
Abstract
Introduction
Hand-foot syndrome (HFS) is a side effect triggered by certain chemotherapeutic agents, specifically pegylated liposomal doxorubicin, capecitabine, 5-fluorouracil, cytarabine, or docetaxel. Incidence of HFS varies from 6% to 64%. Moreover, the incidence of HFS associated with capecitabine is 50% to 60%, while multiple drug combinations can further increase the incidence. 1 Patients typically experience palmoplantar dysesthesia that progresses from tingling sensation to burning pain. In addition to pain, patients may experience palmoplantar erythema, edema, blistering with subsequent desquamation, erosion, and ulceration. Moreover, HFS affects everyday activities, such as walking, drinking, eating, and others. Besides, some patients may lose their fingerprints (dermatoglyphics).2,3 Nevertheless, HFS is not a life-threatening disease; so far, there is only one case of reported death following HFS occurrence. 4 However, the exact pathogenesis of HFS remains poorly understood. It is believed that HFS may be related to a cyclooxygenase inflammatory-type reaction, accumulation of capecitabine metabolites, enzymes, and transporters involved in the metabolism and absorption. 5
Considering that HFS is a chemotherapy-related problem, its symptoms usually disappear following the lowering of chemotherapy dose or treatment suspension. So far, no effective strategies have been found to prevent or reverse HFS. Treatment aims at symptom control, including decreasing inflammation, wound care, decreasing hyperkeratosis, and pain control. So far, various recommendations concerning topical approaches for HFS have been proposed; nevertheless, the evidence on their value is still controversial. For example, some studies have suggested pyridoxine as effective drugs, while others reported no beneficial effect from this therapy and the agent is still controversial.6-9 On the other hand, pregabalin, 10 celecoxib, 11 and urea cream 12 have been shown to possess potential efficiency for HFS. Currently, the most effective management approach for HFS is preventive nursing 3 and dose intensity modification. Nowadays, urea ointment is usually used for HFS patients to alleviate the condition of chapped skin in clinic. HFS is usually a strong predictor of the effect of capecitabine, so dose intensity modification or suspension decrease the curative effect of anti-tumor drug.13,14
Recently, a Chinese herbal extract LC09 decoction has shown to be effective in treating HFS-related pain. 15 In that trial, LC09 was boiled directly into decoction, but in this trial, we use granules to promote convenience and verify whether granules are equally effective. The drug is usually applied externally, by soaking the affected hands and feet in the solution containing the drug, and thus it is considered a safer treatment approach. Previous clinical trials have illustrated the effect of some Chinese herbal medicine for treatment of HFS. 3 But in these trials, external treatment was compared with oral treatment, so they are not a strict randomized controlled trial. This study aimed to evaluate LC09’s validity and safety via a strictly randomized, double-blind, and parallel-controlled trial.
Patients
The inclusion criteria were the following: (1) patients with histologically confirmed colorectal cancer or breast cancer (colorectal cancer was in an advanced stage or patients were undergoing adjuvant therapy after radical resection; breast cancer at the stage of recurrence or metastasis); (2) HFS with level 1 or above after receiving capecitabine as part of routine standard treatment; (3) patients who will be treated with capecitabine for at least 2 cycles, including the cycle that they are enrolled; (4) Eastern Cooperative Oncology Group performance status 0 to 2; (5) ability to cooperate with HFS grade evaluation, understanding and the willingness to sign a written informed consent; and (6) age between 18 and 80 years. Exclusion criteria were the following: (1) concurrent with level 1 or above peripheral neuropathy (such as diabetic neuropathy or chemotherapy induced peripheral neuropathy); (2) other acute or chronic inflammatory conditions or infections of the hands or feet; (3) currently taking other treatment for HFS (including urea-based cream, pyridoxine, celecoxib, etc); and (4) history of severe or uncontrolled organic disease or infection, such as heart, pulmonary, or renal failure that cause the termination of chemotherapy. A total of 195 patients were assessed, and 156 patients met the inclusion criteria.
China-Japan Friendship Hospital Ethics Committee approved the study protocol (Ethical Code: 2016-6), and all patients read and signed the informed consent form.
