
Abstract
Introduction
The availability of complementary and integrative medicine approaches is increasing in oncology care settings,1-3 with an emphasis on supporting the health of those affected by cancer. According to the National Center for Complementary and Integrative Health, Tai Chi (TC) and Qi Gong (QG) fall under the category of mind-body complementary health approaches and can be practiced alone or in a group setting. 4 TC and QG are movement-based, mind-body approaches combining movement with meditation and controlled, regulated breathing. Numerous studies have shown promise for these interventions to relieve symptoms caused by cancer and its treatment. 5 There has been increased interest in learning more about the benefits of TC/QG as complementary health approaches in the context of oncology care.
The health benefits of TC/QG have been studied in cancer and noncancer patient populations. In the noncancer setting, TC/QG have been shown to improve quality of life for patients suffering with a variety of health issues such as cardiovascular disease, neuromuscular disease, pulmonary disease, sleep disorders, fibromyalgia, and mental illness.6-10 In the cancer setting, a recent systematic review and meta-analysis of 22 studies of cancer survivors, including 15 randomized controlled trials, found that TC/QG contributed to significant improvements in fatigue, sleep difficulty, depression, and overall quality of life. 11 There is also moderate-level evidence suggesting that TC improves limb function in breast cancer survivors and reduces levels of cortisol and cancer-related fatigue. 12 One study of a TC/QG program (40 minutes, 3 times per week) for prostate cancer patients undergoing radiotherapy revealed improvement in sleep duration; however, the effects were not long-standing. 13 Another study showed that Tai Chi Chih (a manualized form of TC) performed similarly to cognitive behavior therapy for insomnia in breast cancer survivors, with both interventions showing clinically significant improvement. 14 Although there is evidence that TC and QG are effective for relieving stress and anxiety in healthy adults, 15 to our knowledge no published studies have explored the effect of TC and QG on the health of cancer caregivers.
Complementary health approaches are increasingly available at cancer centers as part of integrative oncology programs. 16 At the University of Texas MD Anderson Cancer Center Integrative Medicine Center, the emphasis is on providing evidence-informed integrative oncology care to those affected by cancer. Our clinical model incorporates education and therapies that address physical, mind-body, and social dimensions of health, and is based on the biopsychosocial model of care. 17 Our clinical services include physician consultations, oncology acupuncture, oncology massage, health psychology, nutrition, physical therapy, and music therapy. As part of our clinical center outpatient group programs, TC and QG are available to patients and caregivers at no cost.
Outside of a clinical trial setting, there is limited research exploring the real-world application of TC or QG group classes on self-reported symptoms and quality of life in cancer patients and their caregivers. Real-world data are of increasing importance in generating clinical evidence outside of conventional clinical trials. 18 Recent real-world research involving integrative therapy interventions has explored the effects of these interventions on participant symptoms. 19 Participants are referred or self-select themselves for an intervention and voluntarily complete self-reported assessments as part of their participation. This is in contrast to a conventional trial where participants may be randomized with or without use of control group, and which include a more homogeneous population, and strict fidelity monitoring to control for the quality/consistency of the research-based intervention. As part of our center-based, clinical practice assessment, participants in either or both TC and QG group classes completed measures before and after the classes. Our aim was to examine the real-world effects of group class participation on self-reported symptoms, identify differences between patients and caregivers, and to compare outcomes between TC and QC for group class participants.
Methods
Participants (patients and caregivers) included individuals attending either a TC or QG group class between October 2017 and April 2019. Participants did not need a medical order to register for a class; some may have attended on recommendation from a physician or other health care professional. Participants did not have to be patients or caregivers at our institution to attend a group class; those without medical record numbers had one assigned to them as part of class enrollment. However, the majority were from MD Anderson Cancer Center. The group classes were offered at no cost in an activity space located within the hospital campus. Group class attendance was limited to 20 participants. Although patients could attend multiple classes over time, we only analyzed data for the first class per participant.
