
Abstract
Keywords
Introduction
The incidence of breast cancer has increased at an annual rate of nearly 3% in the past 30 years in China. 1 Since there are no individual cell surface receptors in triple-negative breast cancer (TNBC), conventional endocrine therapy for estrogen receptor, progesterone receptor, and targeted molecular therapy for human epidermal growth factor receptor-2 (HER-2) overexpressing tumors are not suitable for TNBC. Therefore, chemotherapy is the major treatment. However, tumor recurrence often occurs within 1 to 3 years after the treatment. 2 A 5-year follow-up study demonstrated that the distant metastasis rate of TNBC was 33.9%, while for non-TNBC it was 22.4%. 3 Moreover, when recurrence and metastasis occur in TNBC, the median survival time is only 10 to 12 months. 4 Therefore, many breast cancer patients receive complementary therapies during cancer treatment to relieve symptoms, improve quality of life (QoL), and prolong survival time. 5 Around 48% to 80% of North American breast cancer patients received alternative therapies after diagnosis, mainly focusing on herbal extract and vitamin supplements.5,6
In vitro and in vivo studies 7 indicated that high-dose vitamin C suppresses the invasion and metastasis of breast cancer cells via inhibiting epithelial-mesenchymal transition. It could also kill breast cancer cell by inhibiting energy metabolism via NAD depletion, induced by hydrogen peroxide generation. 8 Clinical trials show its safety and high tolerability.9,10 It has been noted that using intravenous vitamin C (IVC) as an adjunct therapy with standard chemotherapy could increase sensitivity to specific antineoplastic drugs and reduce the side effects that often accompany chemotherapies.11,12 Animal studies indicated that IVC also decreased the toxic side effects of cisplatin, Adriamycin, and paclitaxel, which is known to cause off-target oxidative stress.13-15 In addition, IVC can not only reduce chemotherapeutic agents’ related toxicity but also do not adversely influence the anticancer activity of the drugs. 14
Several clinical trials indicated the potential efficacy of IVC, such as improved the performance status or prolongation of time to disease progression or overall survival (OS) time, in ovarian 16 and pancreatic 17 cancers. Its synergy with chemotherapy improves the QoL.18-20 In our previous phase I clinical study, 21 we found that fasting plasma vitamin C levels were significantly correlated with stage of non–small cell lung cancer. Pharmacokinetic profiles were obtained when they received solely IVC and suggested that IVC is safe and well tolerated. The peak concentration of vitamin C was up to 20 mmol/L when the dosage of IVC was given at 1.5 g/kg/day. The average scores for the functioning scale (physical, emotional, cognitive, and social functioning) increased continuously, and the average values for the symptoms decreased gradually, which indicates that QoL is improved when patients receive the above-mentioned treatments. Thus, IVC is a potentially effective adjunctive therapy to reduce toxicity related to chemotherapeutic agents and as a result may also improve QoL of cancer patients.18-20
Intravenous vitamin C is routinely made available to patients in our cancer center, and IVC patients are self-selected and self-financed. The purpose of this study was to retrospectively analyze the effect of IVC plus chemotherapy on tumor response, tumor markers, Karnofsky Performance Status (KPS) score, progression-free survival (PFS) time, and OS time in patients with advanced TNBC.
Methods
Patient Population
Metastatic TNBC patients who underwent treatment at Clifford Hospital between January 1, 2008, and December 1, 2016, were evaluated for participation in this retrospective study. Eligibility criteria were the following: (1) women aged 18 to 65 years; (2) pathologic type was identified as TNBC by histologic diagnosis and immunohistochemistry; (3) patients with breast cancer TNM stage IV as classified according to the American Joint Commission on Cancer, 7th edition; (4) there was at least one measurable lesion; (5) the presence of distant metastases was confirmed by computed tomography (CT), magnetic resonance imaging, bone scan, or ultrasound; (6) no other primary malignant tumors; (7) patients with KPS ≥70; (8) all patients had a normal glucose-6-phosphate dehydrogenase level; (9) all patients had a normal kidney function; (10) treatment protocol: treatment group: gemcitabine and carboplatin (GC regimen) plus IVC; control group: GC regimen alone; (11) estimated survival time of 3 months or more; and (12) full follow-up data.
