
Abstract
Keywords
Introduction
Complete surgical resection with curative intent is the most effective treatment for localized non–small cell lung cancer (NSCLC). 1 Hospital mortality, in Japan, in patients who undergo lung resection is less than 1%, and most patients have no problems with activities of daily living following hospital discharge. 2 Regarding exercise capacity after surgery, the maximum oxygen uptake (VO2 max) declines by 19% to 28% during the 14 days after surgery.3,4 However, most patients have a short postoperative stay, and the magnitude of impairment in functional exercise capacity at discharge is unclear.
Functional exercise capacity is important in NSCLC patients, because it is a strong independent predictor of survival that may complement traditional markers of prognosis to improve risk stratification. 5 Assessment of functional exercise capacity during the early period after lung resection would permit the detection of significant impairment, and early intervention aimed at ameliorating this impairment. Several studies using the 6-minute walk test (6MWT) showed that 6-minute walk distance (6MWD) decreased significantly when measured within 14 days after surgery.6,7 However, the limitations of these studies include small sample size (n = 28 patients following thoracoscopic surgery) 6 and heterogeneity (including patient with metastatic tumors and those with nonmalignant tumors). 7 Furthermore, peripheral muscle force is strongly related to 6MWD in chronic obstructive pulmonary disease (COPD),8,9 as well as important in exercise capacity of patients after lung resection in lung cancer, 10 but it has not been evaluated in these studies. Participants in the previous study 10 were stable patients within 1 year following surgery. In the early postoperative period, factors such as preoperative pulmonary function, surgical procedure, and postoperative progress may also affect the magnitude of impairment in exercise capacity; however, such data are lacking.
The aims of this study were to identify the following: (1) the magnitude of decline in 6MWD during the early period after surgery and (2) associations between the changes in 6MWD and factors such as preoperative peripheral muscle force and pulmonary function, surgical procedure, and postoperative progress in patients following surgical resection for NSCLC.
Methods
Study Population
This was a prospective observational study. Consecutive patients with preoperative clinical stage I to IIIA NSCLC who underwent lung resection between April 1, 2011, and March 31, 2015, at Nagasaki University Hospital (Nagasaki, Japan) were enrolled. Patients in whom functional exercise capacity and skeletal muscle strength tests were performed pre- and postoperation as standard assessment were potentially eligible for the study. Exclusion criteria were musculoskeletal and neurological disorders, or cognitive impairment, and severe postoperative complications (POCs, Clavien-Dindo ≥grade 3B) 11 affecting the performance of exercise tests. In addition, patients who underwent a pneumonectomy or had a history of thoracic surgery were excluded from the study, because in our hospital, the postoperative care is different for such patients.
The study was approved by the Human Ethics Review Committee of Nagasaki University Graduate School of Biomedical Sciences (Approval Number 12092420-2). All participants gave written informed consent.
Baseline Characteristics
We collected data on clinical stage of cancer, comorbidity, performance status (Eastern Cooperative Oncology Group Performance Status) 12 and nutrition status; pulmonary function (forced expiratory volume in 1 second [FEV1], forced vital capacity [FVC], FEV1/FVC, vital capacity [VC], and diffusing capacity of the lung for carbon monoxide [DLCO]) was measured approximately 1 month prior to surgery.
Pulmonary function tests were performed using a spirometer (CHSTAC-8900; Chest Corporation, Tokyo, Japan) in accordance with international guideline. 13 The predicted FVC and FEV1 were calculated from equations developed in healthy nonsmoking Japanese. 14
The preoperative nutritional status was evaluated using the CONUT (Controlling Nutritional Status) score. 15 The score is derived from serum albumin concentration, total blood cholesterol level, and total peripheral lymphocyte count (Table 1).
Definition of CONUT.

Abbreviations: Alb, serum albumin; CONUT, Controlling Nutritional Status; T-cho, total cholesterol; TLC, total lymphocyte count.
Measurements
The following tests were carried out within 2 days prior to surgery and on day 7 postoperatively. Four physiotherapists (MO, MH, HN, and RK) were involved in data collection.
