
Abstract
Objective:
To assess the feasibility, safety, and preliminary effect of a 12-week multi-modal rehabilitation program targeted at improving health-related quality of life and physical activity levels of patients with lung cancer following treatment.
Methods:
Patients with stage I to IIIA non-small cell lung cancer were included 6 to 12 weeks following completion of treatment. The intervention comprised of aerobic exercise (brisk walking), resistance training and 8-style Tai Chi. The 12-week program included 2 supervised center-based sessions per week of 90 minutes duration and home-based exercise. The primary outcomes were the feasibility and safety of the intervention. Secondary outcomes (assessed pre and post program) were physical and patient-reported outcomes.
Results:
Seventy-eight patients were approached during the 6-month recruitment period and 17 (22%) consented to the study. Eight participants (47%) met the definition of adherence to the program (attending at least 70% of supervised sessions). No serious adverse events occurred. A significant reduction in anxiety and depression was observed post-program. In addition, improvements in respiratory function, sleep quality, and some health-related quality of life domains were observed post-program. There were no significant differences in functional capacity or physical activity levels.
Conclusion:
This multi-modal exercise training program was safe, although the feasibility of the program in its current state is not supported given the low consent rate and low adherence to the intervention.
Introduction
Lung cancer is the most commonly diagnosed type of cancer in China and the leading cause of cancer-related death.1,2 In 2015, there were an estimated 733 000 new lung cancer cases (17% of total cancer incidence) and 610 000 deaths (21.7% of total cancer mortality) in China and the age-standardized lung cancer incidence and mortality rates in China have been steadily increasing since 1990.1,3
Exercise is beneficial for patients after surgery yet poor uptake and adherence to exercise interventions may limit their efficacy. The majority of patients with lung cancer do not meet the exercise guidelines which recommend moderate-intensity aerobic exercise of at least 150 minutes per week and resistance-training at least twice per week.4,5 Studies also report an inverse association between exercise after a cancer diagnosis and mortality. 6
Exercise in the context of cancer is extremely topical in China at present. In 2016, the Chinese government approved the Healthy China 2030 plan, 7 emphasizing the strategic role of health in China’s development. Systematic reviews have demonstrated the benefit of aerobic exercise and resistance training (similar to traditional pulmonary rehabilitation) after lung cancer. 8 This type of exercise training undertaken by people within 12 months of lung resection for non-small cell lung cancer (NSCLC) improves exercise capacity, including peak rate of oxygen uptake (VO2peak), 6-minute walk test distance (6MWT), and quadriceps muscle strength, as well as demonstrating improvements in the physical component of health-related quality of life (HRQoL) and dyspnea. As these pulmonary rehabilitation type exercise programs are not readily accessible to all patients after lung cancer surgery in China (or elsewhere globally), research is required to determine feasible models of care to promote patient uptake and adherence to exercise in order to achieve the aims of the Healthy China plan.
Tai Chi is a traditional Chinese health-promoting exercise which has a supportive broad appeal in China, and it is easy to perform in parks or communities. Evidence has shown that Tai Chi can improve HRQoL, 9 insomnia, 10 fatigue, 11 and physical performance outcomes 12 in cancer survivors. The safety and health benefits of Tai Chi exercise have been documented in a large number of clinical studies focused on specific diseases and health conditions while in cancer populations studies have mainly been conducted in individuals with breast cancer. 13 There is one published trial (and another in progress) demonstrating promising results of the benefit of Tai Chi for patients with lung cancer.11,14 However there is very limited information about the combination of Tai Chi with traditional pulmonary rehabilitation exercise programs after lung cancer surgery. 15
Therefore, the purpose of this study was to investigate whether a multi-modal exercise training program comprised of aerobic exercise, resistance training and 8-style Tai Chi is safe and feasible to integrate into the routine postoperative care of patients 6 to 12 weeks after lung cancer surgery in China. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines 16 were followed in reporting this study.
Methods
Design
This was a single center, prospective, phase I feasibility study conducted at a tertiary hospital in Nantong, China. Recruitment occurred over a 6-month period from November 2018 to April 2019. Ethical approval was obtained from the Ethics Committee of Affiliated Hospital of Nantong University (Number: 2018-K041) and all participants provided written informed consent.