Study Design
The study is a randomized, multiple-center, double-blind, and parallel-controlled trial. Random numbers were produced by computer by the pharmaceutical factory and a serial number was assigned on the packing bags of LC09 or control; identical packing bags were used for LC09 and control. There are 2 copies of the label showing the grouping condition. One copy was kept by the pharmaceutical factory, and the other was kept by the scientific research department of China-Japan Friendship Hospital. If severe adverse reaction occurred, researchers could apply to the scientific research department of China-Japan Friendship Hospital to learn which group the patient was in, stop the trial, and take measures to treat. Doctors, patients, and statisticians were blind to the grouping. Doctors dispensed LC09 from number one to the end according to the sequence of patients’ consults. All patients recognized with HFS were randomly assigned to the treatment group (n = 78) or control group (n = 78). The treatment group received a total of 110 g per day of Chinese herbal compound LC09 (30 g of Astragalus membranaceus, 12 g of flowers carthami, 20 g of lithospermum, 30 g of geranium wilfordii, and 18 g of radix angelicae). The control group was treated with a control formula. In this trial, LC09 was made into granular formulation (for manufacturing method, see Supplementary Figure). Both LC09 and control were prepared by Beijing Tcmages Pharmaceutical Co Ltd. Patients in the treatment group soaked their feet or hand for about 20 minutes (twice daily) in 1000 mL warm water (~35 to 38 °C) that contained dissolved LC09. The control group used a granular formulation made of low-dose herbs in a concentration of about 5% with 95% starch. Low-dose herbs included Rehmannia Glutinosa, rhizoma alismatis, garden burnet, and calamus, which are not effective for HFS according to traditional Chinese medicine (TCM). These 4 herbs are used to simulate the smell and color of LC09, and the concentration of 5% has almost no effect. 16 Additionally, the appearance and smell of the control formula before and after dissolving were similar to LC09. The control group followed the same method as the treatment group. Meanwhile, patients in both groups were given urea cream, which is reported effective for HFS. Urea cream is made by Shanghai Winguide Huangpu Pharmaceutical. Urea cream is different from Vaseline as it is registered. This is mainly because urea cream is more effective than Vaseline, which mainly lubricates skin, and this conforms to ethical standards. Both groups used urea cream, so it would not influence the comparability of the trial groups. LC09 and control were sealed in aluminum foil sachets with the same appearance.
Main outcomes included the National Cancer Institute (NCI) criteria; HFS effectiveness rate (= effect/total patients of one group, effect: NCI grade decrease of one grade or more); Numerical Rating Scale (NRS) pain scores; and pain alleviation rate (= alleviated/total patients of one group, alleviated: NRS pain scores decrease one grade or more; Table 2). Patients were asked to keep a symptom diary based on the related symptoms in their hands and feet and condition of pain. Data from the diary were assessed by the investigator using NCI CTCAE (Common Terminology Criteria for Adverse Events) Version 4.03 17 (Table 1) and NRS pain scores (Table 2) every week for a total of 2 chemotherapy cycles. Secondary indexes were Instrumental Activity of Daily Living (IADL; Cronbach α = 0.932), 18 Dermatology Life Quality Index (DLQI; Cronbach α = 0.87), 19 and chemotherapy completion rate. Patients were assessed with IADL and DLQI before intervention, after 1 week of intervention, and after completing the treatment of 2 cycles. DLQI and IADL have not been tested in HFS patients, and there is no validity and reliability related data. All the data were collected by 2 experienced doctors who were trained and used the same instruction words in conducting evaluations. NCI grade was evaluated by 2 doctors who took photos of every enrolled patient. Then the NCI grade was adjusted by one specialist according to the collected photos. IADL and DLQI scales were filled by patients. Except for explaining some items that were difficult to understand, the 2 doctors did not intervene or guide patients’ choices. The following conditions were considered for trial completion: (1) 2 completed cycles of capecitabine-containing chemotherapy, including the cycle of inclusion; (2) if NCI grade reached the grade 0 after <2 cycles, the trial was concluded and recognized as effective; and (3) if (a) NCI grade was not reduced or was increased by one grade or more, or (b) if NRS pain scores increased for one or more grades, the trial was ended and recognized as showing lack of effectiveness.
NCI-CTCAE Version 4.03 a .

Abbreviations: NCI, National Cancer Institute; CTCAE, Common Terminology Criteria Adverse Events.
NCI grade decreases ≥1grade is recognized as effective.
NRS Pain Scores (From 1 to 10) a .

Abbreviation: NRS, Numerical Rating Scale.
NRS pain score decrease ≥1 grade is recognized as effective.
