulators were fitted on both hands and feet for 30 minutes before and 60 minutes after PTX/nab-PTX administration.

The Hilotherm device.
Outcomes
Patient safety, QoL, and tolerance to cooling were measured using 3 validated scales: a Visual Analogue Scale for pain, Subjective Tolerance Scale, and Symptom Questionnaire (EORTC QLQ-C30 [European Organization for Research and Treatment of Cancer Quality of Life Questionnaire]; edition 3.0). The severity of PN was evaluated by a nurse using the CTCAE (Table 4.03, 2017). The patients were assessed before each treatment cycle, and on day 90 after the completion of treatment. It is too early to evaluate the whole sample for CIPN at 6 months.
Statistical Methods
The background information of the patients, such as age, sex, and risk factors, were presented as counts (percentages). The incidence of PN per cycle, according to CTCAE v.4.0, reasons for early Hilotherapy discontinuation, and chemotherapy (PTX) dose changes during Hilotherapy treatment are shown as counts (percentages). Statistical analyses were performed using STATA 13.0 (StataCorp LP).
Results
Sixty-four consecutive cancer patients were enrolled in the study. The patient characteristics and risk factors are reported in Table 1. All patients were women (100%): 42 (65.6%) patients had breast cancer, 20 (31.3%) patients had gynecological cancer, and 2 (3.1%) patients had pancreatic cancer. The median age was 57 years (interquartile range = 19.25): 1 patient had previously received cisplatin-based treatment, and no patients had received taxanes. Of these 64 patients, 54 (84%) patients completed all cycles of cooling with the hands and feet system.
Patients Characteristics (N = 64).

Abbreviation: IQR, interquartile range.
Safety and Tolerability
Continuous cooling was well tolerated by all patients. Premature Hilotherapy termination was necessary in 10 (23.8%) patients treated with PTX because of: excessive coldness, 1 patient (2.4%); grade 2 paronychia of the fingernails and grade 1 CIPN, 2 patients (4.8%); toxicity related to PTX administration, 2 patients (4.8%); dysgeusia and asthenia, 1 patient (2.4%); hospitalization, 3 patients (7.1%); and disease progression, 1 patient (2.4%). In this group, 1 patient refused Hilotherapy. Among the 20 patients treated with the combination of PTX/carboplatin, 5 patients (25%) stopped Hilotherm because of: excessive coldness, 1 patient (5%); PTX infusional reactions, 1 patient (5%); hematological toxicities, 1 patient (5%); and disease progression, 2 patients (10%). Three patients treated with the combination of PTX/carboplatin refused Hilotherapy. All data are shown in Table 2.
Reasons for Early Hilotherapy Discontinuation.
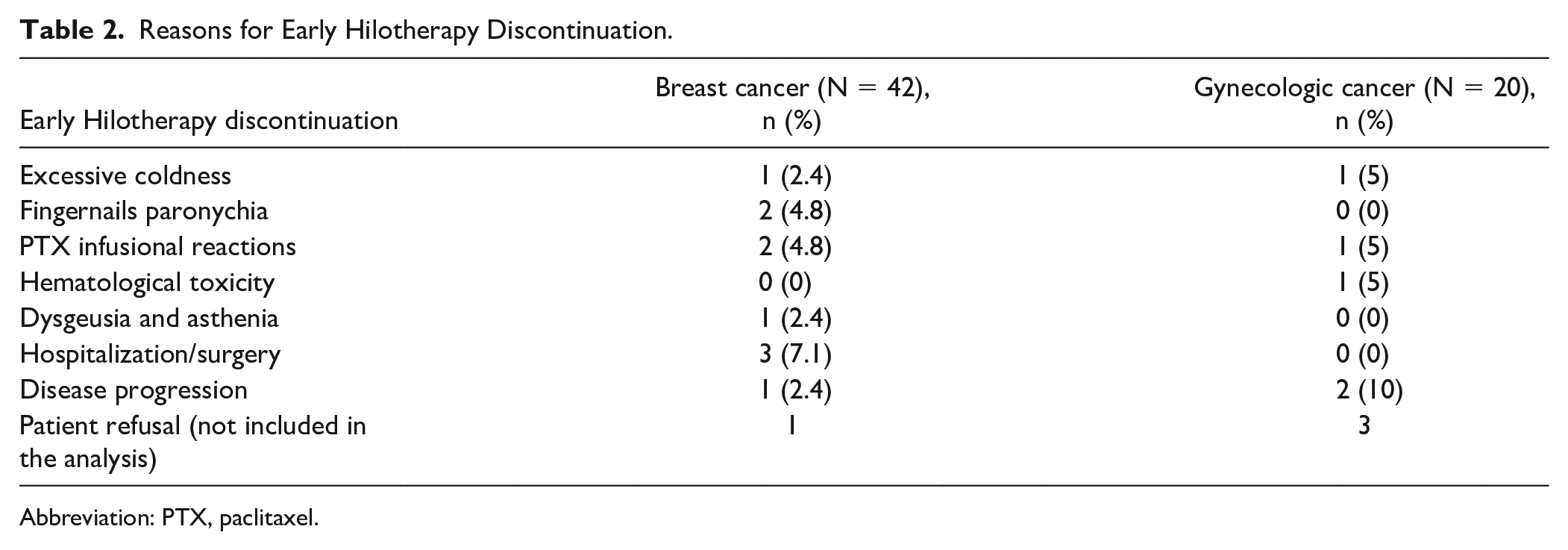
Abbreviation: PTX, paclitaxel.
