
Abstract
Keywords
Introduction
Echoing recommendations from the World Health Organization (WHO) on integrating traditional and complementary medicine into national health systems in an evidence-based manner, 1 there is a need to develop evidence-based clinical service recommendations for traditional and complementary medicine services. Existing systematic reviews (SRs) and overviews of SRs identify certain Chinese medicine (CM) interventions, inclusive of Chinese herbal medicine (CHM) and acupuncture and related therapies, as effective in managing cancer-related symptoms, such as fatigue, nausea, and vomiting, among palliative cancer patients.2-6 The palliative care version of the US National Comprehensive Cancer Network (NCCN) clinical practice guidelines in oncology7,8 has already recommended acupuncture for reducing cancer pain and cancer-related fatigue.
Since multiple stakeholders may have different perspectives and concerns regarding the implementation of these evidence-based CM service recommendations, it is important to bridge the gap between clinical evidence, health care experts’ experience, as well as patients’ values in decision making.9,10 The GRADE-ADOLOPMENT approach is a methodology that combines the advantages of adoption, adaptation, and de novo development of recommendations among an expert panel based on Grading of Recommendations Assessment, Development and Evaluation (GRADE), as well as the associated Evidence to Decision (EtD) framework. 11
As a core component of the approach, the EtD framework is applied for the following purposes:
Providing experts with a concise summary of the best available evidence about each criterion, namely, problem priority, benefits, harms, equity, acceptability, and feasibility
Allowing experts to consider these criteria in a comprehensive manner on whether an intervention should be recommended
Structuring and documenting experts’ justifications on how each criterion described above would influence the direction, strength, and implementability of the recommendations11-13
The GRADE-ADOLOPMENT approach successfully guided the development of recommendations and guidelines in Canada 14 and Australia, 15 and Saudi Arabia. 16 This approach has high adaptability for facilitating the formulation of health service recommendations in different health systems with distinct governance, financing, and service delivery models.
Cancer is a major cause of disease burden in Hong Kong. According to the Hong Kong Hospital Authority, there were 31 468 new cancer cases and 14 209 cancer deaths in 2016. 17 Among local cancer patients, 68.9% received palliative care in publicly funded health care setting in 2015. 18 A 2009 survey reported that over 50% of Hong Kong cancer patients receiving conventional treatments also concurrently utilized CM services with the expectation of reducing side effects of conventional treatments, limiting tumor progression, and improving their quality of life. 19 Nearly 90% of these patients also supported the government to integrate CM and biomedicine (BM) in cancer treatment within the Hong Kong health system. 19
Under the influence of colonial history, CM is commonly used as a complement to BM, with the later occupying a dominant position in the health system. 20 According to previous Hong Kong surveys, physicians and nurses held mixed attitudes toward the value of CM.21,22 Interprofessional collaboration is inevitable if CM services are to be integrated into the Hong Kong health system. 23 Therefore, acceptance and endorsement from physicians and nurses are considered essential in the successful implementation of CM service recommendations in Hong Kong. 24 In line with international experiences, 25 physicians and nurses should be regarded as key stakeholders in the formulation of CM service recommendations.
Numerous factors are hindering the transition from parallel to integrative practice model. 26 A previous SR showed that an unverified perception on the lack of high-quality evidence supporting effectiveness and safety of CM was a common rhetorical tool employed among physicians to oppose collaboration with CM practitioners (CMPs). 25 One of the suggested solutions to change physicians’ opposition toward collaboration with CMPs was to implement existing CM modalities supported with sufficient evidence, and to design interprofessional collaboration plans accordingly. 25
To translate evidence-based CM modalities into integrative practice, the current study aimed to establish consensus on evidence-based CM clinical service recommendations for cancer palliative care among Hong Kong experts using the EtD framework approach.
Methods
This Delphi survey is reported in accordance to the standard for Conducting and Reporting of Delphi Studies (CREDES). 27 Ethical approval was obtained from the Survey and Behavioural Research Ethics Committee, The Chinese University of Hong Kong (Reference No. 023-17). The workflow of the study and details are presented in Figure 1.