Classes were advertised as part of our Integrative Medicine Center newsletter (available in print and online) highlighting outpatient group classes. As part of the standard of care, participants were asked to complete an expectancy scale and Edmonton Symptom Assessment Scale (ESAS) at baseline (pre-class). However, completion of any of the assessments was not a requirement for class participation. Data were collected prospectively and entered into a database as part of an institutional review board (IRB)-approved protocol (MDACC Protocol No. DR11-0149; Registration No. IRB 4 IRB00005015). DR11-0149 includes a waiver of informed consent and waiver of authorization.
Intervention
We provided TC and QG classes as part of our outpatient group programs. The overall goals of the TC and QG classes were to improve strength, balance, flexibility, and activity tolerance, as well as relieve stress and enhance relaxation. Both class types were scheduled for 60 minutes, which included 45 minutes of practice. The classes were led by 1 of 2 certified TC and QG instructors. In all classes, there was an introduction to TC or QG as a mind-body practice within our integrative medicine approach at MD Anderson, followed by the respective content. Although both TC and QG have a high safety profile, instructors were available to supervise those with serious balance problems and/or risk of falling.
The TC form taught at MD Anderson consists of a series of 24 postures that flow together into a form or a “dance” allowing the practitioner to move between the postures fluidly with an attention to mind and synchronized breathing (Supplement A, available online). These 24 postures may also be viewed as individual stances that may be practiced one at a time. The form takes approximately 6 minutes to perform and was originally developed in 1956 by the Chinese Sports Committee to promote health and wellness. This TC form, although short, gives the practitioner an introduction to the essential elements of TC.
The QG class content consists of an exercise called the Eight Pieces of Brocade (Supplement B, available online). It includes 8 separate postures that are performed individually with a focused mind and rhythmic breathing for a specific number of repetitions (3 to 8) based on the health and ability of the person practicing the postures. This ancient form of QG was developed in China to promote health and longevity through breath and movement.
Measures
Participants (patients and caregivers) completed the same measures before and after each group class. An expectancy scale was completed at baseline (before class) asking their expectation of the class to improve 5 health domains: well-being, focus, mood, energy level, and physical fitness (unknown, strongly disagree, disagree, agree, and strongly agree). After class, they were asked a question about how the class met expectations (strongly disagree, disagree, neutral, agree, and strongly agree).
Participants also completed the ESAS (scale 0-10, 10 most severe) on paper before and after their class. The ESAS asks about 10 symptoms: pain, fatigue, nausea, depression, anxiety, drowsiness, appetite, sense of well-being, shortness of breath, and sleep. 20 The ESAS Global Distress Score (GDS) is the sum of all the items excluding sleep (total score 0-90). The Physical Distress Score (PHS) is the sum of pain, fatigue, nausea, drowsiness, appetite, and shortness of breath scores (total 0-60). The Psychological Distress Score (PSS) is the sum of depression and anxiety scores (total 0-20). Clinically significant reduction for individual ESAS symptoms was defined as a symptom score reduction of ≥1; for the ESAS subscales, reduction of GDS ≥3, PHS ≥2, and PSS ≥2 indicated clinically significant changes. 21
Statistics
As an individual could attend more than one group class, we only analyzed data for the first class per participant. Data were summarized using standard descriptive statistics such as mean, standard deviation, median, and range for continuous variables and frequency and proportion for categorical variables. Associations between categorical variables were examined by the χ2 test or Fisher’s exact test when appropriate. Since the continuous variables collected in this study were not normally distributed, the Wilcoxon rank-sum test was used to examine differences in the continuous variables between TC and QG group classes; and the Wilcoxon signed-rank test was used to examine changes (pre- and post-class) in the continuous variables within each group class. All computations were carried out in SAS 9.4 (SAS Institute Inc).
Results
The analysis included 304 participants (October 2017 to April 2019; 184 patients, 120 caregivers; 72% women; 60% white; mean age = 58 years). Race was the only significantly different demographic characteristic between caregivers and patients (P = .02; Table 1).
Patients’ and Caregivers’ Demographic and Medical Characteristics.