High-Performance Liquid Chromatography (HPLC) Analysis
Octadecyl silane chemically bonded silica was used as filler (column length is 100 mm, inside diameter is 2.1 mm, and grain diameter is 1.8 µm). We used acetonitrile as eluent A and 0.2% formic acid as eluent B for calycosin-7-glucoside; acetonitrile-water (32:68) as eluent for astragaloside; methyl alcohol-acetonitrile-0.2% phosphoric acid solution (26:2:72) as eluent for hydroxyl safflower yellow pigment A; methyl alcohol-0.4% phosphoric acid solution (52:48) as eluent for kaempferide; and acetonitrile as eluent A and 0.2% formic acid as eluent B for oxypeucedanin hydrate and imperatorin. We used an ultraviolet detection wavelength of 260 nm for calycosin-7-glucoside; 403 nm for hydroxyl safflower yellow pigment A; 367 nm for kaempferide; and 220 nm for oxypeucedanin hydrate and imperatorin. Besides we used an evaporative light-scattering detector to test astragaloside. The flow rate was 0.3 mL/min, and the column temperature was maintained at 35 °C. About 0.5 g sample was extracted using 50 mL methanol or 50 mL homeopathic alcohol through ultrasonic oscillation (rate of work is 250 kw, frequency is 50 Hz) for 30 to 60 minutes and then filtered. Ten microliters of sample was directly injected into the HPLC system. The retention times for calycosin-7-glucoside, astragaloside, hydroxyl safflower yellow pigment A, kaempferide, oxypeucedanin hydrate, and imperatorin were 12.6, 31.0, 11.5, 17.5, 9.4, and 14.9 minutes, respectively (Figure1). LC09 (1 g) contained 0.68 mg of calycosin-7-glucoside, 0.78 mg of astragaloside, 3.2 mg of hydroxyl safflower yellow pigment A, 0.35 mg of kaempferide, and 0.47 mg of oxypeucedanin hydrate. All these marker substances in LC09 were chosen according to Pharmacopoeia of the People’s Republic of China. The substances were calycosin-7-glucoside and astragaloside for Astragalus membranaceus, hydroxyl safflower yellow pigment A and Kaempferide for flowers carthami, oxypeucedanin hydrate and imperatorin for radix angelicae. There are no marker substances for Geranium wilfordii found in Pharmacopoeia of the People’s Republic of China, and content of lithospermum is very low, so we did not establish fingerprints for lithospermum and Geranium wilfordii.
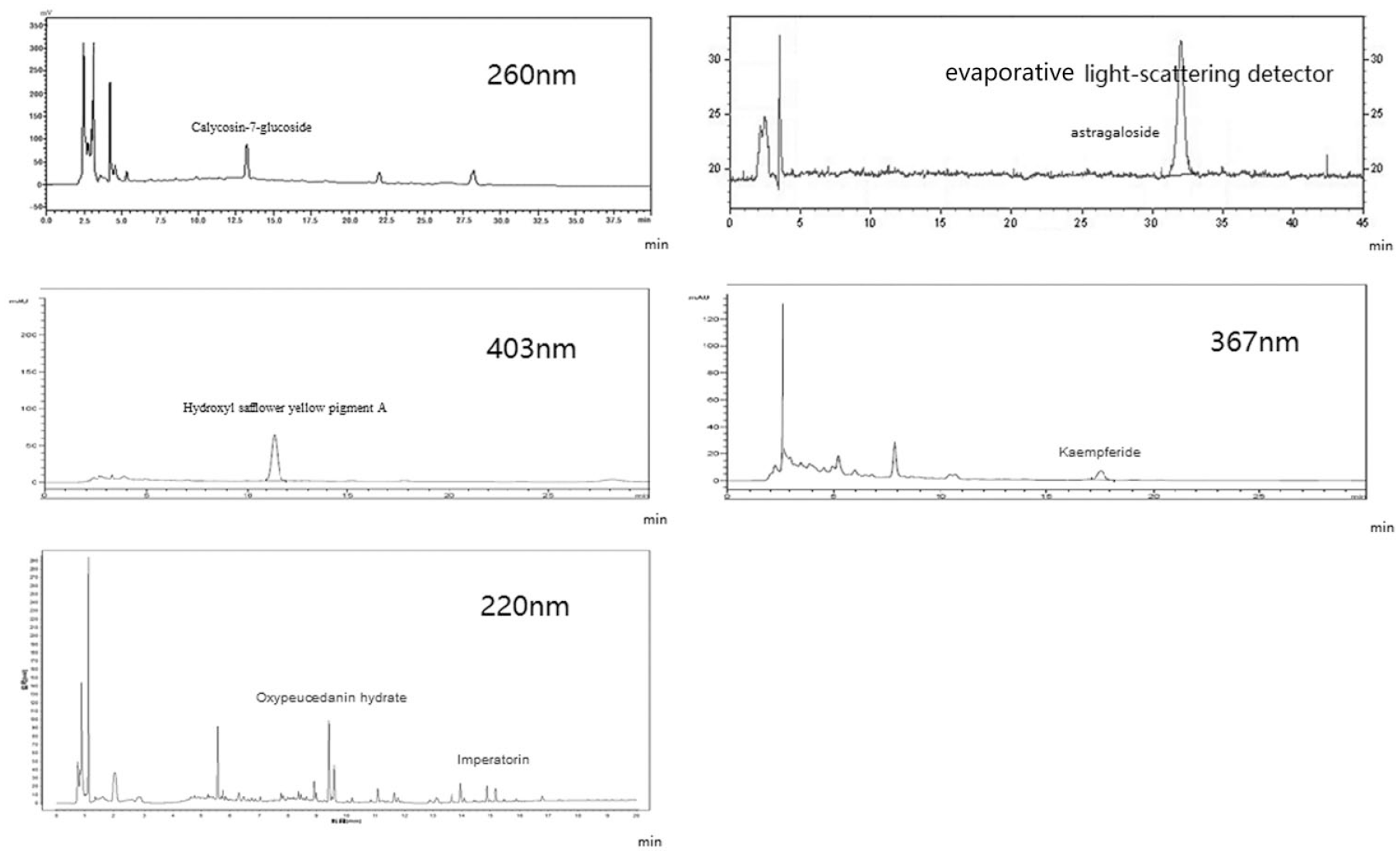
High-performance liquid chromatography/photo diode array detection of LC09.