All patients were informed in advance of possible adverse reactions and precautions to be taken. This study was approved by the Ethics Committee of the Clifford Hospital as a retrospective evaluation of existing clinical data and was conducted according to the principles expressed in the Declaration of Helsinki.
Treatment Protocol
The treatment group received chemotherapy GC regimen plus IVC: gemcitabine 1000 mg/m2 on day 1 and day 8, IV drip; carboplatin area under the curve 5 on day 1 after gemcitabine, 28 consecutive days counting as a cycle. All patients received 2 to 8 cycles according to their conditions. IVC was administered at a dose of 1 g/kg with 900 mmol/L osmotic pressure and 0.5 g/30 minutes infusion speed. The first dose was applied 3 days before chemotherapy, and the second treatment was on day 3, repeated every other day for a total of 25 treatments. The last treatment was applied the same day as that of the second cycle of chemotherapy. We made a paired match of the included patients for the control group, who received the GC regimen alone. The match was done based on the following: ages, menopausal status, and metastatic sites. Ondansetron and/or metoclopramide were used to reduce gastrointestinal reactions. Routine blood examination was conducted during chemotherapy: rhG-CSF injection was given when white blood cell count was <4.0 × 109/L; interleukin-11 was given when platelets were <80 × 109/L.
Follow-up
Pre- and posttreatment evaluation included complete medical history, physical examination, KPS score, complete blood count, tumor markers, enhanced CT scan, and other imaging to record disease. All patients had evaluable lesions. Enhanced CT scans before and after treatments were used to evaluate lesion changes. All scans were assessed by an independent central radiology review. Response measurements were carried out according to RECIST 1.1 (Response Evaluation Criteria in Solid Tumors). All patients were followed-up from the date admitted to Clifford Hospital until March 1, 2017, or death, whichever occurred first.
Response Evaluation
Tumor response was defined as complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD), according to the RECIST 1.1 criteria after 2 cycles of chemotherapy. CR + PR was defined as response rate (RR); CR + PR + SD was defined as clinical benefit rate (CBR). PFS refers to the interval between the initiation of treatment and the first occurrence of progressive disease or death. OS was defined as the period from the date of receiving chemotherapy until the time of death. Tumor markers are molecules occurring in blood that are associated with cancer and whose measurement or identification is useful in patient diagnosis (CEA, CA19-9, CA125, and CA15-3).
Adverse Reactions
Adverse reactions were evaluated using the National Cancer Institute–Common Toxicity Criteria (NCI-CTC 3.0). Oncologists in charge of the patients were responsible for assessing and recording the patient’s adverse reactions daily. A research assistant assisted the researcher in extracting and analyzing the data from the electronic forms.
Statistical Analysis
SPSS20.0 was used for statistical analysis. Incidence was expressed as number and percentage. T test was used for group comparison, and the χ2 test was used for the count data comparison. Rank sum test was used for nonparametric data comparison. Kaplan-Meier analysis and log-rank test were used for PFS and OS for group comparison. P < .05 was considered statistically significant.
Results
Patient Characteristics
A total of 113 TNBC patients received chemotherapy in Clifford Hospital between January 1, 2008, and December 1, 2016. Overall, there were 93 cases that met the eligibility criteria, including 49 cases who received chemotherapy plus IVC and 44 cases who received single chemotherapy. Patients were further matched according to the matching rules mentioned above, and 35 pairs (70 cases) of patients were included in this study. There was no significant difference in baseline characteristics between 2 groups. Every patient received 2 to 8 courses of systemic chemotherapy. The median number courses in which patients received IVC in the treatment group was 4 (0.5-6; every 25 treatments are counted as one course; Table 1).
Patient Characteristics a .