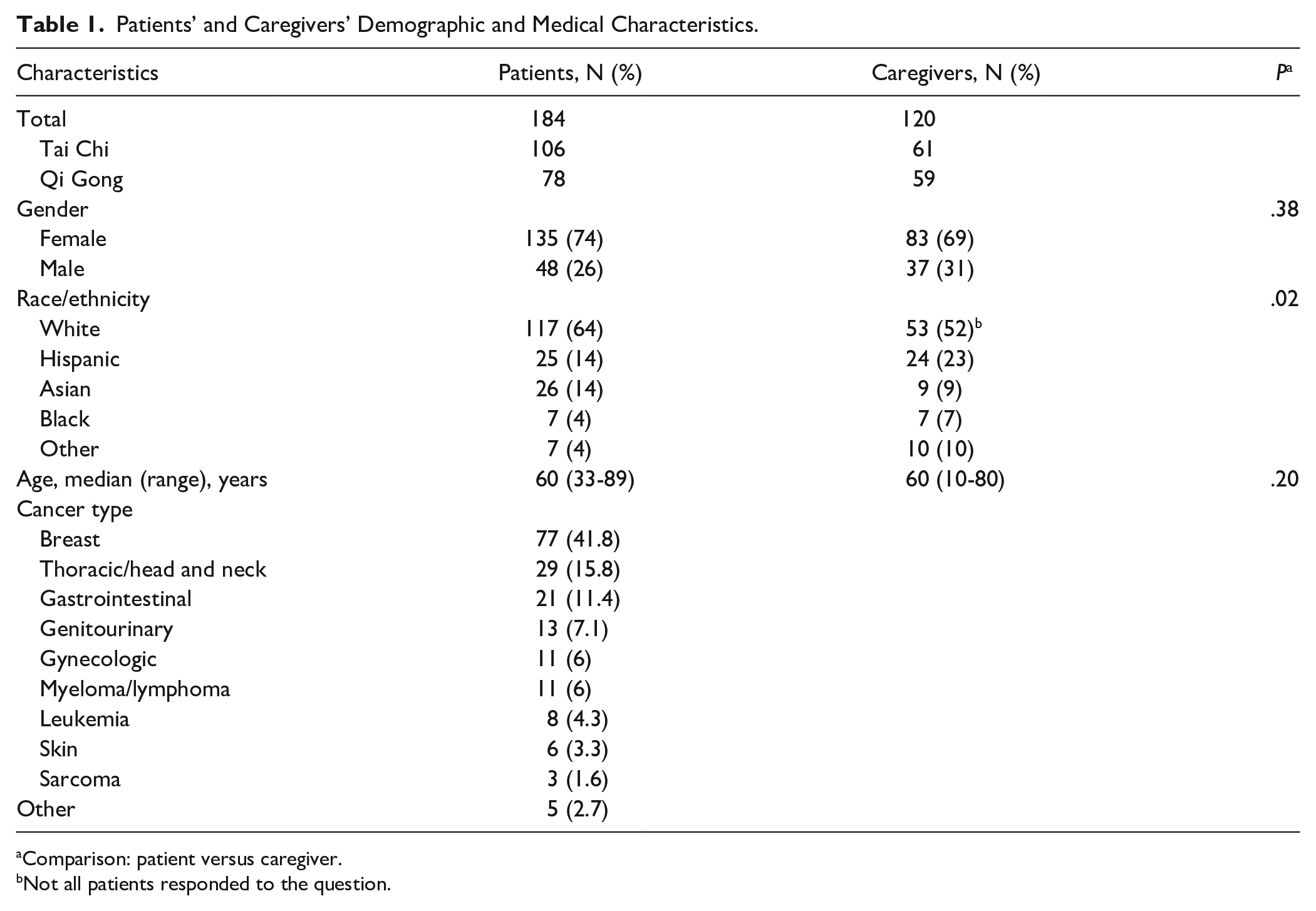
Comparison: patient versus caregiver.
Not all patients responded to the question.
Baseline Expectations and Self-Reported Symptoms: Caregivers Versus Patients
Baseline expectancy for change in energy level as a result of group class participation was significantly different between caregivers and patients (P = .016); this difference was driven by a high percentage of caregivers reporting strong agreement with this expectation (“Strongly Agree”: 22.9% of caregivers vs 9.9% of patients; P = .002).