Calculation
Sample size was calculated according to HFS effectiveness rate (=effect/total patients of one group). Effect was defined as NCI grade decreasing by at least one grade. In earlier studies, the HFS effectiveness rate in the herbal group was about 80% to 90%,20-22 and in our earlier study, LC09’s pain alleviation rate was 88.06%. 15 Because in this trial LC09 is made into granules, and granules may influence dissolution rate, we estimated an effective rate of 80% in the treatment group. For the control group, we used low-dose herbs plus urea cream, and because these articles all have preventive research for HFS, we estimated an effective rate of 50% according our clinical observation. We set 2-side α = 0.05 and β = 0.2. The equation is NA = NB = (PA(1 − PA) + PB(1 − PB))((Z1-α + Z1-β)/(PA − PB − δ)) 2 . We calculated a requirement for 78 patients per group allowing a dropout rate of 20% for 156 patients in total. There were 6 patients in one block and 26 blocks in total. For each block, there are 3 treatment patients and 3 control patients. The data were analyzed with SPSS 20.0 software (SPSS Inc). All data are described using mean ± standard difference or median ± quartile range. Laboratory index (includes age, temperature, pressure, body mass index, gender, blood routine examination, liver and kidney function, coagulation function, and tumor marker) was analyzed using independent-samples t test, χ2 test, or Wilcoxon rank sum test. NRS pain scores, NCI grade, IADL, and DLQI at the end of the study were compared between the treatment group and control group using the Wilcoxon rank sum test or independent-samples t test. HFS effectiveness rate, NRS alleviated rate, chemotherapy completion rate, and incidence of adverse reactions were analyzed using χ2 test or Fisher’s exact test. ANCOVA (analysis of covariance) was used to assess whether treatment and control groups significantly differed on variables assessed at the end of the study using baseline as covariate. Two-sided P value α = .05 was considered statistically significant.
Results
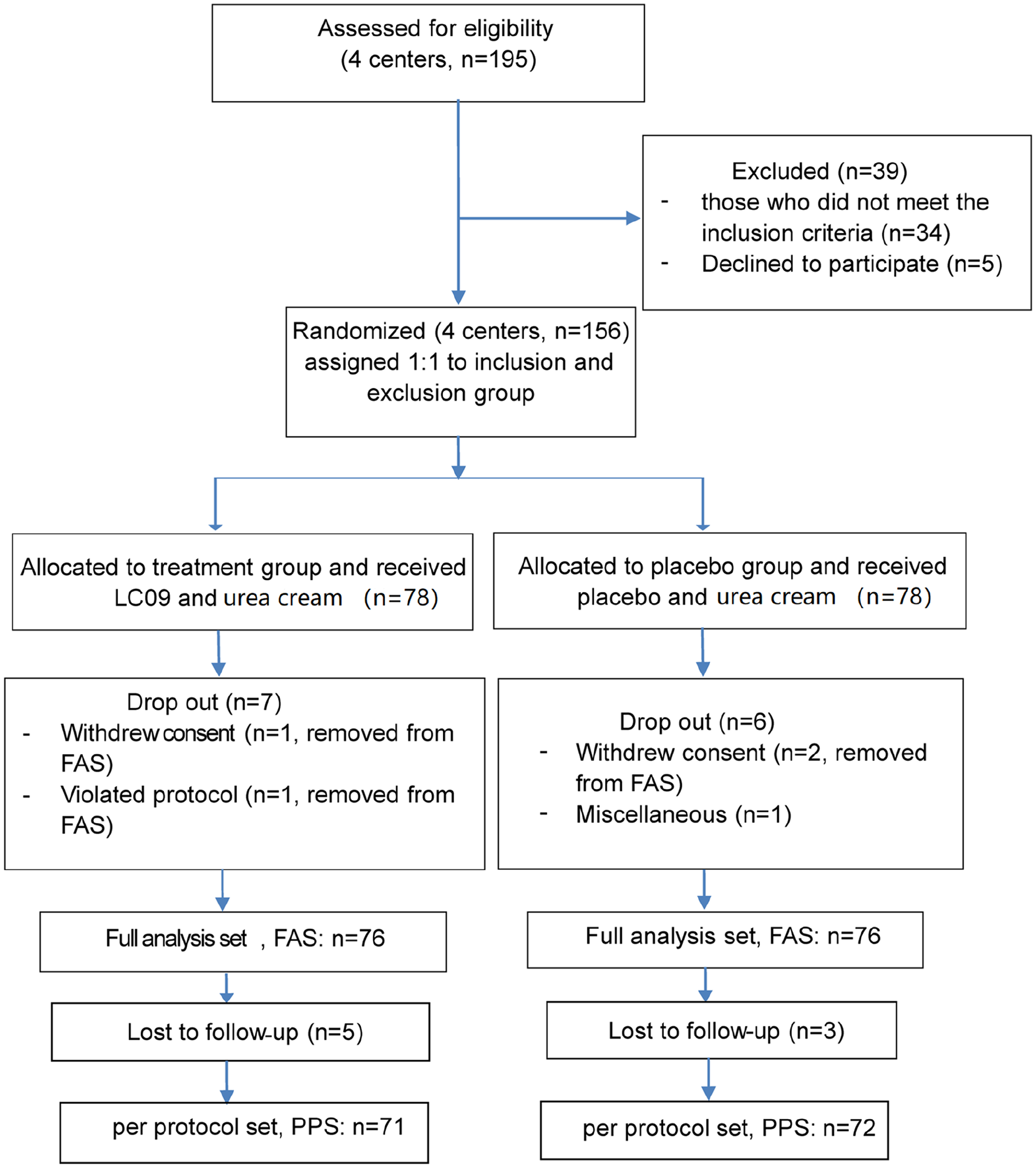
All the patients were from the clinics or wards of 4 different hospitals, including China-Japan Friendship Hospital (66 patients), Cancer Hospital of CAMS (30 patients), Peking University Cancer Hospital (30 patients), and Beijing Chinese Medicine Hospital (30 patients). The study was started after registration and lasted for about 2 years. As shown in Figure 2, the dropout rate (= dropout patients/78) in 2 groups was <15% (P > .05). All patients were followed-up at 1 month and 3 months after completing the trial; no adverse reactions were observed in the 2 groups, except for skin changing color to light brown, which was observed in both groups. Skin discoloration disappeared within 1 week and it did not have any influence on patients.