Participants and Procedures
The inclusion and exclusion criteria are outlined in Table 1. A convenience sample of participants was enrolled using 2 recruitment and screening methods: (1) posters were displayed in hospital departments advertising the study for patients or staff to contact researchers; and (2) researchers screened hospital systems for discharge records from thoracic surgery, radiotherapy, and chemotherapy departments to identify eligible patients. Eligible patients were contacted by telephone to be informed about the study and invited to participate. Patients who consented to the study underwent baseline testing prior to commencing the intervention at the hospital out-patient rehabilitation department.
Inclusion and Exclusion Criteria.
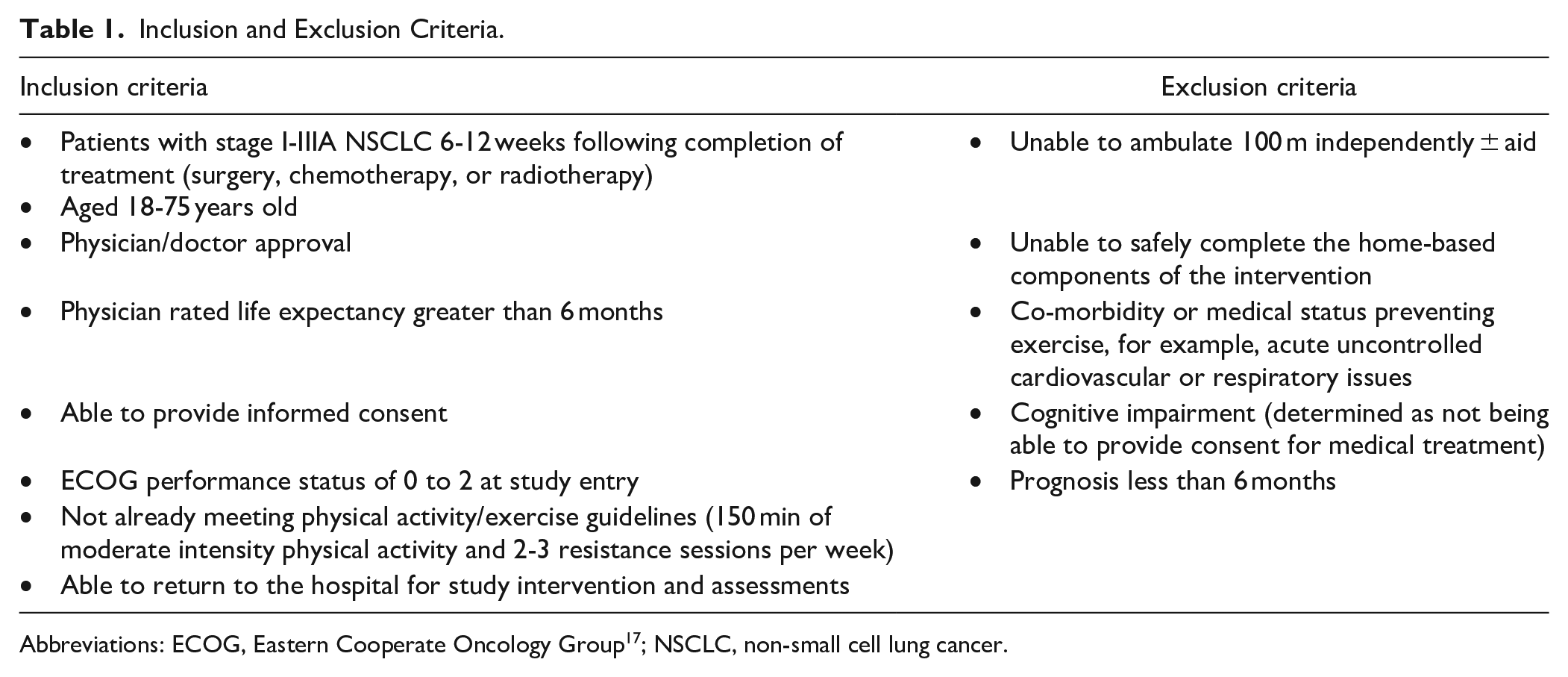
Abbreviations: ECOG, Eastern Cooperate Oncology Group 17 ; NSCLC, non-small cell lung cancer.