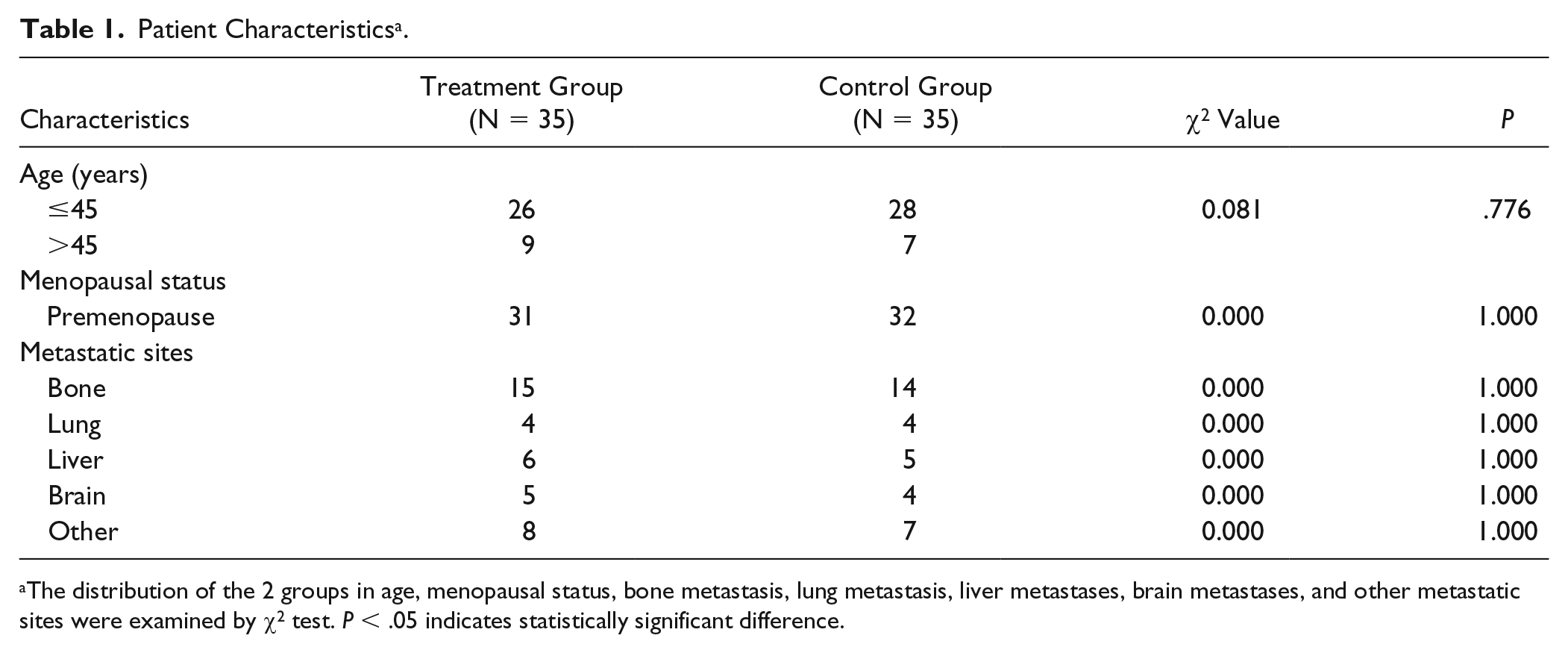
The distribution of the 2 groups in age, menopausal status, bone metastasis, lung metastasis, liver metastases, brain metastases, and other metastatic sites were examined by χ2 test. P < .05 indicates statistically significant difference.
Evaluation of Short-Term Response
There was no significant difference in RR and CBR between the treatment and control groups (Table 2, P > .05). There were 19 premenopausal patients (RR = 47.4%, CBR = 89.5%) and 16 postmenopausal patients (RR = 50.0%, CBR: 81.2%) in the treatment group; there were 17 premenopausal patients (RR = 35.3%, CBR = 94.1%) and 18 postmenopausal patients (RR = 44.4%, CBR = 66.7%) in the control group. In the treatment group, RR was 41.2%, and CBR was 88.2% in patients with the number of metastases >1; while RR was 55.6%, and CBR was 83.3% in patients with the number of metastases ≤1. In the control group, RR was 56.3%, and CBR was 100.0% in patients with metastasis >1; however, RR was 26.3%, and CBR was 63.2% when the metastatic number was ≤1. There was no significant difference between 2 groups (Table 2).