No patient had grade >2 CIPN. Table 3 reports the incidence of PN evaluated according to CTCAE v. 4.0 at the end of each cooling session for each treatment group. Minimal discomfort was reported at the end of each cooling session. No serious or lasting AEs as a result of Hilotherapy were encountered. In addition, no dermatological AEs related to its use were observed.
Peripheral Neuropathy per Cycle in Each Treatment Groups According to CTCAE v. 4.0.

Abbreviation: CTCAE, Common Terminology Criteria for Adverse Event.
The median time of CIPN onset was 77 days for the entire population: 77 and 89 days in breast and gynecological cancer patients, respectively. During treatment, it was observed that few patients required a PTX dose reduction due to the following reasons: hematological toxicity: 1 (2.4%) patient in the breast cancer group and 3 (15%) patients in the gynecological group; PTX toxicity: 1 (2.4%) patient in the breast cancer group and 2 (10%) patients in the gynecological group; infection: 1 (2.4%) patient with breast cancer; and disease progression: 1 (5%) patient in the gynecological group and 1 (50%) patient with pancreatic cancer (Table 4).
Chemotherapy (Paclitaxel) Dose Changes During Hilotherapy Treatment.

Weekly for 12 cycles.
Three-week carboplatin + paclitaxel for 6 cycles.
Weekly nab-paclitaxel + gemcitabine for 8 cycles.
Discussion
Chemotherapy-induced peripheral neuropathy is a significant problem regarding patient QoL during or after the completion of chemotherapy. With taxane regimes, CIPN occurs very frequently. Tanabe et al 42 identified 219 breast cancer patients who received PTX as adjuvant chemotherapy. CIPN developed in 212 (97%) patients, and the median time to neuropathy onset was 21 days for the entire patient population: 35 days for a weekly administration and 21 days every 3-week administration. CIPN caused PTX treatment to be terminated in 7 patients (4%). The median duration of CIPN was 727 days, and the symptoms persisted in 64% of the patients for 1 year after the start of PTX; 41% manifested symptoms after 3 years. 42
According to the guidelines of the American Society of Clinical Oncology 2014, 32 no established prophylactic therapies for CIPN are suggested except for duloxetine, but this drug has limited efficacy in the reduction of chemotherapy-induced neuropathic pain and no effect on numbness or functional disability.