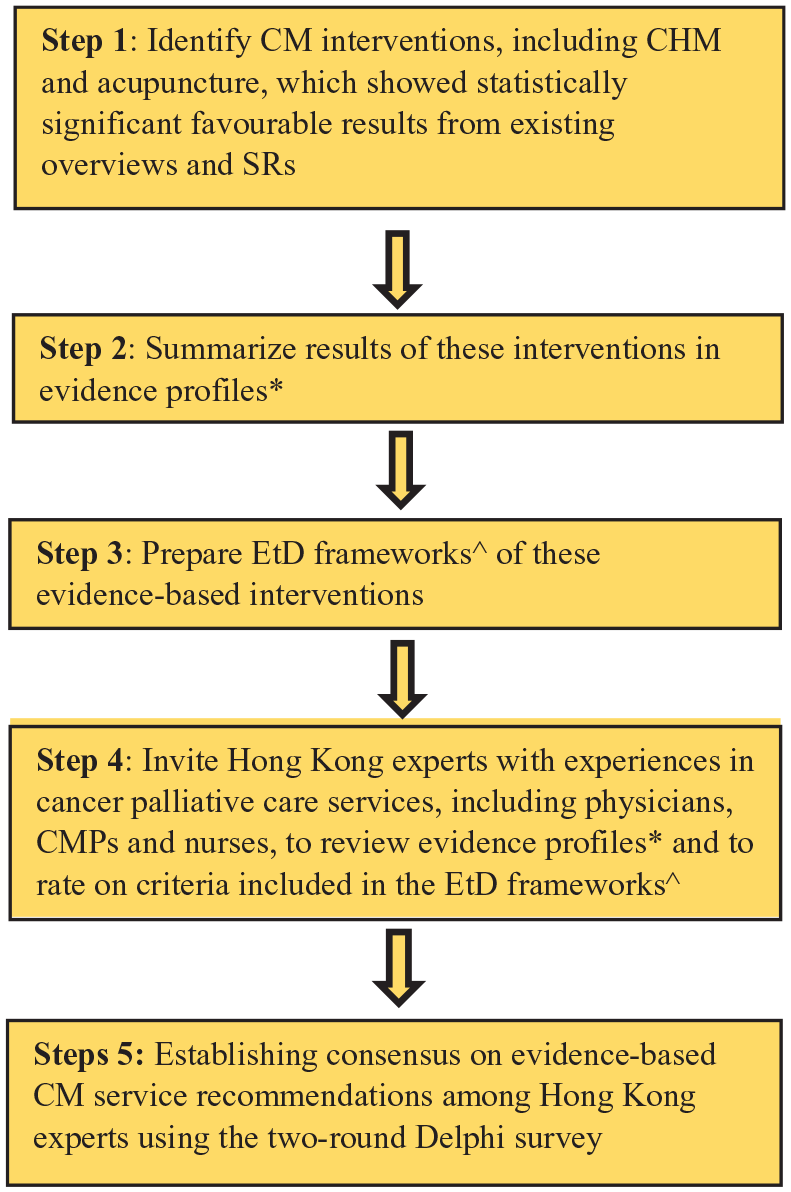
Workflow of developing Chinese medicine clinical service recommendations for cancer palliative care.
Part 1: Preparation of Evidence Profiles and EtD Frameworks of CM Interventions for Cancer Palliative Care
Three overviews of SRs and 2 SRs2-6 on CM interventions for cancer palliative care published in late 2015 and early 2016 were selected for this part. They were selected as they had critically appraised and summarized the most up-to-date clinical evidence on CHM, as well as acupuncture and related therapies, for cancer palliative care at the time of our study. In these rigorous syntheses,2-6 methodological quality of 74 included SRs was evaluated using the AMSTAR instrument, 28 while risk of bias of 88 included randomized controlled trials (RCTs) were assessed with the Cochrane risk of bias tool. 29 Strengths and limitations on the synthesized evidence were also highlighted by the original authors.2-6
By identifying statistically significant favorable results from these synthesis,2-6 our study focused on a total of 7 CM interventions. Results of these interventions were displayed in 7 evidence profiles, which presented in a consistent format: number of studies; number of participants; effects of binary and continuous outcomes including their corresponding 95% confidence intervals (CIs) and P values; and quality of evidence.30,31 Quality of evidence was assessed by the Clinical and Health Intervention Meta-analysis Evidence RAting System (CHIMERAS; Appendix 1, Supplementary material, available online). 32 The rating was conducted by the investigators, and the Delphi experts were not required to rate evidence quality. Evidence profiles of the 7 CM interventions are shown in Appendix 2 (Supplementary material, available online).