Although the overall symptom burden was low (ESAS scores <4), the highest (worst) symptom scores for patients and caregivers were those for sleep, fatigue, and well-being (Table 2). No significant differences were observed between patients and caregivers in baseline ESAS PSS scores (mean: patients = 3.1 vs caregivers = 2.5, P = .072); however, patients had significantly worse scores for PHS (patients = 10.3 vs caregivers = 6.5, P = .0001) and GDS (patients = 16.1 vs caregivers = 1.2, P = .0002).
Baseline Mean ESAS Score of Patients Participating in Tai Chi and Qi Gong.

Abbreviations: ESAS, Edmonton Symptom Assessment System; SD, standard deviation; PHS, Physical Distress Score; PSS, Psychological Distress Score; GDS, GLOBAL DISTRESS SCORE.
For all symptoms, a score change of ≥1 is considered clinically significant. For predetermined subscales, clinical significance is defined as score changes ≥3 for GDS and ≥2 for PHS and PSS.
Indicates P value for differences between Tai Chi and Qi Gong.
PHS equals the sum of pain, fatigue, nausea, drowsiness, appetite, and shortness of breath scores (total 0-60); PSS equals the sum of depression and anxiety scores (total 0-20); and GDS equals the sum of pain, fatigue, nausea, depression, anxiety, drowsiness, appetite, sense of well-being, and shortness of breath scores (total 0-90).
Baseline Expectations and Self-Reported Symptoms: Tai Chi Versus Qi Gong
For caregivers, there was higher expectancy at baseline that TC would contribute to improved focus (P = .017) and energy level (P = .047). For patients, there were no significant differences in baseline expectancy between the TC and QG groups. There were no significant differences in baseline self-reported health or quality of life or ESAS individual symptom scores or subscales for caregivers participating in TC versus QG classes (Table 2). There were also no significant differences in baseline self-reported health or quality of life for patients participating in TC versus QG. However, patients participating in QG had significantly worse baseline scores for drowsiness (P = .003), fatigue (P = .001), PHS (P = .001), and GDS (P = .004) than those participating in TC (Table 2).
Group Class Effects on Self-Reported Symptoms
For patients, we observed (1) clinically significant improvement in fatigue symptom scores for those participating in QG (mean change = 1.44) and (2) clinically significant improvement in anxiety (mean change = 1.00) and well-being (mean change = 1.03) scores for those participating in TC (mean change = 1.03; Table 3). The difference change in patient well-being score between those participating in TC versus QG was also statistically significant (P = .030). In addition, mean score reductions for the ESAS PHS and GDS subscales were clinically significant for both the TC and QG groups (Table 3). Caregivers who participated in QG had clinically significant improvement in fatigue (mean change = 1.00) and well-being (mean change = 1.22) scores. For the symptom of well-being, there was also a statistically significant difference in mean symptom score reduction between class types, favoring QG (mean change = 1.22) over TC (mean change = 0.18; P = .046; Table 3). We also observed clinically significant improvement in GDS for caregivers who participated in TC (mean change = 3.73) or QG (mean change = 4.02).
Comparison Analysis of Effects of Tai Chi and Qi Gong Among Patients and Caregivers.