Functional Exercise Capacity
The 6MWT was used to assess functional exercise capacity with the main test outcome being 6MWD. The test was performed according to published guidelines, 16 and the better of 2 attempts was recorded. A 30-m corridor was used with patients instructed to walk as far as possible in the 6 minutes. Standardized encouragement was given at the end of every minute. Oxygen saturation and pulse rate were monitored continuously throughout the test (PULSOX-300; KONICA MINOLTA, Japan). The modified Borg scale 17 was used to quantify the level of dyspnea and leg fatigue immediately after the test.
Skeletal Muscle Strength
Handgrip force (HF) and quadriceps force (QF) were measured as indices of skeletal muscle strength. The HF was assessed using a dynamometer (T.K.K.5401; Takei-Kiki-Kogyou Corporation, Niigata, Japan). Patients were required to squeeze the dynamometer with maximum effort for at least 5 seconds. Following 1 practice attempt, HF was tested twice with a minimum of 60 seconds rest between each attempt. The highest value of 2 attempts was recorded (kg) on both hands. HF was measured on both limbs to account for the potential influence of pain on the operative side following surgery. During the test, patients were standing upright with their feet hip-width apart and with elbow fully extended, and holding the hand dynamometer, with the wrist in neutral position and index finger flexed at 90°.18,19
Quadriceps force was evaluated as the peak force developed by the dominant leg during a maximal isometric knee extension maneuver in the sitting position using a handheld dynamometer with a fixing belt (µ-Tas F-1; Anima Corporation, Tokyo, Japan) in accordance with a standard protocol. 20 The highest value of at least 2 maneuvers was recorded and expressed in kilograms feet (kgf).
Surgical and Perioperative Management
Patients were selected for thoracoscopic surgery or thoracotomy on the basis of the results of chest radiographic studies, bronchoscopy, the patient’s general condition (performance status), and comorbidities (eg, presence of interstitial lung disease). An epidural or continuous intravenous analgesia was used to manage postoperative incisional pain until removal of the chest drain after which oral analgesics were taken. The definition used for thoracotomy in this study was an incision ≥6 cm and/or use of a rib retractor. We defined POCs as complications that occurred during the postoperative hospital stay. The POCs were diagnosed by a surgeon and/or a radiologist, and we identified these POCs from the medical records according to the Clavien-Dindo classification. 11 The Clavien-Dindo classification categorizes POCs into 5 major groups according to the intervention required for patient care: grade 1, requiring no pharmacological intervention other than antiemetics, antipyretics, analgesics, diuretics, electrolytes, and physiotherapy; grade 2, requiring pharmacological intervention with medications other than those allowed for grade 1 complications; grade 3, requiring further intervention with (3B) or without (3A) general anesthesia; grade 4, life-threatening complications and those requiring intensive care unit management; and grade 5, death of the patient. 11
Postoperative management included physiotherapy comprising early ambulation and airway clearance techniques (as indicated). Physiotherapy was commenced on the first postoperative day and continued until the day prior to discharge. The schedule of postoperative physiotherapy was as follows: postoperative day 1, sit on the edge of the bed, stand, and walk along the corridor (70-200 m, if possible); day 2 to 3, walk 200 to 400 m; day 3 to 6, climb 1 to 3 floors of stairs plus upper and lower limb resistance training; day 7, measurements of muscle strength and functional exercise capacity, and advice about unsupervised exercise training and activities of daily living for postdischarge. No supervised exercise training was provided after the seventh postoperative day.
Statistical Analysis
The Kolmogorov-Smirnov test was used to examine the distribution of data. Variables were expressed as the median and interquartile range or as mean ± standard deviation, absolute number and percentage, or 95% confidence intervals.