EtD frameworks of the 7 evidence-based CM interventions were then prepared. These frameworks facilitated Delphi experts’ decision-making process, moving from results presented in evidence profiles to recommendations, through explicit consideration of the following criteria: deemed priority of the problem, benefits, harms, equity, acceptability, and feasibility of CM interventions. 33 In this structured approach, experts were invited to consider the criteria mentioned above thoroughly,10,12 and subsequently, each expert was invited to provide a rating on whether a specific CM intervention should be recommended in the Hong Kong health system. Rating of recommendations was assessed on a 4-point Likert-type scale, ranging from “recommend against this option” (ie, strongly disagree with the proposed CM intervention), “suggest not this option” (ie, disagree with the proposed CM intervention), “suggest this option” (ie, agree with the proposed CM intervention), to “recommend this option” (ie, strongly agree with the proposed CM intervention).11,34 Experts were also invited to provide additional qualitative comments on implementation, monitoring, evaluation, and future research possibilities.7,31 EtD frameworks of the 7 CM interventions are shown in Appendix 3 (Supplementary material, available online).
Part 2: Sampling of Experts
Purposive sampling is a technique widely used to identify individuals who are especially knowledgeable about, or experienced with, a phenomenon of interest. 35 In the purposive sampling of this study, we selected a balanced number of conventionally trained physicians, CMPs, and nurses (4 experts from each of the 3 professions) with at least 1 year of professional experience in cancer palliative care service provision within the Hong Kong health system. Under such maximum variation sampling strategy, experts from different health care disciplines in cancer palliative care were identified to provide unique and diverse insight on CM service recommendations, ensuring balanced perspectives across members in the expert panel. 35 Since a smaller sample size would enable higher response rate, total number of experts recruited was limited to 12. 36 All participating experts were de-identified to safeguard confidentiality and independence of judgements during the process.
Thirteen potential experts were approached through the investigators’ professional networks. The experts were first contacted via email in July 2018, along with objectives, study details, and written informed consent forms. Online introduction to the Delphi survey procedures was then provided to the 12 experts who returned their signed informed consent. The introductory package included a narrated online presentation of the whole study process, an online video on interpretation of evidence profiles, and an overview of the EtD framework.
Part 3: Round 1 Delphi Survey Data Collection and Data Analysis
The Round 1 Delphi survey package, which included a questionnaire on demographic and professional information, evidence profiles, and EtD frameworks of evidence-based CM interventions prepared in Part 1, was then emailed to the participants. Each expert was invited to complete and return the questionnaire by email.
For each CM intervention, Round 1 median rating of recommendation was calculated alongside interquartile range (IQR) to demonstrate magnitude of disagreement among experts. Median and IQR are preferred as they are less influenced by outliers when compared with mean and standard deviation.36,37 Agreement on the recommendation was expressed in percentage (%). With reference to the agreement standard adopted in previous studies, the consensus cutoff level of this study was set at 75%. 38 In other words, an intervention would reach positive consensus as a service recommendation if ≥75% of experts rated “suggest this option” or “recommend this option” on the 4-point Likert-type scale; while negative consensus would be attained when ≥75% rated “suggest not this option” or “recommend against this option.” 38 Interventions achieving positive consensus in Round 1 were considered as service recommendations. For interventions without consensus, qualitative comments were summarized and presented for further evaluation in Round 2. Besides, assessment results on each EtD framework criterion were expressed in percentage (%), based on the proportion of experts making a specific rating.
Part 4: Round 2 Delphi Survey Data Collection and Data Analysis
In Round 2, the same panel of experts were asked to reassess CM interventions that neither reached positive nor negative consensus in Round 1. Delphi survey package for this round included the following: (1) experts’ own rating in Round 1; (2) median ratings with IQRs and percentage agreement; (3) anonymous qualitative comments; as well as (4) assessment results on each EtD framework criterion from all other experts. Data collection and analysis similar to Round 1 were then performed. A list of finalized, local experts–endorsed CM clinical service recommendations was generated at the end of Round 2, including all interventions with positive consensus across both rounds.