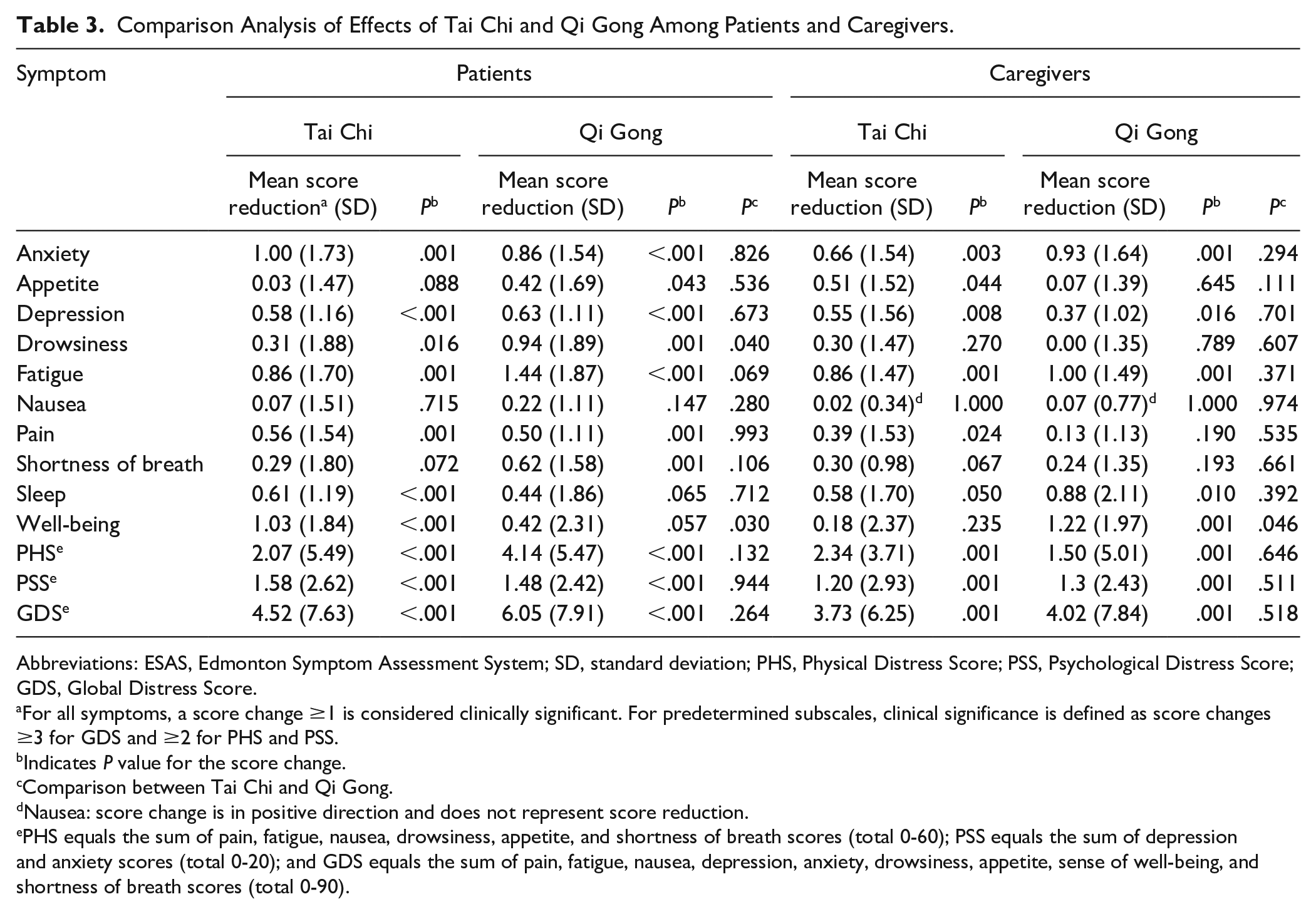
Abbreviations: ESAS, Edmonton Symptom Assessment System; SD, standard deviation; PHS, Physical Distress Score; PSS, Psychological Distress Score; GDS, Global Distress Score.
For all symptoms, a score change ≥1 is considered clinically significant. For predetermined subscales, clinical significance is defined as score changes ≥3 for GDS and ≥2 for PHS and PSS.
Indicates P value for the score change.
Comparison between Tai Chi and Qi Gong.
Nausea: score change is in positive direction and does not represent score reduction.
PHS equals the sum of pain, fatigue, nausea, drowsiness, appetite, and shortness of breath scores (total 0-60); PSS equals the sum of depression and anxiety scores (total 0-20); and GDS equals the sum of pain, fatigue, nausea, depression, anxiety, drowsiness, appetite, sense of well-being, and shortness of breath scores (total 0-90).