Comparisons between pre- and postoperative 6MWD and skeletal muscle strength were made using paired t tests. Multiple linear regression analysis was used to determine the associations between change in 6MWD following surgery with preoperative skeletal muscle strength and pulmonary function, surgical procedure, and postoperative progress. A multiple linear regression analysis, adjusted for preoperative 6MWD, was first performed to identify any potential predictor variables. Variables with a P value <.2 and those considered to be clinically relevant were then included in the multivariate analysis to determine any independent predictors. When multicollinearity was present in the model, highly related variables were identified and only the variable showing the highest univariate relationship with the dependent variable was included in the model.
The level of significance was set at .05 for all statistical tests. Analyses were performed using a statistical software package (IBM SPSS Statistics version 23.0, IBM, Chicago, IL).
Results
Patient Characteristics
Four hundred seventy-two consecutive patients were screened for eligibility of whom 297 (63%) patients were recruited to the study (Figure 1). Of these, 56 (19%) patients refused to complete the 6MWT following surgery due to symptoms such as postoperative pain and fatigue, and presence of chest drainage (Supplementary File 1, available online). Data from 218 (73%) patients were included in the analysis. Table 2 and Supplementary File 2 (available online) show the characteristics of the 218 patients. Forty-nine patients developed POCs: 14 cases of prolonged air leakage for 4 days, 13 cases of atrial fibrillation, 7 cases of chylothorax, 4 of delirium, 3 cases of pneumonia, 3 cases of atelectasis, 2 cases of hemothorax, 2 cases of recurrent nerve paralysis, 1 case of pyothorax, and 1 case of acute exacerbation of COPD. On average, the chest drains and epidural catheters were removed on postoperative day 3. Most patients (65%) ambulated on the first postoperative day (Table 2). Two hundred six patients (95% of the sample) achieved a walking distance of 200 m by postoperative day 4. After surgery, only one patient performed the 6MWT with the chest drain in situ, with the physiotherapist carrying the drainage tube.

Patient flow diagram.
Baseline Characteristics of the Patients (N = 218).

Abbreviations: CONUT, Controlling Nutritional Status; DLCO, diffusing capacity of the lung carbon monoxide; ECOG-PS, Eastern Cooperative Oncology Group Performance Status; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; IQR, interquartile range; VC, vital capacity.
Comparison of 6MWD and Skeletal Muscle Strength Before and After Surgery
Pre- and postoperative 6MWD and skeletal muscle strength are shown in Table 3. 6MWD was decreased, and dyspnea in post-6MWT was significantly increased during the early postoperative period. Skeletal muscle strength was decreased.
Functional Exercise Capacity and Skeletal Muscle Strength.

Abbreviations: 6MWD, 6-minute walk distance; 6MWT, 6-minute walk test; CI, confidence interval; PR, pulse rate; SpO2, percutaneous oxygen saturation.
Relationships Between Postoperative Deterioration in 6MWD and Pre- and Postoperative Factors
First, we explored potential predictors using multiple linear regression adjusted for preoperative 6MWD. As a result, potential predictor variables were age, gender, FEV1, FVC, VC, DLCO, HF, QF, surgical procedure, the duration of chest tube drainage, and presence of POCs (Supplementary File 3, available online). For the following variables, preoperative pulmonary function (FEV1, FVC, VC, DLCO) and muscle strength (HF, QF), we detected the presence of multicollinearity so the variables with the highest prediction accuracy in the multiple linear regression were selected. The duration of chest tube drainage (P < .001), presence of POCs (P = .014), VC (P = .001), and QF (P = .034) before surgery were significant predictors. However, age and gender, and variables related to surgery were not significant contributors to the outcome. Details of the result above analyses are given in Table 4.
Results of Multiple Linear Regression Analysis.