Results
Participants
Twelve cancer palliative care experts agreed to take part in the 2-round Delphi survey. The response rates of completing both rounds were 100.0%. The expert panel comprised physicians (n = 4), CMPs (n = 4), and nurses (n = 4), with 4 of them belonging to more than 1 profession. One third of the experts worked in public tax funded hospitals (33.3%) and one fourth (25%) in private outpatient settings at the time of the study. Majority of experts (66.7%) had professional experience in cancer palliative care for 7 years or more, while 33.3% had been conducting relevant research for over 15 years (Table 1).
Demographic Data of Participants in the 2-Round Delphi Survey (n = 12).

Abbreviation: CMP, Chinese medicine practitioner.
Service Recommendations Developed in Round 1 Delphi Survey
Overall Rating Results
Three out of 7 evidence-based CM interventions reached positive consensus as service recommendations in Round 1. Median rating of these 3 recommendations ranged from 2.5 to 3.0 (IQR = 0.00-1.00) on a 4-point Likert-type scale, while the percentage agreement ranged from 83.4% to 91.7% (Table 2). Among the recommendations, quality of evidence assessed by CHIMERAS on (1) acupuncture for reducing fatigue among palliative cancer patients and (2) acupressure for reducing fatigue among palliative cancer patients were moderate; while the quality of evidence on (3) moxibustion for reducing nausea and vomiting among patients receiving chemotherapy was high.
List of Interventions and Agreement Results in the 2-Round Delphi Survey.

Abbreviations: CHIMERAS, Clinical and Health Intervention Meta-analysis Evidence RAting System; IQR, interquartile range; N/A, not applicable.
Not applicable since the topic has achieved positive consensus in the first round of Delphi survey.
Detailed prescriptions for Gui-dan-san-zi-san (桂丹三籽散): gui zhi桂枝 30 g, bai jie zi 白芥子 30 g, wu zhu yu吳茱萸 30 g, tu si zi菟絲子 30 g.
Detailed prescriptions for Zi-long-jing (紫龍金): 由huang qi 黃芪, dang gui 當歸, bai ying 白英, long kui 龍葵, dan shen 丹參, ban zhi lian 半枝蓮, she mei 蛇莓, yu jin 鬱金等組成, 天津中新藥業集團股份有限公司龍順榕製藥廠生產, 批號 Z20010064.
Rating Results From the Evidence to Decision Framework
Priority of the problem
Over 70% of the experts on the panel agreed that all 3 recommended CM clinical services were “a priority” from their perspectives (Figure 2).
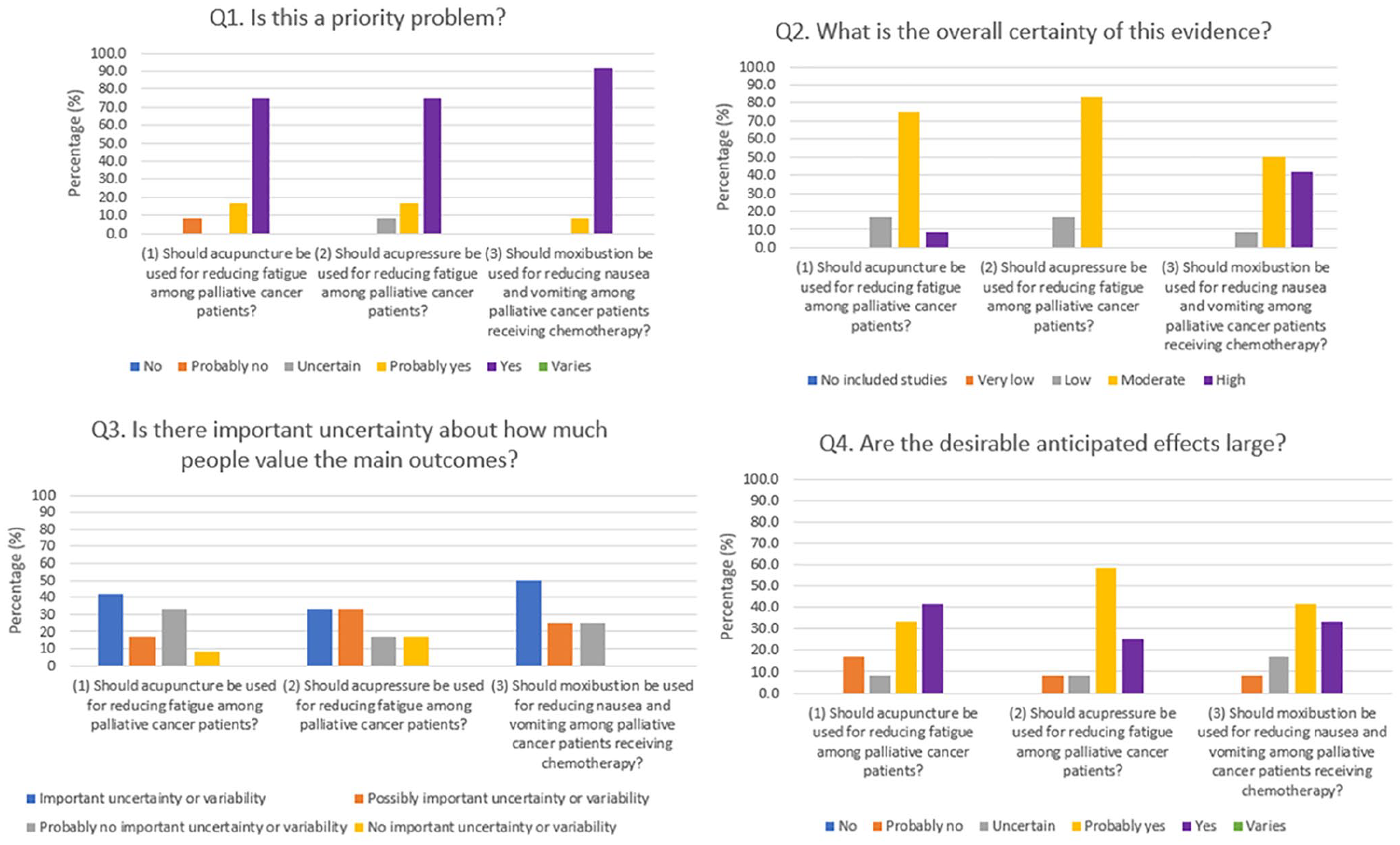