Intervention
All participants in the study received a multi-modal training program which involved aerobic and resistance exercises integrated with traditional Chinese movement Tai Chi. The program was conducted at the physical therapy department and was guided by 2 new graduate physiotherapists who were trained in the intervention protocol. The program ran for 12 weeks and participants were encouraged to exercise in the physical therapy department (supervised) twice a week, 90 minutes per session and exercise at home on the other 3 days. The supervised intervention comprised of 3 parts, and participants were also given a home program:
Resistance training: six different exercises involving major limb movements were utilized, each exercise included 5 progressions (see Table 2). Exercises were prescribed in 3 sets, each set 8 to 15 repetitions, with intensity targeted to Borg 4/10 (somewhat hard). 18 Exercises were progressed by first increasing repetitions and then increasing weight with reduced repetitions. The intensity of the training was increased with the progression of participants’ physical strength.
Simplified 8-style Tai Chi: designed in consultation with a professional Tai Chi instructor from Nantong Aged University with 48 years of teaching experience and adapted to 8 simple styles from the most popular 24-Yang Style Tai Chi. 13 These 8 styles were selected by the physiotherapists with the intention of improving lower limb strength and upper limb range of motion, as well as to improve general mobility. Natural breathing was integrated into the training routine. The intervention physiotherapists received 3 weeks of training from a professional Tai Chi instructor prior to instructing participants. In the first week, the physiotherapists gave a 10-minute introduction to the participants to let them learn some basic principles to practice, and then 5 warm-up movements were taught. Over the following weeks the physiotherapists emphasized the mastery of single forms through multiple repetitions; later weeks focused on repetitions to enhance balance and lower limb strength (see Table 2).
Aerobic exercise (brisk walking): participants were instructed to walk on the treadmill for 15 minutes, at a pace which was 80% of that recorded during the baseline 6MWT. Duration was progressively increased to 30 minutes by the end of the program. Treadmill speed was increased throughout the program to ensure participants exercised at a moderate-intensity throughout (somewhat hard; Borg 4/10). 18
Resistance Training With Progressions and Tai Chi Exercises.

Home program: Participants were provided with education about exercise at home. They were instructed to walk at home for 20 to 30 minutes on any other 3 days of the week when they were not attending supervised sessions. The education included aspects about (1) the importance of the exercise after lung surgery and the amount of the exercise and intensity prescribed every week; (2) dietary advice according to healthy eating international guidelines 19 ; (3) the management of their symptoms such as cough and pain in their daily life; and (4) how to overcome exercise barriers if the environment at home was not suitable for exercise such as bad weather or a lack of space.
Every week when participants returned to the hospital for the supervised sessions the therapists checked if they had completed the exercises at home and gave them updated instructions for the subsequent week depending on their performance to date.
Outcomes
Demographic and medical data were recorded at baseline. This included age, sex, marital status, education background, cancer treatment, and hospital length of stay following surgery. Participants’ respiratory function was measured by their forced expiratory volume in the first second (FEV1), body weight (kg) was measured and the body mass index (BMI; kg/m2) was calculated. Nutritional assessment was assessed using the Mini Nutritional Assessment.