Inclusion and exclusion criteria.
At baseline, there were no differences between control group and treatment group, except for heart rate (P = .015). Moreover, qualitative analysis revealed no differences in hemoglobin, red blood cell count, white blood cell count, alanine aminotransferase, aspartate aminotransferase, urea, creatinine, platelet, activated partial thromboplastin time, CEA, and CA153 between the control group and treatment group. Between the 2 groups, there were no statistical differences for the chemotherapy cycles that patients had finished (P = .811). In addition, there were no significant differences between 2 groups in NCI grade and NRS pain scores (Table 3).
Baseline Data.

Abbreviations: SD, standard difference; QR, quartile range; FAS, full analysis set; SP, systolic pressure; DP, diastolic pressure.
Wilcoxon rank sum test.
Chi-square test.
Student’s t test.
After treatment, significant differences were observed in HFS effectiveness rate and NCI grade between the 2 groups (P [NCI grade] = .003, P [HFS effective rate] = .002; Figures 3 and 4); HFS effectiveness rates in the treatment group and control group were, respectively, 70.42% and 44.44% (odds ratio = 2.98, 95% confidence interval = 1.49-5.93). NRS pain scores and pain alleviation rates also significantly differed (P [NRS pain scores] <.001, P [pain alleviation rate] <.001). Pain alleviation rates in the treatment group and control group were 81.91% and 47.30%, respectively (odds ratio = 4.99, 95% confidence interval = 2.34-10.65). We also compared NCI grade between the 30% of patients who did not respond to LC09 and the 70.42% of patients who were effectively treated. There was no significant difference between them (P = .402), but rank mean of patients with no effectiveness (rank mean = 39.17) was higher than that of effective patients (rank mean = 34.67). Besides, grade III HFS accounts for 57.1% in patients with no effectiveness, compared with 42.0% of effective patients (Table 4).
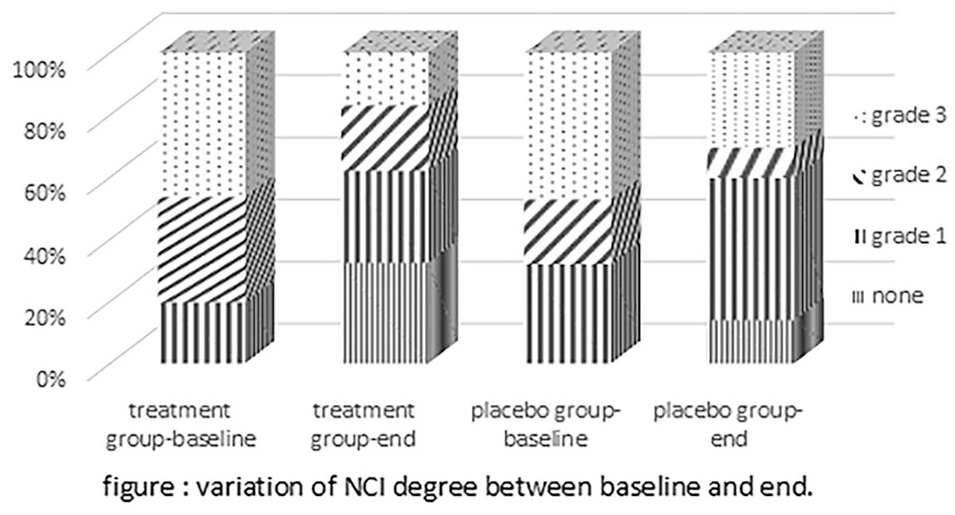
Proportion of 3 NCI (National Cancer Institute) grades at baseline (week 0) and after treatment (2 cycles).