Evidence to Decision (EtD) framework assessment results on Chinese medicine clinical service recommendations: Q1 to Q4.
Benefits and harms of the interventions
More than 80% agreed that overall certainty of evidence among the 3 recommendations were moderate or high (Figure 2). However, over half of experts believed that there was “important” or “possibly important” uncertainty about how much cancer patients might value the main outcomes (Figure 2). More than 75% regarded desirable anticipated effects of the 3 recommendations were “probably large” or “large.” Over 50% indicated that undesirable anticipated effects of the 3 recommendations, except on acupuncture for reducing fatigue, were “probably small” or “small” (Figures 2 and 3). More than 75% agreed that desirable effects were large or probably large relative to undesirable effects (Figure 3).

Evidence to Decision (EtD) framework assessment results on Chinese medicine clinical service recommendations: Q5 to Q8.
Some experts provided qualitative comments on benefits and harms of these 3 recommendations. For (1) acupuncture, one physician believed that it brought less adverse effects than CHM, as the latter might induce herb-drug interactions. However, the physician also suggested that patients receiving chemotherapy were more vulnerable to infection; and therefore, they should avoid receiving acupuncture treatment. For (2) acupressure, one physician pointed out that there was a lack of clinical evidence supporting its use for fatigue. Nonetheless, one CMP and one nurse regarded acupressure as safe and noninvasive under careful administration. For (3) moxibustion, one CMP highlighted that it was a very affordable treatment. As recommended by one physician and one nurse, patients receiving chemotherapy should be monitored for possible burns induced by moxibustion, as this might cause subsequent infections (Table 3).
Qualitative Comments on Chinese Medicine Clinical Service Recommendations.

Abbreviations: CHM, Chinese herbal medicine; CMP, Chinese medicine practitioners; RCTs, randomized controlled trials.
Equity, acceptability, and feasibility of the interventions
More than 40% believed that the 3 recommendations would “increase” or “probably increase” health inequities (Figure 3). However, they provided no qualitative comments on how such inequities might arise, as well as the potential impact of such inequities.