The primary outcomes of the study were feasibility and safety of delivering the training program. Feasibility was assessed using the attendance rate of supervised exercise sessions and an attendance rate of ≥70% was considered a priori to be adherent. This rate of 70% is based on attendance rates reported in prior exercise training studies in the oncology setting. Safety was assessed by the number of adverse events occurring during or within 60 minutes following the intervention. Serious adverse events were defined as any adverse event related to the study that resulted in death or was life threatening, requiring hospitalization or extended existing length of stay, caused disability or incapacity. Minor adverse events were those that were directly caused by exercise such as: a minor fall, increased symptoms, new or progressive pain, transient neurological deficits, transient altered mental status, palpitations or progressive fatigue.20,21
Secondary outcomes were measured pre and post-program (12 weeks) and included a range of objective measures of physical function and patient-reported questionnaires. Physical function was measured using the 6-minute walk test (6MWT) and Short Physical Performance Battery (SPPB). The 6MWT was conducted according to standard guidelines. 22 Participants performed the test using a 30-m corridor, a cone was placed at the 2 turnaround points at either end of the corridor. During the test participants were monitored using portable pulse oximetry. The test was not commenced if the participants had high blood pressure after 10 minutes of rest (≥140/90 mmHg). The SPPB was used to assess balance, gait, strength, and endurance evaluated by examining ability to stand with the feet together in the side-by-side, semi-tandem, and tandem positions, time to walk 8 feet, and time to rise from a chair and return to the seated position 5 times. 23
Physical activity levels were measured using an electronic pedometer commonly used in China (Mi Band 3, Xiaomi Co., Ltd., China) for a 10-day period. 24 The device provided a record of the number of daily steps and distance walked. Participants were instructed to wear the device for 8 hours a day. The pedometer data were only included in analyses when participants wore the device for a minimum of 4 days of 8 hours. 25 The 2 time points of wearing the devices were within 10 days prior to the start of the exercise program and within 10 days after completion of the 12-week program. Step count was not visible on devices to participants to minimize possible changes in their behavior based on the number of daily steps they were performing.
Mood was measured using the Self-rated Anxiety Scale (SAS) and Self-rating Depression Scale (SDS), which are tools to assess the anxiety and depression levels of participants. Both scales have 20 items and responses are measured on a 4-point scale (rated 1-4).26,27 Higher total scores represent worse status. The distress thermometer was also used.
European Organization for the Research and Treatment of Cancer questionnaire and lung cancer module (EORTC-QLQ-C30 and LC13) was used to measure HRQoL. 28 For functional domains and global health status/quality of life scale, a higher score represents better status, while for symptom domains and single-items, lower scores represent less symptoms.
The M. D. Anderson Symptom Inventory-Tumor (MDASI-T) was used to assess symptoms. This is a questionnaire for measuring the severity and interference with daily life of cancer-related symptoms. The scale has 13 items, reliability of the Chinese version has been verified. Its rating scale is 0 to 10, with higher scores indicating greater symptom severity. 29
The Pittsburgh Sleep Quality Index (PSQI) was used to assess sleep. This is a self-rated questionnaire which assesses sleep quality and disturbances over a 1-month time interval. Nineteen individual items generate 7 component scores. The sum score for these 7 components yields an overall global score, 30 with higher scores indicating worse sleep quality.
Sample Size
As this was a phase I feasibility study there was no a priori set sample size. The program was implemented for a 6-month recruitment period.
Statistical Analysis
All data analyses were performed using SPSS Windows Version 23.0 (SPSS, Chicago, IL, USA). Data were first tested for normality using the Shapiro-Wilk statistic. Mean and standard deviation (SD) are reported for parametric data, while median and inter-quartile range (IQR) are reported for non-parametric data. Descriptive statistics were used to summarize demographic characteristics of the participants and the feasibility and safety outcomes. For analyses of changes in secondary outcomes over time, if the data conformed to the normal distribution, paired sample t-tests were used. For data that did not conform to the normal distribution, the Wilcoxon signed rank test was used. Responsiveness was determined by effect sizes and for non-parametric data as r = Z divided by the square root of sample size. All statistical analyses were exploratory given the feasibility nature of this study. As such, statistical significance was understood to be interpretable as a signal rather than a formal probability.
Results
Demographic Information
Seventy-eight eligible participants were approached for inclusion into the study during the 6-month recruitment period (Figure 1). A total of 17 (22%) of these patients consented to the study. The main reasons patients declined to participate were because of the distance from their homes to the hospital (n = 23/61, 38%) and being too busy with personal affairs (n = 22/61, 34%). Seventeen participants completed baseline assessment and 16 (94%) completed the follow-up questionnaire assessment (see Figure 1). The median (IQR) age of participants was 59 [44-63] years (Table 3). The majority of participants were married, female, and retired and most of them were well-nourished at baseline (Table 3). All participants were managed with surgery only without adjuvant chemotherapy or radiotherapy. Lobectomy was the most common surgery type (23.5%, n = 4). The mean hospital length of stay (LOS) for surgical participants was 14.5 ± 2.7 days, the median time from ceasing treatment to study enrollment was 51 [46-65] days.