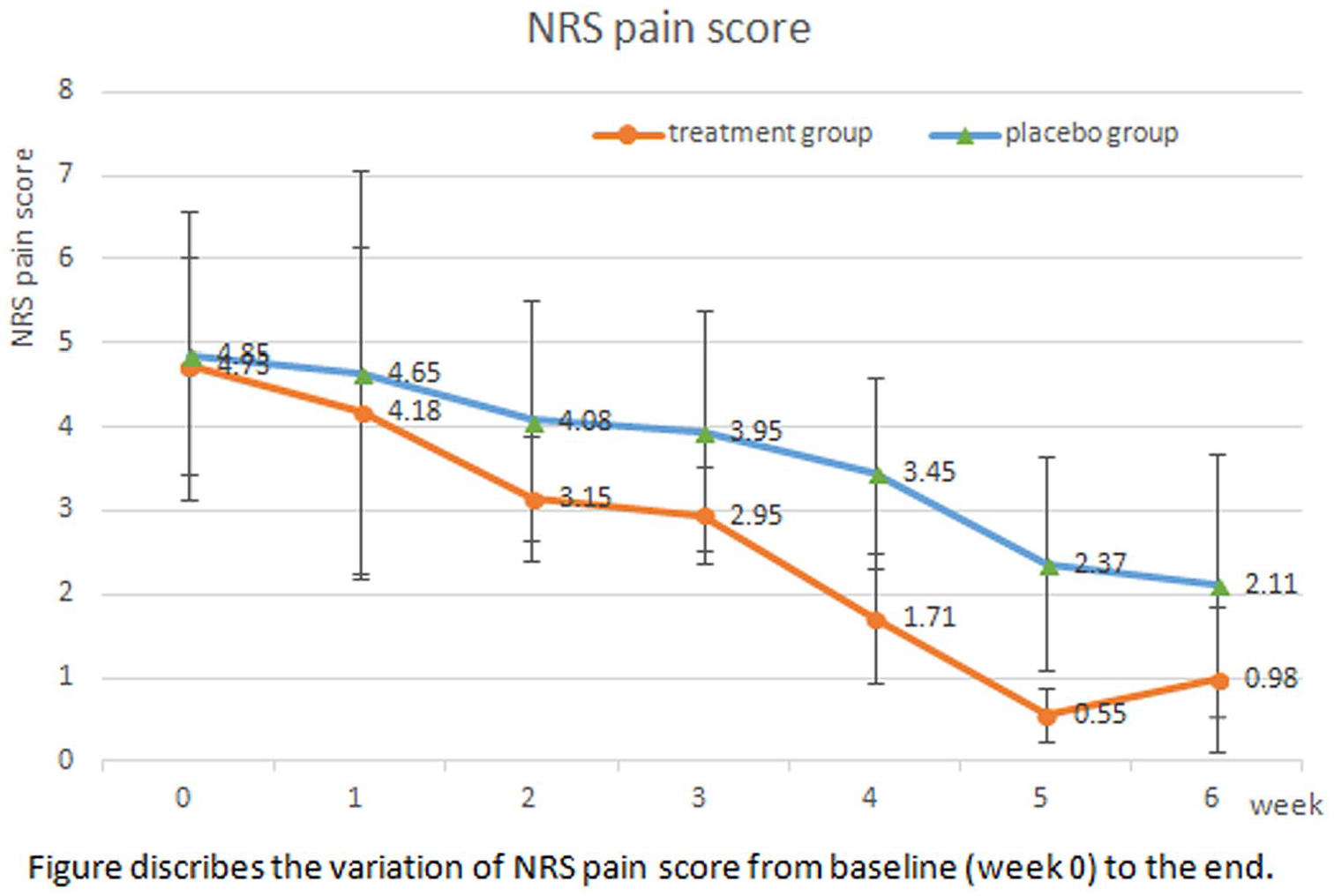
Variation of NRS (Numerical Rating Scale) pain score at baseline (week 0) and after treatment (2 cycles).
Main Indices.

Abbreviations: PPS, per-protocol set; OR, odds ratio; CI, confidence interval; NCIa, National Cancer Institute; NRSb, numeric rating scale; HER, NCIc effective rate (= effective patients/all patients of one group); Effective patients, NCI grade decrease for grade one or more; PARd, pain alleviation rate (= pain alleviated patients/all patients of one group); pain alleviated patient: NRS pain scores increase for one or more grade (see Figure 4).