Over 75% recognized that these recommendations were acceptable to key stakeholders, and were feasible to implement in the Hong Kong health system (Figures 3 and 4). To this end, some experts provided the following qualitative comments: (1) 2 CMPs and 1 nurse claimed that acupuncture would be more acceptable by the public as compared with CHM, since the former would not cause harmful herb-drug interactions; (2) 1 CMP suggested that acupressure would be widely used in hospital and home setting because it was safe and noninvasive; and (3) 1 CMP recommended that appropriate ventilation of smoke particulates emitted during moxibustion would be required during service provision. When implementing these 3 recommendations, 2 CMPs, 1 physician, and 1 nurse suggested that close monitoring of patients’ health conditions would be of high importance, given the vulnerability of palliative cancer patients (Table 3).

Evidence to Decision (EtD) framework assessment results on Chinese medicine clinical service recommendations: Q9 to Q10.
Balance of consequences
More than 60% agreed that desirable consequences of the 3 recommendations probably or clearly outweighed undesirable consequences (Figure 4). Details of experts’ qualitative comments, including recommendations for future research, are shown in Table 3.
Interventions Without Consensus After the 2-Round Delphi Survey
Overall Rating Results
In the Round 2 Delphi survey, evidence profiles and EtD frameworks of the remaining 4 interventions were reevaluated. None of these interventions reached positive or negative consensus. The median rating ranged from 2.00 to 3.00 (IQR = 1.00-1.75), while the percentage agreement ranged from 33.3% to 66.7% (Table 2).
Quality of evidence assessed by CHIMERAS regarding (1) electroacupuncture plus antiemetics among palliative cancer patients for reducing nausea and vomiting and (2) hyperthermia plus Gui-dan-san-zi-san (桂丹三籽散) among patients receiving radiotherapy for reducing pain were moderate; while the quality of evidence on (3) Zi-long-jing (紫龍金) among patients receiving chemotherapy and (4) Ganoderma lucidum (靈芝) extract among patients receiving chemotherapy or radiotherapy for improving quality of life were high.
Panel experts expressed concerns on the safety of these 4 interventions. For (1) electroacupuncture plus antiemetics, one physician suggested the avoidance of electroacupuncture among patients with pacemaker, artificial joints, and neuropathy. For (2) hyperthermia plus Gui-dan-san-zi-san and (3) Zi-long-jing, safety of applying hyperthermia among patients receiving radiotherapy, as well as potentially harmful herb-drug interactions between Zi-long-jing and chemotherapeutic agents, remained to be main concerns among experts from all disciplines. For (4) Ganoderma lucidum extract, one physician and one nurse expressed concerns on its negative impact on blood cell count, as well as possible negative herb-drug interactions between Ganoderma lucidum and chemotherapeutic agents. Detailed reporting of rating results on the EtD framework criteria and other qualitative comments are presented in Appendix 4 (Supplementary material, available online).
Discussion
Summary of Findings
Three out of 7 evidence-based interventions reached positive consensus as service recommendations. These recommendations were (1) acupuncture for reducing fatigue among palliative cancer patients; (2) acupressure for reducing fatigue among palliative cancer patients; and (3) moxibustion for reducing nausea and vomiting among patients receiving chemotherapy.
Considering Patients’ Values in Developing Future Service Recommendations
Although palliative care ideally should align strongly with patient-centered principles, 39 our findings indicated that the experts reported substantial uncertainty about how much patients might value the main outcomes attributable to CM clinical services that failed to reach consensus. This finding was contradictory to the result of a representative survey showing high prevalence of CM service usage in Hong Kong, with 16.5% of the population consulting CMP at least once in a 12-month time frame. 40
According to a previous SR of qualitative and quantitative studies, some patients with chronic or serious diseases, including cancer, chose to use CM because of its perceived strength in (1) providing tonic care; (2) individualizing treatment to address various health needs; (3) bringing few adverse effects; (4) guiding for health maintenance and health promotion; and (5) improving health conditions that could not be cured completely by BM. 41 However, CM was perceived to be less effective in managing serious diseases and slow in demonstrating treatment effect when compared with BM. 41 As patients believed that the co-use of BM and CM would offset weakness of both systems of medicine while retaining their specific strengths, they intended to use BM and CM services simultaneously to address their complex needs in a holistic way. 41 On the other hand, both physicians and CMPs agreed that patients should have the right to choose between BM and CM services in a focus group study. 23 From the perspective of patient-centered care, our findings suggested that it would be important to address health care professionals’ uncertainty about patients’ value in CM clinical services in the future.