Many antidepressants, anticonvulsants, topical gels, and other substances did not show any benefit in prevention and treatment of CIPN, so an increased interest arose over complementary approaches that could control the symptoms in a mechanical way. One positive study recently reported the use of ganglioside-monosialic acid. This ganglioside, which previously showed an ability to reduce in the severity of oxaliplatin-induced neurotoxicity in patients with gastrointestinal cancers, 43 was also tested in patients with breast cancer treated with PTX. Compared with those who used placebo, patients who used of ganglioside-monosialic acid showed a lower incidence of peripheral neurotoxicity grade 1 or higher in the CTCAE v4.0 scale (14.3% vs 100.0%, P < .001) both as sensory neuropathy (26, 4% vs 97.8%, P < .001) and as a motor neuropathy (20.9% vs 81.5%, P < .001). 44
Regarding the use of the mechanical system to prevent the onset of CIPN, a phase IIA single-arm clinical trial tested the use of weekly acupuncture in breast cancer patients who developed CIPN >grade 2 after receiving neoadjuvant/adjuvant weekly PTX. Acupuncture was associated with low rates of grade 3 CIPN and the stabilization of CIPN symptoms. 45
Clinical studies46-51 have reported the effect of transcutaneous electrical nerve stimulation (Scrambler therapy) on relieving symptoms related to CIPN. The results showed significant reduction in CIPN symptoms (53% reduction in pain, 44% reduction in tingling, and a 37% reduction in numbness 47 ) and a long-term effect that was maintained at each follow-up at 5 weeks, 47 10 weeks, 48 and 3 months. 50 Recently, a study is still recruiting breast cancer patients with CIPN after chemotherapy who are randomized to receive, in addition to duloxetine or pregabalin, low-frequency electrostimulation generated by a wristband or a “placebo” bracelet. 52
Tsuyuki et al investigated, in a phase 2 study, the efficacy of using SG compression therapy for nab-PTX–induced PN. 53 SG compression reduced microvascular flow to the fingertips and it significantly reduced the overall incidence of grade 2 or higher nab-PTX–induced CIPN. The patients wore a SG one size smaller than the size that fit their dominant hand, for only 90 minutes; the other hand was used as a control. The incidence of grade 2 or higher CIPN was lowered from 76.1% to 21.4% compared with the control hand. With that result, Tsuyuki et al performed another prospective single-arm study 54 with early primary breast cancer patients, but this time, patients wore SGs on both hands. The study showed that the overall incidence of grade 2 or higher sensory CIPN, according to CTCAE, with SG compression therapy was low at 13.8%, and the rate was significantly lower than that of the control group in the prior study (44.1%), with a complete absence of grade 3 CIPN over time. 54
Another way to reduce microvascular perfusion is using cold temperature, which is called “therapeutic regional hypothermia” or “cryotherapy.”55,56 Various limb cooling modalities have been used, most of which involve the direct application of ice or frozen gloves and cause rapid cooling gradients with varied and often poor tolerability. 57 Large cooling gradients permit only intermittent coolant application and are limited by significant intolerance and sometimes frostbite.58,59 The use of frozen gloves and socks was shown to prevent docetaxel-induced nail and skin toxicity; the control arm was the nonprotected side.60,61 The discomfort due to cold intolerance made 11% of patients drop out of Scotte et al’s study. 60 In a retrospective study, the incidence of docetaxel-induced PN was lower in the patients who used frozen gloves and socks than in patients who did not wear them (35% vs 57%). 61
Breast cancer patients treated with weekly PTX tested the use of frozen flexible gloves and socks. The patients wore gloves and socks on the dominant hand and foot starting 15 minutes before to 15 minutes after the PTX infusion (90 minutes in total), and the nondominant side acted as a control. The frozen gloves were replaced after the first 45 minutes. The incidence of CIPN signs was clinically and significantly lower on the intervention side than on the control side (hand tactile sensitivity 27.8% vs 80.6%, foot tactile sensitivity 25.0% vs 63.9%). 62 A small study, in the same setting of patients, randomized 29 women to wear cooled gloves/socks on either dominant or non-dominant hand/foot. In this study, the dropout rate was high, due to cryotherapy discomfort, in fact only 7 participants (4%) completed the treatment and the postchemotherapy sensory tests. 63 Similarly, the use of cryotherapy by cooling the patients’ hands and feet with crushed ice during PTX administration was investigated. Cryotherapy was well tolerated, but the CIPN sensory scores over 12 weeks of PTX were not found to differ between the study arms (mean difference 3.45, 95% confidence interval = −3.13 to 10.02, P = 0.26). However, the control arm of the current trial experienced less neuropathy than the placebo arms of previous similar trials. 64 Even a study that compared cryotherapy, using a frozen glove, and compression therapy, using a SG, to prevent nab-PTX–induced PN, did not find a difference of outcomes with either the systems used. 65 Instead, the study by Rosenbaek et al 66 demonstrated that the prophylactic use of cryotherapy for PTX treatment to treat early-stage breast cancer in the adjuvant setting had the potential to reduce the risk of a dose-limiting toxicity due to CIPN and increase the proportion of patients who can receive the planned chemotherapy dose (77% of patients).