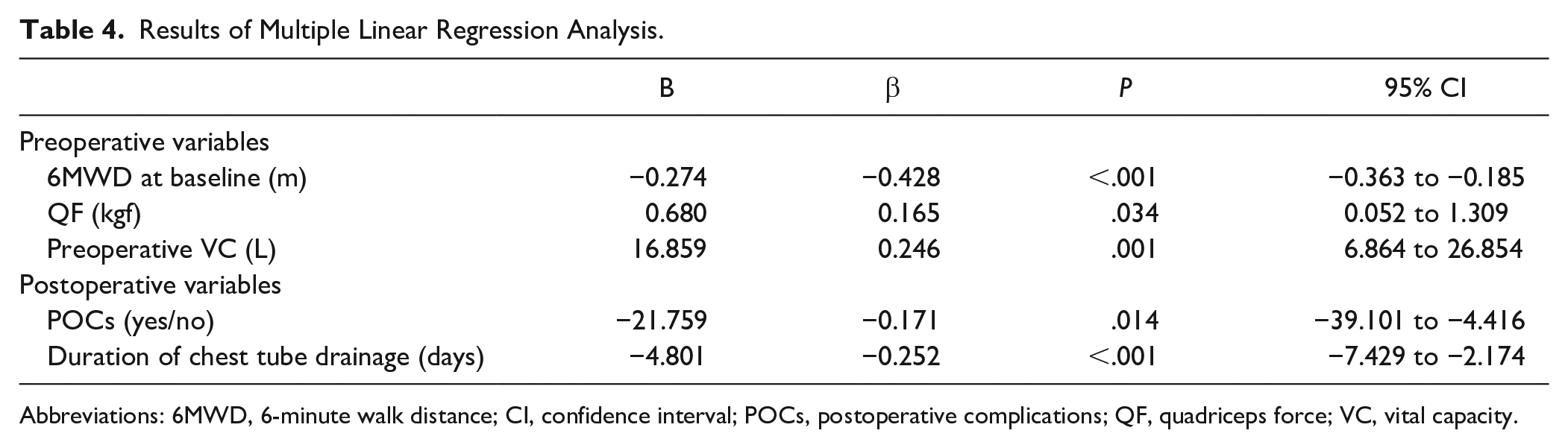
Abbreviations: 6MWD, 6-minute walk distance; CI, confidence interval; POCs, postoperative complications; QF, quadriceps force; VC, vital capacity.
Discussion
We found that (1) the impairment in functional exercise capacity measured as 6MWD during the early postoperative period significantly declined (45 m, 9%); and (2) the preoperative QF and VC, duration of chest tube drainage, and presence of POCs were independent predictors of the decline in 6MWD. To our knowledge, this is the first study to investigate impairment of functional exercise capacity in the early postoperative period following lung resection for NSCLC in a large sample and to examine predictor variables.
We chose to assess functional exercise capacity using the 6MWT. Previous studies3,4 have performed a cardiopulmonary exercise test (CPET) as a postoperative exercise capacity test. Cavalheri et al 21 reported that a CPET is a more maximal test than the 6MWT in patients with lung cancer; however, the 6MWT is more suitable in the early postoperative period because some patients would not tolerate the CPET due to symptom burden (ie, incisional pain, fatigue, and dyspnea). Seventy-three percent of our sample were able to perform the 6MWT in the early postoperative period. However, 19% of patients, especially elderly patients, refused to complete the 6MWT because of fatigue and dyspnea, incisional pain related to thoracotomy, and presence of a chest drain.