Since patients’ role in clinical decision-making is becoming increasingly recognized, 42 future development of evidence-based clinical service recommendations may consider adding patients to the expert panel. 43 Besides, experts suggested using validated patient-reported outcomes (PROs) tools to monitor responses to CM treatments. This may help improving health care professionals’ understanding on impact from CM service delivered, 44 particularly in enhancing patients’ quality of life and functional performance.
Uncertainty on Adverse Events as a Barrier to Interprofessional Collaboration
Modalities for which consensus was reached in this study were acupuncture and related therapies, with the use of electroacupuncture being rejected by the experts. Despite evidence on the effectiveness of electroacupuncture for reducing nausea and vomiting, 3 this intervention was rejected due to physicians’ perceived harm of performing electroacupuncture among patients with cardiac pacemaker 45 and neuropathy. 46 This may indicate an exaggeration of undesirable effects attributable to electroacupuncture, 47 since Delphi result concluded that the use of electroacupuncture should be rejected among all palliative care patients. Such potentially overcautious view implies a need for disseminating evidence on safety of acupuncture treatments among conventionally trained health care professionals, rather than focusing dissemination solely on evidence of efficacy.
Potential interprofessional conflicts over malpractice liability may also be a root cause for deep concerns on CM-related adverse events among the experts. Existing literature suggested a number of strategies for reducing the uncertainty 48 among physicians, CMPs, and nurses: (1) determine clinical risk level; (2) document evidence supporting the choice of BM and CM treatments in an appropriate manner; (3) elicit informed consent for patients before carrying out any integrative treatments; (4) closely monitor patients’ health conditions; and (5) improve communications among different professions and arrange for interprofessional consultation if needed. 48
However, these strategies for reducing uncertainty may not be applicable for the co-use of CHM and conventional medications in an interprofessional collaborative environment. In our study, concerns over potentially harmful herb-drug interactions 49 were repeatedly expressed as a reason for rejecting CHM interventions, even though experts were unable to cite research supporting such concerns. Existing evidence suggested that pharmacokinetic interactions between CHM and chemotherapeutics 50 might lead to unpredictable toxicities and even multi-organ failure. 51 Building a strong evidence base on the safety of CHM, as well as herb-drug interactions using appropriate observational studies should be regarded as a research priority.
Possible Health Inequities Caused by Implementing the Recommendations
In Hong Kong, fees for CM general consultation service in non–private sector are regulated by the government at a standardized and reasonable level, with provision of subsidies for patients who are in need. Private CM consultation fees are determined by the market without regulation. 52 According to the 2019 Thematic Household Survey, a representative survey monitoring health service use among noninstitutionalized Hong Kong population, only 0.5% of the interviewees utilized CM service delivered by non–private sector. Majority (16.0%) consulted CMPs in the private sector. 40 Therefore, if the recommended services are implemented, most patients will access them via private CMPs, which would incur much more out-of-pocket expenses. This could be the reason why our experts expressed concerns on widening inequities on CM service access. Policies to reduce financial barriers are needed prior to implementing our current recommendations, for example, through enhancing public-private partnership (PPP). 26 PPP can facilitate the contractual relationship between a public agency and a private entity, thus promoting greater private sector participation in the provision of evidence-based CM services for those who cannot afford. 53
Tailoring Implementation Strategies to Inform Future Interprofessional Collaboration
While experts were generally positive on the recommendations’ implementability, there is a need to tailor practical strategies for promoting their actual implementation. The design of implementation strategies may follow a 3-step approach described as follows. In Step 1, contextual barriers and facilitators of implementing the recommendations can be identified through conducting qualitative studies guided by the Consolidated Framework for Implementation Research (CFIR). 54 In Step 2, assessment results from Step 1 can guide the generation of implementation strategies. These strategies should be tailored to address barriers, and to enhance facilitators of implementation. Implementation strategies catalogues developed by the Expert Recommendations for Implement-ing Change (ERIC) study 55 offer a wide range of possible interventions. In Step 3, proposed implementation strategies identified in Step 2 should be finalized via establishing local expert consensus using Delphi techniques, so as to increase stakeholders’ acceptability. 56
Strengths and Limitations
A Delphi survey approach based on the GRADE-ADOLOPMENT framework was first applied for developing evidence-based CM clinical service recommendations for cancer palliative care. These evidence-based recommendations have been contextualized to address relationship between BM and CM, as well as features of the Hong Kong health system. The use of EtD framework offered structured recordings of judgements in the process of reaching recommendations among a multidisciplinary panel of experts. This inclusive approach would facilitate interprofessional understanding in the future implementation of these recommendations.