Participant flow through the study.
Patient Demographics and Clinical Characteristics.

Abbreviations: BMI, body mass index; MNA, Mini Nutritional Assessment; ECOG PS, Eastern Cooperate Oncology Group-Performance status; FEV1, forced expiratory volume in the first second; IQR, inter-quartile range; kg, kilograms; m, meters; n, number; SD, standard deviation; LOS, length of stay.
Feasibility and Safety of the Intervention
Forty-seven percent of participants (8/17) attended at least 70% of the scheduled supervised exercise sessions. The total attendance rate was 53% (181/340 possible supervised sessions). The median [IQR] number of intervention sessions attended was 9 [0-20] per participant. Five participants (29.4%) did not attend at all after the baseline assessment. In these 5 participants, 2 stated that they were busy with work, 1 was busy taking care of her children and 1 wasn’t satisfied with the training environment (see Table 4). Three participants discontinued the intervention, 2 due to losing interest and 1 for thyroid surgery.
Feasibility and Safety of the Intervention.

Safety was monitored throughout the intervention and outcome assessments. No serious adverse events occurred. There were 3 minor adverse events related to the intervention reported, these included joint pain due to arthritis (n = 1) and knee pain (n = 2). Only 1 participant required modifications to the prescribed program and initial symptoms resolved in all participants.
Secondary Outcomes
Objective measurements
Across the 12 week follow-up period, there was a significant improvement in FEV1 (mean ± SD baseline 1.9 ± 0.5 L vs follow-up 2.1 ± 0.6 L; P = .02) but no significant change in the 6MWT (mean ± SD baseline 514.2 ± 72.3 m vs follow-up 569.9 ± 52.9 m; P = .06). For 7-day activity, there was no significant improvement in average daily step counts (mean ± SD baseline 7565 ± 2054 steps vs follow-up 8814 ± 3200 steps; P = .330) or walking distance (mean ± SD baseline 1.9 ± 0.5 km vs follow-up 2.1 ± 0.6 km; P = .370). There were no differences in SPPB scores between the 2 time points (12.0 [11.5-12.0] vs 12.0 [12.0-12.0], respectively; P = 1.00) (Table 5).
Changes in Secondary Outcomes.

Abbreviations: 6MWT, 6-Minute-Walk Test; SPPB, Short Physical Performance Battery; EORTC QLQ-C30, European Organization for the Research and Treatment of Cancer; LC-13; lung cancer module; SAS, Self-Rating Anxiety Scale; SDS, Self-Rating Depression Scale; MDASI-T: M. D. Anderson Symptom Inventory-Tumor; PSQI, Pittsburgh Sleep Quality Index.
Higher scores in the EORTC HRQoL and function domains represent better status. Lower scores in the EORTC QLQ-C30 symptom categories, LC13, SAS, SDS, MDASI-T, PSQI represent less symptoms. Effect sizes = 0.2 small difference, 0.50 medium difference, 0.80 large difference.
Data are reported as mean ± standard deviation or median [inter-quartile range].
Patient reported questionnaires
There was a significant improvement in HRQoL including emotional function, global HRQoL and a decrease in symptoms including dyspnea and coughing. In addition, significant improvements were also observed in SAS, SDS, and PSQI (Table 5). There were no significant changes in other domains of HRQoL or the MDAIS-T.
Intervention progress
Participants who attended more than 17 sessions all finished learning the 8 styles of Tai Chi. At the end of the program, all these participants could walk on the treadmill for 20 to 30 minutes. The levels of the resistance exercise protocol prescribed at baseline was 1 to 3 level and at the end of the 12-week program, most participants could reach to the split squat in level 5, except 2 who had problems with their knees, the majority were at level 4 for the other movements. All participants were exercising at an intensity of “4- somewhat hard” on the Borg scale during aerobic and resistance exercise (refer to Table 2).