Furthermore, after treatment, there were no significant differences in DLQI and IADL scores between 2 groups (P > .05). In addition, compared with the control, LC09 and control were both able to improve DLQI and IADL score; however, a higher effect was observed when using LC09 (P = .0149). Although IADL score was significantly improved in treatment group, there was no evidence to support that LC09 was more effective than control. Chemotherapy completion rate in the treatment group (62.86%) was significantly higher compared with control group (40.28%; P = .0021; Table 5).
Secondary Indices.
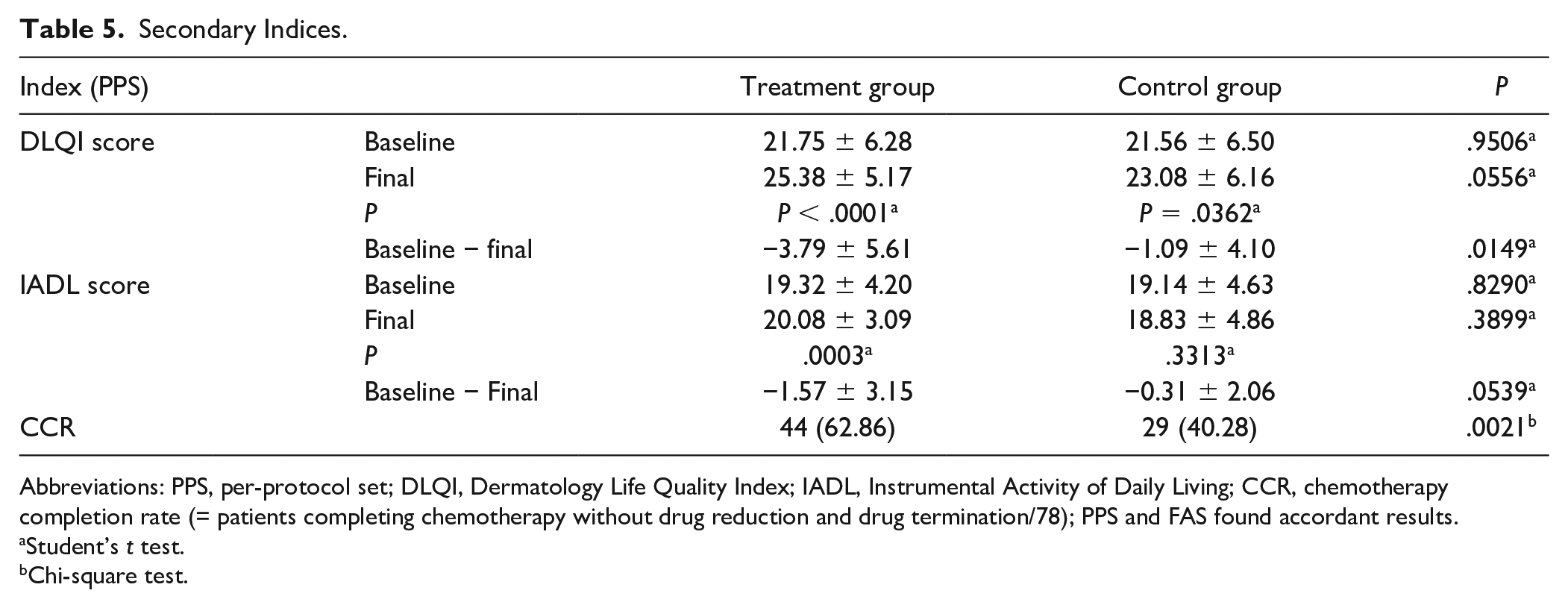
Abbreviations: PPS, per-protocol set; DLQI, Dermatology Life Quality Index; IADL, Instrumental Activity of Daily Living; CCR, chemotherapy completion rate (= patients completing chemotherapy without drug reduction and drug termination/78); PPS and FAS found accordant results.
Student’s t test.
Chi-square test.