Compression therapy and cryotherapy share an analogous mechanism of reduced drug exposure due to vasoconstriction during PTX infusion. The low temperature associated with cryotherapy may also reduce the uptake of PTX, damage to neurons, or mechanic transductions, which might be related to reduced CIPN symptom. 60 However, the limits of frozen glove use are the preparation of frozen gloves, which is time consuming and costly (the frozen gloves need to be dried overnight or longer in a special freezer), the cold intolerance, and the cold-related injuries.
A small study investigated the neuroprotective effect of continuous-flow limb hypothermia, at a coolant temperature of 22 °C, in 20 breast cancer patients who received weekly PTX and showed that the CIPN was grade 3 in 2 patients (10%), grade 2 in 2 patients (10%), grade 1 in 12 patients (60%), and grade 0 in 4 patients (20%). 67
All the results are presented in Table 5.
Nonpharmacologic Interventions for CIPN Prevention/Treatment.
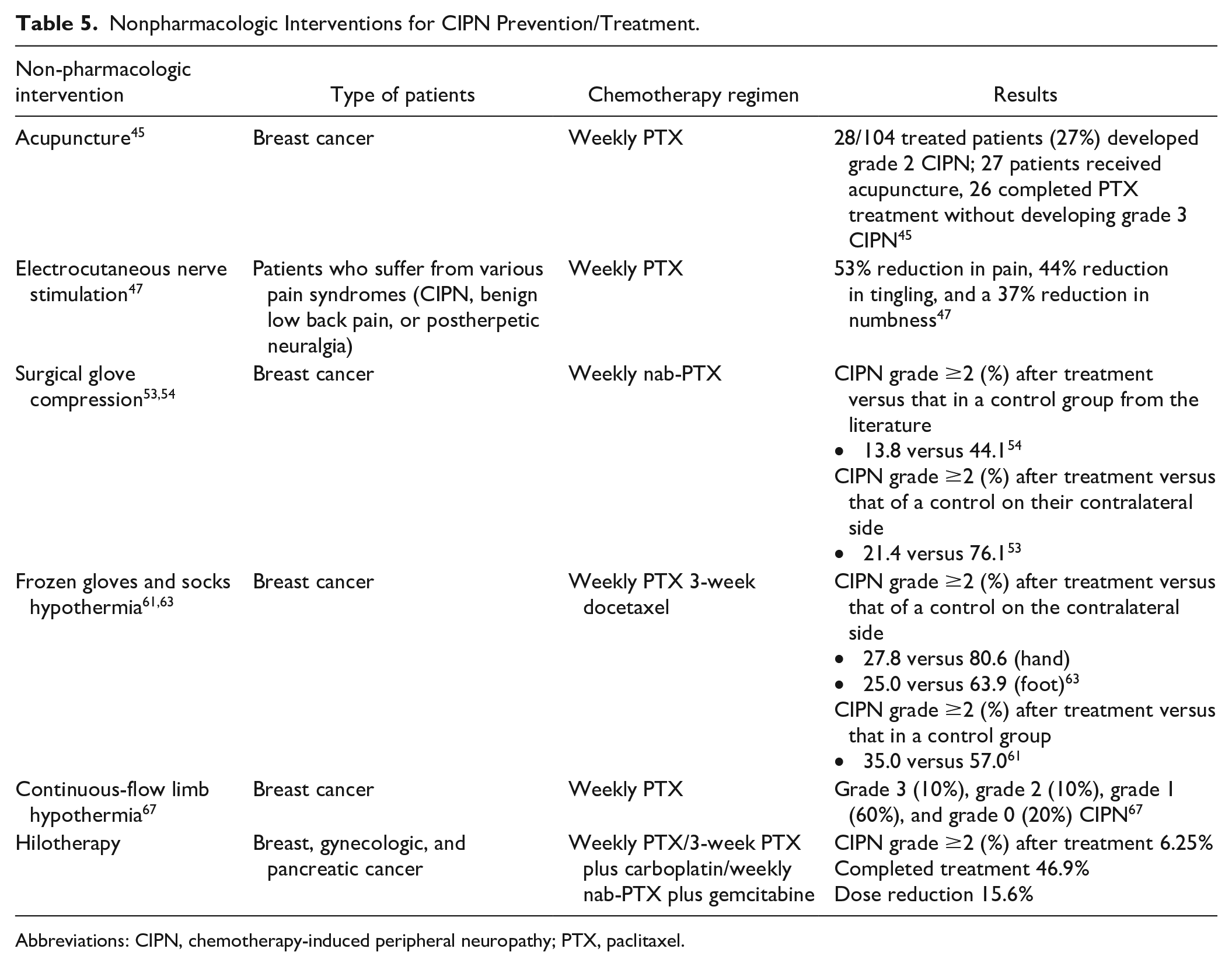
Abbreviations: CIPN, chemotherapy-induced peripheral neuropathy; PTX, paclitaxel.