In our study, 6MWD had declined by 45 m when measured at 7 days after surgery. Arbane et al 22 reported that 6MWD decreased about 130 m at 5 postoperative days, and a decline was almost 3-fold greater than we observed. However, our finding is quite consistent with reports of Nomori et al 6 and Brocki et al, 7 which assessed in the early postoperative period and reported the magnitude of decline in 6MWD (35 m, 47 m). In Arbane’s study, we speculate that their patients’ effort during the 6MWT was submaximal (mean Borg’s dyspnea rating of only 1.4, peak heart rate 101 bpm). Moreover, Granger et al 23 have reported the minimal important difference for the 6MWD in patients with lung cancer to be 22 to 42 m. Because the participants in Granger’s study were lung cancer patients assessed 10 weeks after therapies (chemotherapy, radiotherapy, or surgery), it could not be determined whether these treatments influenced 6MWD. However, we also cannot completely assert that the decline of 45 m in postoperative early period is not a problem, because none of previous studies have reported relationship between the magnitude of impairment of postoperative 6MWD and long-term factors such as exercise capacity, health-related quality of life, and survival. If impairment of postoperative functional capacity and long-term factors are related, it is important to detect the exercise limitation at an early stage following surgery so that training can be initiated, given the evidence for this intervention.24,25
The findings of the multiple linear regression analysis identified 4 variables that were independent predictors for the decline in 6MWD, namely, preoperative QF, VC, duration of chest tube drainage, and development of POCs. Burtin et al 10 recruited patients within 1 year after surgery for lung cancer and, consistent with our findings, reported that QF was a factor determining their exercise capacity. The importance of lower limb muscle strength as a contributor to exercise capacity in patients who undergo lung resection is a consistent finding, 10 and it has also been identified as an important contributor to exercise limitation, in respiratory diseases such as COPD.8,9
We found that the higher the preoperative VC, the lower the magnitude of postoperative impairment in exercise capacity. Several previous studies have shown a relationship between postoperative pulmonary function and exercise capacity.3,4,10,26 In our study, preoperative VC was more related to postoperative exercise capacity than FEV1 or DLCO. Probably, the relationship between pulmonary function and exercise capacity such as postoperative VC, FEV1, or DLCO differs depending on the timing of evaluation. Although ventilatory limitation is caused by the impairment of chest wall movement in the early postoperative period, this recovers by approximately 1 month after surgery. 27 Therefore, we consider the VC involved in ventilation contributed to the decline in exercise capacity in the early postoperative period.
The longer the duration of chest tube drainage the greater decline in postoperative 6MWD. Prolonged chest tube drainage contributes to dysfunction as a result of physical inactivity arising from the associated pain and discomfort. Early removal of the drainage tube is desirable in order to reduce pain and improve ventilatory function in the early postoperative phase. 28
The development of POCs limit physical activity due to factors such as an unstable medical condition leading to enforced rest and the symptoms associated with the POCs. Furthermore, POCs such as pneumonia and atelectasis worsen postoperative pulmonary function and also give rise to catabolism in the peripheral muscle by prolonging inflammation. 29
Age, gender, and time to first ambulation are also potential predictors of postoperative 6MWD. Age and gender have been reported as predictors in a previous study 30 of thoracic surgery patients. In that study, there was a wide age range (17-90 years), in contrast to our study (63-72 years), and this is likely to explain why age was not a predictor in the present study. Regarding gender, 6MWD in a previous study showed a greater postoperative decline in females, 30 although no reason given. Delayed time to first ambulation decreases physical activity and may affect 6MWD. However, the assessment of physical activity was outside the scope of this study.
Interestingly, our results showed that intraoperative factors such as the type of surgery and amount of lung resected were not significantly associated with the decline in 6MWD. Some previous studies have reported the determinants of 6MWD in patients undergoing thoracic surgery.30,31 Moreover, Nomori et al reported the surgical procedure, for example, posterolateral or anterolateral thoracotomy, did contribute to the decline in postoperative exercise capacity. 6 In our sample, half of the patients received complete video-assisted thoracoscopic surgery, or small incisions even if thoracotomy. As a result, the muscle incision during surgery was small and the effects may not have been different. In addition, we excluded those who underwent pneumonectomy or had a history of thoracic surgery, as surgery in such patients is more extensive. Some previous studies have reported the impairment in exercise capacity, as measured by CPET, following lung resection was not related to the amount of lung resected consistent with our finding.32,33 Importantly, irrespective of the surgical procedure and extent of lung volume resected, a similar magnitude of dysfunction in exercise capacity occurs immediately after surgery.
The main limitation of this study is that it was carried out in 1 center only. Furthermore, we were only able to recruit 63% of the potential sample because of comorbidities and difficulties in undertaking preoperative assessments given most patients were hospitalized for only 1 day prior to surgery, and this day was taken up with multiple assessments and interventions. As we excluded those with stage IV, pneumonectomy, and history of thoracic surgery, our results are limited to patients undergoing standard surgery for NSCLC in primary stage.