Discussion
This study aimed to determine the feasibility and safety of a novel 12-week multi-modal exercise program combining supervised aerobic and resistance exercises, simplified 8-style Tai Chi and a home-based program for patients following lung cancer treatment in China. There is a strong evidence base supporting the efficacy of supervised aerobic and resistance training for patients post lung cancer surgery, 8 however in this study we were interested in determining if the addition of traditional Tai Chi exercises would facilitate stronger adherence to exercise in a cohort of patients in China. Despite concluding that the intervention was safe, unfortunately the feasibility of the intervention was poor, and adherence rates to exercise were low and below the defined level of adherence. Promisingly, there were signals of improvements in response to exercise in the secondary outcomes of lung function, sleep, mood, global HRQoL, and some HRQoL domains for participants. However, as there was no control group, improvement over time from cancer treatment may be responsible.
All recruited participants underwent surgery only. There are several factors which made recruitment of patients receiving chemotherapy or radiotherapy difficult including: uncertainty of treatment completion dates, advice from medical staff to avoid crowds following chemotherapy and patients living too far from the hospital. In our study, the majority of participants were female and they were a relatively young cohort compared to the other published lung cancer and exercise trials conducted in Western countries. 8 Similarly, at baseline, most of our participants were well-nourished and had good performance on the 6MWT. Previous trials report baseline 6MWT of 428.6 ± 101.4 m (control group) versus 454.6 ± 116.7 m (intervention group) 31 and 407 ± 102 m (control group) versus 427 ± 124 m (intervention group) 32 ; significantly lower than the distances walked at baseline by our trial participants. These reasons may partially explain the high dropout rate; since the patients were younger, more of them may have had commitments such as work or caring for relatives (such as elderly parents or grandchildren) which made it hard for them to take up and adhere to the supervised exercise sessions. It is also possible that patients with poorer exercise capacity may have been discouraged by family members to participate in our study, as our consent rate was very low. The physical activity levels measured in our study were higher than data in an operable population from a Western country (5818 ± 628 steps/day (10 weeks following diagnosis) and 6171 ± 524 steps/day (6 months following diagnosis)). 5 This phenomenon may be explained by the fact that elderly people in China prefer walking as their main transportation while in Western countries driving by the elderly may be more common. 33 The hospital length of stay post-surgery observed in our study was similar to that previously reported in Western countries (8 [7-13] days). 34
Twenty-one percent of eligible participants who were contacted about the study consented to participation. In part, we attribute this to the fact that few of our patients received education about the benefits of exercise after surgery for lung cancer prior to being contacted about the study. Patients who had lung surgery did not have access to rehabilitation information before or during their hospitalization, so most of them were unfamiliar with this concept. We think it is necessary to promote this education to patients prior to their surgery and during their post-operative inpatient admission in future research and clinical practice.
In China, the Enhanced Recovery After Surgery (ERAS) mode has been recognized and accepted widely, so patients would be encouraged and assisted by the ward nurse to undertake early mobilization post-surgery. During the pre-operative phase, inconsistencies in physiotherapy services exist between hospitals/institutions. Few surgeons in our hospital understand the benefits of exercise during the pre-operative period. The reasons for this have been reported previously and include that physicians and nurses were not sure about what to advise, where to refer to and the services/resources available for them/their patients. 35 Thus, future collaboration and education is warranted for surgeons, nurses, and physiotherapists.