In our study, we investigated the effects of cooling the hands and feet for the prevention and symptomatic relief of CIPN. Our study shows that continuous cooling using a coolant temperature of 10 °C that lasted the duration of chemotherapy is well tolerated and safe. Our results show good tolerability (Table 3) and, importantly, few early terminations of the cooling protocol (Table 2). In contrast to those of ice or frozen gloves, the advantages of continuous cooling are the controlled manner and more tolerable temperature reduction for the duration of chemotherapy infusion with better outcomes. There is not a placebo effect (related to the use of the control side hand and foot as a comparator) that could make difference in the expected results. The patient-reported outcomes are all standard, reproducible, and valid. Moreover, the development of additional CIPN signs could be revealed only with a long-term follow-up so we followed the patients in order to show the effects of Hilotherapy on preventing late CIPN signs and symptoms. The study limitations are single-arm trial without a direct comparator, a comparison between patients with and without intervention could check the difference in CIPN incidence and physiological response to treatment; patients come from a single center, it would be interesting to check whether the same incidence of CIPN is also reported in other centers to check the accuracy of the cooling procedure, for this reason, we believe that the data from the German centre 68 will be very useful for a future comparison. We used a group of patients not homogeneous for pathology and treatment to widen the sample, an extension of the study could favor a better analysis of subgroup by pathology, stage, and treatment; obviously the number of analyzed patients to date represents a limit, which we hope to overcome with an extension of the enrolment. Moreover, the premature termination of Hilotherm before the end of the treatment, although it occurred in a few cases, cannot be neglected; it is necessary to analyze what the individual factors or related chemotherapy factors predisposing to a failure of the method may be. The development of additional CIPN signs is rare after cessation of chemotherapy, but a long-term follow-up would reveal the effects of the treatment on the natural course of CIPN signs and symptoms. The strength of this study is that it used patient-reported toxicity outcome measures and the data reflect a real-world setting of an unselected patient group.
Conclusions
Chemotherapy-induced peripheral neuropathy is a serious consequence of chemotherapy, particularly impairing the QoL of cancer patients. Strategies to prevent CIPN are urgently needed. The regional cooling of hands and feet might have good effectiveness and tolerability, and seems to be able to prevent and reduce the symptoms of CIPN. Other German hospitals are experimenting with this device and have found comparable results. 68 We are still recruiting patients to obtain more data and to collect data at the second follow-up point (T2) 3 months after the end of chemotherapy, with considerations of the low number of evaluable patients 6 months after the end of chemotherapy. Furthermore, we will enrich our results with a deeper overview of the impact of CIPN on patients’ daily lives and on their perceptions and expectations. In conclusion, albeit limited by the low number of patients enrolled so far, we think that Hilotherm device warrants further attention and validation in CIPN prevention.
Footnotes
Author Contributions
Ester Oneda: the author has dealt with the interpretation of data and in the drafting of the article.
Fausto Meriggi: the author has dealt with the interpretation of data and in the revision of the article.
Laura Zanotti: the author has dealt with the analysis of data.
Elisabetta Zaina: the author has dealt with the acquisition and the interpretation of data.
Sara Bighè: the author has dealt with the acquisition of data.
Federica Andreis: the author has dealt with the acquisition of data.
Sabogal Rueda: the author has dealt with the acquisition of data.
Alberto Zaniboni: the author has dealt with the conception and the design of the study, with the revision of the article and with the approval of the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This retrospective chart review study involving human participants was in accordance with the Ethical Standards of the Institutional and National Research Committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The ethics committee of the participating institution approved the study protocol (Approval Number 4034, date: April 21, 2020).
Consent to Participate
Informed consent was obtained from all individual participants included in the study.