Second, we did not assess pulmonary function following surgery or levels of physical activity. In particular, daily activity level may affect postoperative 6MWD and should be evaluated in future studies.
The strengths of our study include the sample size, which is larger than previous reports, and the homogeneity of the sample given the participants were managed in accordance with clinical guidelines for surgery in NSCLC. 1 Furthermore, we extend previous studies by identifying factors that are associated with the deterioration in functional exercise capacity following surgery.
Some identified factors include factors to be improved by preoperative rehabilitation. Preoperative exercise training improves preoperative exercise capacity, reduces the risk of POCs, and the duration of chest tube drainage.34,35 It may also have a role in minimizing impairment of exercise capacity after surgery.
Conclusion
We found that functional exercise capacity during the early postoperative period significantly declined, and the deterioration was related to preoperative QF, VC, and postoperative progress such as the duration of chest tube drainage and development of POCs. However, intraoperative factors such as the surgical procedure and extent of lung resected were not related to the decline. Based on our findings, we recommend the routine evaluation of 6MWD before and after surgery regardless of type of surgery to detect the initial decline in exercise capacity. Future research should evaluate whether preoperative training has any impact on postoperative exercise capacity, as well as the influence of early postoperative training in those patients with identified impairments in exercise capacity.
Supplemental Material
Supplementary_File_1._character_of_patients_who_refused – Supplemental material for Factors Influencing Functional Exercise Capacity After Lung Resection for Non–Small Cell Lung Cancer
Supplemental material, Supplementary_File_1._character_of_patients_who_refused for Factors Influencing Functional Exercise Capacity After Lung Resection for Non–Small Cell Lung Cancer by Masato Oikawa, Masatoshi Hanada, Hiroki Nagura, Tomoshi Tsuchiya, Keitaro Matsumoto, Takuro Miyazaki, Terumitsu Sawai, Naoya Yamasaki, Takeshi Nagayasu and Ryo Kozu in Integrative Cancer Therapies
Supplemental Material
Supplementary_File_2._comorbidity – Supplemental material for Factors Influencing Functional Exercise Capacity After Lung Resection for Non–Small Cell Lung Cancer
Supplemental material, Supplementary_File_2._comorbidity for Factors Influencing Functional Exercise Capacity After Lung Resection for Non–Small Cell Lung Cancer by Masato Oikawa, Masatoshi Hanada, Hiroki Nagura, Tomoshi Tsuchiya, Keitaro Matsumoto, Takuro Miyazaki, Terumitsu Sawai, Naoya Yamasaki, Takeshi Nagayasu and Ryo Kozu in Integrative Cancer Therapies
Supplemental Material
Supplementary_File_3._Results_of_multiple_linear_regression_analysis_(adjusted_for_preoperative_6MWD) – Supplemental material for Factors Influencing Functional Exercise Capacity After Lung Resection for Non–Small Cell Lung Cancer
Supplemental material, Supplementary_File_3._Results_of_multiple_linear_regression_analysis_(adjusted_for_preoperative_6MWD) for Factors Influencing Functional Exercise Capacity After Lung Resection for Non–Small Cell Lung Cancer by Masato Oikawa, Masatoshi Hanada, Hiroki Nagura, Tomoshi Tsuchiya, Keitaro Matsumoto, Takuro Miyazaki, Terumitsu Sawai, Naoya Yamasaki, Takeshi Nagayasu and Ryo Kozu in Integrative Cancer Therapies
Footnotes
Acknowledgements
The authors are deeply indebted to the staff and coworkers, especially people who participated in this study. We greatly appreciate Dr Sue Jenkins (School of Physiotherapy and Exercise Science, Curtin University, and Physiotherapy Department, Sir Charles Gairdner Hospital, Perth, Western Australia) for her help with reviewing the manuscript, and also wish to thank Dr Shuntaro Sato (Clinical Research Center, Nagasaki University Hospital) for his statistical advice.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by Grant-in-Aid for Young Scientists (B) (No. 15K16357 to Masato Oikawa) for Science Research from Japan Society for the Promotion of Science.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.