Discussion
Our study suggested that LC09 is an effective and safe approach that can decrease HFS-associated pain and increase the chemotherapy completion rate. We found no adverse reaction during the trial and at 3 months after the trial completion. However, LC09 was not effective in 30% of patients in the treatment group, which may be due to the following reasons: (1) this trial was conducted at the same time as chemotherapy; chemotherapeutic drugs may induce adverse reaction and affect skin on the hands. (2) In TCM, one same disease may require different TCM for different syndrome type; LC09 may be effective for one or more different syndrome types, which need to be further investigated. (3) Granular formulation was used as intervening measure; however, since our method was based on using hot, but not boiling water, it is possible that some components were not completely dissolved. This may lead to the effectiveness rate being less than we evaluated in sample size calculation. (4) NCI criteria included only 3 grades, leading to poor sensitivity. (5) Content of lithospermum in the granular formulation as dissolved very low, and this may influence the effect. (6) Although there was no statistical difference in NCI grade between patients who did not respond to LC09 and effective patients, different rank mean and proportion of severe HFS between them reflect that the curative effectiveness of LC09 is limited in patients with severe HFS. This may contribute to the reason why about 30% patients did not respond to LC09 to some extent. In addition, we found that 44.4% of patients responded to the control therapy, which is in line with what we evaluated. This illustrates that (1) the control granules contained low-dose herbs and they nearly have no effect as we expected. (2) Patients from both groups were given urea ointment cream, which contributes nearly half the effect to both groups. (3) HFS is chemotherapy-related condition; patients take capecitabine for 2 weeks and then they pause for 1 week; HFS can also be healed by not using capecitabine. In our trial, all patients in the 2 groups are out after the second cycle of treatment, so we decreased the influence of self-healing between 2 groups. (4) The effectiveness in the control group did not reach 50% as in a previous study, 20 which might be because they used the pyridoxine in the control group, which is different from our research.
The characteristics of this trial are the following: (1) granular formulation was used to replace water decoction so as to make treatment convenient, to improve patients’ acceptance, and to identify whether LC09 was still effective in a different form. (2) Control was made of 5% low-dose herbs that are not effective for HFS. (3) The aim was to treat patients who were already suffering from HFS and not to prevent HFS. (4) Symptom diaries were used to make results more accurate.
This study has some limitations: (1) by the fifth week, pain was significantly alleviated with minimal NRS pain scores. However, after the fifth week, NRS pain scores started increasing in the treatment group. Since there were 2 treatment cycles, with the longest one lasting for 6 weeks, it is not possible to conclude whether the observed increase in the sixth week was accidental or related to drug resistance. In our next study, we should prolong intervention time to ascertain LC09’s long-term efficacy after 2 cycles. (2) In this trial, we excluded patients at early disease stages and with severe visceral complications; thus, the effect of LC09 remains unknown for these patients and should be addressed by further studies. (3) DLQI and IADL scales were used to evaluate HFS-associated quality of life, which provided no strong evidence that LC09 had any effect on quality of life. (4) The content of lithospermum in the granule formulation is not satisfactory, and we need more research to improve its content. Nonetheless, the DLQI score in the treatment group improved more than in the control group after intervention, which may because: (1) cancer affects quality of life more than HFS; (2) although LC09 can alleviate HFS, it may not improve the quality of life; and (3) DLQI and IDAL cannot precisely evaluate HFS since they are both universal scales used for all kinds of skin diseases, and thus lack pertinence. In recent years, some specialized scales have appeared, such as HFS-14 scale, 23 HF-Quality of Life scale, 24 and HAMSIQ (Hand-Foot and Mucositis Symptom and Impact Questionnaire) scale, 25 which are more sensitive to HFS. However, there is no Chinese version tested in Chinese patients; thus, they still cannot be used in Chinese clinical trials.
In conclusion, LC09 can alleviate pain and significantly decrease NCI grade. Nevertheless, we found no strong evidence on its effect on the quality of life, which needs to be addressed by further research using specific scales.
Supplemental Material
supplement-EDITS – Supplemental material for Effect of Chinese Herbal Compound LC09 on Patients With Capecitabine-Associated Hand-Foot Syndrome: A Randomized, Double-Blind, and Parallel-Controlled Trial
Supplemental material, supplement-EDITS for Effect of Chinese Herbal Compound LC09 on Patients With Capecitabine-Associated Hand-Foot Syndrome: A Randomized, Double-Blind, and Parallel-Controlled Trial by Ran Yu, Xuefeng Wu, Liqun Jia and Yanni Lou in Integrative Cancer Therapies
Footnotes
Acknowledgements
The authors thank Sun H and He TT of Peking University Cancer Hospital; Wang JY of Cancer Hospital of CAMS; and Yang GW and Cheng PY of Beijing Chinese Medicine Hospital for participating and collecting data in this study. Besides, we also thank Cheng ZQ, Li LY, Li Y, Liu M, Qi ZR, and Wan DG of China-Japan Friendship Hospital for recommending patients to join the study. Thanks to Ruihua Sun for providing statistical advice to our study. Thanks to the Center of Data Analysis of China-Japan Friendship Hospital for conducting the statistical analysis. Finally, thanks to the pharmaceutical factory Beijing Tcmages Pharmaceutical Co Ltd and Zhiqiang Zhang for providing quality control of LC09 and conducting HPLC.
Author Contributions
Jia LQ and Lou YN designed the trial. Yu R and Wu XF performed the trial, which includes recruiting patients, following patients, and organizing the data. Yu R mainly wrote the text. Statistical analysis was carried out by Statistical Analysis Center for Clinical Research of China-Japan Friendship Hospital.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by National Key Technology Support Program (Number: 2015BAI04B07).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.