Evaluation of Short-Term Response Effect a .

Abbreviations: RR, response rate; CR, complete response; PR, partial response; CBR, clinical benefit rate; SD, stable disease; PD, progressive disease.
Number of metastatic sites and the effect of premenopause and postmenopause conditions in both groups on the short-term efficacy were examined by the rank sum test. P < .05 indicates statistically significant difference.
In the treatment group, after 2 cycles of treatment, the tumor markers CEA, CA19-9, CA125, and CA15-3 were significantly lower than those before the treatment (Table 3; P < .05). In the control group, there was no significant difference in tumor markers before and after treatments (Table 3; P > .05).
Tumor Markers a .

The changes of tumor markers in the 2 groups were analyzed by t test. P < .05 indicates statistically significant difference.
In the treatment group, KPS scores after 2 cycles of treatment were significantly higher than those before the treatment (87.7 ± 4.9 vs 78 ± 4.1, P < .0001). However, there was no significant difference in KPS scores in the control group before and after the treatment (79.4 ± 5.4 vs 78 ± 4.1, P = .21). The KPS scores after the treatments in the treatment group were significantly higher than those in the control group (P < .0001).
Adverse Reactions
The adverse reactions were mainly digestive tract reactions and bone marrow suppression. The incidence of adverse reactions was significantly lower in the treatment group than in the control group (Table 4, P < .05), suggesting that IVC can significantly decrease the incidence of adverse reactions associated with chemotherapy.
Adverse Reactions a .

Abbreviations: T, treatment; C, control.
The number of adverse reactions in the treatment group was compared with that in the control group. The rank sum test was used. P < .05 indicates statistically significant difference.
Analysis of Survival Time
All patients were followed-up until March 1, 2017. The median follow-up time for the whole group was 22 months (3-40 months). Seventeen patients survived and 18 patients died in the treatment group, while 7 patients survived and 28 patients died in the control group. The median PFS in the treatment group was 7 months (1.5-28.5 months), and the median OS was 27 months (4-40 months). In the control group, the median PFS was 4.5 months (1.5-8 months), and the median OS was 18 months (3-26 months). PFS (Figure 1; P = .002) and OS (Figure 2; P = .002) in the treatment group were significantly longer than those in the control group. The 3-year survival rate in the treatment group was 40%, compared with only 14.3% in the control group. In the treatment group, 14.3% of patients had a survival time >3 years, while none of those in the control group survived >3 years (Table 5).

Kaplan-Meier plots for progression-free survival (PFS). The log-rank test for PFS for the 2 comparisons: active arm versus control arm (hazard ratio = 0.3177; 95% confidence interval = 0.1022-0.3491; P = .0002).

Kaplan-Meier plots for overall survival (OS). The log-rank test for OS for the 2 comparisons: active arm versus control arm (hazard ratio = 0.2542; 95% confidence interval = 0.06408-0.2311; P < .0001).
Survival Analysis of 2 Groups.

Discussion
Patients diagnosed with advanced TNBC had a high risk of recurrence and poor prognosis. Median OS time after relapse or metastasis is about 10 to 12 months. 4 The results of chemotherapy are discouraging. Therefore, many patients accept complementary therapies during cancer treatment to improve QoL and prolong survival time. The earlier study by Cameron and Pauling 22 demonstrated that IVC significantly prolonged survival time of 11 breast cancer patients in comparison with the control candidates (median survival time was 363 days vs 64 days). Our previous Phase I study 21 demonstrated that 1 g/kg/day IVC was safe and well tolerated in non–small cell lung cancer patients. Therefore, this is the first study to evaluate the clinical response by administering chemotherapy plus IVC in advanced TNBC patients.