Overall, there were statistically significant reductions (improvements) in self-reported symptom scores for anxiety, depression, and fatigue for caregivers and patients participating in either TC or QG (Table 3). Patients and caregivers participating in TC experienced clinically and statistically significant improvement in ESAS PHS scores (decrease ≥2; both P ≤ .001). We observed clinically and statistically significant improvement in ESAS GDS scores (decrease ≥3; both P ≤ .0001) for patients and caregivers participating in TC or QG (Table 3).
For the after-class expectancy measure (“Class Met Expectations”), 90% of all participants (patients and caregivers) reported “Agree” or “Strongly Agree,” and no difference was seen between those participating in TC versus QG (P = .6680).
Subgroup Analysis, Moderate to Severe Symptom Burden: Patients Only
We examined patients reporting moderate to severe symptom burden (individual score ≥4) at baseline and observed clinically significant benefits in both TC and QG participants for symptoms of anxiety, depression, drowsiness, fatigue, pain, shortness of breath, and well-being. These analyses were not conducted for the caregivers as the number of caregivers experiencing symptoms of ≥4 was too small. The greatest mean score reductions were observed for anxiety (TC mean change = 2.9, QG mean change = 2.8) and shortness of breath (TC mean change = 2.8, QG mean change = 2.3), with no statistically significant difference in symptom score reduction between TC and QG participants. For patients reporting at least one individual ESAS symptom with a moderate to severe score (≥4) as part of the sum of their ESAS subscale score (PHS, PSS, or GDS), we observed clinically significant improvement in ESAS PHS scores for TC and QG participants, with significant differences between QG and TC (QG mean change = 5.19, TC mean change = 2.68; P = .043). For the GDS and PSS ESAS subscales, both TC and QG contributed to clinically significant improvement, with no significant differences between TC and QG.
Discussion
Our real-world, clinic-based study supports prior reports from randomized controlled trials. We found that both patients and caregivers participating in TC/QG experienced significant improvement across several individual self-reported symptoms and physical, psychological, and global distress subscales. Among our group class participants, baseline physical symptom burden and global distress were highest in patients, but there were no significant differences between patients and caregivers in baseline anxiety and depression. These findings are consistent with our prior studies analyzing symptom burden using pre- and post-ESAS assessments in patients and caregivers participating in group classes.22,23 Even though patients and caregivers may start the TC/QG class with different symptom presentations, they benefit from class participation in similar ways. Overall, our results suggest that a 60-minute, low- to moderate-intensity group class of a mind-body movement practice such as TC/QG can positively affect cancer patients and caregivers in various physical and mental health domains. Our results support the value of making TC/QG classes available for patients and caregivers.
We observed a higher overall symptom burden at baseline in patients participating in QG versus TC group classes. This may be explained in part by 2 factors: (1) the group class description used to advertise the classes lists QG as low intensity and TC as moderate intensity and (2) our clinical providers more often recommend that patients with more limited physical function participate in QG rather than TC classes because QG’s lower intensity.
We observed differences in symptom change according to participant type (patient vs caregiver) and class type (TC vs QG). Our findings are consistent with prior systematic reviews suggesting differences in symptom change based on class type.5,11,12 For example, one systematic review reported evidence that both TC and QG contributed to improvements in fatigue, mental health, and quality of life, with TC but not QG contributing to improvement in anxiety. 24 We found that for both patients and caregivers, only QG contributed to clinically significant improvement in fatigue (≥1 point change); however, there were no statistically significant differences between QG and TC. It is important to note that the choice of which class to attend (TC or QG) was by self-selection, resulting in differences in certain baseline variables between groups for patients including drowsiness, fatigue, PHS, and GDS. Examination of change scores from baseline should help to account for these differences, but conducting the analyses examining postclass levels controlling for baseline (regressor variable approach) might provide additional useful information. However, to be consistent with some of our other studies,22,23 and for ease of comparison and interpretation, we used the change score approach. Although future research could randomize patients to the different classes, the purpose here was to assess the outcomes in a real-world clinical setting.