Since this study focused on CHM and acupuncture and related therapies identified from existing overviews of SRs and SRs,2-6 we have omitted other important interventions, such as Tai Chi,57,58 Qigong,57,58 Tuina, 58 and cupping. 59 Purposive sampling of experts via the investigators’ professional networks might induce researcher bias in the selection process. 60 Nevertheless, we believe that the impact of researcher bias would be small, as service recommendations could not be made unless experts across all disciplines arrived at consensus. It is unlikely that researcher bias alone could foster consensus at a high cutoff level of 75% during the Delphi process. Last, our service recommendations were generated without involvement of patients and caregivers. Future Delphi studies should consider adding them to the expert panel, of which the process will empower them in coproducing evidence-based guidelines meaningfully. 43
Conclusion
Three evidence-based CM interventions reached positive consensus as service recommendations for cancer palliative care among experts in this GRADE-ADOLOPMENT–based 2-round Delphi survey. To implement these 3 service recommendations in the Hong Kong health system where BM and CM are practiced in a parallel manner, further study is needed for tailoring implementation strategies that address needs of local context, with strong inputs from frontline clinicians across the 2 disciplines.
Supplemental Material
ServiceGRADE_clean_20200520_v1 – Supplemental material for Development of Evidence-Based Chinese Medicine Clinical Service Recommendations for Cancer Palliative Care Using Delphi Approach Based on the Evidence to Decision Framework
Supplemental material, ServiceGRADE_clean_20200520_v1 for Development of Evidence-Based Chinese Medicine Clinical Service Recommendations for Cancer Palliative Care Using Delphi Approach Based on the Evidence to Decision Framework by Charlene H. L. Wong, Irene X. Y. Wu, Jon Adams, Amie Steel, Jon Wardle, Justin C. Y. Wu, Ting Hung Leung and Vincent C. H. Chung in Integrative Cancer Therapies
Supplemental Material
Supplementary_material_20200520 – Supplemental material for Development of Evidence-Based Chinese Medicine Clinical Service Recommendations for Cancer Palliative Care Using Delphi Approach Based on the Evidence to Decision Framework
Supplemental material, Supplementary_material_20200520 for Development of Evidence-Based Chinese Medicine Clinical Service Recommendations for Cancer Palliative Care Using Delphi Approach Based on the Evidence to Decision Framework by Charlene H. L. Wong, Irene X. Y. Wu, Jon Adams, Amie Steel, Jon Wardle, Justin C. Y. Wu, Ting Hung Leung and Vincent C. H. Chung in Integrative Cancer Therapies
Footnotes
Author Contributions
The following contributed to this work. Study concept and design: CHLW, IXYW, and VCHC. Acquisition of data: CHLW and VCHC. Interpretation of data: CHLW, IXYW, and VCHC. Figures 1 to 4 preparation: CHLW. Tables 1 to 3 preparation: CHLW and IXYW. ![]() preparation: CHLW. Drafting of the manuscript: CHLW. Critical revision of the manuscript for important intellectual content: IXYW, JA, AS, JW, JCYW, THL, and VCHC. Administrative, technical, or material support: CHLW. All authors reviewed the manuscript, agreed to all the contents, and agreed for the submission.
preparation: CHLW. Drafting of the manuscript: CHLW. Critical revision of the manuscript for important intellectual content: IXYW, JA, AS, JW, JCYW, THL, and VCHC. Administrative, technical, or material support: CHLW. All authors reviewed the manuscript, agreed to all the contents, and agreed for the submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the High-level Talents Introduction Plan from Central South University (No. 502045003).
Ethical Approval
Ethical approval was obtained from the Survey and Behavioural Research Ethics Committee, The Chinese University of Hong Kong (Reference No. 023-17).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.