In this feasibility study, 47% of participants completed at least 17 of the desired 24 supervised sessions (70%), which is lower than in previously published trials of exercise interventions in cancer. 36 There are some reasons we may consider for explaining this low adherence rate. First, there were no previous randomized controlled trials conducted in mainland China focusing on lung cancer rehabilitation 6 to 12 weeks after surgery. 36 Although the enrolled patients’ homes were within a reasonable distance to hospital, there are still costs associated with travel, parking, and family members taking time off work so that participants could attend supervised exercise sessions. In the future, studies could involve participants’ family members or care givers in the decisions around participating in an exercise program so that they may have time to support the participant’s attendance for the study as needed. Thirdly, more than one third of our participants (35.3%) were still working, which was higher than the proportion of a similar study in Australia, wherein the percentage was 12%. 5 Adjusting the intervention frequency to once per week or altering times so participants can attend after work or on the weekend should both be considered in the future to ensure the participants can participate in the entire program. Two participants discontinued the exercise stating it was not enjoyable to them. Kampshoff et al found moderate evidence for a positive association between exercise history and exercise adherence, 37 additionally, Wong et al reviewed exercise program preferences among cancer survivors and found a wide variation of preferences, suggesting that tailored programs may optimize program adherence. 38 It is important for patients to perform exercise they enjoy. Tai Chi, the Chinese martial art involving slow and rhythmic movement, is popular among middle-aged and older Chinese people. 39 There is currently limited evidence regarding the benefits of adding Tai Chi to pulmonary rehabilitation programs for people with lung cancer. A trial of Tai-Chi delivered post lung cancer surgery (n = 120) is published as a protocol and is currently recruiting. 14 In the future we could individualize our aerobic exercise prescription by initially asking participants about their preferred exercise type. Anderson and Taylor 40 also found programs that included regulatory factors (ie, self-monitoring, action planning) resulted in the greatest levels of program adherence, in future we could utilize patient exercise diaries and or activity trackers for patients to self-monitor their exercise.
There were no severe adverse events associated with the study and only 3 minor events of musculoskeletal nature. This finding about safety is consistent with previous reports in the literature 8 and a review of Tai Chi which concluded it was unlikely to result in serious adverse events, but it might be associated with minor musculoskeletal aches and pains. 41
The promising findings regarding the secondary outcomes from this study support the future conduct of an adequately powered RCT, albeit with improvements to address the issues of adherence. Similar to our preliminary results for self-reported questionnaires, lung function, some domains of HRQoL and subjective sleep quality, previous RCTs and systematic reviews report positive improvements across several tumor streams,42,43 including 1 meta-analysis using a Tai Chi intervention. 44
In our study, the changes in 6MWT distance, SPPB and steps per day did not reach significance. This was influenced by the small sample size and the large variability in measures. It may also have been related to ceiling effects of the tests given the good baseline performance and maximal score for SPPB obtained. Alternate tests of exercise capacity, and function should be chosen in a future trial in China such as the incremental shuttle walk test and 30 second sit to stand test.
There are some inherent limitations of our study; first, the study is a feasibility study with no control group. We cannot therefore attribute the post-program improvements to the exercise program as these may be a result of natural recovery. Second, the sample of the study was too small to show the efficacy of the intervention; third, according to previous research, patients who are willing to be enrolled into supervised exercise programs may have a better baseline condition. 45 Finally, we did not record the duration of incomplete supervised sessions nor the adherence to the unsupervised home component of the program. Lack of knowledge of these details may weaken the fidelity of the program that was delivered. We plan to add use of a patient exercise diary to record unsupervised exercise adherence in the following RCT. While this study did not include a qualitative component, informal feedback from participants will be used in modifications made to the interventions investigated in future trials.
The findings from this study will inform changes to the design of a future adequately powered multi-site, assessor-blinded RCT of exercise and Tai Chi to be conducted in this population at 2 large centers in Jiangsu Province, China (registry number: NCT04185467).
Conclusion
This study demonstrated that a multi-modal exercise training program was safe when implemented 6 to 12 weeks after surgery, although the feasibility of the program in its current state is not supported given the low consent rate and low adherence to the intervention. Therefore, changes we recommend implementing to improve feasibility include: expanding the inclusion criteria, promoting education about surgery, deep breathing and exercise to patients prior to their surgery and/or during their post-operative inpatient admission. The positive change in the secondary outcomes indicate that this multi-modal exercise program has the potential to result in improvements for patients with lung cancer. Future large randomized control trials are warranted to test its effect.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Affiliated Hospital of Nantong University and Jiangsu provincial government (grant number BE2018670).