In this study, we did not find significant differences of tumor RR (RR and CBR, Table 2, P = .470 and .526) between the control and treatment groups. However, we noticed that KPS scores after 2 cycles of treatment were significantly better than in the control group and also than before the treatment, while the control group had no significant change before and after the treatment. This indicated that IVC can improve general conditions of these patients during chemotherapy. It might be due to the ability of IVC to reduce the toxicities associated with gemcitabine and carboplatin.
We found that the incidence of grade III-IV adverse reactions in the treatment group was significantly lower than that in the control group, which included leukopenia (14.3% vs 25.8%), anemia (11.5% vs 20%), and thrombocytopenia (17.2% vs 31.4%; Table 4, P < .05). This suggested that IVC can significantly decrease the incidence of adverse reactions during chemotherapy, improve patient tolerance to chemotherapy, and enable the successful completion of the whole process. Zhang 23 administered traditional Chinese medicine (TCM) and chemotherapy to treat TNBC patients with liver metastasis, which showed grade III to IV digestive tract reactions were 40%, and that grade III to IV bone marrow suppression was 36%. Our study suggested that the frequency of the occurrence and the severity of adverse reactions during the treatment were significantly reduced in comparison with Zhang, indicating that the application of IVC in reducing side effects of chemotherapy was better than usage of TCM alone (Shugan Jianpi Yishen Tang, which contains doses of TCM for dredging the liver, and strengthening the spleen and kidney).
Median PFS and OS in the treatment group in this study were significantly longer than in the control group. The median PFS and median OS of the control group in our study were similar to another study, 24 which administered only carboplatin and gemcitabine; the median time-to-progression was 7 months, and the median OS was 10.5 months. It suggested that IVC can prolong the PFS and OS of advanced TNBC patients and improve clinical outcome.
The responses of different cancers to IVC therapy are different, depending on their underlying mechanisms. Several possible anticancer mechanisms of IVC have been demonstrated, such as extracellular generation of hydrogen peroxide, 25 downregulation of hypoxia-inducible factor, and enhancement of ten eleven translocation enzyme activity, 26 as well as antioxidant and anti-inflammatory functions. 27 In this study, we speculated the possible underlying mechanism, which was addressed in our previous in vitro study 28 : vitamin C can modulate the MDA-MB-468 cell cycle, suppress the process of angiogenesis, and inhibit cell invasion through the EGFR/PI3K/Akt pathway. In many cancers, this pathway is overactive, thus reducing apoptosis and allowing proliferation. 29
Limitations of this retrospective study include 3 aspects; first, we reviewed previous clinical data, which restricts the analysis of data that are available in those records; second, patients were self-selected/self-financed to receive IVC therapy, which limited this study from providing more robust evidence; third, this study had a small sample size.
Conclusion
This study suggested that although there was no significant difference in tumor response between the 2 groups, IVC can significantly reduce the side effects from chemotherapy, which might contribute to the longer survival of patients in the treatment group. Thus, IVC plus chemotherapy might be an option for advanced TNBC patients. However, the results and limitations that arise from this retrospective study suggest the need for well-designed, prospective randomized controlled trials to evaluate the effect of IVC in combination with chemotherapy in patients with advanced TNBC.
Research Data
Research_Data for A Retrospective Study of Gemcitabine and Carboplatin With or Without Intravenous Vitamin C on Patients With Advanced Triple-Negative Breast Cancer
Research_Data for A Retrospective Study of Gemcitabine and Carboplatin With or Without Intravenous Vitamin C on Patients With Advanced Triple-Negative Breast Cancer by Junwen Ou, Xinyu Zhu, Hongyu Zhang, Yanping Du, Pengfei Chen, Junhua Wang, Xiufan Peng, Shuang Bao, Xinting Zhang, Tao Zhang and Clifford L. K. Pang in Integrative Cancer Therapies
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Traditional Chinese Medicine Bureau of Guangdong Province, China (Funding Number: 20161046).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.