In the subgroup of patients with moderate to severe symptom burden at baseline, QG contributed to greater self-reported physical health improvement than did TC. Greater insight into differences in symptom change according to participant type and class type can help with the development of personalized clinical recommendations. For example, after a baseline symptom assessment, mind-body approaches such as TC or QG could be recommended to patients based on the symptom profile. Our findings will lend insight into the design of a future randomized controlled trial exploring which symptom profiles or clusters could benefit most from TC, QG, or other mind-body approaches.
This study has several limitations. First, it was conducted at a single institution. As part of a real-world clinical application, there was no control group and participants were self-selected rather than randomly assigned to TC or QG classes. Also, patients and caregivers reported relatively low-symptom burdens before class; therefore, it is not clear if the effects would be more clinically significant for patients with a higher symptom burden. Also of note, we did not measure the dyad effect of patients and caregivers attending the classes together. In addition, the findings were limited to the changes associated with one class, and presumably the effects would accumulate with repeated exposure. For the current analysis, it is noteworthy that even with one exposure, participants noted clinically significant reductions in their symptoms. For future research, we will consider exploration of the long term effects of ongoing class participation on participants’ self-reported symptoms. In addition, we did not account for patients and caregivers who may have attended multiple TC or QG group classes or had a regular mind-body practice prior to or during the study period. Therefore, it is difficult to determine if our results were solely related to a single 60-minute intervention. However, we did examine the outcomes from the first class a patient or caregiver may have attended. A future study should examine whether there is an interaction effect between the number of classes attended and outcomes over time.
Although efforts were made to calibrate the intensity and maintain the consistency of class content through an outlined curriculum, fidelity monitoring was not as strict as might be expected in a research-based intervention (eg, use of video monitoring). Future studies could examine a more homogeneous participant population (eg, patients with a single cancer type and stage) and one with greater symptom burden (eg, advanced cancer patients) to learn more about the effect of class content on symptom change. Of note, when we analyzed a subgroup of our patients with moderate to severe symptom burden at baseline, both TC and QG contributed to improvements in physical and psychosocial symptoms. Overall, the generalizability of these findings is good because the data were collected as part of routine clinical care.
Conclusion
We consider TC/QG an important part of our integrative oncology group program at MD Anderson. The classes contribute to the biopsychosocial approach to cancer care, and our results show clinically significant positive short-term outcomes. Our study findings build on the literature demonstrating the importance of mind-body interventions for whole-person, patient-centered cancer care. Additional research is warranted to learn more about how differences in class content, length, frequency, and participant type (ie, patient vs caregiver, cancer type, and cancer stage) may contribute to personalized recommendations for the optimization of symptom management.
Supplemental Material
Supplement_A_Tai_chi_Curriculum_1 – Supplemental material for Effects of Center-Based Delivery of Tai Chi and Qi Gong Group Classes on Self-Reported Symptoms in Cancer Patients and Caregivers
Supplemental material, Supplement_A_Tai_chi_Curriculum_1 for Effects of Center-Based Delivery of Tai Chi and Qi Gong Group Classes on Self-Reported Symptoms in Cancer Patients and Caregivers by Gabriel Lopez, Santhosshi Narayanan, Aimee Christie, Catherine Powers-James, Wenli Liu, M Kay Garcia, Telma Gomez, Jimin Wu, Aditi Chunduru, Janet L. Williams, Yisheng Li, Eduardo Bruera and Lorenzo Cohen in Integrative Cancer Therapies
Supplemental Material
Supplement_B_Qi_gong_Curriculum_1 – Supplemental material for Effects of Center-Based Delivery of Tai Chi and Qi Gong Group Classes on Self-Reported Symptoms in Cancer Patients and Caregivers
Supplemental material, Supplement_B_Qi_gong_Curriculum_1 for Effects of Center-Based Delivery of Tai Chi and Qi Gong Group Classes on Self-Reported Symptoms in Cancer Patients and Caregivers by Gabriel Lopez, Santhosshi Narayanan, Aimee Christie, Catherine Powers-James, Wenli Liu, M Kay Garcia, Telma Gomez, Jimin Wu, Aditi Chunduru, Janet L. Williams, Yisheng Li, Eduardo Bruera and Lorenzo Cohen in Integrative Cancer Therapies
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.